
Oligometastatic Mixed Neuroendocrine Adenocarcinoma of the Esophago-Gastric Junction: A Case of Successful Multidisciplinary Management, the Lessons Learnt and Review of the Literature

 ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Case Presentation
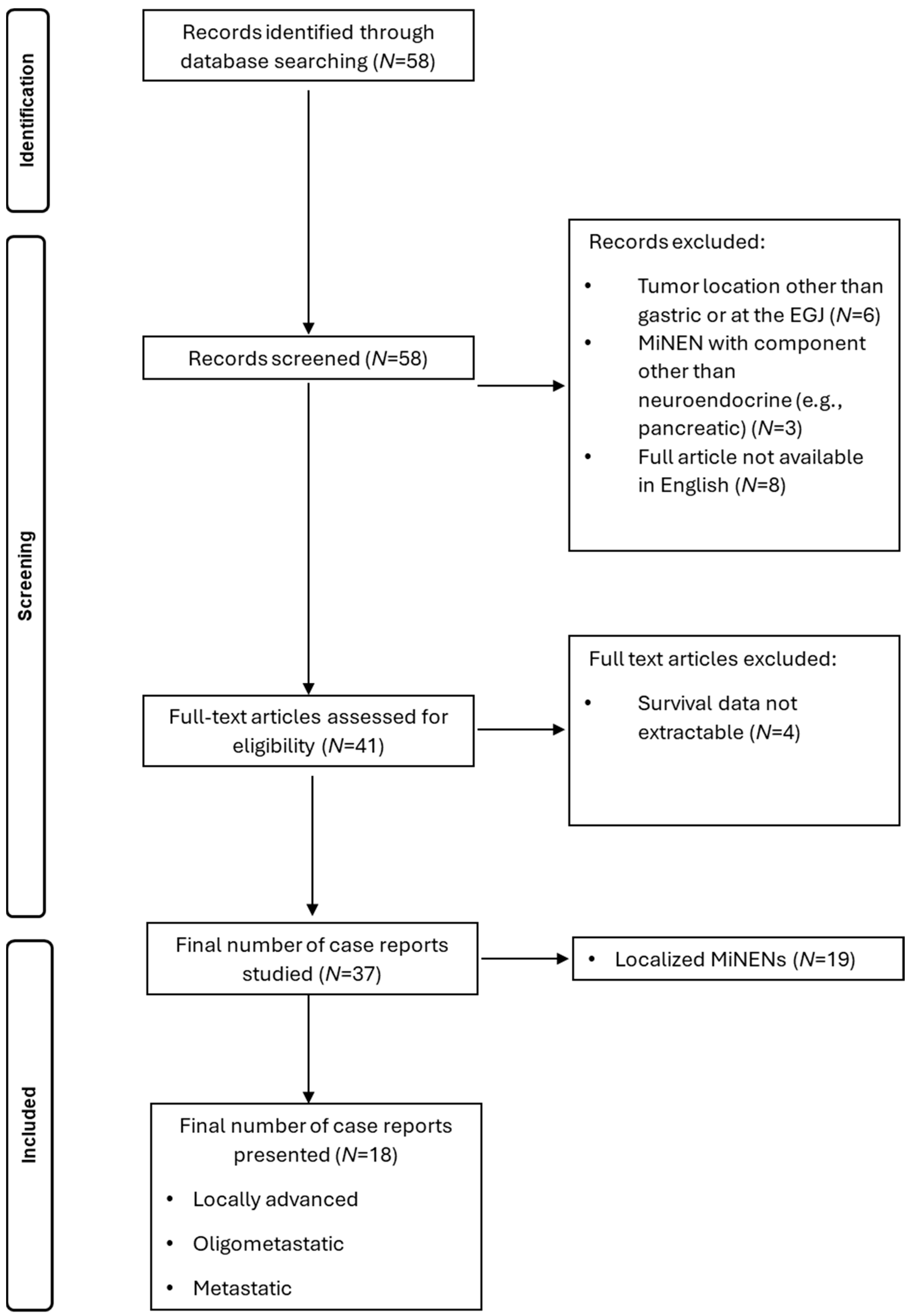
2.3. Search of Literature
3. Results
3.1. Case Management
3.2. Literature Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Locally Advanced | Oligo-Metastatic | Metastatic | Neuroendocrine to Non-Neuroendocrine Ratio | Induction Chemotherapy Regimen | Surgery | Adjuvant Therapy | Other Therapies | Overall Survival |
|---|---|---|---|---|---|---|---|---|---|
| Zheng et al., 2024 [17] | Yes | No | No | 50%/50% | No | Total gastrectomy pT3N1M0 | Delayed due to postoperative condition | Progression with liver metastasis treated with etoposide, cisplatin, toripalumab (6 cycles) | Ongoing at 1 y |
| Lun Tao Woo et al., 2022 Patient 1 [18] | Yes | Left liver lobe | No | 80%/20% | Irinotecan plus cisplatin (4 cycles) | Total gastrectomy and partial left liver resection pT1aN1M0 | Irinotecan plus cisplatin (2 cycles) | No | Ongoing at 3 y |
| Lun Tao Woo et al., 2022 Patient 2 [18] | Yes | No | No | 80%/20% | No | Total gastrectomy pT4aN3aM0 | Irinotecan plus cisplatin (6 cycles) | VATS due to recurrence at 2 y with metastatic lesions at the lower lobe of the right lung | Ongoing at 7 y |
| Deliwala et al., 2021 [32] | Yes | No | Left liver lobe, paraaortic lymph nodes | N/A | Carboplatin plus etoposide (2 cycles) | No | No | Capecitabine plus temozolomide following osseous metastases | 3 m, disease progression |
| Millet et al., 2021 [33] | Yes | No | Liver, retroperitoneal adenopathy, mesenteric implants | N/A | No | No | No | Palliative treatment | Unknown, disease progression |
| Ricco et al., 2020 [19] | Yes | No | No | 60%/40% | Carboplatin plus etoposide (3 cycles) | Total gastrectomy pT4N1M0 | mFOLFOX6 (6 cycles) | Multiple chemotherapy regimens, radiation therapy and antiPD-1 treatment due to disease progression | Ongoing |
| Lin et al., 2019 [20] | Yes | No | No | N/A | No | Total gastrectomy | Oxaliplatin plus capecitabine (4 cycles) | Radiofrequency Ablation due to hepatic metastasis at 4 cycles, paclitaxel plus Cisplatin (6 cycles), Abatinib | Ongoing |
| Golombek et al., 2019 [34] | Yes | No | Liver, distant lymph nodes | N/A | Etoposide plus cisplatin | No | No | No | 9 months, disease progression |
| Tang et al., 2017 Patient 1 [21] | Yes | No | No | 70%/30% | No | Total gastrectomy pT4aN1M0 | Etoposide plus cisplatin | No | Ongoing at 6-month follow up |
