Abstract
Background: Metabolic dysfunction-Associated Steatotic Liver Disease (MASLD) is becoming a leading indication for liver transplantation in the United States. In this growing recipient population, the combined effects of underlying liver disease etiology and associated comorbidities on the evaluation pathway to transplantation warrant closer examination of patient outcomes. Methods: We analyzed adult liver transplant referrals (n = 9981) from the California Liver Network, a multi-center retrospective cohort spanning six high-volume California transplant centers between 2018 and 2020. A total of 6709 patients who underwent formal evaluation were included. Patients were stratified by MASLD vs. non-MASLD etiology and compared for demographics, comorbidities, transplant evaluation timelines, listing rates, and outcomes. Results: MASLD patients (n = 1477) were older, had higher BMI, and had greater prevalence of metabolic comorbidities than non-MASLD patients (n = 5232; p < 0.001 for all). Compared to non-MASLD candidates, MASLD patients were more likely to be waitlisted (OR 1.52, 95% CI 1.33–1.74; p < 0.001). However, MASLD and non-MASLD patients had no statistically significant difference in the rate of transplant (p = 0.182), with clinically similar but statistically inferior post-transplant survival outcomes at 5 years post-transplant (88% vs. 83%; p = 0.014). Competing-risk analysis showed that MASLD candidates had higher cumulative incidence of death on the waitlist (p < 0.001), although MASLD was not independently associated with waitlist mortality when adjusting for covariates (p = 0.300). MASLD patients demonstrated increased mortality following waitlist removal (HR 1.64, 95% CI 1.14–2.35; p = 0.008), primarily among those removed for clinical deterioration (HR 1.50, 95% CI 1.01–2.23; p = 0.044). Conclusions: MASLD patients face unique challenges in liver transplant evaluation. MASLD patients are associated with higher comorbidities, increased incidence of waitlist mortality, and significantly higher mortality rate following waitlist removal. However, transplantation provides significant survival benefit with comparable outcomes to non-MASLD recipients; thus, early access to transplant may optimize outcomes for MASLD liver transplant candidates.
1. Introduction
As the prevalence of metabolic syndrome and obesity in the United States continues to rise, the downstream effects on disease-specific presentation continue to proliferate—especially in liver transplantation [1]. Since 2018, Metabolic dysfunction-Associated Steatotic Liver Disease (MASLD) has quickly emerged as the second most common etiology of liver disease, trailing only alcohol-associated liver disease [2]. Similarly, MASLD is the second most common indication for liver transplant in the United States [3], and has been the most rapidly increasing indication for liver transplantation, in both patients with and without hepatocellular carcinoma [4]. The impact of MASLD on liver transplant is only poised to increase, with MASLD-related waitlist addition predicted to increase by 55.4% between 2016 and 2030 [5].
Metabolic syndrome increases the complexity of patient management across the transplant spectrum, as optimal patient management must simultaneously address liver disease and the comorbidities of metabolic syndrome—including diabetes mellitus, hypertension, coronary artery disease, and hyperlipidemia—both pre- and post-transplant [6]. MASLD has been shown to be an independent risk factor for the development of cardiovascular disease, which is a leading cause of mortality in liver transplant patients [7]. While prior national database studies have demonstrated comparable graft and patient survival between MASLD and non-MASLD liver transplant recipients [8], studies have identified metabolic comorbidities as barriers to patients receiving liver transplantation [9]. Therefore, despite comparable transplant outcomes, further studies are needed to distinguish the overall waitlist and transplant trajectories of MASLD and non-MASLD etiologies.
Importantly, the effects of metabolic syndrome, obesity, and associated complications on liver transplant referral and evaluation practice patterns are not well understood. In addition, most current studies utilize large databases and lack the granularity to understand how the particular facets of metabolic syndrome impact a candidate’s likelihood to undergo liver transplant evaluation and subsequently proceed to waitlisting. Here, we utilize the California Liver Network—a research collaborative evaluating all liver transplant referrals over a two-year period at six large volume transplant centers in California—to evaluate the impact of MASLD on patient waitlisting and waitlisting outcomes as compared to non-MASLD candidates. This detailed dataset comprising over 75% of all liver transplant referrals in California enables a granular analysis of patient progression and risk factors, providing potential insights to optimize patient pre-transplant management for liver transplant candidates with MASLD.
2. Materials and Methods
This study utilizes the California Liver Network (CLN), a retrospective consortium of six high-volume liver transplant centers in California (University of California San Francisco, University of California Los Angeles, University of California San Diego, Cedars-Sinai Medical Center, Stanford University, and University of Southern California) formed to investigate referral and evaluation practices in liver transplantation. All adult liver transplant referrals received between 201 January 8 and 31 December 2020 were included in this study (n = 9981), with follow-up for outcomes through July 2022. Basic demographic data, including site, age, gender, insurance and address, was obtained for patients who did not initiate evaluation (n = 3272). Clinical, demographic, and psychosocial data were retrospectively collected for evaluated patients. Outcomes of evaluation, selection, waitlisting, and transplantation were monitored. Patients were stratified by disease etiology to compare outcomes between MASLD and non-MASLD candidates, as determined by clinical evaluation. Number of patients at each timepoint is shown in Figure 1.
