Abstract
Despite the wealth of evidence in favour of SGLT2 inhibitor use in patients with chronic heart failure, their role in the very early stages of heart failure is still unclear. While the latest update of the European Society of Cardiology guidelines on heart failure advocates the use SGLT2 inhibitors in the acute phases of heart failure based on the results of the latest trials, it does not clarify the appropriate timing to start this therapy, leaving the clinician to decide whether SGLT2 inhibitors should be started directly during hospitalization or at discharge. Conversely, the recently published focused update of the American College of Cardiology expert consensus decision pathway on the clinical assessment, management, and trajectory of patients hospitalized with heart failure clearly supports the safety and early clinical benefit use of SGLT2 inhibitors based on evidence coming from the EMPULSE and SOLOIST-WHF trials. The expert consensus decision pathway states that SGLT2 inhibitors can be initiated regardless of left ventricular ejection fraction at any time during hospitalization and places a greater emphasis on implementing the other pillars of therapy for heart failure with reduced ejection fraction after stabilization. Moreover, the results of the very recent DAPA ACT HF–TIMI 68 trial on dapagliflozin in patients with acute heart failure, although limited by a follow-up of only 2 months, did not show a reduction in mortality or heart failure hospitalizations. Based on the currently available published data, we will review what is already known about the use of these drugs in the early phases of acute heart failure and analyze their pathophysiological rationale from a practical perspective.
1. Upfront Utilization of SGLT2 Inhibitors in Acute Heart Failure
After the publication of the recent heart failure (HF) guidelines [1], SGLT2 inhibitors (SGLT2i) were recognized as one of the recommended treatments in patients with HF and reduced ejection fraction (HFrEF) irrespective of the presence of type 2 diabetes mellitus (class I recommendation, level of evidence A) due to the demonstrated reduction in mortality and hospitalization rates in these patients.
Shortly afterwards, important clinical evidence in favour of SGLT2i use in patients with HF and preserved ejection fraction (HFpEF) became available and it was taken up by the subsequently published [2,3] American and European guidelines. SGLT2is have indeed been shown to reduce cardiovascular mortality and hospitalizations for HF decompensation, even in the population of patients with HFpEF (recommendation class IIa, level of evidence B).
At variance with the strong evidence in the chronic HF setting, the management of the acute patient still leaves room for some doubt. Endocrinology and diabetes guidelines advise against SGLT2i use during hospitalizations for acute episodes due to the potential increase in adverse events such as genitourinary infections, euglycemic ketoacidosis, and acute renal failure [4,5,6]. The 2023 update of the European Society of Cardiology Heart Failure Guidelines introduced the possibility of using SGLT2is in acute HF based on the results of the EMPULSE study, but it did not provide any recommendations regarding the best time to start therapy (during hospitalization vs. at discharge) [7]. Conversely, the recently published update on the decision-making and management pathway for patients hospitalized for HF by the American College of Cardiology (ACC) clearly states that SGLT2i therapy can be started any time during HF hospitalization, regardless of ejection fraction (EF), while placing more emphasis on the initiation of the other pillars of HFrEF therapy only after stabilization [8].
For many years, drugs that have been tested for efficacy in the setting of acute HF have produced disappointing results, and the therapy of this condition is still largely based on the clinical experience of the attending cardiologist. The strong evidence of the efficacy and safety of the ‘four pillars’ of HFrEF therapy demonstrated in the registration trials has prompted the quest for the optimal timing and strategy to initiate such therapies. While expeditious introduction near hospital discharge and the rapid titration of drugs in the first month post-discharge were shown to reduce mortality and HF hospitalizations [9,10], it is less clear which drugs should be administered early during the decongestion phase of hospitalization. Beyond their long-term prognostic benefit, SGLT2is exhibit some peculiarities that might favour their use early during an acute HF admission, which include the following: 1. a potential synergistic effect with loop diuretics in achieving decongestion; 2. ease of use and a high safety and tolerability profile, with negligible effects on arterial blood pressure and no effect on heart rate; 3. the ability to counterbalance the risk of hyperkalemia associated with starting drugs that act on the renin–angiotensin–aldosterone axis (RAAS); and 4. the improvement in cardiomyocyte metabolism in a phase of high oxidative stress such as acute HF (Figure 1).
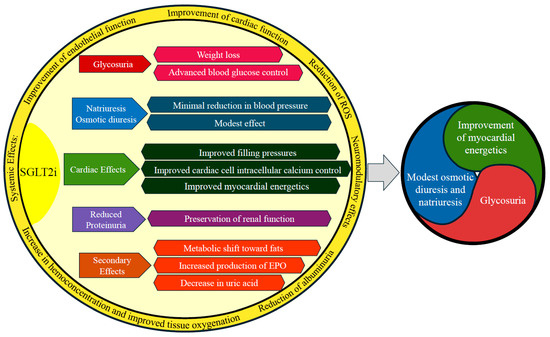
Figure 1.