| Tang et al., 2017 Patient 2 [21] | Yes | No | No | 30%/70% | No | Total gastrectomy pT4aN1M0 | No treatment due to general weakness | No | 6 m, general weakness |
| Kheiri et al., 2017 [22] | Yes | No | No | N/A | No | Partial gastrectomy T4aN2M0 | mFOLFOX (12 cycles) | No | Ongoing at 2 y follow up |
| Pham et al., 2017 [35] | Yes | No | Liver, pancreas, distant lymph nodes | 80–90%/10–20% | No | No | S-1, CDDP, Trastuzumab (5 cycles) | Yes | 7 m, disease progression |
| Ambesh et al., 2017 [23] | Yes | No | No | 60%/40% | No | Ivor-Lewis Esophagogastrectomy pT3N1M0 | No | No | Unknown |
| Cazzo et al., 2016 [24] | Yes | No | No | 40%/60% | No | Total gastrectomy pT4N0M0 | 5-fluorouracil plus leucovorin (5 cycles) plus radiation therapy | No | Ongoing at 1 y follow up |
| Taguchi et al., 2015 [25] | Yes | No | No | 30%/70% | No | Total gastrectomy | Tegafur plus uracil | No | Ongoing at 1 y and 4 m |
| Gurzu et al., 2015 [26] | Yes | No | No | 40%/60% | No | Total gastrectomy pT4N3b | Patient refused treatment | No | 5 m, disease progression |
| Levi et al., 2014 [27] | Yes | No | No | 30%/70% | No | Total gastrectomy pT4aN0M0 | Cisplatin, doxorubicin, and vincristine | No | Ongoing at 6 m follow up |
| Zhang et al., 2014 [29] | Yes | Left liver lobe | No | N/A | No | Total gastrectomy and left liver resection | Patient refused treatment | No | 2.5 m, disease progression |
| Pericleous et al., 2012 [31] | Yes | No | >3 liver lesions | N/A | No | No | No | Somatostatin analogues | Unknown |
| Miguchi et al., 2012 [28] | Yes | No | No | N/A | No | Total gastrectomy | S-1 | No | Ongoing at 6 m follow up |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MiNEN | Mixed neuroendocrine–non-neuroendocrine neoplasm |
| EGJ | Esophagogastric junction |
| MDT | Multidisciplinary team |
| MANEC | Mixed adenoneuroendocrine carcinoma |
References
- Díaz-López, S.; Jiménez-Castro, J.; Robles-Barraza, C.E.; Ayala-de Miguel, C.; Chaves-Conde, M. Mixed neuroendocrine non-neuroendocrine neoplasms in gastroenteropancreatic tract. World J. Gastrointest. Oncol. 2024, 16, 1166–1179. [Google Scholar] [CrossRef] [PubMed]
- Cordier, R. Les Cellules argentaffines dans les tumeurs intestinales. Arch. Int. Med. 1924, 1, 59–63. [Google Scholar]
- La Rosa, S.; Sessa, F.; Uccella, S. Mixed Neuroendocrine-Nonneuroendocrine Neoplasms (MiNENs): Unifying the Concept of a Heterogeneous Group of Neoplasms. Endocr. Pathol. 2016, 27, 284–311. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; The WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Couvelard, A.; Cazes, A.; Cros, J. Updates in histopathological classification and tissue biomarkers of digestive neuroendocrine neoplasms: What the clinician should know. Best Pract. Res. Clin. Endocrinol. Metab. 2023, 37, 101795. [Google Scholar] [CrossRef] [PubMed]