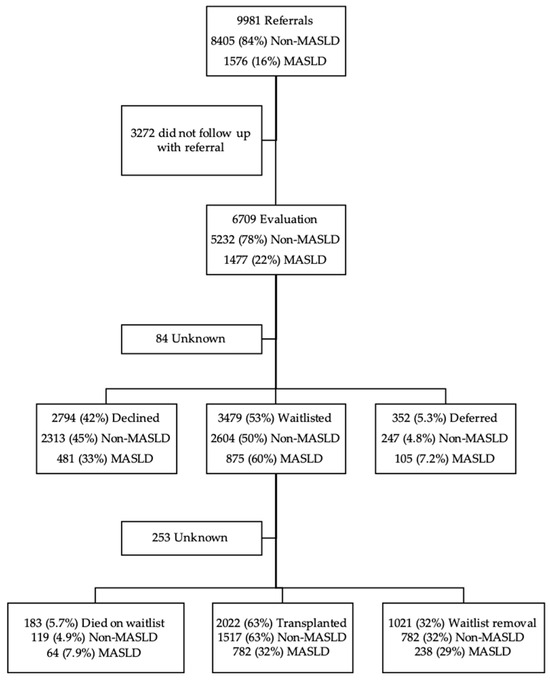
Figure 1.
Cohort Selection and Evaluation Outcomes of Patients Referred for Liver Transplantation.
All patients proceeding with liver transplant evaluation within the CLN were included in this study (n = 6709). Patients were analyzed for demographics including age, sex, body mass index (BMI), race, MELD, and marital status. Etiology of liver disease was classified as MASLD versus non-MASLD (including alcohol, hepatitis C, hepatitis B, autoimmune hepatitis, primary biliary cirrhosis, primary sclerosing cholangitis, cryptogenic, and other). Candidates were identified as having compensated versus decompensated cirrhosis. Decompensated cirrhosis was defined as events including presence of ascites, hepatic encephalopathy, variceal bleeding, hepatopulmonary syndrome, and portopulmonary syndrome. Comorbidities of metabolic syndrome were likewise captured including diabetes mellitus, hypertension, hyperlipidemia and coronary artery disease requiring intervention.
Baseline patient characteristics were compared between the MASLD and non-MASLD groups using the Wilcoxon rank-sum test for continuous variables and Pearson’s chi-squared test for categorical variables, as appropriate. Missing data for all multivariable analyses were handled using multiple imputation by chained equations (MICE) with five imputations [10]. The imputation model included all variables listed in Table 1. Multivariable analyses were performed on each imputed dataset, and results were pooled using Rubin’s rules [11].
Time-to-event analyses were conducted using both the Cox proportional hazards model and the Fine and Gray subdistribution hazard model. For the outcome of waitlisting, time from waitlist entry to removal, transplantation, or death was analyzed, treating these as competing events. Cumulative incidence functions were estimated for each outcome, and cumulative incidence curves between MASLD and non-MASLD groups were compared using Gray’s test [12]. The Fine and Gray model was used to assess factors associated with each competing outcome, adjusting for relevant patient and clinical covariates.
Factors associated with waitlisting were investigated using a generalized linear mixed-effects model with a random intercept for transplant center. Covariates included age, sex, transplant site, BMI, MELD at listing, presence of comorbidities, and etiology of liver disease.. To assess potential effect modification by BMI class, site, and sex on the association between MASLD and waitlisting, interaction terms were included in the model, adjusting for the same covariates.
Overall survival following waitlist removal was estimated using the Kaplan–Meier method and compared between MASLD and non-MASLD groups using the log-rank test. Time to death was defined as the interval from waitlist removal to death or last follow-up. The Cox proportional hazards model was used to assess factors associated with overall survival post-waitlist removal, adjusting for relevant patient and clinical covariates. Effect modification by removal reason on the association between MASLD and overall survival was assessed by including an interaction term in the model. The proportional hazards assumption was evaluated using Schoenfeld residuals and the goodness-of-fit test described by Grambsch and Therneau [13].
All statistical analyses were performed using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value < 0.05 was considered statistically significant.
3. Results
3.1. Demographics
A total of 6709 patients were evaluated for liver transplant in the CLN consortium, of which 1477 (22.0%) had MASLD and 5232 (78.0%) had non-MASLD etiologies. The demographics of each cohort are summarized in Table 1.

Table 1.
Demographics.
Table 1.
