
Spanish Validation of the Problem Area in Diabetes-Pediatric Version Survey and Its Weak Association with Metabolic Control Parameters in Pediatric Diabetes: A Cross-Sectional Multicenter Study
 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design, Setting, and Participants
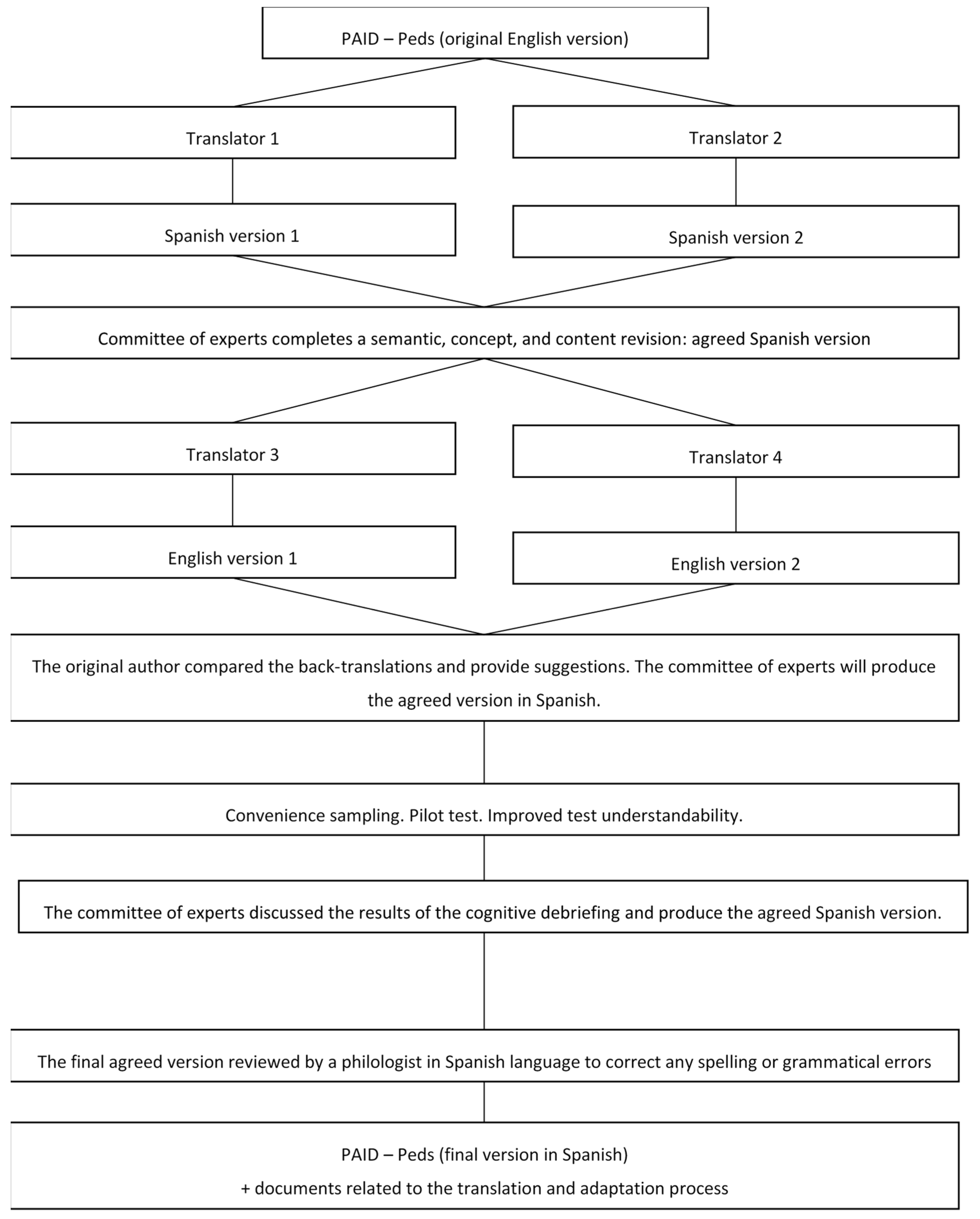
2.2. Instrument with Validity and Reliability
2.3. Sampling and Recruitment
2.4. Data Sources/Collection
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Demographic and Clinical Characteristics of Participants
3.2. Incidence of Acute Descompensations, Therapeutic Regimen, and Medical Background
3.3. Survey Score, Response Time, Correlations, and Multivariate Regression Analysis of PAID-Peds and Metabolic Control Parameters
3.4. Response Distribution for Survey Items and Sex
3.5. Reliability Analysis and Model Fit
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Libman, I.; Haynes, A.; Lyons, S.; Pradeep, P.; Rwagasor, E.; Tung, J.Y.; Jefferies, C.A.; Oram, R.A.; Dabelea, D.; Craig, M.E. ISPAD Clinical Practice Consensus Guidelines 2022: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr. Diabetes 2022, 23, 1160–1174. [Google Scholar] [CrossRef] [PubMed]
- Gregory, G.A.; Robinson, T.I.G.; Linklater, S.E.; Wang, F.; Colagiuri, S.; de Beaufort, C.; Donaghue, K.C.; Magliano, D.J.; Maniam, J.; Orchard, T.J.; et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: A modelling study. Lancet Diabetes Endocrinol. 2022, 10, 741–760. [Google Scholar] [CrossRef] [PubMed]
- Dennick, K.; Sturt, J.; Speight, J. What is diabetes distress and how can we measure it? A narrative review and conceptual model. J. Diabetes Complicat. 2017, 31, 898–911. [Google Scholar] [CrossRef] [PubMed]
- Stahl-Pehe, A.; Landwehr, S.; Lange, K.S.; Bächle, C.; Castillo, K.; Yossa, R.; Lüdtke, J.; Holl, R.W.; Rosenbauer, J. Impact of quality of life (QoL) on glycemic control (HbA1c) among adolescents and emerging adults with long-duration type 1 diabetes: A prospective cohort-study. Pediatr. Diabetes 2017, 18, 808–816. [Google Scholar] [CrossRef]
- Iturralde, E.; Rausch, J.R.; Weissberg-Benchell, J.; Hood, K.K. Diabetes-Related Emotional Distress Over Time. Pediatrics 2019, 143, e20183011. [Google Scholar] [CrossRef]
- Skinner, T.C.; Joensen, L.; Parkin, T. Twenty-five years of diabetes distress research. Diabet. Med. 2020, 37, 393–400. [Google Scholar] [CrossRef]
- Eilander, M.M.A.; Snoek, F.J.; Rotteveel, J.; Aanstoot, H.-J.; Bakker-van Waarde, W.M.; Houdijk, E.C.A.M.; Nuboer, R.; Winterdijk, P.; De Wit, M. Parental Diabetes Behaviors and Distress Are Related to Glycemic Control in Youth with Type 1 Diabetes: Longitudinal Data from the DINO Study. J. Diabetes Res. 2017, 2017, 1462064. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Rico, I.; Pérez-Marín, M.; Montoya-Castilla, I. Type 1 Diabetes mellitus: Brief review of the main associated psychological factors. Pediatr. Engl. Ed. 2015, 82, e143–e146. [Google Scholar] [CrossRef]
- Iturralde, E.; Hood, K.K.; Weissberg-Benchell, J.; Anderson, B.J.; Hilliard, M.E. Assessing strengths of children with type 1 diabetes: Validation of the Diabetes Strengths and Resilience (DSTAR) measure for ages 9 to 13. Pediatr. Diabetes 2019, 20, 1007–1015. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee; ElSayed, N.A.; Aleppo, G.; Bannuru, R.R.; Bruemmer, D.; Collins, B.S.; Ekhlaspour, L.; Hilliard, M.E.; Johnson, E.L.; Khunti, K.; et al. 14. Children and Adolescents: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47, S258–S281. [Google Scholar] [CrossRef]
- Weissberg-Benchell, J.; Shapiro, J.B.; Bryant, F.B.; Hood, K.K. Supporting Teen Problem-Solving (STEPS) 3 year outcomes: Preventing diabetes-specific emotional distress and depressive symptoms in adolescents with type 1 diabetes. J. Consult. Clin. Psychol. 2020, 88, 1019–1031. [Google Scholar] [CrossRef]
- Weldring, T.; Smith, S.M.S. Article Commentary: Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv. Insights 2013, 6, 61–68. [Google Scholar] [CrossRef]
- Lee, J.; Lee, E.H.; Chae, D.; Kim, C.J. Patient-reported outcome measures for diabetes self-care: A systematic review of measurement properties. Int. J. Nurs. Stud. 2020, 105, 103498. [Google Scholar] [CrossRef]
