
Bone Densitometry Parameters in Females with Ehlers-Danlos Syndrome—Does the Hypermobile Subtype Increase the Risk of Low Bone Mass in Patients with Ehlers-Danlos Syndrome?


 , , , ,
, , , ,
Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scicluna, K.; Formosa, M.M.; Farrugia, R.; Borg, I. Hypermobile Ehlers-Danlos syndrome: A review and a critical appraisal of published genetic research to date. Clin. Genet. 2022, 101, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Concolino, P.; Falhammar, H. CAH-X Syndrome: Genetic and Clinical Profile. Mol. Diagn. Ther. 2022, 26, 293–300. [Google Scholar] [CrossRef]
- Coussens, M.; Banica, T.; Lapauw, B.; De Wandele, I.; Rombaut, L.; Malfait, F.; Calders, P. Bone parameters in hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorder: A comparative cross-sectional study. Bone 2023, 166, 116583. [Google Scholar] [CrossRef]
- Available online: https://www.orpha.net/ (accessed on 14 September 2024).
- Demmler, J.C.; Atkinson, M.D.; Reinhold, E.J.; Choy, E.; Lyons, R.A.; Brophy, S.T. Diagnosed prevalence of Ehlers-Danlos syndrome and hypermobility spectrum disorder in Wales, UK: A national electronic cohort study and case-control comparison. BMJ Open 2019, 9, e031365. [Google Scholar] [CrossRef] [PubMed]
- Gensemer, C.; Burks, R.; Kautz, S.; Judge, D.P.; Lavallee, M.; Norris, R.A. Hypermobile Ehlers-Danlos syndromes: Complex phenotypes, challenging diagnoses, and poorly understood causes. Dev. Dyn. 2021, 250, 318–344. [Google Scholar] [CrossRef]
- Tinkle, B.; Castori, M.; Berglund, B.; Cohen, H.; Grahame, R.; Kazkaz, H. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome type III and Ehlers-Danlos syndrome hypermobility type): Clinical description and natural history. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 48–69. [Google Scholar] [CrossRef] [PubMed]
- Fukada, T.; Civic, N.; Furuichi, T.; Shimoda, S.; Mishima, K.; Higashiyama, H.; Idaira, Y.; Asada, Y.; Kitamura, H.; Yamasaki, S.; et al. The zinc transporter SLC39A13/ZIP13 is required for connective tissue development; its involvement in BMP/TGF-beta signaling pathways. PLoS ONE 2008, 3, e3642. [Google Scholar] [CrossRef]
- Galli, G.G.; Honnens de Lichtenberg, K.; Carrara, M.; Hans, W.; Wuelling, M.; Mentz, B.; Multhaupt, H.A.; Fog, C.K.; Jensen, K.T.; Rappsilber, J.; et al. Prdm5 regulates collagen gene transcription by association with RNA polymerase II in developing bone. PLoS Genet. 2012, 8, e1002711. [Google Scholar] [CrossRef]