Demographics.
| Characteristic | Overall N = 6709 1 | Non-MASLD N = 5232 1 | MASLD N = 1477 1 | p-Value 2 |
|---|---|---|---|---|
| Age at Referral | 59 (50, 65) | 57 (48, 64) | 63 (56, 67) | <0.001 |
| Sex | <0.001 | |||
| female | 2693 (40.1%) | 1892 (36.2%) | 801 (54.2%) | |
| male | 4012 (59.8%) | 3336 (63.7%) | 676 (45.8%) | |
| Unknown | 4 | 4 | 0 | |
| Ethnicity | <0.001 | |||
| Hispanic/Latino | 2840 (43.8%) | 2065 (40.9%) | 775 (54.0%) | |
| Not Hispanic/Latino | 3642 (56.1%) | 2983 (59.0%) | 659 (45.9%) | |
| Unknown | 227 | 184 | 43 | |
| Race | <0.001 | |||
| African American | 234 (3.7%) | 219 (4.4%) | 15 (1.1%) | |
| American Indian/Alaskan Native | 65 (1.0%) | 48 (1.0%) | 17 (1.2%) | |
| Asian American/Pacific Islander | 692 (10.9%) | 589 (11.9%) | 103 (7.3%) | |
| White | 3706 (58.5%) | 2847 (57.7%) | 859 (61.3%) | |
| Other/Multiracial | 1637 (25.8%) | 1229 (24.9%) | 408 (29.1%) | |
| Unknown | 375 | 300 | 75 | |
| Body Mass Index (BMI) | 28 (24, 32) | 27 (23, 31) | 31 (27, 36) | <0.001 |
| Unknown | 51 | 41 | 10 | |
| BMI Class | <0.001 | |||
| Underweight | 156 (2.3%) | 136 (2.6%) | 20 (1.4%) | |
| Normal | 1999 (30.0%) | 1801 (34.6%) | 198 (13.4%) | |
| Overweight | 2143 (32.2%) | 1736 (33.4%) | 407 (27.7%) | |
| Obese | 1972 (29.6%) | 1300 (25.0%) | 672 (45.8%) | |
| Morbidly Obese | 388 (5.8%) | 218 (4.2%) | 170 (11.6%) | |
| Unknown | 51 | 41 | 10 | |
| Decompensated Cirrhosis | 4620 (68.8%) | 3465 (66.2%) | 1155 (78.2%) | <0.001 |
| Hepatocellular Carcinoma | 1530 (22.8%) | 1217 (23.2%) | 313 (21.2%) | 0.094 |
| Comorbidities | ||||
| Diabetes Mellitus | 1748 (26.1%) | 993 (19.0%) | 755 (51.2%) | <0.001 |
| Hypertension | 2013 (30.0%) | 1368 (26.1%) | 645 (43.7%) | <0.001 |
| Hyperlipidemia | 848 (12.6%) | 506 (9.7%) | 342 (23.1%) | <0.001 |
| Coronary Artery Disease | 312 (4.7%) | 213 (4.1%) | 99 (6.7%) | <0.001 |
1 Median (Q1, Q3); n (%); 2 Wilcoxon rank sum test; Pearson’s Chi-squared test.
Patients in the MASLD cohort were significantly older than those in the non-MASLD cohort (median age 63 [56–67] years vs. 57 [48–64] years; p < 0.001). The MASLD group included a lower proportion of male patients (45.8% vs. 63.7%; p < 0.001). Racial and ethnic distribution differed significantly between groups (p < 0.001 for both). MASLD patients had a higher proportion of Hispanic/Latino patients (54.0% vs. 40.9%) than non-MASLD patients. The MASLD cohort had a lower proportion of African American (1.1% vs. 4.4%) and Asian American/Pacific Islander patients (7.3% vs. 12%), but a higher proportion of White patients (61.3% vs. 57.7%).
Body mass index (BMI) was significantly higher among MASLD patients (median 31 [27–36] vs. 27 [23–31]; p < 0.001). Correspondingly, obesity was more prevalent in the MASLD group, with higher rates of both obesity (BMI 30–39.9; 45.8% vs. 25.0%) and morbid obesity (BMI ≥ 40; 11.6% vs. 4.2%; p < 0.001). MASLD patients also had a higher prevalence of comorbid conditions, including diabetes mellitus (51.2% vs. 19.0%), hypertension (43.7% vs. 26.1%), hyperlipidemia (23.1% vs. 9.7%), and coronary artery disease (6.7% vs. 4.1%; p < 0.001 for all). Decompensated cirrhosis was more frequent in the MASLD cohort (78.2% vs. 66.2%; p < 0.001). Rates of hepatocellular carcinoma were similar between groups (21.2% vs. 23.2%; p = 0.094).
3.2. Predictors and Interaction Analyses of Waitlisting Among MASLD and Non-MASLD Candidates
Overall, 57.8% of MASLD and 48.3% of non-MASLD patients were waitlisted for transplant. A multivariable mixed-effects logistic regression model was performed to identify independent factors associated with waitlisting (Table 2). In this model, older age at referral was associated with slightly lower odds of waitlisting (OR 0.99 per year increase, 95% CI 0.99–1.00; p < 0.001). Sex and MELD at evaluation were not significantly associated with waitlisting. Compared with patients with normal BMI, those classified as morbidly obese had significantly lower odds of waitlisting (OR 0.65, 95% CI 0.52–0.82; p < 0.001), whereas other BMI categories were not significantly different.