- Scardoni, M.; Vittoria, E.; Volante, M.; Rusev, B.; Bersani, S.; Mafficini, A.; Gottardi, M.; Giandomenico, V.; Malleo, G.; Butturini, G.; et al. Mixed adenoneuroendocrine carcinomas of the gastrointestinal tract: Targeted next-generation sequencing suggests a monoclonal Origin of the Two Components. Neuroendocrinology 2014, 100, 310–316. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, S. Diagnostic, Prognostic, and Predictive Role of Ki67 Proliferative Index in Neuroendocrine and Endocrine Neoplasms: Past, Present, and Future. Endocr. Pathol. 2023, 34, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekar, V.T.; Hamade, N.; Desai, M.; Rai, T.; Gorrepati, V.S.; Jegadeesan, R.; Sathyamurthy, A.; Sharma, P. Significantly lower annual rates of neoplastic progression in short-compared to long-segment non-dysplastic Barrett’s esophagus: A systematic review and meta-analysis. Endoscopy 2019, 51, 665–672. [Google Scholar] [CrossRef]
- Siewert, J.R.; Stein, H.J. Classification of adenocarcinoma of the oesophagogastric junction. Br. J. Surg. 1998, 85, 1457–1459. [Google Scholar] [CrossRef]
- Daiko, H.; Kato, K. Updates in the 8th edition of the TNM staging system for esophagus and esophagogastric junction cancer. Jpn. J. Clin. Oncol. 2020, 50, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.H.; Goldner, W.S.; Benson, A.B.; Bergsland, E.; Blaszkowsky, L.S.; Brock, P.; Chan, J.; Das, S.; Dickson, P.V.; Fanta, P.; et al. Neuroendocrine and Adrenal Tumors, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 839–868. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.C.; Huang, C.W.; Karmakar, R.; Mukundan, A.; Chen, T.H.; Chou, C.K.; Yang, K.Y.; Wang, H.C. Precision Imaging for Early Detection of Esophageal Cancer. Bioengineering 2025, 12, 90. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Zhao, Y.; Zhou, Y.; Tian, Y.; He, Q.; Lin, J.; Hao, H.; Zou, B.; Jiang, L.; Zhao, G.; et al. Comparison of survival and patterns of recurrence in gastric euroendocrine carcinoma, mixed adenoneuroendocrine carcinoma, and adenocarcinoma. JAMA Netw. Open 2021, 4, e2114180. [Google Scholar] [CrossRef] [PubMed]
- Brathwaite, S.; Rock, J.; Yearsley, M.M.; Bekaii-Saab, T.; Wei, L.; Frankel, W.L.; Hays, J.; Wu, C.; Abdel-Misih, S. Mixed Adeno-neuroendocrine Carcinoma: An Aggressive Clinical Entity. Ann. Surg. Oncol. 2016, 23, 2281–2286. [Google Scholar] [CrossRef]
- Liu, L.; Li, Q.; Liu, W.; Qiu, Z.; Wu, Z.; Yu, D.; Deng, W. Gastric mixed neuroendocrine non-neuroendocrine neoplasms. Front. Oncol. 2024, 14, 1335760. [Google Scholar] [CrossRef]
