
Evaluation of Prospective ECG-Triggered CT Scan as a Practical Alternative to Standard Retrospective ECG-Gated Scan for Pre-TAVI Patients

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Scanning Protocols and Patient Selection
2.2.1. CT Data Acquisition and Analysis
2.2.2. Selection of Scanning Protocol
2.3. CT Post-Processing
2.4. TAVI Procedure
2.5. Echocardiography
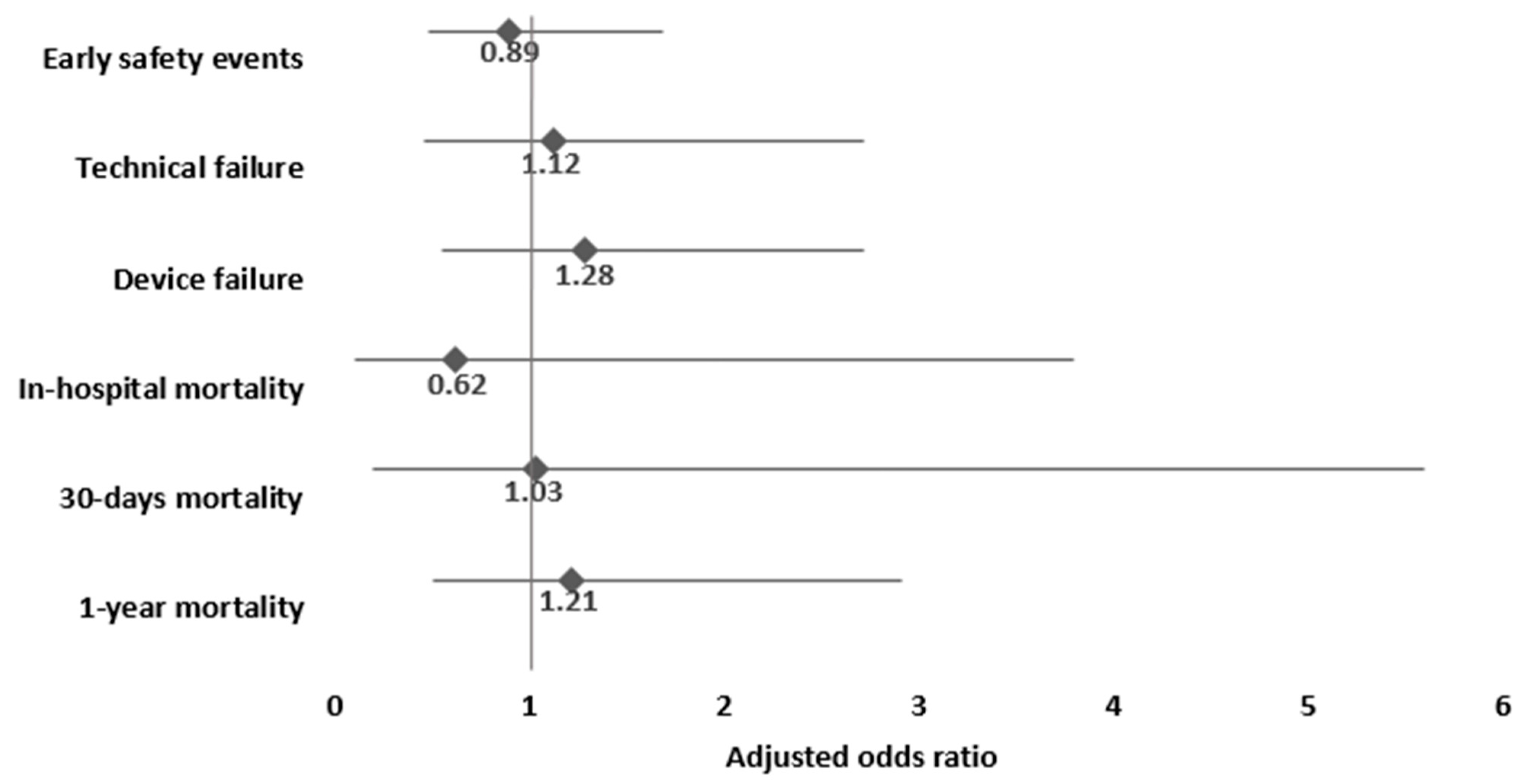
2.6. Study Outcomes
- Composite Valve Academic Research Consortium3 (VARC-3) endpoints for technical failure, device failure, and early safety events [27]. [See the Supplementary Materials (S4) for a detailed description of the elements comprising the composite outcomes.]
