
Characterization and Management of Adverse Events of Low-Dose Oral Minoxidil Treatment for Alopecia: A Narrative Review

 , ,
, ,
Abstract
1. Introduction
2. Methods
3. Hypertrichosis
3.1. Frequency and Risk Factors
- Minoxidil dose. Dose is the main factor associated with hypertrichosis, with a statistically significant association [2,9,10]. A meta-analysis of individual patient data found that the frequency of hypertrichosis increased with higher doses of LDOM [10]. Other recent meta-analyses have found similar results, confirming that hypertrichosis is a dose-dependent AE [9,11]. It is estimated that for every up-titration of 1 mg, the risk of hypertrichosis increases by 17.6% [12].
- Gender and age. Several studies have shown a higher frequency of hypertrichosis in women than in men [2,3,9]. This may seem contrary to the aforementioned dose-dependent relationship, given that men usually receive higher doses than women. However, there is probably a reporting bias in the detection of this AE since many men do not perceive the increase in body and facial hair as an AE or are not even aware of it, while, in our experience, women are usually more concerned about this AE. In this sense, it has been observed that the average dose to produce hypertrichosis is higher in men (4.1 mg) than in women (1.4 mg) [2]. In addition, dose reduction or discontinuation of LDOM due to hypertrichosis is much more common in women than in men [13]. In terms of age, only one study found that younger age was associated with an increased risk of hypertrichosis in men [4].
- Phototype. Although it has not been objectively studied, patients with dark-colored hair tend to have more obvious hypertrichosis than those with light hair [3]. In fact, it can be observed that the reported rate of hypertrichosis is usually higher in studies carried out in geographical areas where dark-colored hair predominates, such as Brazil or Thailand [4,8].
- Pharmaceutical form and posology. Vaño-Galvan’s study showed an increased risk of hypertrichosis in patients taking minoxidil compounded capsules compared to those taking commercially available tablets, suggesting that it may be due to some dose variability in the compounded dosages. Additionally, an every-other-day regimen was associated with a lower risk of hypertrichosis compared to a daily regimen; however, this observation was not substantiated with a plausible explanation [2].
- Concomitant treatments. Several studies suggest that concomitant treatment of LDOM with androgen receptor inhibitor drugs, such as bicalutamide or spironolactone, may reduce the frequency of hypertrichosis.
3.2. Affected Areas
3.3. Severity and Management
4. Blood Pressure
4.1. Influence of LDOM on Blood Pressure
4.2. Postural Hypotension, Orthostatism or Dizziness
5. Fluid Retention, Edema
5.1. Frequency and Risk Factors
5.2. Affected Areas
5.3. Severity and Management
6. Tachycardia, Arrhythmias and ECG Abnormalities
7. Pericardial Effusion and Serious Adverse Effects
8. Other Adverse Effects
9. Summary and Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Loniten (Minoxidil Tablets USP). Pharmacia & Upjohn Company LLC, Pfizer Canada Inc.: Kirkland, QC, Canada. 2013. Available online: https://labeling.pfizer.com/ShowLabeling.aspx?id=2199 (accessed on 21 September 2024).