- Chan, H.; Zhang, L.; Choti, M.A.; Kulke, M.; Yao, J.C.; Nakakura, E.K.; Bloomston, M.; Benson, A.B.; Shah, M.H.; Strosberg, J.R.; et al. Recurrence Patterns after Surgical Resection of Gastroenteropancreatic Neuroendocrine Tumors: Analysis from the National Comprehensive Cancer Network Oncology Outcomes Database. Pancreas 2021, 50, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Sun, L.; Ma, J. Favorable response to PD-1 inhibitor plus chemotherapy as first-line treatment for metastatic gastric mixed neuroendocrine-non-neuroendocrine tumor: A case report. Front. Pharmacol. 2024, 15, 1295134. [Google Scholar] [CrossRef] [PubMed]
- Woo, L.T.; Ding, Y.F.; Mao, C.Y.; Qian, J.; Zhang, X.M.; Xu, N. Long-term survival of gastric mixed neuroendocrine-non-neuroendocrine neoplasm: Two case reports. World J. Clin. Cases 2022, 10, 7936–7943. [Google Scholar] [CrossRef] [PubMed]
- Riccò, B.; Salati, M.; Reggiani Bonetti, L.; Dominici, M.; Luppi, G. PD-1 blockade in deficient mismatch repair mixed adenoneuroendocrine carcinoma of the stomach: New hope for an orphan disease. Tumori 2020, 106, NP57–NP62. [Google Scholar] [CrossRef]
- Lin, Z.; Chen, J.; Guo, Y. Efficacy of XELOX adjuvant chemotherapy for gastric mixed adenoneuroendocrine carcinoma: A case report. Medicine 2019, 98, e16000. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.; Zhou, Z.; Chen, J.; Di, M.; Ji, J.; Yuan, W.; Liu, Z.; Wu, L.; Zhang, X.; Li, K.; et al. Correlation of metastasis characteristics with prognosis in gastric mixed adenoneuroendocrine carcinoma: Two case reports. Medicine 2017, 96, e9189. [Google Scholar] [CrossRef]
- Kheiri, B.; Osman, M.; Congdon, D.; Bachuwa, G. A rare case of gastric mixed adenoneuroendocrine carcinoma (MANEC) with gastric Helicobacter pylori -negative mucosa-associated lymphoid tissue (MALT) lymphoma. BMJ Case Rep. 2017, 2017, bcr-2017. [Google Scholar] [CrossRef] [PubMed]
- Ambesh, P.; Weissbrot, J.; Ratner, S.; Sinha, A.; Patti, R.; Balderacchi, J.; Marcelin, M.; Wolf, L.; Kamholz, S. Mixed Adenoneuroendocrine Carcinoma of the Gastroesophageal Junction: A Rare Find. J. Investig. Med. High Impact Case Rep. 2017, 5, 2324709617750180. [Google Scholar] [CrossRef] [PubMed]
- Cazzo, E.; Saito, H.P.d.A.d. Adenocarcinoma neuroendócrino misto do coto gástrico após gastrectomia à Billroth II: Relato de caso e revisão de literatura. Sao Paulo Med. J. 2016, 134, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, J.; Shinozaki, K.; Baba, S.; Kurogi, J.; Nakane, T.; Kinoshita, Y.; Ishii, K.; Ueno, T.; Torimura, T.; Yano, H. A resected case of neuroendocrine carcinoma of the stomach with unusual lymph node metastasis. Med. Mol. Morphol. 