Summary of the main effects of SGLT2is. Abbreviations: ROS, reactive oxygen species; EPO, erythropoietin.
In this review, we will examine the available data for the use of SGLT2is in the acute phase of HF, critically discuss the pathophysiological rationale for their use, and attempt to provide practical guidance.
2. Early Benefit from Trials on SGLT2is in Chronic HF
The data in favour of the use of SGLT2is in patients with chronic HF are robust. Both empaglifozin, in the EMPEROR-Reduced [2] and EMPEROR-Preserved [3] trials, and dapaglifozin, in the DAPA-HF [11] and DELIVER [12] trials, demonstrated significant reductions in the primary endpoint of cardiovascular mortality and HF hospitalization with respect to placebo across the range of reduced and preserved EF. Of particular relevance to their potential use in the acute HF stage was the documentation of early benefit after drug initiation. In DAPA-HF [11], the reduction in the primary outcome was already evident after 28 days of therapy (hazard ratio, 0.51; 95% confidence interval [CI], 0.28 to 0.94). In EMPEROR-Reduced [2], a statistically significant reduction in cardiovascular mortality emerged between the two arms (hazard ratio [HR] 0.42; 95% CI 0.19–0.92) after only 12 days of treatment start. The DELIVER [12] trial also enrolled inpatients hospitalized for acute HF (10.4%) and documented a reduction in the primary endpoint (HR 0.82, 95% CI 0.73–0.92; p < 0.001) in patients randomized to dapaglifozin vs. placebo both during a HF hospitalization and in a stable clinical state [13], without differences according to EF level or the presence or absence of diabetes. These large and early benefits, documented even in patients with a recent HF admission, have paved the way to an early use of SGLT2is in the acute HF stages.
3. Studies on the Use of SGLT2is in Acute Heart Failure
Several studies investigated the impact of SGLT2is during a hospitalization for acute HF or in the first 30 days after discharge (Table 1).

Table 1.
Summary of the main studies testing the use of SGLT2 inhibitors in patients with acute heart failure.
4. Empagliflozin
EMPAG-HF was the first randomized double-blind study to test the use of empagliflozin 25 mg or placebo in addition to standard decongestant therapy during the first 5 days of hospitalization for acute HF in 60 patients. The work showed a significant increase in total diuresis (10.8 litres vs. 8.7 litres; mean difference 2.2 litres; 95% CI 0.84–3.6; p = 0.003) and a better efficiency of the loop diuretic in terms of millilitres of diuresis/milligram of furosemide administered (8.3 mL/mg vs. −25.9 mL/mq; mean difference 43.7 mL/mg; 95% CI 0.1–0.93; p = 0.041) after 5 days of treatment compared to the placebo group [22].
The subsequent EMPA-RESPONSE-AHF trial randomized 80 patients, with and without diabetes, with clinical signs of congestion, need for intravenous diuretic therapy, and an NT-ProBNP ≥ 1400 pg/mL [15] to treatment with empagliflozin 10 mg or placebo within 24 h of admission for acute HF. No significant differences were documented in the primary endpoint, improvement in dyspnea according to a predetermined score, response to diuretic therapy, duration of hospitalization, and reduction in NT-ProBNP levels. However, the drug was well tolerated, and an increase in urinary volume and a reduction in HF episodes, re-hospitalizations for HF decompensation, and cardiovascular death at 60 days were observed. The results of this pilot trial formed the rationale for the recently published [16] double-blind, randomized EMPULSE study. This trial randomized 530 patients with newly diagnosed or relapsed HF to empagliflozin 10 mg or placebo. Of the 530 randomized patients, 361 had HFrEF and 169 HfpEF. The median time to randomisation was 3 days (range 2–4 days) since admission to hospital for HF. The primary endpoint was death from all causes, first HF hospitalization, total number of HF hospitalizations, and change from baseline of at least five points on the Kansas City Cardiomyopathy Questionnaire (KCCQ-TSS). The safety parameters taken into account were volume depletion, hypotension, and renal failure. Empagliflozin was superior to placebo in 53.9% of paired comparisons and placebo superior to empagliflozin in 39.7%. Empagliflozin benefit was independent of both HF type (de novo vs. recurrent) and EF (≤40% vs. >40%). The incidence of adverse events was overall lower in patients treated with empagliflozin compared to placebo, while the drug was discontinued due to adverse events in 8.5% and 13%, respectively.