- Vañó-Galván, S.; Pirmez, R.; Hermosa-Gelbard, A.; Moreno-Arrones, Ó.M.; Saceda-Corralo, D.; Rodrigues-Barata, R.; Jimenez-Cauhe, J.; Koh, W.L.; Poa, J.E.; Jerjen, R.; et al. Safety of low-dose oral minoxidil for hair loss: A multicenter study of 1404 patients. J. Am. Acad. Dermatol. 2021, 84, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Talukder, M.; Shemer, A. Efficacy and safety of low-dose oral minoxidil in the management of androgenetic alopecia. Expert Opin. Pharmacother. 2024, 25, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Sanabria, B.; de Nardo Vanzela, T.; Miot, H.A.; Müller Ramos, P. Adverse effects of low-dose oral minoxidil for androgenetic alopecia in 435 patients. J. Am. Acad. Dermatol. 2021, 84, 1175–1178. [Google Scholar] [CrossRef] [PubMed]
- Bonilla Hernandez, J.D.; Vaño Galvan, S.; Saceda Corralo, D.; Imbernon, A. Minoxidil oral en alopecias no androgénicas. Piel 2023, 39, 161–168. [Google Scholar] [CrossRef]
- Vañó-Galván, S.; Fernandez-Crehuet, P.; Garnacho, G.; Gómez-Zubiaur, A.; Hermosa-Gelbard, A.; Moreno-Arrones, O.; Saceda-Corralo, D.; Serrano, C.; Spanish Trichology Research Group. Recomendaciones sobre el manejo clínico de la alopecia androgénica: Un documento de consenso del Grupo Español de Tricología de la Academia Española de Dermatología y Venereología. Actas Dermosifiliogr. 2024, 115, 347–355. [Google Scholar] [CrossRef]
- Pirmez, R.; Salas-Callo, C.I. Very low dose oral minoxidil in male androgenetic alopecia: A study with quantitative trichoscopic documentation. J. Am. Acad. Dermatol. 2020, 82, e21–e22. [Google Scholar] [CrossRef]
- Panchaprateep, R.; Lueangarun, S. Efficacy and Safety of Oral Minoxidil 5 mg Once Daily in the Treatment of Male Patients with Androgenetic Alopecia: An Open-Label and Global Photographic Assessment. Dermatol. Ther. 2020, 10, 1345–1357. [Google Scholar] [CrossRef]
- Gupta, A.K.; Talukder, M.; Shemar, A.; Piraccini, B.M.; Tosti, A. Low-Dose Oral Minoxidil for Alopecia: A Comprehensive Review. Skin Appendage Disord. 2023, 9, 423–437. [Google Scholar] [CrossRef]
- Jimenez‐Cauhe, J.; Saceda‐Corralo, D.; Rodrigues‐Barata, R.; Moreno‐Arrones, O.M.; Ortega‐Quijano, D.; Fernandez‐Nieto, D.; Jaen‐Olasolo, P.; Vaño‐Galvan, S. Safety of low-dose oral minoxidil treatment for hair loss. A systematic review and pooled-analysis of individual patient data. Dermatol. Ther. 2020, 33, e14106. [Google Scholar] [CrossRef]
- Gupta, A.K.; Talukder, M.; Venkataraman, M.; Bamimore, M.A. Minoxidil: A comprehensive review. J. Dermatolog. Treat. 2022, 33, 1896–1906. [Google Scholar] [CrossRef]
- Gupta, A.K.; Hall, D.C.; Talukder, M.; Bamimore, M.A. There Is a Positive Dose-Dependent Association between Low-Dose Oral Minoxidil and Its Efficacy for Androgenetic Alopecia: Findings from a Systematic Review with Meta-Regression Analyses. Skin Appendage Disord. 2022, 8, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Cauhe, J.; Saceda-Corralo, D.; Rodrigues-Barata, R.; Hermosa-Gelbard, A.; Moreno-Arrones, O.M.; Gil-Redondo, R.; Ortega-Quijano, D.; Fernandez-Nieto, D.; Jaen-Olasolo, P.; Vaño-Galvan, S. Characterization and management of hypertrichosis induced by low-dose oral minoxidil in the treatment of hair loss. J. Am. Acad. Dermatol. 2021, 84, 222–223. [Google Scholar] [CrossRef] [PubMed]