- Martin-Delgado, J.; Guilabert, M.; Mira-Solves, J. Patient-Reported Experience and Outcome Measures in People Living with Diabetes: A Scoping Review of Instruments. Patient 2021, 14, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Ling Wee, P.J.; Kwan, Y.H.; Fang Loh, D.H.; Phang, J.K.; Puar, T.H.; Østbye, T.; Thumboo, J.; Yoon, S.; Leng Low, L. Measurement properties of patient-reported outcome measures for diabetes: Systematic review. J. Med. Internet Res. 2021, 23, e25002. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQLTM 4.0: Reliability and Validity of the Pediatric Quality of Life InventoryTM Version 4.0 Generic Core Scales in Healthy and Patient Populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.M.W.S.; Al-Yahyawi, N.Y.; Choi, H.S.; Stewart, L.L.; Bone, J.N.; Tang, T.S.; Amed, S. Diabetes Distress and Transition Readiness in Youths with Type 1 Diabetes Transitioning from Pediatric to Adult Care. Pediatr. Diabetes 2023, 2023, 5580180. [Google Scholar] [CrossRef]
- Markowitz, J.T.; Volkening, L.K.; Butler, D.A.; Antisdel-Lomaglio, J.; Anderson, B.J.; Laffel, L.M.B. Re-examining a measure of diabetes-related burden in parents of young people with Type 1 diabetes: The Problem Areas in Diabetes Survey—Parent Revised version (PAID-PR). Diabet. Med. 2012, 29, 526–530. [Google Scholar] [CrossRef]
- Carey, M.P.; Jorgensen, R.S.; Weinstock, R.S.; Sprafkin, R.P.; Lantinga, L.J.; Carnrike, C.L.M.; Baker, M.T.; Meisler, A.W. Reliability and validity of the Appraisal of Diabetes Scale. J. Behav. Med. 1991, 14, 43–50. [Google Scholar] [CrossRef]
- Bradley, C.; Todd, C.; Gorton, T.; Symonds, E.; Martin, A.; Plowright, R. The development of an individualized questionnaire measure of perceived impact of diabetes on quality of life: The ADDQoL. Qual. Life Res. 1999, 8, 79–91. [Google Scholar] [CrossRef]
- Meadows, K.; Steen, N.; McColl, E.; Eccles, M.; Shiels, C.; Hewison, J.; Hutchinson, A. The Diabetes Health Profile (DHP): A New instrument for assessing the psychosocial profile of insulin requiring patients? Development and psychometric evaluation. Qual. Life Res. 1996, 5, 242–254. [Google Scholar] [CrossRef]
- Sari, S.A.; Agadayi, E.; Celik, N.; Karahan, S.; Komurluoglu Tan, A.; Doger, E. The Turkish version of the problem areas in diabetes-parents of teens (P-PAID-T): Cross-cultural adaptation, reliability, and validity. J. Pediatr. Nurs. 2023, 73, e146–e153. [Google Scholar] [CrossRef]
- Saßmann, H.; Kim-Dorner, S.-J.; Framme, J.; Heidtmann, B.; Kapellen, T.; Kordonouri, O.; Krosta, K.M.E.; Pisarek, N.; Lange, K. Psychometric properties of the German teen and parent versions of the Problem Areas in Diabetes Scale (PAID). Psychol. Assess. 2023, 35, e31–e42. [Google Scholar] [CrossRef] [PubMed]
- Rahbæk, M.Ø.; Jensen, S.D.; Hansen, K.K.; Sandbæk, A.; Lund, S.; Andersen, A. The Danish Version of the Problem Areas in Diabetes-Teen (PAID-T) Scale: Translation and Linguistic Validation. Pediatr. Diabetes 2023, 2023, 4655563. [Google Scholar] [CrossRef]
- Markowitz, J.T.; Volkening, L.K.; Butler, D.A.; Laffel, L.M.B. Youth-Perceived Burden of Type 1 Diabetes. J. Diabetes Sci. Technol. 2015, 9, 1080–1085. [Google Scholar] [CrossRef] [PubMed]
- Commissariat, P.; Tinsley, L.; Volkening, L.; Butler, D.; Anderson, B.; Laffel, L. Establishing a Clinical Cut-Point for the PAID-Peds (Problem Areas in Diabetes-Pediatric) Survey. Diabetes 2018, 67, 795-P. [Google Scholar] [CrossRef]
- Casanovas-Marsal, J.; Monzón, E.C.; Duce, M.P.F.; de la Cuesta, D.G.; Valverde, R.Y.; Repiso, V.P.; Manterola, I.G.; Muñoz, A.d.A. Study protocol of translation into Spanish and cross-cultural adaptation and validation of the problem areas in diabetes—Pediatric version (PAID-Peds) survey. Nurs. Open 2024, 11, e2128. [Google Scholar] [CrossRef]
- Casanovas-Marsal, J.-O.; Monzón, E.C.; Duce, M.P.F.; Lozano, M.F.; Callau, M.V.; de la Cuesta, D.G.; Valverde, R.Y.; Repiso, V.P.; Manterola, I.G.; Muñoz, A.d.A. Translation and psychometric evaluation of the Spanish version of the problem areas in diabetes–pediatric version (PAID-Peds) survey. Diabetol. Metab. Syndr. 2023, 15, 219. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P.; ISPOR Task Force for Translation and Cultural Adaptation. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Carrascosa Lezcano, A.; Fernández García, J.M.; Fernández Ramos, C.; Ferrández Longás, A.; López-Siguero, J.P.; Sánchez González, E.; Sobradillo Ruiz, B.; Yeste Fernández, D.; Español, G.C. Estudio transversal español de crecimiento 2008. Parte II: Valores de talla, peso e índice de masa corporal desde el nacimiento a la talla adulta. Ann. Pediatr. (Engl. Ed). 2008, 68, 552–569. [Google Scholar] [CrossRef] [PubMed]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Sörbom, D. Testing Structural Equation Models Statistical models with latent variables: Testing the limits of sample size and model fit. Vol. Sage. 1993. [Google Scholar]