- Nielsen, R.H.; Couppé, C.; Jensen, J.K.; Olsen, M.R.; Heinemeier, K.M.; Malfait, F.; Symoens, S.; De Paepe, A.; Schjerling, P.; Magnusson, S.P.; et al. Low tendon stiffness and abnormal ultrastructure distinguish classic Ehlers-Danlos syndrome from benign joint hypermobility syndrome in patients. FASEB J. 2014, 28, 4668–4676. [Google Scholar] [CrossRef] [PubMed]
- Rombaut, L.; Malfait, F.; De Wandele, I.; Mahieu, N.; Thijs, Y.; Segers, P.; De Paepe, A.; Calders, P. Muscle-tendon tissue properties in the hypermobility type of Ehlers-Danlos syndrome. Arthritis Care Res. 2012, 64, 766–772. [Google Scholar] [CrossRef]
- Mazziotti, G.; Dordoni, C.; Doga, M.; Galderisi, F.; Venturini, M.; Calzavara-Pinton, P.; Maroldi, R.; Giustina, A.; Colombi, M. High prevalence of radiological vertebral fractures in adult patients with Ehlers-Danlos syndrome. Bone 2016, 84, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Dolan, A.L.; Arden, N.K.; Grahame, R.; Spector, T.D. Assessment of bone in Ehlers Danlos syndrome by ultrasound and densitometry. Ann. Rheum. Dis. 1998, 57, 630–633. [Google Scholar] [CrossRef]
- Eller-Vainicher, C.; Bassotti, A.; Imeraj, A.; Cairoli, E.; Ulivieri, F.M.; Cortini, F.; Dubini, M.; Marinelli, B.; Spada, A.; Chiodini, I. Bone involvement in adult patients affected with Ehlers-Danlos syndrome. Osteoporos. Int. 2016, 27, 2525–2531. [Google Scholar] [CrossRef] [PubMed]
- Yew, K.S.; Kamps-Schmitt, K.A.; Borge, R. Hypermobile Ehlers-Danlos syndrome and Hypermobility Spectrum Disorders. Am. Fam. Physician 2021, 103, 481–492. [Google Scholar]
- Available online: www.ehlers-danlos.com/wp-content/uploads/hEDS-Dx-Criteria-checklist-1.pdf (accessed on 15 September 2024).
- Available online: https://m.facebook.com/StowarzyszenieEhlersDanlosPolska/ (accessed on 15 September 2024).
- Carbone, L.; Tylavsky, F.A.; Bush, A.J.; Koo, W.; Orwoll, E.; Cheng, S. Bone density in Ehlers-Danlos syndrome. Osteoporos. Int. 2000, 11, 388–392. [Google Scholar] [CrossRef]
- Banica, T.; Coussens, M.; Verroken, C.; Calders, P.; de Wandele, I.; Malfait, F. Higher fracture prevalence and smaller bone size in patients with hEDS/HSD-a-prospective cohort study. Osteoporos. Int. 2020, 31, 849–856. [Google Scholar] [CrossRef]