2016, 49, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Gurzu, S.; Kadar, Z.; Bara, T.J.; Tamasi, A.; Azamfirei, L.; Jung, I. Mixed adenoneuroendocrine carcinoma of gastrointestinal tract: Report of two cases. World J. Gastroenterol. 2015, 21, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Levi Sandri, G.B.; Carboni, F.; Valle, M.; Visca, P.; Garofalo, A. Mixed adenoneuroendocrine gastric carcinoma: A case report and review of the literature. J. Gastric Cancer 2014, 14, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Miguchi, M.; Iseki, M.; Shimatani, K. Advanced gastric neuroendocrine carcinoma with an adenocarcinoma component. Case Rep. Gastroenterol. 2012, 6, 52–57. [Google Scholar] [CrossRef]
- Zhang, W.; Xiao, W.; Ma, H.; Sun, M.; Chen, H.; Zheng, S. Neuroendocrine Liver Metastasis in Gastric Mixed Adenoneuroendocrine Carcinoma with Trilineage Cell Differentiation: A Case Report. Int. J. Clin. Exp. Pathol. 2014, 7, 6333. [Google Scholar] [PubMed]
- Kroese, T.E.; Bronzwaer, S.; van Rossum, P.S.; Schoppman, S.F.; Deseyne, P.R.; van Cutsem, E.; Haustermans, K.; Nafteux, P.; Thomas, M.; Obermannova, R.; et al. European clinical practice guidelines for the definition, diagnosis, and treatment of oligometastatic esophagogastric cancer (OMEC-4). Eur. J. Cancer 2024, 20, 114062. [Google Scholar] [CrossRef] [PubMed]
- Pericleous, M.; Toumpanakis, C.; Lumgair, H.; Caplin, M.E.; Morgan-Rowe, L.; Clark, I.; Luong, T.V. Gastric mixed adenoneuroendocrine carcinoma with a trilineage cell differentiation: Case report and review of the literature. Case Rep. Oncol. 2012, 5, 313–319. [Google Scholar] [CrossRef]
- Deliwala, S.S.; Ponnapalli, A.; Gakhal, I.; Modi, V.; Haykal, T.; Bachuwa, G.; Chawla, S. When Variants Collide: An Unusual Presentation of Metastatic Gastric Mixed Neuroendocrine-Non-Neuroendocrine Neoplasm. ACG Case Rep. J. 2021, 8, e00569. [Google Scholar] [CrossRef] [PubMed]
- Millet, C.; Farokhian, A.; Mekheal, N.; Singh, B.; Baddoura, W. Massive Mixed Adenoneuroendocrine Carcinoma: A Case Report. Cureus 2021, 13, e15928. [Google Scholar] [CrossRef] [PubMed]
- Golombek, T.; Henker, R.; Rehak, M.; Quäschling, U.; Lordick, F.; Knödler, M. A Rare Case of Mixed Adenoneuroendocrine Carcinoma (MANEC) of the Gastroesophageal Junction with HER2/neu Overexpression and Distinct Orbital and Optic Nerve Toxicity after Intravenous Administration of Cisplatin. Oncol. Res. Treat. 2019, 42, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Pham, Q.D.; Mori, I.; Osamura, R.Y. A Case Report: Gastric Mixed Neuroendocrine-Nonneuroendocrine Neoplasm with Aggressive Neuroendocrine Component. Case Rep. Pathol. 2017, 201, 9871687. [Google Scholar] [CrossRef]