- Steiger, J.H. Structural Model Evaluation and Modification: An Interval Estimation Approach. Multivar. Behav. Res. 1990, 1, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Browne, M.W.; Cudeck, R. Testing Structural Equation Models: Alternative Ways of Assessing Model Fit; Sage: Thousand Oaks, CA, USA, 1993. [Google Scholar]
- Young-Hyman, D.; de Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Psychosocial Care for People With Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2126–2140. [Google Scholar] [CrossRef]
- Hagger, V.; Hendrieckx, C.; Cameron, F.; Pouwer, F.; Skinner, T.C.; Speight, J. Diabetes distress is more strongly associated with HbA1c than depressive symptoms in adolescents with type 1 diabetes: Results from Diabetes MILES Youth-Australia. Pediatr. Diabetes 2018, 19, 840–847. [Google Scholar] [CrossRef] [PubMed]
- de Bock, M.; Codner, E.; Craig, M.E.; Huynh, T.; Maahs, D.M.; Mahmud, F.H.; Marcovecchio, L.; DiMeglio, L.A. ISPAD Clinical Practice Consensus Guidelines 2022: Glycemic targets and glucose monitoring for children, adolescents, and young people with diabetes. Pediatr. Diabetes 2022, 23, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.; Byrne, M.; Casey, D.; Gillespie, P.; Hobbins, A.; Newell, J.; Morrissey, E.; Dinneen, S.F. Improving Outcomes Among Young Adults with type 1 diabetes: The D1 Now Randomised Pilot Study Protocol. Diabet. Med. 2020, 37, 1590–1604. [Google Scholar] [CrossRef] [PubMed]
- Vesco, A.T.; Jedraszko, A.M.; Garza, K.P.; Weissberg-Benchell, J. Continuous Glucose Monitoring Associated With Less Diabetes-Specific Emotional Distress and Lower A1c Among Adolescents With Type 1 Diabetes. J. Diabetes Sci. Technol. 2018, 12, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Godoi, A.; Marques, I.R.; Padrão, E.M.H.; Mahesh, A.; Hespanhol, L.C.; Júnior, J.E.R.L.; de Souza, I.A.F.; Moreira, V.C.S.; Silva, C.H.; Miyawaki, I.A.; et al. Glucose control and psychosocial outcomes with use of automated insulin delivery for 12 to 96 weeks in type 1 diabetes: A meta-analysis of randomised controlled trials. Diabetol. Metab. Syndr. 2023, 15, 190. [Google Scholar] [CrossRef] [PubMed]
- Kim-Dorner, S.-J.; Saßmann, H.; Framme, J.R.; Heidtmann, B.; Kapellen, T.M.; Kordonouri, O.; Nettelrodt, K.M.E.; Pisarek, N.; Schweizer, R.; von Sengbusch, S.; et al. Psychometric properties of the German versions of the Problem Areas in Diabetes Scale for Children (PAID-C) with Type 1 Diabetes and Their Parents (P-PAID-C). Psychol. Assess. 2024, 36, e38–e50. [Google Scholar] [CrossRef] [PubMed]
- Hilliard, M.E.; De Wit, M.; Wasserman, R.M.; Butler, A.M.; Evans, M.; Weissberg-Benchell, J.; Anderson, B.J. Screening and support for emotional burdens of youth with type 1 diabetes: Strategies for diabetes care providers. Pediatr. Diabetes 2018, 19, 534–543. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Original | Translation 1 Version 1 | Translation 2 Version 2 | Reconciliation and Synthesis | Back-Translation 3 Version 1 | Back-Translation 4 Version 2 | Final Report Revised by Hispanic Philologist |
|---|---|---|---|---|---|---|
| Problem Areas in Diabetes-Pediatric (Paid-Peds) Survey | Áreas Problemáticas en la Diabetes (Paid)-Cuestionario Pediátrico (Paid-Peds) | Áreas Problemáticas en la Diabetes-Cuestionario Pediátrico (Paid-Peds) | Áreas Problemáticas en la Diabetes (Paid)-Cuestionario Pediátrico (Paid-Peds) | Problem Areas in Diabetes (Paid)-Pediatric Questionnaire (Paid-Peds) | Problem Areas in Diabetes (Paid)-Paediatric (Paid-Peds) Survey | Aspectos Problemáticos de la Diabetes (Paid)-Cuestionario Pediátrico (Paid-Peds) |
| The following statements describe diabetes-related issues that may or may not be a concern for you. For each item, choose the ONE answer that best describes how much you agree or disagree with that statement. | Las siguientes afirmaciones describen cuestiones relacionadas con la diabetes que pueden suponer un problema para ti o no. Elige la respuesta que mejor describa tu grado de acuerdo o desacuerdo con la afirmación de cada ítem. | Las siguientes afirmaciones describen aspectos relacionados con la diabetes que pueden preocuparte o no. En cada ítem, elige la respuesta que describe mejor tu nivel de acuerdo o desacuerdo con la afirmación. | Las siguientes afirmaciones describen cuestiones