- In hospital, 30-day, and 1-year mortality.
- Paravalvular leak (PVL)—defined as more then mild PVL.
- Safety parameters—need for a second valve, valve malposition, in-hospital stroke/transient ischemic attack (TIA), acute kidney injury (AKI) (VARC-3, stage 1–3), major vascular complications (VARC-3), new post-procedural complete atrioventricular (AV) block, and new permanent pacemaker implantation.
2.7. Statistical Analysis
3. Propensity Score Matching
4. Results
4.1. Patient Characteristics
4.2. CT and Procedural Data
4.3. Mortality
4.4. Procedural and Technical Outcome
4.5. Clinical Safety Outcomes
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Blanke, P.; Weir-McCall, J.R.; Achenbach, S.; Delgado, V.; Hausleiter, J.; Jilaihawi, H.; Marwan, M.; Nørgaard, B.L.; Piazza, N.; Schoenhagen, P.; et al. Computed Tomography Imaging in the Context of Transcatheter Aortic Valve Implantation (TAVI)/Transcatheter Aortic Valve Replacement (TAVR). JACC Cardiovasc. Imaging 2019, 12, 1–24. [Google Scholar] [CrossRef]
- Schuppert, C.; Salatzki, J.; André, F.; Riffel, J.; Mangold, D.L.; Melzig, C.; Hagar, M.T.; Kauczor, H.-U.; Weber, T.F.; Rengier, F.; et al. Feasibility of Reduced Iodine Loads for Vascular Assessment Prior to Transcatheter Aortic Valve Implantation (TAVI) Using Spectral Detector CT. Diagnostics 2024, 14, 879. [Google Scholar] [CrossRef]
- Almeida, J.G.; Ferreira, S.M.; Fonseca, P.; Dias, T.; Guerreiro, C.; Barbosa, A.R.; Teixeira, P.; Carvalho, M.; Ferreira, W.; Ferreira, N.D.; et al. Association between implantation depth assessed by computed tomography and new-onset conduction disturbances after transcatheter aortic valve implantation. J. Cardiovasc. Comput. Tomogr. 2017, 11, 332–337. [Google Scholar] [CrossRef]
- Sinning, J.M.; Hammerstingl, C.; Vasa-Nicotera, M.; Adenauer, V.; Lema Cachiguango, S.J.; Scheer, A.C.; Hausen, S.; Sedaghat, A.; Ghanem, A.; Müller, C.; et al. Aortic Regurgitation Index Defines Severity of Peri-Prosthetic Regurgitation and Predicts Outcome in Patients After Transcatheter Aortic Valve Implantation. J. Am. Coll. Cardiol. 2012, 59, 1134–1141. [Google Scholar] [CrossRef]
- Blanke, P.; Reinöhl, J.; Schlensak, C.; Siepe, M.; Pache, G.; Euringer, W.; Geibel-Zehender, A.; Bode, C.; Langer, M.; Beyersdorf, F.; et al. Prosthesis Oversizing in Balloon-Expandable Transcatheter Aortic Valve Implantation Is Associated with Contained Rupture of the Aortic Root. Circ. Cardiovasc. Interv. 2012, 5, 540–548. [Google Scholar] [CrossRef]
- Kazui, T.; Izumoto, H.; Yoshioka, K.; Kawazoe, K. Dynamic morphologic changes in the normal aortic annulus during systole and diastole. J. Heart Valve Dis. 2006, 15, 617–621. [Google Scholar] [PubMed]
- Blanke, P.; Russe, M.; Leipsic, J.; Reinöhl, J.; Ebersberger, U.; Suranyi, P.; Siepe, M.; Pache, G.; Langer, M.; Schoepf, U.J.; et al. Conformational Pulsatile Changes of the Aortic Annulus. JACC Cardiovasc. Interv. 2012, 5, 984–994. [Google Scholar] [CrossRef] [PubMed]
- Jochheim, D.; Schneider, V.S.; Schwarz, F.; Kupatt, C.; Lange, P.; Reiser, M.; Massberg, S.; Gutiérrez-Chico, J.-L.; Mehilli, J.; Becker, H.-C.; et al. Contrast-induced acute kidney injury after computed tomography prior to transcatheter aortic valve implantation. Clin. Radiol. 2014, 69, 1034–1038. [Google Scholar] [CrossRef]