- Yoon, S.E.; Kim, J.H.; Lee, S.J.; Lee, J.; Park, S.H.; Park, J.O.; Lim, H.Y.; Kang, W.K.; Park, Y.S.; Kim, S.T. The impact of primary tumor site on outcomes of treatment with etoposide and cisplatin in grade 3 gastroenteropancreatic neuroendocrine carcinoma. J. Cancer 2019, 10, 3140–3144. [Google Scholar] [CrossRef] [PubMed]
- Morizane, C.; Machida, N.; Honma, Y.; Okusaka, T.; Boku, N.; Kato, K.; Nomura, S.; Hiraoka, N.; Sekine, S.; Taniguchi, H.; et al. Effectiveness of Etoposide and Cisplatin vs Irinotecan and Cisplatin Therapy for Patients with Advanced Neuroendocrine Carcinoma of the Digestive System: The TOPIC-NEC Phase 3 Randomized Clinical Trial. JAMA Oncol. 2022, 8, 1447–1455. [Google Scholar] [CrossRef]
- Jepsen, D.N.M.; Fiehn, A.-M.K.; Garbyal, R.S.; Engel, U.; Holm, J.; Federspiel, B. Immunohistochemical Staining With Neuroendocrine Markers is Essential in the Diagnosis of Neuroendocrine Neoplasms of the Esophagogastric Junction. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 454–461. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sotiropoulou, A.; Avgoustidou, M.; Milionis, V.; Papadimitriou, I.; Vergadis, C.; Schizas, D.; Arkadopoulos, N.; Lyros, O. Oligometastatic Mixed Neuroendocrine Adenocarcinoma of the Esophago-Gastric Junction: A Case of Successful Multidisciplinary Management, the Lessons Learnt and Review of the Literature. J. Clin. Med. 2025, 14, 1503. https://doi.org/10.3390/jcm14051503
Sotiropoulou A, Avgoustidou M, Milionis V, Papadimitriou I, Vergadis C, Schizas D, Arkadopoulos N, Lyros O. Oligometastatic Mixed Neuroendocrine Adenocarcinoma of the Esophago-Gastric Junction: A Case of Successful Multidisciplinary Management, the Lessons Learnt and Review of the Literature. Journal of Clinical Medicine. 2025; 14(5):1503. https://doi.org/10.3390/jcm14051503
Chicago/Turabian StyleSotiropoulou, Anastasia, Maria Avgoustidou, Vassilis Milionis, Ioannis Papadimitriou, Chrysovalantis Vergadis, Dimitrios Schizas, Nikolaos Arkadopoulos, and Orestis Lyros. 2025. "Oligometastatic Mixed Neuroendocrine Adenocarcinoma of the Esophago-Gastric Junction: A Case of Successful Multidisciplinary Management, the Lessons Learnt and Review of the Literature" Journal of Clinical Medicine 14, no. 5: 1503. https://doi.org/10.3390/jcm14051503
APA StyleSotiropoulou, A., Avgoustidou, M., Milionis, V., Papadimitriou, I., Vergadis, C., Schizas, D., Arkadopoulos, N., & Lyros, O. (2025). Oligometastatic Mixed Neuroendocrine Adenocarcinoma of the Esophago-Gastric Junction: A Case of Successful Multidisciplinary Management, the Lessons Learnt and Review of the Literature. Journal of Clinical Medicine, 14(5), 1503. https://doi.org/10.3390/jcm14051503