- Moussa, A.; Kazmi, A.; Bokhari, L.; Sinclair, R.D. Bicalutamide improves minoxidil-induced hypertrichosis in female pattern hair loss: A retrospective review of 35 patients. J. Am. Acad. Dermatol. 2022, 87, 488–490. [Google Scholar] [CrossRef]
- Trüeb, R.M.; Luu, N.N.C.; Rezende, H.D. Comment on “Bicalutamide Improves Minoxidil-Induced Hypertrichosis in Female Pattern Hair Loss: A Retrospective Review of 35 Patients”. J. Am. Acad. Dermatol. 2022, 87, e29–e30. [Google Scholar] [CrossRef] [PubMed]
- Olamiju, B.; Craiglow, B.G. Combination oral minoxidil and spironolactone for the treatment of androgenetic alopecia in adolescent girls. J. Am. Acad. Dermatol. 2021, 84, 1689–1691. [Google Scholar] [CrossRef]
- Darendeliler, F.; Baş, F.; Balaban, S.; Bundak, R.; Demirkol, D.; Saka, N.; Günöz, H. Spironolactone therapy in hypertrichosis. Eur. J. Endocrinol. 1996, 135, 604–608. [Google Scholar] [CrossRef]
- Nohria, A.; Desai, D.; Sikora, M.; Mandal, S.; Caplan, A.; Shapiro, J.; Sicco, K.I.L. To evaluate hypertrichosis with low dose oral minoxidil and spironolactone combination therapy for alopecia. Arch. Dermatol. Res. 2024, 316, 510. [Google Scholar] [CrossRef]
- Sinclair, R.D. Female pattern hair loss: A pilot study investigating combination therapy with low-dose oral minoxidil and spironolactone. Int. J. Dermatol. 2018, 57, 104–109. [Google Scholar] [CrossRef]
- Pang, K.C.; Nguyen, T.P.; Upreti, R. Case Report: Successful Use of Minoxidil to Promote Facial Hair Growth in an Adolescent Transgender Male. Front. Endocrinol. 2021, 12, 725269. [Google Scholar] [CrossRef]
- Shokravi, A.; Zargham, H. Facial hair enhancement with minoxidil-an off-label use. SAGE Open Med. Case Rep. 2024, 12, 2050313X241231490. [Google Scholar] [CrossRef]
- Beach, R.A.; McDonald, K.A.; Muylaert Barrett, B. Low-dose oral minoxidil for treating alopecia: A 3-year North American retrospective case series. J. Am. Acad. Dermatol. 2021, 84, 761–763. [Google Scholar] [CrossRef] [PubMed]
- Pirmez, R.; Spagnol Abraham, L. Eyebrow Regrowth in Patients with Frontal Fibrosing Alopecia Treated with Low-Dose Oral Minoxidil. Skin Appendage Disord. 2021, 7, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Desai, D.D.; Nohria, A.; Brinks, A.; Needle, C.; Shapiro, J.; Sicco, K.I.L. Minoxidil-induced hypertrichosis: Pathophysiology, clinical implications, and therapeutic strategies. JAAD Rev. 2024, 2, 41–49. [Google Scholar] [CrossRef]
- Trüeb, R.M. Causes and management of hypertrichosis. Am. J. Clin. Dermatol. 2002, 3, 617–627. [Google Scholar] [CrossRef]
- Messenger, A.G.; Rundegren, J. Minoxidil: Mechanisms of action on hair growth. Br. J. Dermatol. 2004, 150, 186–194. [Google Scholar] [CrossRef]
- Fleishaker, J.C.; Andreadis, N.A.; Welshman, I.R.; Wright, C.E. The pharmacokinetics of 2.5- to 10-mg oral doses of minoxidil in healthy volunteers. J. Clin. Pharmacol. 1989, 29, 162–167. [Google Scholar] [CrossRef]
- Ramos, P.M.; Sinclair, R.D.; Kasprzak, M.; Miot, H.A. Minoxidil 1 mg Orally versus Minoxidil 5% Solution Topically for the Treatment of Female Pattern Hair Loss: A Randomized Clinical Trial. J. Am. Acad. Dermatol. 2020, 82, 252–253. [Google Scholar] [CrossRef]