Table 2.
Multivariable Logistic Regression for Waitlisting.
The effect of relevant comorbidities (hypertension, coronary artery disease, diabetes, hyperlipidemia) was also evaluated. Patients with one comorbidity had slightly higher odds of being waitlisted compared to those without comorbidities (OR 1.15, 95% CI 1.01–1.30; p = 0.029), whereas patients with more than one comorbidity did not have significantly higher odds of being waitlisted. Importantly, MASLD etiology was independently associated with greater likelihood of waitlisting compared with non-MASLD etiologies (OR 1.52, 95% CI 1.33–1.74; p < 0.001).
To assess whether the association between liver disease etiology and waitlisting varied by BMI class, transplant center, or sex, interaction analyses were performed (Table 3). In the BMI interaction model, MASLD patients classified as overweight or obese had higher odds of being waitlisted compared with non-MASLD counterparts (overweight: OR 1.13, 95% CI 1.07–1.19; p < 0.001; obese: OR 1.12, 95% CI 1.07–1.17; p < 0.001). Normal-weight and underweight BMI classes showed no significant difference with waitlisting odds, and the overall interaction between BMI and etiology was also not significant (p for interaction = 0.096).
Table 3.
Logistic Interaction with Waitlisting with BMI, Site Interaction, and Sex.
In the site interaction model, variation in odds of waitlisting across transplant centers was observed (p for interaction = 0.014). Sites 1, 2, 5 demonstrated significantly higher odds of waitlisting MASLD patients when compared to non-MASLD patients (site 1: OR 1.18, 95% CI 1.11–1.25; p < 0.001; site 2: OR 1.12, 95% CI 1.06–1.18; p < 0.001; site 5: OR 1.15, 95% CI 1.05–1.26; p = 0.002). In contrast, no significant interaction was observed between sex and etiology (p for interaction = 0.571). Odds of waitlisting were comparable between male and female candidates in both MASLD and non-MASLD groups.
3.3. Waitlist Outcomes
At five years after waitlist registration, approximately 15% of MASLD patients had died on the waitlist compared with 10% of non-MASLD patients, while rates of removal were similar between groups (both approximately 25%). The cumulative probability of liver transplantation by five years was 60–65% in both cohorts. Year-specific cumulative incidence rates for each outcome are shown in Supplemental Figure S1.
Competing-risk analysis demonstrated distinct cumulative incidence patterns for waitlist outcomes between MASLD and non-MASLD candidates (Figure 2). Patients with MASLD had a significantly higher cumulative incidence of waitlist death compared with non-MASLD candidates (p < 0.001; Figure 2A). Conversely, there was no significant difference in cumulative incidence of waitlist removal (p = 0.311; Figure 2B) or eventual liver transplantation (p = 0.192; Figure 2C).
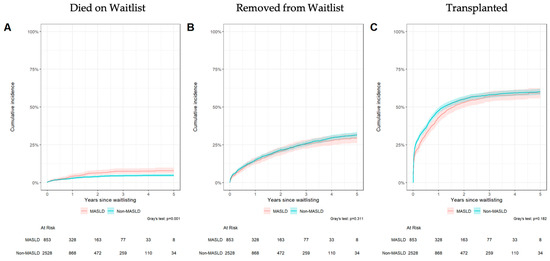
Figure 2.
Cumulative Incidence analysis of waitlist mortality (A), removal from waitlist (B), and liver transplantation (C).
Given the competing nature of transplant and death events, subsequent Fine–Gray competing-risk models were used to evaluate time-dependent outcomes of waitlist death, waitlist removal, and transplantation adjusting for covariates (Table 4). Older age at referral was independently associated with higher risk of death while on the waitlist (HR 1.02, 95% CI 1.00–1.03; p = 0.039), but not with waitlist removal or transplantation. Male candidates had a lower subdistribution hazard of waitlist death compared to females (HR 0.72, 95% CI 0.53–0.98; p = 0.036) but higher likelihood of transplantation (HR 1.19, 95% CI 1.06–1.32; p = 0.002).
Table 4.
Fine-Gray Competing Risk Model for Waitlist Removal, Death, and Transplant.
Significant site variation was observed across transplant centers (p < 0.001). Compared with the reference site, Site 1 demonstrated higher hazards for death on the waitlist (HR 1.62, 95% CI 1.02–2.41; p = 0.017), while site 4 and 5 showed lower risk (site 4: HR 0.25, 95% CI 0.11–0.52; p = 0.002. Site 5: HR 0.45, 95% CI 0.23–0.88; p = 0.02). Furthermore, site 1 demonstrated significantly higher hazards for waitlist removal (HR 1.27, 95% CI 1.07–1.52; p = 0.007) and lower rates for transplantation (HR 0.67, 95% CI 0.57–0.58; p < 0.001). On the other hand, site 4, who has lower risk of waitlist death, also showed higher odds of proceeding with transplantation (HR 1.3, 95% CI 1.08–1.56; p = 0.005).