- Basalom, S.; Rauch, F. Bone Disease in Patients with Ehlers-Danlos Syndromes. Curr. Osteoporos. Rep. 2020, 18, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Yue, F.; Era, T.; Yamaguchi, T.; Kosho, T. Pathophysiological Investigation of Skeletal Deformities of Musculocontractural Ehlers-Danlos Syndrome Using Induced Pluripotent Stem Cells. Genes 2023, 14, 730. [Google Scholar] [CrossRef]
- Love, A.N.; Palmer, B. Presentation and Management of a Novel Ehlers-Danlos COL5A1 Variant With Birt-Hogg-Dube Syndrome: A Case Study. Cureus 2023, 15, e35866. [Google Scholar] [CrossRef] [PubMed]
- Scheper, M.C.; Nicholson, L.L.; Adams, R.D.; Tofts, L.; Pacey, V. The natural history of children with joint hypermobility syndrome and Ehlers-Danlos hypermobility type: A longitudinal cohort study. Rheumatology 2017, 56, 2073–2083. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, J.V.; Herbland, A.; Hakim, A.; Ninis, N.; Lever, W.; Aziz, Q.; Cairins, M. Exercise beliefs and behaviours of individuals with joint hypermobility syndrome/Ehlers-Danlose syndrome—Hypermobility type. Disabil. Rehabil. 2019, 41, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Robbins, S.M.; Cossette-Levasseur, M.; Kikuchi, K.; Sarjeant, J.; Shiu, Y.G.; Azar, C.; Hazel, E.M. Neuromuscular activation differences during gait in patients with Ehlers-Danlos syndrome and healthy adults. Arthritis Care Res. 2020, 72, 1653–1662. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, R.H.; Jensen, J.K.; Voermans, N.C.; Heinemeier, K.M.; Schjerling, P.; Holm, L.; Agergaard, J.; Mackey, A.L.; Andersen, J.L.; Remvig, L.; et al. Skeletal muscle morphology, protein synthesis, and gene expression in Ehlers-Danlose syndrome. J. Appl. Physiol. 2017, 123, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Stern, C.M.; Pepin, M.J.; Stoler, J.M.; Kramer, D.E.; Spencer, S.A.; Stein, C.J. Musculoskeletal conditions in a pediatric population with Ehlers-Danlos syndrome. J. Pediatr. 2017, 181, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Chopra, P.; Tinkle, B.; Hamonet, C.; Brock, I.; Gompel, A.; Bulbena, A.; Francomano, C. Pain management in the Ehlers-Danlos syndromes. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175, 212–219. [Google Scholar] [CrossRef]
- Ericson, W.B.; Wolman, R. Orthopaedic management of the Ehlers-Danlos syndromes. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175, 188–194. [Google Scholar] [CrossRef] [PubMed]