- Ong, M.; Do, H.; Ho, B.; Lipner, S.R. Low-dose oral minoxidil for androgenetic alopecia is not associated with clinically significant blood-pressure changes: A retrospective study. J. Am. Acad. Dermatol. 2024, 90, 425–427. [Google Scholar] [CrossRef]
- Sanabria, B.D.; Palmegiani, E.; Seron, A.F.; Perdomo, Y.C.; Miot, H.A.; Müller Ramos, P. Prospective cardiovascular evaluation with 24-hour Holter and 24-hour ambulatory blood pressure monitoring in men using 5-mg oral minoxidil for androgenetic alopecia. J. Am. Acad. Dermatol. 2023, 88, 436–437. [Google Scholar] [CrossRef]
- Jimenez-Cauhe, J.; Saceda-Corralo, D.; Hermosa-Gelbard, A.; Moreno-Arrones, O.M.; Pindado-Ortega, C.; Berna-Rico, E.d.D.; Ortega-Quijano, D.; Fernandez-Nieto, D.; Vaño-Galvan, S. Before-after study with 24-hour ambulatory blood pressure monitoring after the first dose of 5 mg oral minoxidil. J. Am. Acad. Dermatol. 2022, 87, e235–e237. [Google Scholar] [CrossRef]
- Imhof, R.; Villalpando, B.; Torgerson, R. Safety and tolerability of low dose oral minoxidil monotherapy in female pattern hair loss: A retrospective review with longitudinal ambulatory blood pressure monitoring. JAAD Int. 2023, 13, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Weichert, M.; Guo, W.; Ruzic, R.; Briley, J. Low-dose oral minoxidil does not significantly affect blood pressure: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2025, 92, 554–555. [Google Scholar] [CrossRef] [PubMed]
- Sanabria, B.D.; Perdomo, Y.C.; Miot, H.A.; Ramos, P.M. Oral minoxidil 7.5 mg for hair loss increases heart rate with no change in blood pressure in 24 h Holter and 24 h ambulatory blood pressure monitoring. An. Bras. Dermatol. 2024, 99, 734–736. [Google Scholar] [CrossRef] [PubMed]
- Ramos, P.M.; Melo, D.F.; Bhoyrul, B.; Sanabria, B.D.; Jimenez-Cauhe, J.; Saceda-Corralo, D.; Sharma, P.; Ramos, M.; Miot, H.A.; Vaño-Galvan, S. Prospective evaluation of blood pressure, heart rate, and side effects in hypertensive patients using low-dose oral minoxidil for hair loss. J. Am. Acad. Dermatol. 2024, 91, 1011–1012. [Google Scholar] [CrossRef]
- Jimenez-Cauhe, J.; Pirmez, R.; Müller-Ramos, P.; Melo, D.F.; Ortega-Quijano, D.; Moreno-Arrones, O.; Saceda-Corralo, D.; Gil-Redondo, R.; Hermosa-Gelbard, A.; Dias-Sanabria, B.; et al. Safety of Low-Dose Oral Minoxidil in Patients With Hypertension and Arrhythmia: A Multicenter Study of 264 Patients. Actas Dermosifiliogr. 2024, 115, T28–T35. [Google Scholar] [CrossRef]
- Albaladejo Blanco, C.; Alonso Martínez, R. Oral minoxidil unrelated to arterial hypertension: Incidences due to its increasing use. Hipertens. Riesgo Vasc. 2023, 40, 228–230. [Google Scholar] [CrossRef]
- Godse, K.; De, A.; Vedamurthy, M.; Shankar, D.S.K.; Shah, B.; Girdhar, M.; Bhat, R.; Ganjoo, A.; Tahiliani, S.; Patil, A. Low-dose Oral Minoxidil in the Treatment of Alopecia: Evidence and Experience-based Consensus Statement of Indian Experts. Int. J. Trichology 2023, 15, 91. [Google Scholar] [CrossRef]
- Sica, D.A. Minoxidil: An underused vasodilator for resistant or severe hypertension. J. Clin. Hypertens. 2004, 6, 283–287. [Google Scholar] [CrossRef]
- Garner, B.R.; Stolarz, A.J.; Stuckey, D.; Sarimollaoglu, M.; Liu, Y.; Palade, P.T.; Rusch, N.J.; Mu, S. KATP Channel Openers Inhibit Lymphatic Contractions and Lymph Flow as a Possible Mechanism of Peripheral Edema. J. Pharmacol. Exp. Ther. 2021, 376, 40–50. [Google Scholar] [CrossRef]