5. Sotagliflozin
The SOLOIST-WHF study is a randomized double-blind trial that tested the use of sotagliflozin (SLGT2-SGLT1 inhibitor) vs. placebo in patients with type 2 diabetes mellitus hospitalized for acute HF [23]. The trial enrolled 1222 patients and 79% of these had an EF < 50%, so both patients with HFrEF and HFpEF were included. Treatment with sotagliflozin could be started as early as on the first day of hospitalization and no later than three days after discharge, after switching from intravenous to oral diuretics, in all hemodynamically stable patients with a systolic blood pressure above 100 mmHg. The trial was stopped early due to discontinuation of financial support by the sponsor but still demonstrated a reduction in the primary outcome, the composite of death from cardiovascular causes and emergency admissions/visits for HF, after a mean follow-up of 12 months (HR 0.67; 95% CI 0.52–0.85; p < 0.001). The primary outcome was predominantly determined by a reduction in emergency admissions/visits for HF (HR 0.64; 95% CI 0.49–0.83; p < 0.001). A higher incidence of episodes of diarrhea (6.9% vs. 4.1%, p = 0.032) and severe hypoglycemia (1.5% vs. 0.3%, p = 0.037) occurred in the sotagliflozin group. These latter adverse effects appear to be related to SGLT1 inhibition by sotagliflozin. A subsequent sub-analysis in patients starting sotagliflozin during an HF hospitalization also showed a reduction in total mortality at 30 and 90 days [14].
6. Dapagliflozin
The efficacy and safety of dapagliflozin on top of standard decongestion therapy in patients with de novo or exacerbated acute HF was initially tested in several small randomized trials. The primary endpoints of these studies were related to decongestion measures such as weight loss, improvement in dyspnea, reduction in NT-ProBNP levels, and efficiency of loop diuretics.
In the study by Ibrahim et al. [20], 100 patients with type 2 diabetes mellitus, LVEF≤ 40%, and a history of HF with an ongoing exacerbation (defined according to clinical criteria) were randomized to placebo or dapagliflozin 10 mg on top of conventional decongestion. The study showed an increase in urinary output in the dapagliflozin-treated group (18.46 ± 0.5 litres vs. 14.43 ± 0.7 litres; p < 0.001), better efficiency of the loop diuretic in terms of ml of diuresis/mg of furosemide administered (34.75 ± 2.2 mL/mg vs. 19.49 ± 1.2 mL/mg; p < 0.001), and a greater weight loss (76.51 ± 6.0 kg vs. 79.63 ± 8.9 kg, p = 0.046) against a non-statistically significant trend of worsening renal function in the dapagliflozin-arm (28 vs. 16%, p = 0.148). These results were more recently confirmed by the DAPA-RESPONSE-AHF and the DICTATE-AHF trials [17,19]. The DAPA-RESPONSE-AHF is a similarly designed double-blind trial that also included patients without type 2 diabetes mellitus and showed not only a reduction in congestion by adding dapagliflozin to standard therapy but also a reduction in re-hospitalizations at 30 days (p = 0.017). DICTATE-AHF tested the use of dapagliflozin in combination with a standardized titration of loop diuretic therapy in order to reach a daily diuresis between 3 and 5 litres. Unlike previous studies, which allowed liberal use of diuretic therapy, DICTATE-AHF standardized the use of the loop diuretic and excluded patients treated with doses ≥ 12.5 mg hydrochlorothiazide in order to avoid potential bias. No significant differences emerged with regard to the primary outcome of the study, which was the efficiency of diuretic therapy measured as a reduction in body weight in relation to the cumulative dose of loop diuretic after 5 days of therapy ((−0.42; interquartile range −0.52 to −0.33) Kg/40 mg furosemide vs. −0.31 (interquartile range −0.39 to −0.23) Kg/40 mg furosemide; mean difference 0.65: 95% CI 0.41–1.02; p = 0.06)). However, implementation in the first 24 h of dapagliflozin was safe. There was no increase in hypoglycemic episodes nor a significant worsening glomerular filtration rate (−2 mL vs. −3.2 mL; mean difference 1.06 mL: 95% CI 0.68–1.65; p = 0.79) and no episodes of euglycemic ketoacidosis were observed. Dapagliflozin was also compared with metolazone in patients with resistance to loop diuretics in the DAPA-RESIST study [18]. In this multicentre randomized study, 61 patients hospitalized for an acute HF exacerbation were randomized in the first 24 h of hospitalization to therapy with dapagliflozin 10 mg or metolazone 5–10 mg on top of standard decongestion for the first 3 days of hospitalization. The study did not show a statistically significant difference in the primary endpoint, weight loss at 96 h after hospitalization (−3 kg vs. −3.6 kg; mean difference 0.65 kg; 95% CI −0.12–1.41; p = 0.11), nor in the efficiency of diuretic therapy (−0.15 kg/40 mg furosemide vs. −0.25 kg/40 mg furosemide; mean difference −0.08: 95% CI −0.17–0.01; p = 0.11), but the increase in urea and creatinine was lower with dapagliflozin than with metolazone.