- McKeon, K.E.; London, D.A.; Osei, D.A.; Gelberman, R.H.; Goldfarb, C.h.A.; Boyer, M.I.; Calfee, R.P. Ligamentous hyperlaxity and dorsal wrist ganglions. J. Hand Surg. Am. 2013, 38, 2138–2143. [Google Scholar] [CrossRef] [PubMed]
- Castori, M.; Camerota, F.; Celletti, C.; Danese Ch Santilli, V.; Saraceni, V.M.; Grammatico, P. Natural history and manifestations of the hypermobility type Ehlers-Danlos syndrome: A pilot study on 21 patients. Am. J. Med. Genet. Part A 2010, 152A, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Malfait, F.; Francomano, C.; Byers, P.; Francomano, C.; Tinkle, B.; Malfait, F. The 2017 international classification of the Ehlers-Danlos syndromes. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175, 8–26. [Google Scholar] [CrossRef] [PubMed]
- Hakim, A.J.; Grahame, R. A simple questionnaire to detect hypermobility: An adjunct to the assessment of patients with diffuse musculoskeletal pain. Int. J. Clin. Pract. 2003, 57, 163–166. [Google Scholar] [CrossRef] [PubMed]
- De Wandele, I.; Rombaut, L.; Malfait, F.; De Backer, T.; De Paepe, A.; Calders, P. Clinical heterogeneity in patients with the hypermobility type of Ehlers-Danlos syndrome. Res. Dev. Disabil. 2013, 34, 873–881. [Google Scholar] [CrossRef] [PubMed]
- McGillis, L.; Mittal, N.; Mina, D.S.; So, J.; Soowamber, M.; Weinrib, A.; Soever, L.; Rozenberg, D.; Liu, L.; Tse, Y.; et al. Utilization of the 2017 diagnostic criteria for hEDS by the Toronto GoodHope Ehlers-Danlos syndrome clinic: A retrospective review. Am. J. Med. Genet. Part A 2020, 182, 484–492. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Group 1 (N = 9) | Group 2 (N = 21) | Significance of the Difference (p-Value) |
|---|---|---|---|
| Left femur neck BMD [g/cm2] | 0.919 ± 0.133 | 0.947 ± 0.118 | 0.824 |
| Left femur neck age-matched BMD [%] | 92.875 ± 13.432 | 94 ± 11.369 | 0.979 |
| Left femur upper neck BMD [g/cm2] | 0.75 ± 0.2 | 0.814 ± 0.144 | 0.572 |
| Left femur upper neck age-matched BMD [%] | 92.333 ± 24.799 | 99.476 ± 17.394 | 0.734 |
| Left femur lower neck BMD [g/cm2] | 1.066 ± 0.139 | 1.075 ± 0.127 | 0.928 |
| Left femur Ward’s triangle BMD [g/cm2] | 0.781 ± 0.119 | 0.795 ± 0.148 | 0.751 |
| Left femur Ward’s triangle age-matched BMD [%] | 88.111 ± 10.925 | 88.286 ± 15.153 | 0.964 |
| Left femur trochanter BMD [g/cm2] | 0.726 ± 0.126 | 0.725 ± 0.125 | 0.982 |
| Left femur trochanter age-matched BMD [%] | 86.222 ± 12.143 | 85.333 ± 12.055 | 0.803 |
| Left femur shaft BMD [g/cm2] | 1.146 ± 0.138 | 12.055 ± 0.167 | 0.635 |