- Salas, J.; Esse, I.; Kincaid, C.M.; Birda, A.; Choe, S.; Mesinkovska, N.A. Characterizing Low-Dose Oral Minoxidil-Induced Peripheral Edema in Alopecia Patients. J. Am. Acad. Dermatol. 2025, 92, 632–634. [Google Scholar] [CrossRef]
- Mir-Bonafé, J.F.; Mir-Bonafé, M.; Rozas-Muñoz, E.; Mir-Bonafé, J.M. Morning Periorbital Edema Related to Low-Dose Oral Minoxidil. Actas Dermosifiliogr. 2023, 114, 460–461. [Google Scholar] [CrossRef]
- Gbadamosi, W.A.; Melvin, J.; Lopez, M. Atypical Case of Minoxidil-Induced Generalized Anasarca and Pleuropericardial Effusion. Cureus 2021, 13, e15424. [Google Scholar] [CrossRef] [PubMed]
- Dlova, N.C.; Jacobs, T.; Singh, S. Pericardial, pleural effusion and anasarca: A rare complication of low-dose oral minoxidil for hair loss. JAAD Case Rep. 2022, 28, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Arrones, O.; Rodrigues-Barata, R.; Morales, C.; Imbernon-Moya, A.; Saceda-Corralo, D.; Matji, A.; Vañó-Galván, S. Serious Adverse effects From Compounding Errors With Low-Dose Oral Minoxidil for Alopecia Treatment. Actas Dermosifiliogr. 2022, 113, 725–727. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture; US Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed. Dietary Guidelines, December 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf (accessed on 19 November 2024).
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef]
- Devjani, S.; Ezemma, O.; Jothishankar, B.; Saberi, S.; Kelley, K.J.; Makredes Senna, M. Efficacy of Low-Dose Spironolactone for Hair Loss in Women. J. Drugs Dermatol. 2024, 23, e91–e92. [Google Scholar]
- Martin, W.B.; Spodick, D.H.; Zins, G.R. Pericardial disorders occurring during open-label study of 1,869 severely hypertensive patients treated with minoxidil. J. Cardiovasc. Pharmacol. 1980, 2 (Suppl. S2), S217–S227. [Google Scholar] [CrossRef]
- Reichgott, M.J. Minoxidil and pericardial effusion: An idiosyncratic reaction. Clin. Pharmacol. Ther. 1981, 30, 64–70. [Google Scholar] [CrossRef]
- Ibraheim, M.K.; Elsensohn, A.; Hauschild, C.; Hilliard, A.; Dao, H. Low dose oral minoxidil and the conundrum of cardiovascular complications. Dermatol. Online J. 2023, 29, 2. [Google Scholar] [CrossRef]
- Pasala, K.K.; Gujja, K.; Prabhu, H.; Vasavada, B.; Konka, S. Short-term minoxidil use associated with pericardial effusion and cardiac tamponade: An uncommon presentation. Am. J. Ther. 2012, 19, e186–e188. [Google Scholar] [CrossRef]
- Bentivegna, K.; Zhou, A.E.; Adalsteinsson, J.A.; Sloan, B. Letter in reply: Pericarditis and peripheral edema in a healthy man on low-dose oral minoxidil therapy. JAAD Case Rep. 2022, 29, 110–111. [Google Scholar] [CrossRef] [PubMed]
- Trüeb, R.M.; Caballero-Uribe, N.; Luu, N.N.C.; Dmitriev, A. Serious complication of low-dose oral minoxidil for hair loss. JAAD Case Rep. 2022, 30, 97–98. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. List of Nationally Authorised Medicinal Products: Minoxidil (Non-Topical Formulations). Available online: www.ema.europa.eu/en/documents/psusa/minoxidil-non-topical-formulations-list-nationally-authorised-medicinal-products-psusa00002066202010_en.pdf (accessed on 25 February 2025).