relacionadas con la diabetes que pueden suponer un problema para ti o no. Elige la respuesta que mejor describa tu grado de acuerdo o desacuerdo con la afirmación de cada ítem. | The following statements describe aspects related to diabetes that may or may not represent a problem for you. Choose the answer that best describes your degree of agreement or disagreement with the statement for each item. | The following statements describe diabetes-related issues that may or may not be a problem for you. Choose the answer that best describes your degree of agreement or disagreement with the statement in each item. | Las siguientes afirmaciones describen cuestiones relacionadas con la diabetes que pueden suponer o no un problema para ti. Elige la respuesta que mejor describa tu grado de acuerdo o desacuerdo con la afirmación de cada punto. |
| 1. I feel sad a lot when I think about having diabetes. | 1. Me pongo muy triste cuando pienso que tengo diabetes. | 1. Me entristece mucho pensar que tengo diabetes. | 1. Me pongo muy triste cuando pienso que tengo diabetes. | 1. I get very sad when I think I have diabetes. | 1. I feel very sad when I think about having diabetes. | 1. Me pongo muy triste cuando pienso en que tengo diabetes. |
| 2. I feel like diabetes has taken over my life. | 2. Tengo la sensación de que la diabetes controla mi vida. | 2. Siento como si la diabetes hubiera tomado el control de mi vida. | 2. Siento que la diabetes controla mi vida. | 2. I feel that diabetes controls my life. | 2. I feel like diabetes has taken control of my life. | 2. Siento que la diabetes controla mi vida. |
| 3. I feel like it is my fault when my blood sugar is out of range. | 3. Siento que es mi culpa cuando mi nivel de glucosa está fuera de rango. | 3. Siento que es mi culpa cuando mi azúcar en sangre está fuera de los límites normales. | 3. Siento que es mi culpa cuando mi nivel de azúcar está fuera de rango. | 3. I feel that it is my fault when my blood sugar is out of range. | 3. I feel it is my fault when my blood sugar is out of range. | 3. Siento que es mi culpa cuando mi nivel de azúcar está fuera de rango. |
| 4. It bothers me to think so much about what I eat. | 4. Me molesta pensar tanto lo que como. | 4. Me fastidia tener que estar pensando lo que como. | 4. Me molesta tener que estar pensando lo que como. | 4. It annoys me to have to think about what I eat. | 4. It bothers me to have to think about what I eat. | 4. Me molesta tener que estar pensando en lo que como. |
| 5. I worry all the time about how diabetes will affect me when I am older. | 5. Me preocupa todo el tiempo cómo me afectará la diabetes cuando sea mayor. | 5. Me preocupo constantemente por cómo me afectará la diabetes de mayor. | 5. Me preocupo constantemente por cómo me afectará la Diabetes cuando sea mayor. | 5. I am always worrying about how diabetes will affect me when I am older. | 5. I worry all the time about how diabetes will affect me when I am older. | 5. Me preocupo constantemente por cómo me afectará la diabetes cuando sea mayor. |
| 6. I feel upset when my blood sugar is out of range. | 6. Me desagrada que mi nivel de glucosa esté fuera de rango. | 6. Me molesta que mi azúcar en sangre esté fuera de los límites normales. | 6. Me molesta que mi nivel de glucosa esté fuera de rango. | 6. It annoys me that my blood sugar is out of range. | 6. It bothers me that my blood sugar is out of range. | 6. Me molesta que mi nivel de azúcar esté fuera de rango. |
| 7. I am too tired of having diabetes to take care of it. | 7. Estoy demasiado cansado/a de tener diabetes para cuidar de la enfermedad. | 7. Estoy demasiado cansado/a de tener diabetes para cuidar de ella. | 7. Estoy demasiado cansado/a de tener diabetes para cuidar de ella. | 7. I am too tired of having diabetes to care about it. | 7. I am too tired of having diabetes to take care of it. | 7. Estoy demasiado cansado/a de tener diabetes como para cuidar de ella. |
| 8. I feel left out when I cannot eat things other kids/teens are eating. | 8. Me siento excluido/a cuando no puedo comer lo que comen otros niños/niñas/adolescentes. | 8. Me siento excluido/a cuando no puedo comer lo mismo que otros niños/as o adolescentes. | 8. Me siento excluido/a cuando no puedo comer lo mismo que otros niños/as o adolescentes. | 8. I feel excluded when I cannot eat the same as other children or teenagers. | 8. I feel excluded when I cannot eat what other kids/teenagers eat. | 8. Me siento excluido/a cuando no puedo comer lo mismo que otros niños/as o adolescentes. |