| Left femur total BMD [g/cm2] | 0.956 ± 0.122 | 0.948 ± 0.136 | 0.965 |
| Left femur total age-matched BMD [%] | 95.333 ± 9.152 | 95.048 ± 12.002 | 0.909 |
| L1–L4 BMD [g/cm2] | 1.218 ± 0.212 | 1.261 ± 0.181 | 0.476 |
| L1–L4 age-matched BMD [%] | 101.333 ± 14.361 | 104.1 ± 10.004 | 0.570 |
| L1 BMD [g/cm2] | 1.121 ± 0.176 | 1.189 ± 0.218 | 0.469 |
| L1 age-matched BMD [%] | 97.444 ± 12.4 | 101.55 ± 10.928 | 0.369 |
| L2 BMD [g/cm2] | 1.199 ± 0.252 | 1.262 ± 0.175 | 0.222 |
| L3 age-matched BMD [%] | 98 ± 16.256 | 103 ± 11.272 | 0.257 |
| L3 BMD [g/cm2] | 1.261 ± 0.233 | 1.324 ± 0.184 | 0.175 |
| L3 age-matched BMD [%] | 103.111 ± 15.004 | 107.45 ± 9.506 | 0.310 |
| L4 BMD [g/cm2] | 1.262 ± 0.233 | 1.259 ± 0.181 | 0.928 |
| L4 age-matched BMD [%] | 103.667 ± 17.493 | 102.45 ± 10.899 | 0.887 |
| L1–L2 BMD [g/cm2] | 1.162 ± 0.212 | 1.227 ± 0.189 | 0.319 |
| L1–L2 age-matched BMD [%] | 97.778 ± 14.087 | 102.5 ± 11.009 | 0.408 |
| L1–L3 BMD [g/cm2] | 1.197 ± 0.217 | 1.262 ± 0.186 | 0.205 |
| L1–L3 age-matched BMD [%] | 100.444 ± 14.293 | 105 ± 10.126 | 0.321 |
| L2–L3 BMD [g/cm2] | 1.232 ± 0.239 | 1.294 ± 0.176 | 0.124 |
| L2–L3 age-matched BMD [%] | 100.778 ± 15.352 | 105.35 ± 9.99 | 0.228 |
| L2–L4 BMD [g/cm2] | 1.245 ± 0.228 | 1.28 ± 0.175 | 0.469 |
| L2–L4 age-matched BMD [%] | 101.889 ± 15.536 | 104.25 ± 10.02 | 0.637 |
| L3–L4 BMD [g/cm2] | 1.263 ± 0.225 | 1.289 ± 0.18 | 0.556 |
| L3–L4 age-matched BMD [%] | 103.667 ± 15.716 | 104.65 ± 9.832 | 0.869 |
| Characteristics | Group 1 (N = 9) | Group 2 (N = 21) | Significance of the Difference (p-Value) |
|---|---|---|---|
| Age [years] | 39.8 ± 8.3 | 33.5 ± 9.0 | 0.045 |
| Body weight [kg] | 74 ± 20.3 | 68 ± 17.4 | 0.283 |
| BMI [kg/m2] | 26.7 ± 6.6 | 25.3 ± 6.6 | 0.348 |
| Total calcium [mmol/L] | 2.403 ± 0.106 | 2.399 ± 0.074 | 0.756 |
| Inorganic phosphate [mg/dL] | 3.642 ± 0.958 | 3.406 ± 0.443 | 0.449 |
| PTH [pg/mL] | 50.522 ± 16.4 | 39.552 ± 13.679 | 0.064 |
| 25-OH vitamin D [ng/mL] | 22.489 ± 10.144 | 34.076 ± 18.011 | 0.022 |
| Alkaline phosphatase [µg/L] | 10.7 ± 2.46 | 9.029 ± 2.672 | 0.077 |
| CTx [ng/mL] | 0.379 ± 0.209 | 0.395 ± 0.181 | 0.789 |
| Osteocalcin [ng/mL] | 19.4 ± 7.191 | 21.081 ± 7.597 | 0.449 |
| Sodium [mmol/L] | 140.889 ± 2.759 | 141.619 ± 2.085 | 0.563 |
| Potassium [mmol/L] | 4.766 ± 0.301 | 4.599 ± 0.403 | 0.193 |
| TSH [µIU/mL] | 1.946 ± 0.975 | 2.187 ± 1.526 | 0.929 |