Recently, a larger randomized trial has tested dapagliflozin in the setting of acute HF. The DAPA ACT HF-TIMI 68 study, a randomized double-blind study, enrolled 2401 patients with acute HF to assess whether initiating dapagliflozin in the acute phase is able to reduce cardiovascular mortality or worsening HF, defined as deterioration during the index hospitalization, re-hospitalization, or urgent visit for HF in the first 2 months after discharge. Enrolment was independent of LVEF, presence of type 2 diabetes, and de novo or worsening chronic HF. Participants were randomized to blinded treatment for a 2-month period. Key safety endpoints comprise symptomatic hypotension and decline in renal function. The composite endpoint occurred in 10.9% of patients receiving dapagliflozin and 12.7% of those on placebo, with no statistically significant difference (HR 0.86; 95% CI 0.68–1.08; p = 0.20). All individual components of the composite primary endpoint were numerically lower with dapagliflozin but none reached statistical significance: cardiovascular mortality (2.5% vs. 3.1%; HR 0.78; 95% CI 0.48–1.27), all-cause mortality (3.0% vs. 4.5%; HR 0.66; 95% CI 0.43–1.00), and HF worsening (7.4% vs. 8.6%; HR 0.85; 95% CI 0.64–1.13). Finally, the safety endpoints were reassuring, with only modestly higher rates of symptomatic hypotension (3.6% vs. 2.2%) and numerically higher renal function decline (5.9% vs. 4.7%) among patients treated with dapagliflozin [21]. These data suggest that in more vulnerable populations, care should be taken to minimize other potential drivers of symptomatic hypotension, such as volume depletion or rapid escalation in the dosing of neurohormonal antagonists, when initiating SGLT2is.
All these data, together with the results of some meta-analyses [24,25], support the implementation of SGLT2is already during the early stages of HF hospitalization. As explicitly stated in the ACC document [8], SGLT2is and mineralocorticoid antagonists have little effect in reducing arterial blood pressure and, in the absence of contraindications, can be started at any time during hospitalization and continued after discharge. This would allow a subsequent rapid implementation of the other guideline-recommended treatment for HF. It is important to emphasize that in clinical practice, the implementation of such therapy is often not so rapid due to the fear that the combined effect of all the recommended drugs may not be tolerated. In particular, early and concomitant initiation of ARNI and SGLT2is could affect arterial blood pressure and renal function, which are a well-known and critical issue in these patients. Of note, neuromodulation through inhibition of the RAAS, neprilysin, and beta-adrenergic systems has potent effects on the circulation and requires careful titration compared to SGLT2 and MRA inhibitors, which have a trivial effect on reducing arterial blood pressure and do not impact cardiac output. Therefore, unlike SGLT2is, the introduction and optimization of neurohormonal modulation will depend mainly on the hospital course and the patient’s characteristics/profile during the hospital stay [26].
7. Mechanisms of SGLT2is in Acute Heart Failure
SGLT2is act primarily at the proximal tubule level, where they block sodium–glucose reabsorption via the SGLT2 co-transporter, thereby promoting osmotic diuresis. During acute decompensation, sympathetic hyperactivity upregulates renal SGLT2 expression, amplifying glycosuria in this setting [27]. In addition, SGLT2 activity modulates the sodium–hydrogen (NH3) exchanger at the proximal tubule; its inhibition contributes to reduced sodium reabsorption [28] (Figure 2A). However, SGLT2 and NH3 inhibition is rapidly counterbalanced by compensatory mechanisms at the loop of Henle and distal tubule, triggered by elevated sodium chloride delivery. These include increased aldosterone and vasopressin release, enhanced sodium and bicarbonate reabsorption through carbonic anhydrase, and vasoconstriction of the afferent arteriole reducing glomerular filtration. As a result, SGLT2is induce only a short-lived osmotic diuresis, followed by strong activation of water- and sodium-retaining mechanisms, particularly in patients with acute HF (Figure 2B). Thus, their direct decongestive effect appears physiologically modest [29].

Figure 2.
Site of action and main compensatory mechanism of SGLT2is. (A): Site of action of SGLT2is in the kidney. (B): Main compensatory mechanism of SGLT2is in patients with acute heart failure.
Studies assessing plasma volume have reported only modest reductions, which are later offset by increased red blood cell mass due to SGLT2i-induced erythropoiesis [30]. This mechanism also explains the limited effect on natriuretic peptide levels, which decline only slightly in acute HF [31]. Early studies suggested that SGLT2is may reduce extracellular volume more effectively than loop diuretics [32]. However, the decongestive action of loop diuretics results from plasma volume reduction, which promotes capillary refill from the interstitial space and increased lymphatic flow, ultimately leading to fluid excretion and edema resolution [33]. The hypothesis that SGLT2is sustain aquaresis and plasma osmolarity, thereby mobilizing edema, does not account for their erythropoiesis-driven plasma volume expansion and has not been confirmed by clinical data [28].