Among BMI categories, obesity was associated with an increased hazard of dying on waitlist compared with normal BMI (HR 1.52, 95% CI 1.00–2.30; p = 0.049), as well as lower odds for proceeding to transplantation (HR 0.86, 95%CI 0.75–0.99; p = 0.03). Other BMI groups did not show significant associations. Higher MELD score at listing was associated with mildly lower likelihood of being removed from waitlist (HR 0.97, 95% CI 0.97–0.98; p < 0.001) and greater likelihood of transplant (HR 1.06, 95% CI 1.05–1.07; p < 0.001).
Notably, in the adjusted Fine-Gray competing risk analysis, MASLD etiology was not independently associated with the subdistribution hazards of waitlist death, waitlist removal, or transplantation compared with non-MASLD etiologies.
3.4. MASLD Patients Have Lower Survival Rate After Waitlist Removal and Transplantation
Survival analyses were performed to evaluate post-waitlist removal and post-transplant survival among MASLD and non-MASLD patients. For patients who received a transplantation, MASLD recipients demonstrated lower 5-year post-transplant survival (83%, 95% CI 78–88%) compared to non-MASLD patients (88%, 95% CI 85–90%, log-rank p = 0.014; Figure 3A). In Cox analysis of post-transplant survival (Supplemental Table S2), MASLD remained a risk factor for inferior patient survival (HR 1.43; 95% CI 1.03–2.06; p = 0.033). Furthermore, in post-transplant survival analysis, when accounting for liver disease etiology, patients who were underweight had a significantly higher hazard ratio for mortality (HR 2.29; 95% CI 1.12–4.70; p = 0.02), while overweight patients had significantly lower hazard ratio for mortality (HR 0.66; 95% CI 0.46–0.96; p = 0.03).
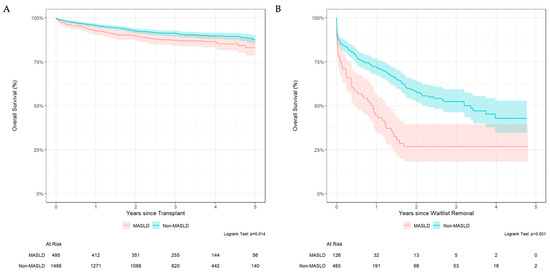
Figure 3.
Kaplan–Meier Survival following liver transplantation (A) and for patients following waitlist removal (B).
Kaplan–Meier analysis for survival following waitlist removal revealed significantly reduced survival rates among MASLD candidates compared with non-MASLD candidates (log-rank p < 0.001; Figure 3B). In the adjusted multivariable Cox model, higher MELD at listing (HR 1.04, 95% CI 1.03–1.04, p < 0.001) and MASLD etiology (HR 1.64, 95% CI 1.14–2.35; p = 0.008) were significant predictors of mortality following waitlist removal (Supplemental Table S3). Age, sex, and BMI class were not significant predictors for mortality following waitlist removal. Regarding comorbidities, the presence of fewer than 4 comorbidities was not associated with mortality, while patients with four or more comorbidities demonstrated increased mortality risk following waitlist removal (HR 13.8, 95% CI 2.71–70.3; p = 0.002) although this finding may be confounded by small sample size given extremely wide confidence interval.
Additional Kaplan–Meier analyses stratified by reason of waitlist removal were shown in Supplemental Figure S1. When adjusting for covariates, the overall interaction between etiology and reason for waitlist removal was not significant (p for interaction = 0.809, Supplemental Table S4). However, subgroup analysis revealed higher mortality among MASLD compared with non-MASLD patients removed from the waitlist for clinical deterioration (HR 1.50, 95% CI 1.01–2.23; p = 0.044). No significant differences were observed for psychosocial (HR 1.63, 95% CI 0.47–5.59; p = 0.436), medical contraindication (HR 1.79, 95% CI 0.70–4.56; p = 0.221), condition improved (HR 4.88, 95% CI 0.29–83.35; p = 0.273), patient choice (HR 2.93, 95% CI 0.67–12.76; p = 0.152), or other reasons (HR 6.00, 95% CI 0.39–92.60; p = 0.199), noting wide confidence intervals consistent with small event counts in several strata.
4. Discussion
MASLD continues to grow as a leading indication for liver transplantation (LT), and the management of these patients throughout the transplantation process poses a challenge to the healthcare system [2]. Through this study of the California Liver Network, we identified that MASLD patients have higher rates of mortality on the waitlist, increased mortality following waitlist removal, and slightly impaired survival post-LT as compared to non-MASLD liver transplant candidates. The findings of this study identify areas of focus and potential intervention for MASLD candidates to optimize transplant outcomes in this growing cohort.