| 9. I am annoyed when I have to stop what I am doing to check my blood sugar. | 9. Me fastidia tener que dejar de hacer algo para comprobar mi nivel de glucosa. | 9. Me desagrada tener que dejar de hacer lo que estoy haciendo para medir mi azúcar en sangre. | 9. Me fastidia tener que dejar de hacer lo que estoy haciendo para medir mi azúcar en sangre. | 9. It bothers me that I have to stop doing what I am doing to measure my blood sugar. | 9. It annoys me to have to stop what I am doing to check my blood sugar. | 9. Me fastidia tener que dejar de hacer lo que estoy haciendo para medir mi azúcar en sangre. |
| 10. I am tired of trying to figure out my insulin dose at every meal. | 10. Estoy cansado/a de intentar calcular la dosis de insulina en cada comida. | 10. Estoy cansado/a de intentar calcular la dosis de insulina en cada comida. | 10. Estoy cansado/a de intentar calcular la dosis de insulina en cada comida. | 10. I am tired of trying to calculate the insulin dose at each meal. | 10. I am tired of trying to calculate my insulin dose at every meal. | 10. Estoy cansado/a de intentar calcular la dosis de insulina en cada comida. |
| 11. I feel embarrassed about having diabetes. | 11. Me avergüenzo de tener diabetes. | 11. Me avergüenza tener diabetes. | 11. Me siento avergonzado de tener diabetes. | 11. I feel ashamed of having diabetes. | 11. I feel embarrassed about having diabetes. | 11. Me avergüenza tener diabetes. |
| 12. My friends and/or family act like the “diabetes police” (for example, always reminding me to eat right, check blood sugars, or take insulin). | 12. Mis amigos y/o familia actúan como la «policía de la diabetes» (siempre recordándome comer bien, comprobar el nivel de glucosa o ponerme la insulina). | 12. Mis amigos y/o mi familia se comportan como la «policía de la diabetes» (por ejemplo, me recuerdan continuamente que coma bien, que me mida el azúcar en sangre o que me ponga insulina). | 12. Mis amigos y/o mi familia se comportan como la «policía de la diabetes» (por ejemplo, me recuerdan continuamente que coma bien, que me mida el azúcar en sangre o que me ponga insulina. | 12. My friends and/or family behave like the “diabetes police” (for example, they are always reminding me to eat correctly, to measure my blood glucose, or to take insulin). | 12. My friends and/or family act like the “diabetes police” (for example, they remind me all the time to eat well, to check my blood sugar, or to take my insulin). | 12. Mis amigos y/o mi familia se comportan como la «policía de la diabetes» (por ejemplo, me recuerdan continuamente que coma bien, que me mida el azúcar en sangre o que me ponga la insulina). |
| 13. I am tired of remembering to give insulin or shots or bolus. | 13. Estoy cansado/a de tener que recordar ponerme insulina o bolos. | 13. Estoy cansado/a de acordarme de las inyecciones de insulina o de ponerme bolos. | 13. Estoy cansado/a de tener que recordar ponerme las inyecciones de insulina o los bolos. | 13. I am tired of having to remember to inject my insulin or bolus. | 13. I am tired of having to remember my insulin shoots or bolus. | 13. Estoy cansado/a de tener que acordarme de ponerme las inyecciones de insulina o los bolos. |
| 14. It seems like no matter how hard I try, my blood sugars are out of control. | 14. Tengo la sensación de que, haga lo que haga, mis niveles de glucosa siempre están fuera de control. | 14. Parece que, por mucho que me esfuerce, mi azúcar en sangre siempre está fuera de control. | 14. Tengo la sensación de que, haga lo que haga, mis niveles de azúcar siempre están fuera de control. | 14. I feel that, whatever I do, my blood sugar is always out of control. | 14. I feel like, no matter what, my blood sugar is always out of range. | 14. Tengo la sensación de que, haga lo que haga, mis niveles de azúcar siempre están fuera de control. |
| 15. I feel like I do not fit in with other kids/teens my age because of my diabetes. | 15. Siento que no encajo con otros niños/niñas/adolescentes de mi edad debido a la diabetes. | 15. Siento que no encajo con otros niños/as o adolescentes de mi edad por culpa de la diabetes. | 15. Siento que no encajo con otros niños/as o adolescentes de mi edad por culpa de la diabetes. | 15. I feel that I do not fit in with other children or teenagers of my age because of diabetes. | 15. I feel like I do not fit in with other kids/teenagers my age due to my diabetes. | 15. Siento que no encajo con otros niños/as o adolescentes de mi edad por culpa de la diabetes. |