- Van Linden, A.; Kempfert, J.; Rastan, A.J.; Holzhey, D.; Blumenstein, J.; Schuler, G.; Mohr, F.W.; Walther, T. Risk of acute kidney injury after minimally invasive transapical aortic valve implantation in 270 patients. Eur. J. Cardiothorac. Surg. 2011, 39, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Hayashida, K.; Mouillet, G.; Hovasse, T.; Chevalier, B.; Oguri, A.; Watanabe, Y.; Dubois-Randé, J.-L.; Morice, M.-C.; Lefèvre, T.; et al. Prognostic Value of Chronic Kidney Disease After Transcatheter Aortic Valve Implantation. J. Am. Coll. Cardiol. 2013, 62, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Scherner, M.; Wahlers, T. Acute kidney injury after transcatheter aortic valve implantation. J. Thorac. Dis. 2015, 7, 1527–1535. [Google Scholar]
- Shuai, T.; Li, W.; You, Y.; Deng, L.; Li, J.; Peng, L.; Li, Z. Combined Coronary CT Angiography and Evaluation of Access Vessels for TAVR Patients in Free-Breathing with Single Contrast Medium Injection Using a 16-cm-Wide Detector CT. Acad. Radiol. 2021, 28, 1662–1668. [Google Scholar] [CrossRef]
- Cour, A.; Burel, J.; Garnier, M.; Durand, E.; Demeyere, M.; Dacher, J.N. CT annulus sizing prior to transcatheter aortic valve replacement (TAVR): Evaluation of free-breathing versus breath-holding acquisition. Eur. Radiol. 2023, 33, 8521–8527. [Google Scholar] [CrossRef]
- Tops, L.F.; Wood, D.A.; Delgado, V.; Schuijf, J.D.; Mayo, J.R.; Pasupati, S.; Lamers, F.P.; van der Wall, E.E.; Schalij, M.J.; Webb, J.G.; et al. Noninvasive Evaluation of the Aortic Root with Multislice Computed Tomography. JACC Cardiovasc. Imaging 2008, 1, 321–330. [Google Scholar] [CrossRef]
- Plank, F.; Friedrich, G.; Bartel, T.; Mueller, S.; Bonaros, N.; Heinz, A.; Klauser, A.; Cartes-Zumelzu, F.; Grimm, M.; Feuchtner, G.; et al. Benefits of High-Pitch 128-Slice Dual-Source Computed Tomography for Planning of Transcatheter Aortic Valve Implantation. Ann. Thorac. Surg. 2012, 94, 1961–1966. [Google Scholar] [CrossRef]
- Bittner, D.O.; Arnold, M.; Klinghammer, L.; Schuhbaeck, A.; Hell, M.M.; Muschiol, G.; Gauss, S.; Lell, M.; Uder, M.; Hoffmann, U.; et al. Contrast volume reduction using third generation dual source computed tomography for the evaluation of patients prior to transcatheter aortic valve implantation. Eur. Radiol. 2016, 26, 4497–4504. [Google Scholar] [CrossRef]
- Schicchi, N.; Fogante, M.; Pirani, P.E.; Agliata, G.; Piva, T.; Tagliati, C.; Marcucci, M.; Francioso, A.; Giovagnoni, A. Third generation dual source CT with ultra-high pitch protocol for TAVI planning and coronary tree assessment: Feasibility, image quality and diagnostic performance. Eur. J. Radiol. 2020, 122, 108749. [Google Scholar] [CrossRef]
- Bischoff, B.; Meinel, F.G.; Del Prete, A.; Reiser, M.F.; Becker, H.C. High-pitch coronary CT angiography in dual-source CT during free breathing vs. breath holding in patients with low heart rates. Eur. J. Radiol. 2013, 82, 2217–2221. [Google Scholar] [CrossRef]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F.; Otto, C.M. Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 254–275. [Google Scholar] [CrossRef] [PubMed]