| DHEA-S [µg/dL] | 194.278 ± 85.494 | 217.086 ± 103.734 | 0.624 |
| Cortisol [µg/dL] | 14.756 ± 4.231 | 15.243 ± 6.63 | 0.859 |
| History of fractures | 4 (44.44%) | 13 (61.905%) | 0.476 |
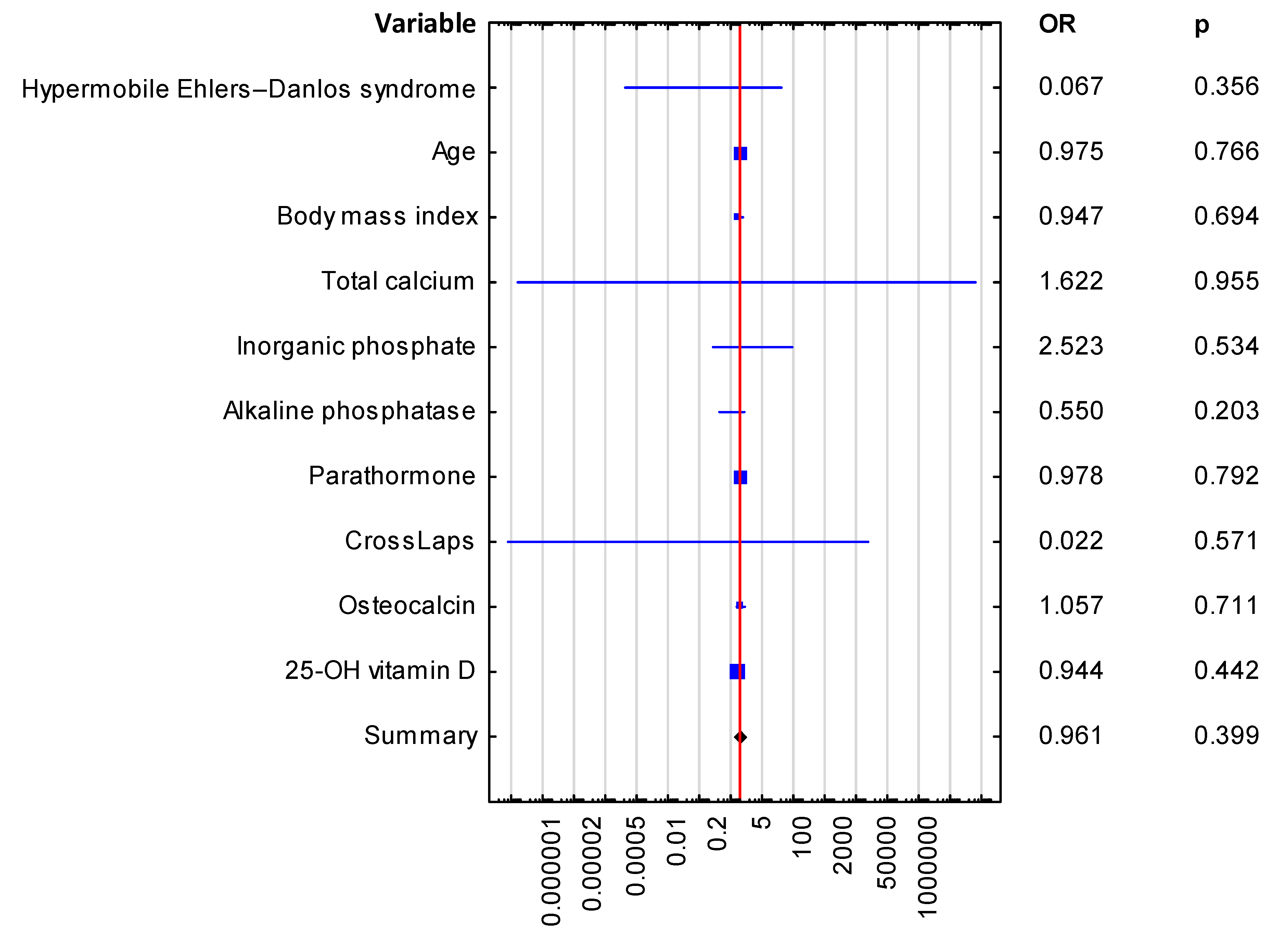
| Variable | Odds Ratio, OR (95% Cl) | Significance of the Difference (p-Value) |
|---|---|---|
| Hypermobile Ehlers-Danlos syndrome | 0.067 (0.0–20.927) | 0.356 |
| Age | 0.975 (0.823–1.155) | 0.766 |
| Body mass index | 0.947 (0.724–1.24) | 0.694 |
| Total calcium | 1.622 (0.0–32,902,246.74) | 0.955 |
| Inorganic phosphate | 2.523 (0.137–46.529) | 0.534 |
| Alkaline phosphatase | 0.550 (0.219–1.38) | 0.203 |
| Parathormone | 0.978 (0.828–1.155) | 0.792 |
| CrossLaps (CTx) | 0.022 (0.0–12,177.508) | 0.571 |
| Osteocalcin | 1.057 (0.789–1.417) | 0.711 |
| 25-OH vitamin D | 0.944 (0.816–1.093) | 0.442 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kałuża, B.; Rychlik, I.; Domański, J.; Żuk-Łapan, A.; Babula, E.; Poprawa, I.; Podstawka, J.; Kowalów, E.; Franek, E. Bone Densitometry Parameters in Females with Ehlers-Danlos Syndrome—Does the Hypermobile Subtype Increase the Risk of Low Bone Mass in Patients with Ehlers-Danlos Syndrome? J. Clin. Med. 2025, 14, 941. https://doi.org/10.3390/jcm14030941
Kałuża B, Rychlik I, Domański J, Żuk-Łapan A, Babula E, Poprawa I, Podstawka J, Kowalów E, Franek E. Bone Densitometry Parameters in Females with Ehlers-Danlos Syndrome—Does the Hypermobile Subtype Increase the Risk of Low Bone Mass in Patients with Ehlers-Danlos Syndrome? Journal of Clinical Medicine. 2025; 14(3):941. https://doi.org/10.3390/jcm14030941
Chicago/Turabian StyleKałuża, Bernadetta, Ivan Rychlik, Jan Domański, Aleksandra Żuk-Łapan, Emilia Babula, Iga Poprawa, Jakub Podstawka, Ewa Kowalów, and Edward Franek. 2025. "Bone Densitometry Parameters in Females with Ehlers-Danlos Syndrome—Does the Hypermobile Subtype Increase the Risk of Low Bone Mass in Patients with Ehlers-Danlos Syndrome?" Journal of Clinical Medicine 14, no. 3: 941. https://doi.org/10.3390/jcm14030941
APA StyleKałuża, B., Rychlik, I., Domański, J., Żuk-Łapan, A., Babula, E., Poprawa, I., Podstawka, J., Kowalów, E., & Franek, E. (2025). Bone Densitometry Parameters in Females with Ehlers-Danlos Syndrome—Does the Hypermobile Subtype Increase the Risk of Low Bone Mass in Patients with Ehlers-Danlos Syndrome? Journal of Clinical Medicine, 14(3), 941. https://doi.org/10.3390/jcm14030941