A more plausible pathophysiological mechanism for SGLT2is’ role in decongestion may lie in offsetting loop diuretic resistance. Resistance is driven by hypochloremia, which enhances sodium–potassium–chloride co-transporter activity at the loop of Henle, the target of loop diuretics. By raising chloride concentration at this site, SGLT2is may attenuate resistance, thereby augmenting loop diuretic efficacy. This effect is likely more significant in chronic HF, consistent with conflicting data on loop diuretic efficiency in acute settings with SGLT2i. Nonetheless, their efficacy, as shown in the DAPA-RESIST trial, remains inferior to the effect of thiazides within sequential nephron blockade, albeit with greater renal safety [18,34].
The EMPULSE trial, the largest to date evaluating empagliflozin in acute HF, reported significant benefits in a post hoc analysis: greater weight loss (−3.2 vs. −1.23 kg; mean difference −1.97 kg; 95% CI −2.86 to −1.08; p < 0.0001), improved loop diuretic efficiency (−3.33 vs. −1.02 kg/40 mg furosemide; mean difference −2.31 kg; 95% CI −3.77 to −0.85; p = 0.0020), reduced NT-proBNP (ratio of adjusted geometric mean 0.92; 95% CI 0.86–0.98; p = 0.0101), and improvement in congestion score (−1.78 vs. −1.43 points; mean difference −0.34; 95% CI −0.60 to −0.09; p = 0.0079) at 15 days [31]. However, urinary sodium or volume data were not presented. Thus, it remains uncertain whether these results reflect direct decongestion (free water/sodium excretion) or rather weight loss driven by glycosuria and concomitant caloric restriction in acutely decompensated patients [35]. Overall, the evidence suggests a modest decongestive role for SGLT2i.
Importantly, the early clinical benefits of SGLT2i in acute HF may be mediated by direct effects on the cardiomyocyte. By mimicking fasting, they enhance fatty acid and ketone body metabolism, reduce oxidative stress, promote autophagy, and ultimately protect cardiomyocytes. In acute HF, these mechanisms may translate into reduced re-hospitalization and mortality as early as 30 days after therapy initiation [25]. For this reason, even if their decongestive capacity is limited, early initiation during hospitalization is essential. In a patient is already on SGLT2i therapy, continuation during decompensation appears reasonable—provided that the patient is hemodynamically stable and has no clear contraindications such as severe renal deterioration (Figure 3) [36,37]. In Table 2, we have summarized the advantages and disadvantages of SGLT2i therapy usage.
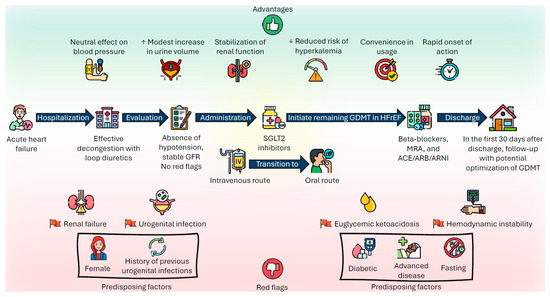
Figure 3.
Practical approach to the use of SGLT2is in patients with acute decompensated heart failure.
Table 2.
Benefits and drawbacks of SGLT2i therapy.
8. Red Flags for Deferred Use
Safety is among the features that have emerged most robustly from the clinical trials that have tested SGLT2is in all their fields of application. However, there are clinical scenarios in which initiation should be postponed in order to avoid adverse effects that, although rare, can sometimes be serious:
1. Hemodynamic instability: SGLT2 inhibitors have not been tested in hemodynamically unstable patients and therefore these drugs should not be started in patients requiring inotropes, vasopressors, intravenous vasodilators, or short-term mechanical circulatory support. It appears advisable to start SGLT2is when systolic blood pressure is above 95 mmHg, in the absence of hypotensive episodes for at least 12 h [24,28].
2. Renal insufficiency: Dapagliflozin and empagliflozin have been shown to be safe down to a glomerular filtration rate of 25 and 20 mL/min, respectively, and to slow the progressive deterioration of renal function in chronic patients. In the acute phase, and particularly during intravenous diuretic therapy, the risk of volume depletion associated with loop diuretics and/or sequential nephron blockade may cause acute renal failure. Starting SGLT2is during an acute decompensation hospitalization should therefore be postponed in case of excessive fluid depletion. Monitoring of fluid status and renal function during hospitalization is crucial, particularly in the case of concomitant initiation of sacubitril/valsartan [24].
3. Genitourinary tract infections: Diabetic patients, women, and patients with obesity had a higher incidence of urinary tract infections in trials. Such events were infrequent in studies testing SGLT2is in the acute phase. It is recommended to postpone SGLT2i initiation in case of ongoing genitourinary tract infections, particularly in subjects with recurrent episodes, patients with diabetes, or with other predisposing factors for infections [24].