- Fogante, M.; Esposto Pirani, P.; Cela, F.; Balardi, L.; Piva, T.; Argalia, G.; Schicchi, N. Ultra-low radiation dose and contrast volume CT protocol and TAVI-CT score for TAVI planning and outcome. Br. J. Radiol. 2023, 96, 20221026. [Google Scholar] [CrossRef] [PubMed]
- Hagar, M.T.; Kluemper, T.; Hein, M.; Muhlen, C.v.Z.; Faby, S.; Capilli, F.; Schmitt, R.; Ruile, P.; Westermann, D.; Schlett, C.L.; et al. Photon-counting CT-angiography in pre-TAVR aortic annulus assessment: Effects of retrospective vs. prospective ECG-synchronization on prosthesis valve selection. Int. J. Cardiovasc. Imaging 2024, 40, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Landes, U.; Barsheshet, A.; Finkelstein, A.; Guetta, V.; Assali, A.; Halkin, A.; Vaknin-Assa, H.; Segev, A.; Bental, T.; Ben-Shoshan, J.; et al. Temporal trends in transcatheter aortic valve implantation, 2008-2014: Patient characteristics, procedural issues, and clinical outcome: Temporal trends in TAVI: 2008–2014. Clin. Cardiol. 2017, 40, 82–88. [Google Scholar] [CrossRef]
- Finkelstein, A.; Steinvil, A.; Rozenbaum, Z.; Halkin, A.; Banai, S.; Barbash, I.; Guetta, V.; Segev, A.; Danenberg, H.; Orvin, K.; et al. Efficacy and safety of new-generation transcatheter aortic valves: Insights from the Israeli transcatheter aortic valve replacement registry. Clin. Res. Cardiol. 2019, 108, 430–437. [Google Scholar] [CrossRef]
- Barbash, I.M.; Finkelstein, A.; Barsheshet, A.; Segev, A.; Steinvil, A.; Assali, A.; Ben Gal, Y.; Assa, H.V.; Fefer, P.; Sagie, A.; et al. Outcomes of Patients at Estimated Low, Intermediate, and High Risk Undergoing Transcatheter Aortic Valve Implantation for Aortic Stenosis. Am. J. Cardiol. 2015, 116, 1916–1922. [Google Scholar] [CrossRef]
- VARC-3 WRITING COMMITTEE.; Généreux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; A Leipsic, J.; Blanke, P.; et al. Valve Academic Research Consortium 3: Updated endpoint definitions for aortic valve clinical research. Eur. Heart J. 2021, 42, 1825–1857. [Google Scholar] [CrossRef]
- Martin, G.P.; Sperrin, M.; Hulme, W.; Ludman, P.F.; de Belder, M.A.; Toff, W.D.; Alabas, O.; Moat, N.E.; Doshi, S.N.; Buchan, I.; et al. Relative Survival After Transcatheter Aortic Valve Implantation: How Do Patients Undergoing Transcatheter Aortic Valve Implantation Fare Relative to the General Population? J. Am. Heart Assoc. 2017, 6, e007229. [Google Scholar] [CrossRef]
- Steffen, J.; Beckmann, M.; Haum, M.; Fischer, J.; Andreae, D.; Orban, M.; Rizas, K.; Braun, D.; Orban, M.; Curta, A.; et al. Systolic or diastolic CT image acquisition for transcatheter aortic valve replacement—An outcome analysis. J. Cardiovasc. Comput. Tomogr. 2022, 16, 423–430. [Google Scholar] [CrossRef]
- Francone, M.; Budde, R.P.J.; Bremerich, J.; Dacher, J.N.; Loewe, C.; Wolf, F.; Natale, L.; Pontone, G.; Redheuil, A.; Vliegenthart, R.; et al. CT and MR imaging prior to transcatheter aortic valve implantation: Standardisation of scanning protocols, measurements and reporting-a consensus document by the European Society of Cardiovascular Radiology (ESCR). Eur. Radiol. 2020, 30, 2627–2650. [Google Scholar] [CrossRef]