- Vademecum Vidal. Equivalencias Internacionales. Available online: www.vademecum.es/busqueda_internacional?equivalencia=loniten (accessed on 25 February 2025).
- Desai, S.; Sadur, A.; Farah, M.; Nasseri, M.; Friedman, A. The Potential Impact of Off-Label Medication Use on Patient Access: A Cross-Sectional Survey of Minoxidil Availability. J. Drugs Dermatol. 2024, 23, 1360–1361. [Google Scholar] [CrossRef] [PubMed]
- Gudeman, J.; Jozwiakowski, M.; Chollet, J.; Randell, M. Potential Risks of Pharmacy Compounding. Drugs R D 2013, 13, 1–8. [Google Scholar] [CrossRef]
- Kincaid, C.M.; Sharma, A.N.; Sargent, B.; Gradus-Pizlo, I.; Dineen, E.H.; Mesinkovska, N.A. Evaluation of Pericardial Effusions in Alopecia Patients on Low-Dose Oral Minoxidil Therapy. J. Drugs Dermatol. 2024, 23, 725–728. [Google Scholar] [CrossRef]
- Nohria, A.; Desai, D.; Sikora, M.; Mandal, S.; Shapiro, J.; Lo Sicco, K. Combating “dread shed”: The impact of overlapping topical and oral minoxidil on temporary hair shedding during oral minoxidil initiation. JAAD Int. 2024, 15, 220–224. [Google Scholar] [CrossRef]
- Blume-Peytavi, U.; Hillmann, K.; Dietz, E.; Canfield, D.; Garcia Bartels, N. A randomized, single-blind trial of 5% minoxidil foam once daily versus 2% minoxidil solution twice daily in the treatment of androgenetic alopecia in women. J. Am. Acad. Dermatol. 2011, 65, 1126–1134.e2. [Google Scholar] [CrossRef]
- Shadi, Z. Compliance to Topical Minoxidil and Reasons for Discontinuation among Patients with Androgenetic Alopecia. Dermatol. Ther. 2023, 13, 1157–1169. [Google Scholar] [CrossRef]
- Desai, D.; Nohria, A.; Sikora, M.; Buontempo, M.; Shapiro, J.; Caplan, A.S.; Garshick, M.; Sicco, K.I.L. Assessing the influence of medications with antagonistic effects on low-dose oral minoxidil in patients with alopecia: A retrospective study. JAAD Int. 2024, 17, 1–3. [Google Scholar] [CrossRef]
- Alhanshali, L.; Desai, D.; Nohria, A.; Shapiro, J.; Lo Sicco, K. Oral minoxidil and the exacerbation of alcohol hangover symptoms. Int. J. Dermatol. 2024, 63, 975–976. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Study | Design | Results |
|---|---|---|
| Ong et al., 2024 [29] | n = 151 (89 women) LDOM 0.625–5 mg Retrospective Single measurement at baseline and with LDOM (mean 17 weeks) | - No significant variation in SBP or DBP - Only a significant slight reduction in DBP was found in men aged 35–49 years (81 → 78 mmHg) |
| Imhof et al., 2023 [32] | n = 25 (women) LDOM 0.625–2.5 mg Retrospective ABPM 24 h baseline and at 16 weeks | - Slight reduction in SBP (−2.8 mmHg) and DBP (−1.4 mmHg) - HR increase (+4.4 bpm) - Does not specify level of statistical significance |