| 16. I am annoyed by having to rotate injection sites or pump infusion sites. | 16. Me fastidia tener que rotar las zonas de inyección o de infusión de la bomba. | 16. Me desagrada tener que cambiar las áreas de punción o de infusión de la bomba. | 16. Me molesta tener que rotar las zonas de inyección o de infusión de la bomba. | 16. It annoys me to have to change the injection or pump infusion zones. | 16. It bothers me to have to rotate injection or pump infusion areas. | 16. Me molesta tener que rotar las zonas de inyección o de infusión de la bomba. |
| 17. I feel angry a lot when I think about having diabetes. | 17. Me enfado mucho cuando pienso en que tengo diabetes. | 17. Me enfado mucho al pensar que tengo diabetes. | 17. Me enfado mucho cuando pienso en que tengo diabetes. | 17. I get very angry when I think I have diabetes. | 17. I feel very angry when I think about having diabetes. | 17. Me enfado mucho cuando pienso en que tengo diabetes. |
| 18. My friends and family do not understand what it is like to have diabetes. | 18. Mis amigos y familia no entienden lo que es tener diabetes. | 18. Mis amigos y mi familia no entienden cómo es tener diabetes. | 18. Mis amigos y familia no entienden lo que es tener diabetes. | 18. My friends and family do not understand what it is like to have diabetes. | 18. My friends and family do not understand what it is like to have diabetes. | 18. Mis amigos y mi familia no entienden lo que es tener diabetes. |
| 19. I worry about going low, especially during physical activities (for example, spots, playing outside, dance class). | 19. Me preocupa tener una bajada, especialmente al hacer ejercicio (por ejemplo, al practicar deportes, jugar en el exterior o en clase de baile). | 19. Me preocupa tener una bajada de azúcar, especialmente durante las actividades físicas (deportes, juegos en el exterior, clases de baile, etc.). | 19. Me preocupa tener una bajada de azúcar, especialmente durante el ejercicio (deportes, juegos en el exterior, clases de baile, etc.). | 19. I worry about having a decrease in blood sugar levels, especially during exercise (sports, outdoor games, dance classes, etc.). | 19. I worry about having a drop in blood sugar, especially during physical exercise (sports, outdoor games, dance class, etc.). | 19. Me preocupa tener una bajada de azúcar, especialmente al hacer ejercicio (deportes, juegos al aire libre, clases de baile, etc.). |
| 20. My parents worry about me and my diabetes too much. | 20. Mis padres se preocupan demasiado por mí y por la diabetes. | 20. Mis padres se preocupan demasiado por mí y mi diabetes. | 20. Mis padres se preocupan demasiado por mí y por mi diabetes. | 20. My parents worry too much about me and my diabetes. | 20. My parents worry too much about me and my diabetes. | 20. Mis padres se preocupan demasiado por mí y por mi diabetes. |
| Mean | SD | CI 95% | Median | IQR | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Current Age (years) | 13.60 | 2.74 | 13.37 | 13.83 | 13.89 | 4.36 |
| Age onset (years) | 7.49 | 3.84 | 7.17 | 7.82 | 7.61 | 5.95 |
| Time with T1DM (years) | 6.16 | 3.92 | 5.83 | 6.50 | 5.57 | 5.60 |
| Weight (kg) | 52.73 | 16.15 | 51.40 | 54.14 | 52.60 | 22.48 |
| SD weight | 0.07 | 0.98 | −0.01 | 0.16 | −0.09 | 1.12 |
| Height (cm) | 158.17 | 14.74 | 156.92 | 159.42 | 160.00 | 20.03 |
| SD height | 0.11 | 1.07 | 0.02 | 0.20 | 0.07 | 1.51 |
| BMI | 20.60 | 3.84 | 20.27 | 20.92 | 20.27 | 4.82 |
| SBP (mmHg) | 112.57 | 12.84 | 111.48 | 113.66 | 112.00 | 15.00 |
| DBP (mmHg) | 69.38 | 8.94 | 68.61 | 70.13 | 70.00 | 11.00 |
| Hb1Ac (%) | 7.34 | 0.99 | 7.26 | 7.43 | 7.20 | 1.20 |
| Hb1Ac previous 3 months (%) | 7.31 | 0.92 | 7.23 | 7.39 | 7.20 | 1.10 |
| Hb1Ac previous 6 months (%) | 7.30 | 1.01 | 7.22 | 7.39 | 7.20 | 1.00 |
| Hb1Ac previous 9 months (%) | 7.23 | 0.99 | 7.15 | 7.32 | 7.10 | 1.20 |
| Hb1Ac previous 12 months (%) | 7.25 | 1.03 | 7.16 | 7.34 | 7.10 | 1.10 |
| Current GMI (%) | 7.29 | 0.80 | 7.22 | 7.36 | 7.20 | 0.90 |
| Glucose (mg/dL) | 165.21 | 30.69 | 162.62 | 167.81 | 160.50 | 39.00 |
| CV diabetes (%) | 37.75 | 7.53 | 37.11 | 38.39 | 37.35 | 9.43 |
| Time <54 mg/dL (%) | 0.57 | 1.28 | 0.46 | 0.68 | 0.00 | 1.00 |
| Time 54–70 mg/dL (%) | 3.36 | 4.87 | 2.95 | 3.77 | 2.00 | 3.00 |
| Time 70–180 mg/dL (%) | 61.33 | 16.64 | 59.92 | 62.74 | 63.00 | 24.75 |
| Time 180–250 mg/dL | 22.79 | 8.93 | 22.04 | 23.55 | 22.00 | 12.00 |