- Elnwagy, M.M.; Baraka, M.M.A.; Hafez, M.S.; Kamal, D.; El-Sayed, M.H.; Mostafa, A.E. Impact of prosthesis oversizing on clinical outcomes of transcatheter aortic valve implantation using a self-expandable Evolut R valve. Egypt Heart J. 2024, 76, 20. [Google Scholar] [CrossRef]
- Afilalo, J.; Lauck, S.; Kim, D.H.; Lefèvre, T.; Piazza, N.; Lachapelle, K.; Martucci, G.; Lamy, A.; Labinaz, M.; Peterson, M.D.; et al. Frailty in Older Adults Undergoing Aortic Valve Replacement. J. Am. Coll. Cardiol. 2017, 70, 689–700. [Google Scholar] [CrossRef]

{kind=link}
| Unmatched Population | Propensity-Matched Population * | ||||||
|---|---|---|---|---|---|---|---|
| Total | Retrospective ECG-Gated Scan | Prospective ECG-Triggered | p Value | Retrospective ECG-Gated Scan | Prospective ECG-Triggered | p Value | |
| N | 419 | 191 | 228 | 171 | 171 | ||
| Demographics | |||||||
| Age (mean (SD)) | 80.6 (7.8) | 80 (7.8) | 81 (7.6) | 0.13 | 80.1 (7.8) | 81.1 (7.8) | 0.25 |
| Male (%) | 225 (53.7%) | 96 (50%) | 129 (56%) | 0.19 | 90 (52.6%) | 95 (55.6%) | 0.58 |
| BMI (%) | 27.6 (6.2) | 27.9 (5.7) | 27.4 (6.6) | 0.4 | 27.6 (5.4) | 27.5 (6.9) | 0.87 |
| Medical background | |||||||
| Coronary artery disease (%) | 180/415 (43.4%) | 79 (42%) | 101 (44%) | 0.67 | 74 (43.3%) | 68 (39.8%) | 0.51 |
| Hypertension (%) | 254/346 (73.4%) | 121 (73%) | 133 (74%) | 0.83 | 113 (74.3%) | 102 (75.6%) | 0.81 |
| Diabetes mellitus (%) | 141/336 (42%) | 62 (38%) | 79 (45%) | 0.18 | 59 (39.9%) | 57 (42.5%) | 0.65 |
| COPD (%) | 33/415 (8%) | 18 (9.6%) | 15 (6.5%) | 0.25 | 18 (10.5%) | 10 (5.8%) | 0.11 |
| NYHA-Class (%) | 0.77 | 0.98 | |||||
| Class 2 | 25/415 (6%) | 13 (6.9%) | 12 (5.2%) | 13 (7.6%) | 12 (7.0%) | ||
| Class 3 | 322/415 (77.6%) | 144 (77%) | 178 (78%) | 130 (76.0%) | 131 (76.6%) | ||
| Class 4 | 68/415 (16.4%) | 30 (16%) | 38 (16%) | 28 (16.4%) | 28 (16.4%) | ||
| Chronic kidney disease (%) | 180 (43%) | 68 (35%) | 112 (49%) | 0.005 | 63 (36.8%) | 68 (36.8%) | 1 |
| Chronic dialysis (%) | 8/414 (1.9%) | 5 (2.7%) | 3 (1.3%) | 0.31 | 5 (2.9%) | 3 (1.8%) | 0.47 |
| GFR (mL/min) (mean (SD)) | 64.2 (25.2) | 67.2 (22.7) | 61.6 (26.8) | 0.02 | 66.5 (22.8) | 66.2 (23.2) | 0.89 |
| Peripheral vascular disease (%) | 14/415 (3.4%) | 3 (1.6%) | 11 (4.8%) | 0.07 | 3 (1.8%) | 8 (4.7%) | 0.12 |
| STS score (mean (SD)) | 3.05 (2.7) | 3.07 (3.2) | 3.03 (2.2) | 0.88 | 3.19 (3.4) | 2.88 (2.1) | 0.31 |
| EuroSCORE II (mean (SD)) | 5.51 (5.7) | 5.11 (4.9) | 5.83 (6.2) | 0.19 | 5.34 (5.1) | 5.60 (6.0) | 0.66 |
| Retrospective ECG-Gated Scan | Prospective ECG-Triggered | p Value | |
|---|---|---|---|
| N | 171 | 171 | |
| CT estimated effective radiation dose (mSv), median (IQR) | 8.04 (10.3) | 4.42 (3.6) | <0.001 |
| CT contrast (mL), median (IQR) | 70.0 (48) | 40.0 (12) | <0.001 |
| Aortic valve annulus diameter (mm), median (IQR) | 24.5 (3.6) | 23.3 (3.2) | 0.004 |
| Aortic valve annulus area (mm2), median (IQR) | 469.05 (130.8) | 426.6 (121.0) | 0.006 |
| Contrast material volume (mL) during TAVI, median (IQR) | 100.0 (50) | 100.0 (40) | 0.014 |
| Artifact due to respiratory motion | 13 (7.6%) | 1 (0.6%) | 0.001 |
| Prosthetic valve size, mean (SD) | 26.5 (2.8) | 25.6 (2.4) | 0.001 |
| Prosthetic valve size by groups | 0.001 | ||
| 20–24 | 31 (18.5%) | 59 (34.5%) | |