4. Euglycemic ketoacidosis: This is an extremely rare but potentially fatal complication, particularly in patients with acute HF. In this phase, the coexistence of prolonged fasting and hypotension can cause an insulin deficit that favours the onset of ketoacidosis. This condition is almost exclusive to insulin-treated diabetics and occurred in 2 patients out of the approximately 900 included in the SOLOIST-WHF, EMPULSE, and EMPA-RESPONSE-AHF studies. Awareness of its possible occurrence is crucial in order to institute prompt treatment. To prevent the risk of euglycemic ketoacidosis, SGLT2is should be started after resumption of oral feeding in patients admitted for acute HF decompensation [24].
5. The data available until now on heart and kidney transplant recipients treated with SGLT2is seems to be promising in this subgroup of patients as well; however, the risk of genitourinary infections could be higher in this population due to their chronic immunosuppressant drug regimen.
In Figure 4, we have summarized a practical flowchart for initiating SGLT2 inhibitors in patients with acute HF.
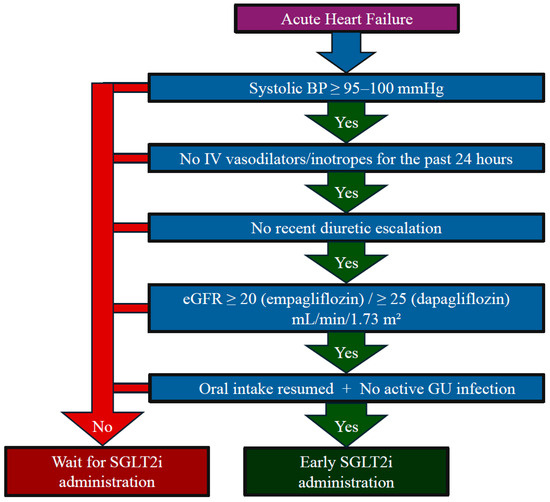
Figure 4.
Flowchart for practical use of SGLT2is in patients with acute heart failure.
9. Conclusions
Acute HF is a frequent cause of emergency room admission and hospitalization, associated with high in-hospital mortality and short-term re-hospitalization. Therapeutic optimization and early treatment are the key to reducing these adverse outcomes. The use of SGLT2is in patients with acute HF is reassuring, and their use appears to be safe. Moreover, although studies show a rather modest direct decongestive effect, early introduction should always be pursued, in the absence of contraindications, as it brings prognostic advantages and facilitates the introduction of the other guideline-recommended treatments for heart failure.
Author Contributions
M.B. and C.D.N. contributed to the conceptualization, validation, methodology, data curation, and writing—original draft preparation. R.D.M., A.H.M. and S.C. contributed to conceptualization, methodology, formal analysis, and project administration. L.D.G., P.M., M.V.M., V.R., M.D.T., G.G., A.I., F.C., M.G. and F.O. contributed to conceptualization, formal analysis, and writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
The APC was funded by Associazione Medici Cardiologi Ospedalieri (ANMCO).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 16. Diabetes Care in the Hospital: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46 (Suppl. S1), S267–S278. [Google Scholar] [CrossRef] [PubMed]
- Korytkowski, M.T.; Muniyappa, R.; Antinori-Lent, K.; Donihi, A.C.; Drincic, A.T.; Hirsch, I.B.; Luger, A.; McDonnell, M.E.; Murad, M.H.; Nielsen, C.; et al. Management of Hyperglycemia in Hospitalized Adult Patients in Non-Critical Care Settings: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2022, 107, 2101–2128. [Google Scholar] [CrossRef]
- Pasquel, F.J.; Lansang, M.C.; Dhatariya, K.; Umpierrez, G.E. Management of diabetes and hyperglycaemia in the hospital. Lancet Diabetes Endocrinol. 2021, 9, 174–188. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, S.M.; Stevenson, L.W.; Ahmad, T.; Bozkurt, B.; Butler, J.; Davis, L.L.; Drazner, M.H.; Kirkpatrick, J.N.; Morris, A.A.; Page, R.L., 2nd; et al. 2024 ACC Expert Consensus Decision Pathway on Clinical Assessment, Management, and Trajectory of Patients Hospitalized with Heart Failure Focused Update: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2024, 84, 1241–1267. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Straus, S.E.; Farkouh, M.E.; Austin, P.C.; Taljaard, M.; Chong, A.; Fahim, C.; Poon, S.; Cram, P.; Smith, S.; et al. Trial of an Intervention to Improve Acute Heart Failure Outcomes. N. Engl. J. Med. 2023, 388, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Davison, B.; Chioncel, O.; Cohen-Solal, A.; Diaz, R.; Filippatos, G.; Metra, M.; Ponikowski, P.; Sliwa, K.; Voors, A.A.; et al. Safety, tolerability and efficacy of up-titration of guideline-directed medical therapies for acute heart failure (STRONG-HF): A multinational, open-label, randomised, trial. Lancet Lond. Engl. 2022, 400, 1938–1952. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Solomon, S.D.; Vaduganathan, M.; Claggett, B.L.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Cunningham, J.W.; Vaduganathan, M.; Claggett, B.L.; Kulac, I.J.; Desai, A.S.; Jhund, P.S.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; et al. Dapagliflozin in Patients Recently Hospitalized with Heart Failure and Mildly Reduced or Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2022, 80, 1302–1310. [Google Scholar] [CrossRef]
- Pitt, B.; Bhatt, D.L.; Szarek, M.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Effect of Sotagliflozin on Early Mortality and Heart Failure-Related Events: A Post Hoc Analysis of SOLOIST-WHF. JACC Heart Fail. 2023, 11 Pt 1, 879–889. [Google Scholar] [CrossRef]
- Damman, K.; Beusekamp, J.C.; Boorsma, E.M.; Swart, H.P.; Smilde, T.D.J.; Elvan, A.; van Eck, J.W.M.; Heerspink, H.J.L.; Voors, A.A. Randomized, double-blind, placebo-controlled, multicentre pilot study on the effects of empagliflozin on clinical outcomes in patients with acute decompensated heart failure (EMPA-RESPONSE-AHF). Eur. J. Heart Fail. 2020, 22, 713–722. [Google Scholar] [CrossRef]
- Damman, K.; Beusekamp, J.C.; Boorsma, E.M.; Swart, H.P.; Smilde, T.D.J.; Elvan, A.; van Eck, J.W.M.; Heerspink, H.J.L.; Voors, A.A. The SGLT2 inhibitor empagliflozin in patients hospitalized for acute heart failure: A multinational randomized trial. Nat. Med. 2022, 28, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Emara, A.N.; Wadie, M.; Mansour, N.O.; Shams, M.E.E. The clinical outcomes of dapagliflozin in patients with acute heart failure: A randomized controlled trial (DAPA-RESPONSE-AHF). Eur. J. Pharmacol. 2023, 961, 176179. [Google Scholar] [CrossRef]
- Yeoh, S.E.; Osmanska, J.; Petrie, M.C.; Brooksbank, K.J.M.; Clark, A.L.; Docherty, K.F.; Foley, P.W.X.; Guha, K.; Halliday, C.A.; Jhund, P.S.; et al. Dapagliflozin vs. metolazone in heart failure resistant to loop diuretics. Eur. Heart J. 2023, 44, 2966–2977. [Google Scholar] [CrossRef] [PubMed]
- Cox, Z.L.; Collins, S.P.; Hernandez, G.A.; McRae, A.T., 3rd; Davidson, B.T.; Adams, K.; Aaron, M.; Cunningham, L.; Jenkins, C.A.; Lindsell, C.J.; et al. Efficacy and Safety of Dapagliflozin in Patients With Acute Heart Failure. J. Am. Coll. Cardiol. 2024, 83, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Ghaleb, R.; Mansour, H.; Hanafy, A.; Mahmoud, N.M.; Abdelfatah Elsharef, M.; Kamal Salama, M.; Elsaughier, S.M.; Abdel-Wahid, L.; Embarek Mohamed, M.; et al. Safety and Efficacy of Adding Dapagliflozin to Furosemide in Type 2 Diabetic Patients With Decompensated Heart Failure and Reduced Ejection Fraction. Front. Cardiovasc. Med. 2020, 7, 602251. [Google Scholar] [CrossRef]
- Berg, D.D.; Patel, S.M.; Haller, P.M.; Cange, A.L.; Palazzolo, M.G.; Bellavia, A.; Kuder, J.F.; Desai, A.S.; Inzucchi, S.E.; McMurray, J.J.V.; et al. Dapagliflozin in Patients Hospitalized for Heart Failure: Primary Results of the DAPA ACT HF-TIMI 68 Randomized Clinical Trial and Meta-Analysis of Sodium-Glucose Cotransporter-2 Inhibitors in Patients Hospitalized for Heart Failure. Circulation 2025. [Google Scholar] [CrossRef] [PubMed]
- Schulze, P.C.; Bogoviku, J.; Westphal, J.; Aftanski, P.; Haertel, F.; Grund, S.; von Haehling, S.; Schumacher, U.; Möbius-Winkler, S.; Busch, M. Effects of Early Empagliflozin Initiation on Diuresis and Kidney Function in Patients with Acute Decompensated Heart Failure (EMPAG-HF). Circulation 2022, 146, 289–298. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Morillas, H.; Galcerá, E.; Alania, E.; Seller, J.; Larumbe, A.; Núñez, J.; Valle, A. Sodium-glucose Co-transporter 2 Inhibitors in Acute Heart Failure: A Review of the Available Evidence and Practical Guidance on Clinical Use. Rev. Cardiovasc. Med. 2022, 23, 139. [Google Scholar] [CrossRef]