Consistent with existing literature, MASLD patients frequently present with a higher burden of medical comorbidities [6]. Specifically, MASLD patients are more likely to have history of diabetes, hypertension, hyperlipidemia and coronary disease as compared to non-MASLD LT candidates. Furthermore, MASLD candidates are more likely to present with decompensated cirrhosis at the time of listing. In all, these additional layers of complexity may help explain why MASLD patients have lower survival rate when removed from waitlist and even after transplant compared to non-MASLD patients. Although MASLD patients demonstrated higher waitlist mortality in this study, Fine-Gray analysis did not identify MASLD etiology as an independent predictor of waitlist mortality. This suggests that the ways MASLD physiology, associated comorbidities, and metabolic syndrome contribute to impaired survival across the transplant pathway are multifactorial. Regardless, there was still significant survival benefit after transplantation compared to patients who were removed from waitlist. This emphasizes the critical importance of timely access to transplantation for the MASLD cohort, even given their higher baseline risks. MASLD patients are likely to benefit from management of metabolic syndrome through weight loss and optimization of comorbidities as they progress through the transplant pathway. Pharmacologic agents such as glucagon-like peptide 1 (GLP-1) receptor agonists represent an emerging therapeutic class that may improve metabolic control, slow the progression of liver disease, and decrease risk for decompensation in MASLD patients, although the effects in cirrhotic patients and transplant recipients have not been fully investigated [14,15,16].
The effect of BMI on liver transplant candidacy also must be acknowledged. Our study demonstrated that morbid obesity (BMI ≥ 40) was associated with decreased likelihood for waitlisting overall. This reflects the technical complexity associated with performing a liver transplant in the morbidly obese recipient. Nonetheless, overweight (BMI 25.0–29.9) and obese (BMI 30–39.9) MASLD patients were more likely to be waitlisted than non-MASLD patients with similar BMI. Further, obese patients were more likely to die on the waitlist and less likely to proceed to transplant as compared to patients with normal BMI. In patients who were transplanted, underweight LT recipients (BMI < 18.5) demonstrated inferior post-transplant survival while overweight LT recipients demonstrated superior post-transplant survival. Frailty is known to be a negative predictor of post-transplant outcomes, and these results highlight the challenge in assessing frailty within the MASLD population. It is important to note that elevated BMI in chronic liver failure may be attributable to anasarca and/or fluid overload, which can mask underlying patient frailty. In fact, MASLD patients have a six-fold increased risk of having sarcopenic obesity [17]. One recent study demonstrated that for MASLD patients, lower BMI was associated with worse long-term graft and patient survival, in contrast to non-MASLD patients, where higher BMI was associated with worse survival [18]. While this study did not identify BMI as an overall predictor of post-transplant outcomes, studies have shown that patients with higher BMI were >10% more likely to be turned down for an organ [19]. These results suggest an inherent reluctance to transplant higher BMI candidates without clear evidence that they have worse post-transplant outcomes [18]. For patients whose BMI reflects obesity with potential technical challenge, weight loss approaches including glucagon-like-peptide 1 (GLP-1) receptor agonists and simultaneous liver transplant with sleeve gastrectomy are options to be considered to facilitate the technical aspects of transplantation, particularly in patients undergoing outpatient evaluation [20,21].
Transplant center site was an independent factor affecting waitlisting for both MASLD and non-MASLD patients. While an interesting finding, the underlying drivers of variance in practice between large academic institutions are likely multifactorial, including center-specific waitlisting practices and thresholds, differences in transplant candidate acuity and frailty, and differing approaches to managing medically complex patients. In the context of MASLD, we hope that the results of this study and further research help contribute to an informed, uniform approach to MASLD patients and associated comorbidities to guide waitlisting practices and ensure wider access to transplant.
This study likewise redemonstrated some gender-based disparity in access to liver transplant and post-transplant outcomes. In this study, there was no difference in waitlisting probability between male and female patients—distinct from previous studies demonstrating disparity in waitlisting for female patients [22]. However, the results of this study continued to demonstrate decreased rates of waitlist mortality and higher likelihood of transplant for male candidates as compared to female candidates. While sarcopenia and body habitus may be limiting factors in access to transplant and outcomes, this gender disparity should remain a focus in future studies.
A key strength of this study lies in the granular nature of its clinical data, which allowed for a detailed assessment of waitlist removal reasons and patient-level factors—information often sparse in large national databases. Additionally, the study population reflects greater racial and ethnic diversity compared to national cohorts, reflecting California’s demographic composition. However, this study is limited in its general applicability on a national scale, as California transplant centers represent higher median MELD at transplant than other regions throughout the United States [23]. Furthermore, the study period (2018–2020) overlapped with the early phase of the COVID-19 pandemic, which may have impacted listing and transplant practices. As longer-term follow-up data become available, it will be important to evaluate the consistency of these trends. Finally, the data source utilized in this study is limited, as donor and liver allograft data are not included in the analysis, which are known to impact transplant outcomes.