| 25–28 | 85 (50.6%) | 80 (46.8%) | |
| 29–34 | 52 (31.0%) | 32 (18.7%) | |
| Retrospective ECG-Gated Scan | Prospective ECG-Triggered | p Value | |
|---|---|---|---|
| N | 171 | 171 | |
| Mortality | |||
| Mean follow-up (month, SD) | 26.01 (14.1) | 27.29 (12.5) | 0.37 |
| Procedural mortality (%) | 1 (0.6%) | 1 (0.6%) | 1 |
| In-hospital mortality (%) | 2 (1.2%) | 3 (1.6%) | 0.65 |
| 30-day mortality (%) | 3 (1.8%) | 3 (1.8%) | 1 |
| 1-year mortality (%) | 10 (5.8%) | 12 (7.0%) | 0.66 |
| Overall mortality (%) | 21 (12.3%) | 32 (15.7%) | 0.2 |
| Composite outcomes | |||
| Technical failure (%) | 10 (5.8%) | 11 (6.4%) | 0.82 |
| Device failure (%) | 14 (8.2%) | 17 (9.9%) | 0.57 |
| Early safety events (%) | 22 (12.9%) | 24 (14.0%) | 0.75 |
| Paravalvular leak | |||
| Angiographic paravalvular leak (%) | 0.6 | ||
| None | 153 (89.5%) | 158 (92.9%) | |
| Minimal | 11 (6.4%) | 6 (3.5%) | |
| Mild | 5 (2.9%) | 5 (2.9%) | |
| Moderate | 2 (1.2%) | 1 (0.7%) | |
| Severe | 0 | 0 | |
| Echocardiographic paravalvular leak (%) | 0.31 | ||
| None | 149 (93.7%) | 156 (96.9%) | |
| Mild | 6 (3.8%) | 4 (2.5%) | |
| Moderate | 4 (2.5%) | 1 (0.6%) | |
| Complications | |||
| Need for a second valve (%) | 3 (1.8%) | 3 (1.8%) | 0.99 |
| Valve malposition (%) | 3 (1.8%) | 2 (1.2%) | 0.65 |
| In-hospital stroke/TIA (%) | 4 (2.4%) | 3 (1.8%) | 0.9 |
| Acute kidney injury (VARC-3) (stage 1–3) (%) | 2 (1.2%) | 3 (1.8%) | 0.6 |
| Major vascular complications (VARC-3) (%) | 2 (1.2%) | 7 (4.1%) | 0.24 |
| New post-procedural complete AV block (%) | 13 (7.6%) | 14 (8.2%) | 0.8 |
| New permanent pacemaker implantation (%) | 13 (7.6%) | 16 (9.4%) | 0.57 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amsalem, I.; Vitkon-Barkay, I.; Rav-Acha, M.; Dvir, D.; Elkan, M.; Pichkhadze, O.; Bogot, N.; Shaheen, F.; Hitter, R.; Chutko, B.; et al. Evaluation of Prospective ECG-Triggered CT Scan as a Practical Alternative to Standard Retrospective ECG-Gated Scan for Pre-TAVI Patients. J. Clin. Med. 2025, 14, 878. https://doi.org/10.3390/jcm14030878
Amsalem I, Vitkon-Barkay I, Rav-Acha M, Dvir D, Elkan M, Pichkhadze O, Bogot N, Shaheen F, Hitter R, Chutko B, et al. Evaluation of Prospective ECG-Triggered CT Scan as a Practical Alternative to Standard Retrospective ECG-Gated Scan for Pre-TAVI Patients. Journal of Clinical Medicine. 2025; 14(3):878. https://doi.org/10.3390/jcm14030878
Chicago/Turabian StyleAmsalem, Itshak, Itzhak Vitkon-Barkay, Moshe Rav-Acha, Danny Dvir, Matan Elkan, Olga Pichkhadze, Naama Bogot, Fauzi Shaheen, Rafael Hitter, Boris Chutko, and et al. 2025. "Evaluation of Prospective ECG-Triggered CT Scan as a Practical Alternative to Standard Retrospective ECG-Gated Scan for Pre-TAVI Patients" Journal of Clinical Medicine 14, no. 3: 878. https://doi.org/10.3390/jcm14030878
APA StyleAmsalem, I., Vitkon-Barkay, I., Rav-Acha, M., Dvir, D., Elkan, M., Pichkhadze, O., Bogot, N., Shaheen, F., Hitter, R., Chutko, B., Glikson, M., Leipsic, J., & Wolak, A. (2025). Evaluation of Prospective ECG-Triggered CT Scan as a Practical Alternative to Standard Retrospective ECG-Gated Scan for Pre-TAVI Patients. Journal of Clinical Medicine, 14(3), 878. https://doi.org/10.3390/jcm14030878