- Carvalho, P.E.P.; Veiga, T.M.A.; Simões ESilva, A.C.; Gewehr, D.M.; Dagostin, C.S.; Fernandes, A.; Nasi, G.; Cardoso, R. Cardiovascular and renal effects of SGLT2 inhibitor initiation in acute heart failure: A meta-analysis of randomized controlled trials. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2023, 112, 1044–1055. [Google Scholar] [CrossRef]
- Cox, Z.L.; Nandkeolyar, S.; Johnson, A.J.; Lindenfeld, J.; Rali, A.S. In-hospital Initiation and Up-titration of Guideline-directed Medical Therapies for Heart Failure with Reduced Ejection Fraction. Card. Fail. Rev. 2022, 8, e21. [Google Scholar] [CrossRef]
- Boorsma, E.M.; Beusekamp, J.C.; Ter Maaten, J.M.; Figarska, S.M.; Danser, A.H.J.; van Veldhuisen, D.J.; van der Meer, P.; Heerspink, H.J.L.; Damman, K.; Voors, A.A. Effects of empagliflozin on renal sodium and glucose handling in patients with acute heart failure. Eur. J. Heart Fail. 2021, 23, 68–78. [Google Scholar] [CrossRef]
- Packer, M.; Wilcox, C.S.; Testani, J.M. Critical Analysis of the Effects of SGLT2 Inhibitors on Renal Tubular Sodium, Water and Chloride Homeostasis and Their Role in Influencing Heart Failure Outcomes. Circulation 2023, 148, 354–372. [Google Scholar] [CrossRef]
- Marton, A.; Saffari, S.E.; Rauh, M.; Sun, R.N.; Nagel, A.M.; Linz, P.; Lim, T.T.; Takase-Minegishi, K.; Pajarillaga, A.; Saw, S.; et al. Water Conservation Overrides Osmotic Diuresis During SGLT2 Inhibition in Patients with Heart Failure. J. Am. Coll. Cardiol. 2024, 83, 1386–1398. [Google Scholar] [CrossRef]
- Omar, M.; Jensen, J.; Burkhoff, D.; Frederiksen, P.H.; Kistorp, C.; Videbæk, L.; Poulsen, M.K.; Gustafsson, F.; Køber, L.; Borlaug, B.A.; et al. Effect of Empagliflozin on Blood Volume Redistribution in Patients with Chronic Heart Failure and Reduced Ejection Fraction: An Analysis from the Empire HF Randomized Clinical Trial. Circ. Heart Fail. 2022, 15, e009156. [Google Scholar] [CrossRef] [PubMed]
- Biegus, J.; Voors, A.A.; Collins, S.P.; Kosiborod, M.N.; Teerlink, J.R.; Angermann, C.E.; Tromp, J.; Ferreira, J.P.; Nassif, M.E.; Psotka, M.A.; et al. Impact of empagliflozin on decongestion in acute heart failure: The EMPULSE trial. Eur. Heart J. 2023, 44, 41–50. [Google Scholar] [CrossRef]
- Hallow, K.M.; Helmlinger, G.; Greasley, P.J.; McMurray, J.J.V.; Boulton, D.W. Why do SGLT2 inhibitors reduce heart failure hospitalization? A differential volume regulation hypothesis. Diabetes Obes. Metab. 2018, 20, 479–487. [Google Scholar] [CrossRef]
- Itkin, M.; Rockson, S.G.; Burkhoff, D. Pathophysiology of the Lymphatic System in Patients with Heart Failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 278–290. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, C.S.; Shen, W.; Boulton, D.W.; Leslie, B.R.; Griffen, S.C. Interaction Between the Sodium-Glucose-Linked Transporter 2 Inhibitor Dapagliflozin and the Loop Diuretic Bumetanide in Normal Human Subjects. J. Am. Heart Assoc. 2018, 7, e007046. [Google Scholar] [CrossRef]
- Ferrannini, G.; Hach, T.; Crowe, S.; Sanghvi, A.; Hall, K.D.; Ferrannini, E. Energy Balance After Sodium-Glucose Cotransporter 2 Inhibition. Diabetes Care 2015, 38, 1730–1735. [Google Scholar] [CrossRef]
- Nakagaito, M.; Imamura, T.; Joho, S.; Ushijima, R.; Nakamura, M.; Kinugawa, K. Efficacy of Continuing SGLT2 Inhibitors on Outcomes in Patients with Acute Decompensated Heart Failure. Int. Heart J. 2021, 62, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Butler, J.; Zeller, C.; Pocock, S.J.; Brueckmann, M.; Ferreira, J.P.; Filippatos, G.; Usman, M.S.; Zannad, F.; Anker, S.D. Blinded Withdrawal of Long-Term Randomized Treatment with Empagliflozin or Placebo in Patients with Heart Failure. Circulation 2023, 148, 1011–1022. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).