In summary, as MASLD becomes a more common indication for liver transplantation, it is imperative that perioperative and waitlist management strategies evolve to address the unique challenges of this patient population. Our findings support earlier identification and referral of MASLD patients before decompensation, integration of metabolic optimization during evaluation, and development of standardized criteria for MASLD patients to improve equity and transplantation access. Proactive optimization of comorbid conditions, a nuanced assessment of body composition rather than sole reliance on BMI, and multidisciplinary care are critical steps to improve waitlist outcomes and reduce mortality among MASLD patients.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm14217841/s1, Table S1. Cumulative Incidence Table for Waitlist Death, Waitlist Removal and Transplantation. Table S2. Cox Model for Mortality Following Transplant. Table S3. Cox Model for Mortality Following Waitlist Removal. Table S4. Cox Model for Mortality Following Waitlist Removal with Interaction by Removal Reason. Figure S1. Kaplan–Meier Curves for Survival Following Waitlist Removal by Reason for Removal.
Author Contributions
Conceptualization, T.Y.L., J.S., H.T. and S.A.W.; methodology, T.Y.L., J.S., H.T. and S.A.W.; software, S.A.W.; formal analysis, T.Y.L. and S.A.W.; investigation, T.Y.L. and S.A.W.; resources, S.A.W.; data curation, All authors; writing—original draft preparation, T.Y.L. and S.A.W.; writing—review and editing, All authors; visualization, T.Y.L., M.L. and S.A.W.; supervision, S.A.W.; project administration, T.Y.L. and S.A.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Review Board at each participating center: Cedars-Sinai Medical Center (STUDY#00002483) approved date: 1 January 2025, University of Southern California (#HS-21-00570), Stanford University (#40344), University of California Los Angeles (IRB#22-001661), University of California San Francisco (#20-32625), and University of California San Diego (#201014). A data use agreement was established and agreed upon between all centers to establish a multi-center registry, with University of California San Francisco serving as the organizing center. Data was collected using a HIPAA-compliant RedCap system.
Informed Consent Statement
Informed consent is exempted from this study as it is a retrospective anonymized cohort, inclusion of the study does not place additional risk on patients.
Data Availability Statement
The datasets presented in this article are not readily available because the data are part of ongoing studies and due to privacy issues. Requests to access the datasets should be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MASLD | Metabolic dysfunction-associated steatotic liver disease |
| LT | Liver Transplantation |
| MELD | Model for End-Stage Liver Disease |
| BMI | Body Mass Index |
| CLN | California Liver Network |
| GLP-1 | Glucagon-Like Peptide 1 |
References
- Le, P.; Tatar, M.; Dasarathy, S.; Alkhouri, N.; Herman, W.H.; Taksler, G.B.; Deshpande, A.; Ye, W.; Adekunle, O.A.; McCullough, A.; et al. Estimated Burden of Metabolic Dysfunction-Associated Steatotic Liver Disease in US Adults, 2020 to 2050. JAMA Netw. Open 2025, 8, e2454707. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Stepanova, M.; Al Shabeeb, R.; Eberly, K.E.; Shah, D.; Nguyen, V.; Ong, J.; Henry, L.; Alqahtani, S.A. The changing epidemiology of adult liver transplantation in the United States in 2013–2022: The dominance of metabolic dysfunction-associated steatotic liver disease and alcohol-associated liver disease. Hepatol. Commun. 2024, 8, e0352. [Google Scholar] [CrossRef]
- Kwong, A.J.; Schnellinger, E.; Foutz, J.; Cafarella, M.; Nagai, S.; Biggins, S.W.; Pomposelli, J.; Trotter, J. Excess waitlist mortality among candidates for multivisceral liver-intestine transplant in acuity circle allocation. Am. J. Transplant. 2024, 24, 1080–1086. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Stepanova, M.; Ong, J.; Trimble, G.; AlQahtani, S.; Younossi, I.; Ahmed, A.; Racila, A.; Henry, L. Nonalcoholic Steatohepatitis Is the Most Rapidly Increasing Indication for Liver Transplantation in the United States. Clin. Gastroenterol. Hepatol. 2021, 19, 580–589.e5. [Google Scholar] [CrossRef]
- Parikh, N.D.; Marrero, W.J.; Wang, J.; Steuer, J.; Tapper, E.B.; Konerman, M.; Singal, A.G.; Hutton, D.W.; Byon, E.; Lavieri, M.S. Projected Increase in Obesity and Non-Alcoholic-Steatohepatitis–Related Liver Transplantation Waitlist Additions in the United States. Hepatology 2019, 70, 487–495. [Google Scholar] [CrossRef]