| Jimenez-Cauhe et al., 2023 [31] | n = 10 (men), LDOM 5 mg Before-After Study ABPM 24 h baseline and the day of the first intake | - No significant differences in mean SBP, DBP or HR in 24 h ABPM - Slight and non-significant reduction in DBP and DBP in the first 2 h after taking LDOM |
| Sanabria et al., 2022 [30] | n = 34 (men), LDOM 5 mg Prospective ABPM 24 h at baseline and at 24 weeks | - Significant slight reduction in SBP (−3 mmHg; 125 → 122) and DBP (−2 mmHg; 76 → 74). - Non-significant increase in HR (+2.4 bpm; 72.5 → 74.9) |
| Panchaprateep et al., 2020 [8] | n = 30 (men), LDOM 5 mg Retrospective Single baseline measurement, 1 h after first dose and at 24 weeks | - 1 h after the first dose: non-significant variation in SBP (−2.5 mmHg), DBP (+0.5 mmHg) and HR (−4 bpm) - 24 weeks: non-significant reduction in SBP (−3.9 mmHg) and DBP (−1.1 mmHg). Non-significant increase in HR (+0.8 bpm) |
| Ramos et al., 2019 [28] | n = 30 (female), LDOM 1 mg RCT (vs. topical minoxidil) Single measurement at baseline and at 24 weeks | - Non-significant reduction in MAP (−2 mmHg; 93 → 91). No differences compared to the control group - Significant increase in HR (72 → 77 bpm), with differences with the control group |
| Article | Patient Characteristics | Minoxidil Treatment | Clinical Presentation | Intervention |
|---|---|---|---|---|
| Dlova et al., 2022 [44] South Africa | Female, 40 years old No prior comorbidities | 0.25 mg for 3 weeks Not specified if it was a pharmaceutical compounding | Generalized edema (extremities and face), pericardial effusion | Hospital admission LDOM suspension IV Furosemide |
| Trüeb et al., 2022 [54] Switzerland | “Young, Healthy Woman” Age not specified | 1.25 mg for “few weeks” Not specified if it was a pharmaceutical compounding | Dyspnea, chest pain, orthostatism, leg edema, pericardial effusion. | Not specified |
| Bentivegna et al., 2022 [53] USA | Male, 52 years old High intensity sport Personal history of pericarditis and pericardial effusion 5 years earlier | 2.5 mg for 2 weeks Commercially available drug | Peripheral edema and pericarditis, without pericardial effusion | LDOM suspension Oral colchicine for 3 months |
| Adverse Effect | Characteristics | Management |
|---|---|---|
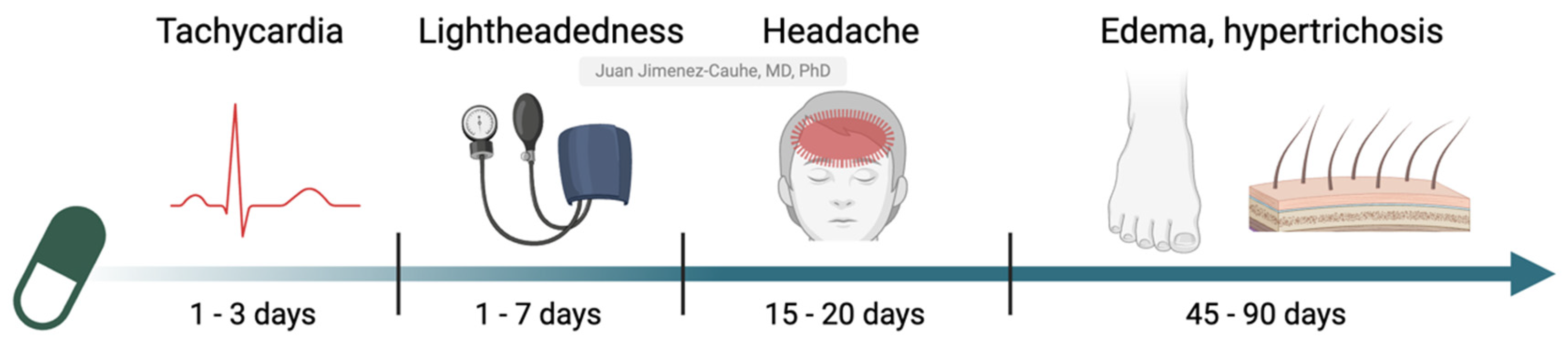
| Leg edema | - 1.3–4% of patients - Appears at 2 months (45–90 days) - More common in women and hot weather | - Restriction of salt intake - Furosemide, spironolactone (women) - Reduce or discontinue LDOM |