| Time >250 mg/dL (%) | 11.95 | 11.52 | 10.97 | 12.92 | 9.00 | 15.00 |
| Time spent answering the questionnaire (min) | 4.22 | 2.78 | 3.98 | 4.45 | 3.48 | 2.74 |
| PAID-Peds® total score | 45.05 | 18.13 | 43.52 | 46.59 | 45.00 | 27.05 |
| Glucose Range | Recommendations | % Patients |
|---|---|---|
| <54 mg/dL | <1% | 68.22 |
| 54–70 mg/dL | <4% | 64.68 |
| 70–180 mg/dL | >70% | 33.09 |
| 180–250 mg/dL | <25% | 60.97 |
| >250 mg/dL | <5% | 30.86 |
| Age Group (Years Old) | N | Mean | SD | p | |
|---|---|---|---|---|---|
| Hb1Ac (%) | 8–12 | 161 | 7.07 | 0.76 | <0.001 |
| 13–18 | 377 | 7.46 | 1.06 | ||
| Current GMI (%) | 8–12 | 161 | 7.13 | 0.62 | <0.001 |
| 13–18 | 377 | 7.36 | 0.86 | ||
| Glucose (mg/dL) | 8–12 | 161 | 158.54 | 27.64 | <0.001 |
| 13–18 | 377 | 168.06 | 31.50 | ||
| CV diabetes (%) | 8–12 | 161 | 36.59 | 6.28 | 0.03 |
| 13–18 | 377 | 38.24 | 7.96 | ||
| Time <54 mg/dL (%) | 8–12 | 161 | 0.36 | 0.70 | 0.04 |
| 13–18 | 377 | 0.66 | 1.46 | ||
| Time 54–70 mg/dL (%) | 8–12 | 161 | 3.06 | 4.39 | 0.26 |
| 13–18 | 377 | 3.49 | 5.06 | ||
| Time 70–180 mg/dL (%) | 8–12 | 161 | 65.03 | 14.73 | <0.001 |
| 13–18 | 377 | 59.75 | 17.17 | ||
| Time 180–250 mg/dL | 8–12 | 161 | 22.12 | 8.80 | 0.14 |
| 13–18 | 377 | 23.08 | 8.98 | ||
| Time >250 mg/dL (%) | 8–12 | 161 | 9.43 | 9.81 | <0.001 |
| 13–18 | 377 | 13.02 | 12.03 | ||
| Time spent answering the questionnaire (min) | 8–12 | 161 | 5.32 | 3.29 | <0.001 |
| 13–18 | 377 | 3.75 | 2.38 | ||
| PAID-Peds® total score | 8–12 | 161 | 46.39 | 17.83 | 0.29 |
| 13–18 | 377 | 44.48 | 18.26 |
| Item % (n) | Agree | -> | Neither Agree Nor Disagree | -> | Disagree |
|---|---|---|---|---|---|
| Q1 | 6.51 (35) | 15.24 (82) | 29.18 (157) | 20.63 (111) | 28.44 (153) |
| Q2 | 10.22 (55) | 20.26 (109) | 25.28 (136) | 26.39 (142) | 17.84 (96) |
| Q3 | 10.59 (57) | 30.48 (164) | 29.37 (158) | 16.73 (90) | 12.83 (69) |
| Q4 | 21.56 (116) | 25.28 (136) | 17.84 (96) | 22.86 (123) | 12.45 (67) |
| Q5 | 10.59 (57) | 23.23 (125) | 27.32 (147) | 19.52 (105) | 19.33 (104) |
| Q6 | 22.12 (119) | 46.28 (249) | 19.70 (106) | 8.36 (45) | 3.53 (19) |
| Q7 | 9.85 (53) | 13.20 (71) | 19.52 (105) | 28.62 (154) | 28.81 (155) |
| Q8 | 10.97 (59) | 19.52 (105) | 13.20 (71) | 22.49 (121) | 33.83 (182) |
| Q9 | 22.86 (123) | 28.25 (152) | 17.29 (93) | 19.33 (104) | 12.27 (66) |
| Q10 | 9.67 (52) | 14.50 (78) | 26.77 (144) | 28.07 (151) | 21.00 (113) |
| Q11 | 2.79 (15) | 5.39 (29) | 10.59 (57) | 22.68 (122) | 58.55 (315) |
| Q12 | 24.16 (130) | 30.11 (162) | 26.39 (142) | 13.01 (70) | 6.32 (34) |
| Q13 | 12.27 (66) | 20.45 (110) | 22.86 (123) | 23.98 (129) | 20.45 (110) |
| Q14 | 7.06 (38) | 13.38 (72) | 23.05 (124) | 31.97 (172) | 24.54 (132) |
| Q15 | 2.79 (15) | 3.35 (18) | 9.67 (52) | 26.02 (140) | 58.18 (313) |
| Q16 | 13.94 (75) | 17.29 (93) | 21.38 (115) | 24.54 (132) | 22.86 (123) |
| Q17 | 6.51 (35) | 13.94 (75) | 18.96 (102) | 25.46 (137) | 35.13 (189) |
| Q18 | 7.99 (43) | 13.94 (75) | 21.19 (114) | 21.75 (117) | 35.13 (189) |
| Q19 | 21.00 (113) | 35.50 (191) | 21.19 (114) | 13.20 (71) | 9.11 (49) |
| Q20 | 34.39 (185) | 32.16 (173) | 21.19 (114) | 7.99 (43) | 4.28 (23) |
| % (n) | 0 | 1 | 2 | 3 | 4 | p Value (CC) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | Male | Female | Male | Female | Male | Female | Male | Female | Male | CC | |
| Q1 | 3.7 | 2.8 | 8.6 | 6.7 | 17.1 | 12.1 | 7.8 | 12.8 | 11.2 | 17.3 | <0.001 |
| (20) | (15) | (46) | (36) | (92) | (65) | (42) | (69) | (60) | (93) | 0.19 | |
| Q2 | 5.4 | 4.8 | 11.5 | 8.7 | 11.9 | 13.4 | 12.3 | 14.1 | 7.2 | 10.6 | 0.19 |
| (29) | (26) | (62) | (47) | (64) | (72) | (66) | (76) | (39) | (57) | N/A | |
| Q3 | 5.58 | 5.02 | 16.17 | 14.31 | 13.20 | 16.17 | 7.25 | 9.48 | 6.13 | 6.69 | 0.47 |
| (30) | (27) | (87) | (77) | (71) | (87) | (39) | (51) | (33) | (36) | N/A | |
| Q4 | 11.52 | 10.04 | 13.57 | 11.71 | 8.18 | 9.67 | 10.04 | 12.83 | 5.02 | 7.43 | 0.22 |
| (62) | (54) | (73) | (63) | (44) | (52) | (54) | (69) | (27) | (40) | N/A | |
| Q5 | 5.39 | 5.20 | 11.90 | 11.34 | 13.20 | 14.13 | 9.29 | 10.22 | 8.55 | 10.78 | 0.86 |
| (29) | (28) | (64) | (61) | (71) | (76) | (50) | (55) | (46) | (58) | N/A | |
| Q6 | 11.52 | 10.59 | 23.23 | 23.05 | 8.55 | 11.15 | 3.16 | 5.20 | 1.86 | 1.67 | 0.38 |
| (62) | (57) | (125) | (124) | (46) | (60) | (17) | (28) | (10) | (9) | N/A | |
| Q7 | 5.58 | 4.28 | 6.69 | 6.51 | 9.67 | 9.85 | 14.50 | 14.13 | 11.90 | 16.91 | 0.28 |
| (30) | (23) | (36) | (35) | (52) | (53) | (78) | (76) | (64) | (91) | N/A | |