- Steggerda, J.A.; Mahendraraj, K.; Todo, T.; Noureddin, M. Clinical considerations in the management of non-alcoholic steatohepatitis cirrhosis pre- And post-transplant: A multi-system challenge. World J. Gastroenterol. 2020, 26, 4018–4035. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Tilg, H. MASLD: A systemic metabolic disorder with cardiovascular and malignant complications. Gut 2024, 73, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Altshuler, P.J.; Dang, H.; Frank, A.M.; Shah, A.P.; Glorioso, J.; Zhan, T.; Rios Diaz, A.; Shaheen, O.; Ramirez, C.B.; Maley, W.R.; et al. Evaluating Outcomes Related to Donor and Recipient Metabolic Environment: Macrosteatotic Allografts and Nonalcoholic Steatohepatitis. Liver Transplant. 2022, 28, 623–635. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Marchesini, G.; Pinto-Cortez, H.; Petta, S. Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: Implications for Liver Transplantation. Transplantation 2019, 103, 22–27. [Google Scholar] [CrossRef]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 1987. [Google Scholar] [CrossRef]
- Gray, R.J. A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann. Statist. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Grambsch, P.M.; Therneau, T.M. Proportional hazards tests ad diagnostics based on weighted residuals. Biometrika 1994, 81, 515–526. [Google Scholar] [CrossRef]
- Kanwal, F.; Kramer, J.R.; Li, L.; Yang, Y.X.; Cao, Y.; Yu, X.; Samuel, R.; Ali, B.; Desiderio, R.; Cholankeril, G.; et al. GLP-1 Receptor Agonists and Risk for Cirrhosis and Related Complications in Patients With Metabolic Dysfunction-Associated Steatotic Liver Disease. JAMA Intern. Med. 2024, 184, 1314–1323. [Google Scholar] [CrossRef]
- Wester, A.; Shang, Y.; Grip, E.T.; Matthews, A.A.; Hagström, H. Glucagon-like peptide-1 receptor agonists and risk of major adverse liver outcomes in patients with chronic liver disease and type 2 diabetes. Gut 2024, 73, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.H.; Wong, G.; Garner, E.; Izzy, M.; Srivastava, G. Utility of glucagon-like peptide 1 receptor agonists as anti-obesity medications in liver transplant recipients. Liver Transpl. 2024, 30, 226–228. [Google Scholar] [CrossRef] [PubMed]
- Carias, S.; Castellanos, A.L.; Vilchez, V.; Nair, R.; Dela Cruz, A.C.; Watkins, J.; Barrett, T.; Trushar, P.; Esser, K.; Gedaly, R. Nonalcoholic steatohepatitis is strongly associated with sarcopenic obesity in patients with cirrhosis undergoing liver transplant evaluation. J. Gastroenterol. Hepatol. 2016, 31, 628–633. [Google Scholar] [CrossRef]
- Satapathy, S.K.; Jiang, Y.; Agbim, U.; Wu, C.; Bernstein, D.E.; Teperman, L.W.; Kedia, S.K.; Aithal, G.P.; Bhamidimarri, K.R.; Duseja, A.; et al. Posttransplant Outcome of Lean Compared With Obese Nonalcoholic Steatohepatitis in the United States: The Obesity Paradox. Liver Transplant. 2020, 26, 68–79. [Google Scholar] [CrossRef]
- Segev, D.L.; Thompson, R.E.; Locke, J.E.; Simpkins, C.E.; Thuluvath, P.J.; Montgomery, R.A.; Maley, W.R. Prolonged waiting times for liver transplantation in obese patients. Ann. Surg. 2008, 248, 863–870. [Google Scholar] [CrossRef]
- Larson, E.L.; Ellias, S.D.; Blezek, D.J.; Klug, J.; Hartman, R.P.; Ziller, N.F.; Bamlet, H.; Mao, S.A.; Perry, D.K.; Nimma, I.R.; et al. Simultaneous liver transplant and sleeve gastrectomy provides durable weight loss, improves metabolic syndrome and reduces allograft steatosis. J. Hepatol. 2025, 83, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.G.; Bitetto, D.; Fornasiere, E.; Fumolo, E.; Ferrarese, A.; Toniutto, P. Efficacy and Safety of GLP-1 Receptor Agonists and SGLT-2 Inhibitors in the Treatment of Diabetes Mellitus and Obesity in Liver Transplant Recipients: A Systematic Review. J. Clin. Med. 2025, 14, 4619. [Google Scholar] [CrossRef]
- Karnam, R.S.; Chen, S.; Xu, W.; Chen, C.; Elangainesan, P.; Ghanekar, A.; McGilvray, I.; Reichman, T.; Sayed, B.; Selzner, M.; et al. Sex Disparity in Liver Transplant and Access to Living Donation. JAMA Surg. 2021, 156, 1010–1017. [Google Scholar] [CrossRef] [PubMed]
- Croome, K.P.; Lee, D.D.; Burns, J.M.; Keaveny, A.P.; Taner, C.B. Intraregional model for end-stage liver disease score variation in liver transplantation: Disparity in our own backyard. Liver Transplant. 2018, 24, 488–496. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).