| Periorbital or facial edema | - 0.3–1% of patients - Usually in the morning and self-resolving in minutes or hours | - Explain and calm the patient - Reduce or discontinue LDOM if persistent |
| Dizziness, lightheadedness, postural hypotension | - 1–1.7% of patients - Appears in the first week - More common in women and patients on antihypertensive treatment | - Take LDOM at night; increase water intake; take sodium chloride or licorice gum - Adjust antihypertensive - Reduce or discontinue LDOM |
| Tachycardia | - 0.9–4% of patients - Typically appears on the first day (1–3 days) - Usually mild and transient | If persistent: - Refer to cardiologist - Reduce or discontinue LDOM - Add beta-blockers |
| Headache | - 0.4–9% of patients - Appears at 15–20 days - Usually mild and transient | - Common analgesics - Reduce or discontinue LDOM if persistent |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jimenez-Cauhe, J.; Lo Sicco, K.I.; Shapiro, J.; Hermosa-Gelbard, A.; Burgos-Blasco, P.; Melian-Olivera, A.; Ortega-Quijano, D.; Pindado-Ortega, C.; Buendia-Castaño, D.; Asz-Sigall, D.; et al. Characterization and Management of Adverse Events of Low-Dose Oral Minoxidil Treatment for Alopecia: A Narrative Review. J. Clin. Med. 2025, 14, 1805. https://doi.org/10.3390/jcm14061805
Jimenez-Cauhe J, Lo Sicco KI, Shapiro J, Hermosa-Gelbard A, Burgos-Blasco P, Melian-Olivera A, Ortega-Quijano D, Pindado-Ortega C, Buendia-Castaño D, Asz-Sigall D, et al. Characterization and Management of Adverse Events of Low-Dose Oral Minoxidil Treatment for Alopecia: A Narrative Review. Journal of Clinical Medicine. 2025; 14(6):1805. https://doi.org/10.3390/jcm14061805
Chicago/Turabian StyleJimenez-Cauhe, Juan, Kristen I. Lo Sicco, Jerry Shapiro, Angela Hermosa-Gelbard, Patricia Burgos-Blasco, Ana Melian-Olivera, Daniel Ortega-Quijano, Cristina Pindado-Ortega, Diego Buendia-Castaño, Daniel Asz-Sigall, and et al. 2025. "Characterization and Management of Adverse Events of Low-Dose Oral Minoxidil Treatment for Alopecia: A Narrative Review" Journal of Clinical Medicine 14, no. 6: 1805. https://doi.org/10.3390/jcm14061805
APA StyleJimenez-Cauhe, J., Lo Sicco, K. I., Shapiro, J., Hermosa-Gelbard, A., Burgos-Blasco, P., Melian-Olivera, A., Ortega-Quijano, D., Pindado-Ortega, C., Buendia-Castaño, D., Asz-Sigall, D., & Vaño-Galvan, S. (2025). Characterization and Management of Adverse Events of Low-Dose Oral Minoxidil Treatment for Alopecia: A Narrative Review. Journal of Clinical Medicine, 14(6), 1805. https://doi.org/10.3390/jcm14061805