| Q8 | 6.13 | 4.83 | 11.15 | 8.36 | 6.51 | 6.69 | 11.15 | 11.34 | 13.38 | 20.45 | 0.04 |
| (33) | (26) | (60) | (45) | (35) | (36) | (60) | (61) | (72) | (110) | 0.14 | |
| Q9 | 11.34 | 11.52 | 14.31 | 13.94 | 7.43 | 9.85 | 8.92 | 10.41 | 6.32 | 5.95 | 0.75 |
| (61) | (62) | (77) | (75) | (40) | (53) | (48) | (56) | (34) | (32) | N/A | |
| Q10 | 4.46 | 5.20 | 8.55 | 5.95 | 12.64 | 14.13 | 13.01 | 15.06 | 9.67 | 11.34 | 0.38 |
| (24) | (28) | (46) | (32) | (68) | (76) | (70) | (81) | (52) | (61) | N/A | |
| Q11 | 1.86 | 0.93 | 3.53 | 1.86 | 5.95 | 4.65 | 10.04 | 12.64 | 26.95 | 31.60 | 0.08 |
| (10) | (5) | (19) | (10) | (32) | (25) | (54) | (68) | (145) | (170) | N/A | |
| Q12 | 12.27 | 11.90 | 13.94 | 16.17 | 12.64 | 13.75 | 5.20 | 7.81 | 4.28 | 2.04 | 0.11 |
| (66) | (64) | (75) | (87) | (68) | (74) | (28) | (42) | (23) | (11) | N/A | |
| Q13 | 6.51 | 5.76 | 12.08 | 8.36 | 8.92 | 13.94 | 10.78 | 13.20 | 10.04 | 10.41 | 0.03 |
| (35) | (31) | (65) | (45) | (48) | (75) | (58) | (71) | (54) | (56) | 0.14 | |
| Q14 | 4.09 | 2.97 | 7.43 | 5.95 | 11.71 | 11.34 | 14.13 | 17.84 | 10.97 | 13.57 | 0.28 |
| (22) | (16) | (40) | (32) | (63) | (61) | (76) | (96) | (59) | (73) | N/A | |
| Q15 | 1.49 | 1.30 | 1.86 | 1.49 | 5.58 | 4.09 | 13.94 | 12.08 | 25.46 | 32.71 | 0.16 |
| (8) | (7) | (10) | (8) | (30) | (22) | (75) | (65) | (137) | (176) | N/A | |
| Q16 | 6.13 | 7.81 | 8.18 | 9.11 | 12.27 | 9.11 | 12.45 | 12.08 | 9.29 | 13.57 | 0.11 |
| (33) | (42) | (44) | (49) | (66) | (49) | (67) | (65) | (50) | (73) | N/A | |
| Q17 | 3.53 | 2.97 | 6.69 | 7.25 | 10.04 | 8.92 | 13.38 | 12.08 | 14.68 | 20.45 | 0.23 |
| (19) | (16) | (36) | (39) | (54) | (48) | (72) | (65) | (79) | (110) | N/A | |
| Q18 | 4.83 | 3.16 | 7.43 | 6.51 | 10.59 | 10.59 | 9.11 | 12.64 | 16.36 | 18.77 | 0.23 |
| (26) | (17) | (40) | (35) | (57) | (57) | (49) | (68) | (88) | (101) | N/A | |
| Q19 | 9.29 | 11.71 | 18.40 | 17.10 | 10.97 | 10.22 | 5.58 | 7.62 | 4.09 | 5.02 | 0.48 |
| (50) | (63) | (99) | (92) | (59) | (55) | (30) | (41) | (22) | (27) | N/A | |
| Q20 | 17.29 | 17.10 | 15.61 | 16.54 | 9.48 | 11.71 | 3.90 | 4.09 | 2.04 | 2.23 | 0.93 |
| (93) | (92) | (84) | (89) | (51) | (63) | (21) | (22) | (11) | (12) | N/A | |
| Item Reliability Statistics | Item–Rest Correlation | If Item Dropped |
|---|---|---|
| Cronbach’s α | ||
| Q1 | 0.66 | 0.89 |
| Q2 | 0.61 | 0.89 |
| Q3 | 0.39 | 0.90 |
| Q4 | 0.68 | 0.89 |
| Q5 | 0.51 | 0.90 |
| Q6 | 0.30 | 0.90 |
| Q7 | 0.65 | 0.89 |
| Q8 | 0.60 | 0.89 |
| Q9 | 0.57 | 0.90 |
| Q10 | 0.65 | 0.89 |
| Q11 | 0.50 | 0.90 |
| Q12 | 0.46 | 0.90 |
| Q13 | 0.69 | 0.89 |
| Q14 | 0.52 | 0.90 |
| Q15 | 0.57 | 0.90 |
| Q16 | 0.37 | 0.90 |
| Q17 | 0.71 | 0.89 |
| Q18 | 0.42 | 0.90 |
| Q19 | 0.36 | 0.90 |
| Q20 | 0.37 | 0.90 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Civitani Monzón, E.; Ferrer Duce, M.P.; De Arriba Muñoz, A.; Goicoechea Manterola, I.; Yelmo Valverde, R.; Casanovas-Marsal, J.-O. Spanish Validation of the Problem Area in Diabetes-Pediatric Version Survey and Its Weak Association with Metabolic Control Parameters in Pediatric Diabetes: A Cross-Sectional Multicenter Study. J. Clin. Med. 2025, 14, 523. https://doi.org/10.3390/jcm14020523
Civitani Monzón E, Ferrer Duce MP, De Arriba Muñoz A, Goicoechea Manterola I, Yelmo Valverde R, Casanovas-Marsal J-O. Spanish Validation of the Problem Area in Diabetes-Pediatric Version Survey and Its Weak Association with Metabolic Control Parameters in Pediatric Diabetes: A Cross-Sectional Multicenter Study. Journal of Clinical Medicine. 2025; 14(2):523. https://doi.org/10.3390/jcm14020523
Chicago/Turabian StyleCivitani Monzón, Elisa, María Pilar Ferrer Duce, Antonio De Arriba Muñoz, Irune Goicoechea Manterola, Rosa Yelmo Valverde, and Josep-Oriol Casanovas-Marsal. 2025. "Spanish Validation of the Problem Area in Diabetes-Pediatric Version Survey and Its Weak Association with Metabolic Control Parameters in Pediatric Diabetes: A Cross-Sectional Multicenter Study" Journal of Clinical Medicine 14, no. 2: 523. https://doi.org/10.3390/jcm14020523
APA StyleCivitani Monzón, E., Ferrer Duce, M. P., De Arriba Muñoz, A., Goicoechea Manterola, I., Yelmo Valverde, R., & Casanovas-Marsal, J.-O. (2025). Spanish Validation of the Problem Area in Diabetes-Pediatric Version Survey and Its Weak Association with Metabolic Control Parameters in Pediatric Diabetes: A Cross-Sectional Multicenter Study. Journal of Clinical Medicine, 14(2), 523. https://doi.org/10.3390/jcm14020523