

Integrating Artificial Intelligence into Orthodontic Education: A Systematic Review and Meta-Analysis of Clinical Teaching Application



Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Exclusion Criteria
2.4. Information Sources and Search Strategy
2.5. Selection Process
2.6. Data Collection Process
2.7. Data Items
2.8. Study Risk of Bias Assessment
2.9. Certainty of Evidence (GRADE Assessment)
2.10. Data Synthesis and Statistical Analysis
3. Results
3.1. Study Selection Process
3.2. Data Synthesis
3.3. Outcome Categorization
3.4. Descriptive Characteristics of Included Studies
3.5. AI as an Instructional Adjunct in Orthodontic Education
3.6. Effectiveness in Enhancing Knowledge Acquisition and Diagnostic Skill
3.7. Perceptions, Attitudes, and Readiness Toward AI in Orthodontic Education
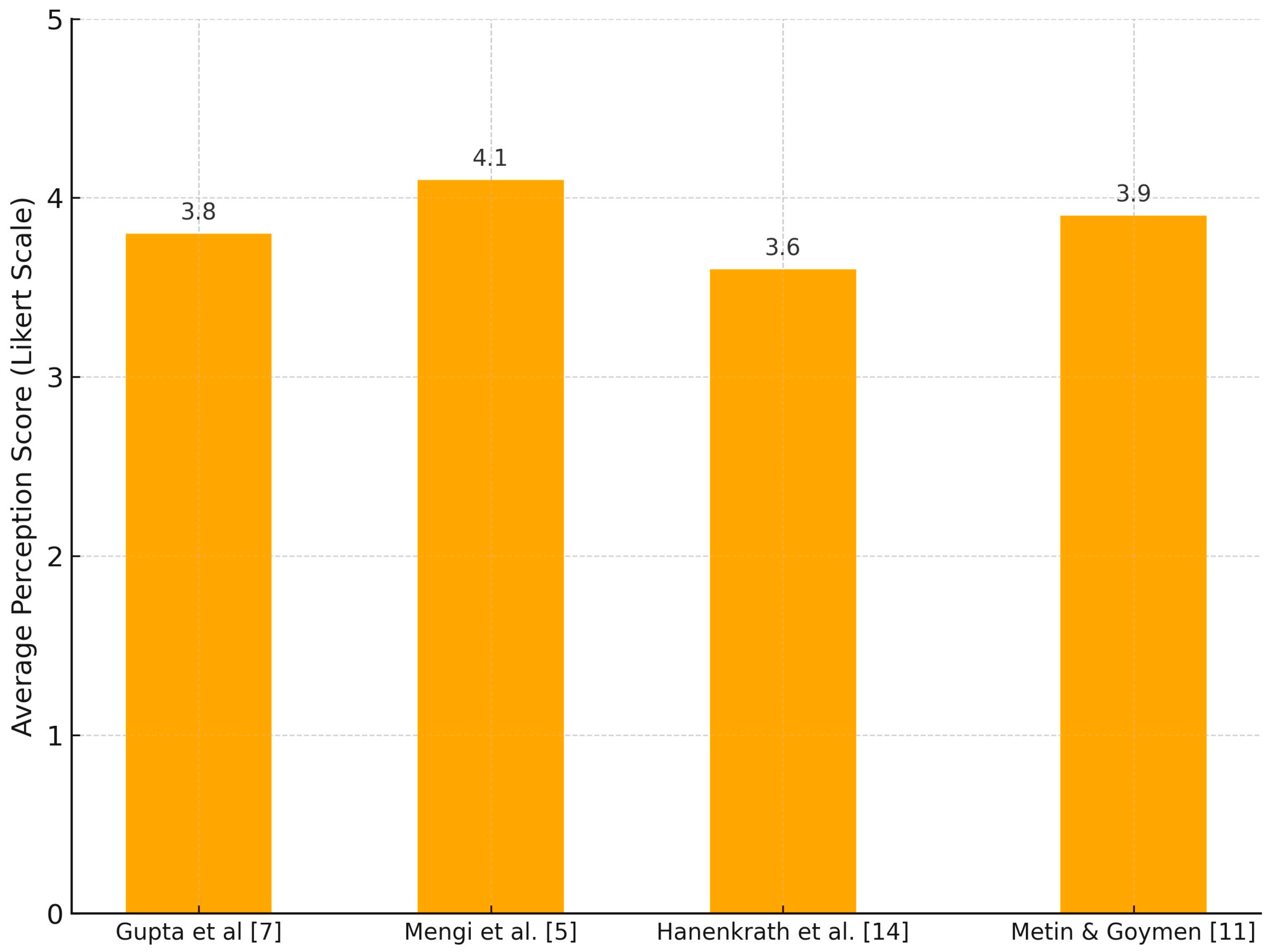
3.8. Quantitative Synthesis of Educational Quality Scores
3.9. Risk of Bias (ROBINS-I)
3.10. GRADE Evidence Summary
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Schwendickle Samek, F.; Krois, J. Artificial intelligence in dentistry: Chances and challenges. J. Dent. Res. 2020, 99, 769–774. [Google Scholar] [CrossRef]
- Monill-Gonzalez, A.; Rovira-Calatayud, L.; d’Oliveria, N.G.; Ustrell-Torrent, J.M. Artificial intelligence in orthodontics: Where are we now? A scoping review. Dec. Orthod. Craniofac Res. 2021, 24 (Suppl. 2), 6–15. [Google Scholar] [CrossRef]
- Shan, T.; Tay, F.R.; Gu, L. Application of Artificial Intelligence in Dentistry. J. Dent. Res. 2021, 100, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Park, J.B.; Chang, M.S.; Ryu, J.J.; Lim, W.H.; Jung, S.K. Influence of the depth of the convolutional neural networks on an artificial intelligence model for diagnosis of orthognathic surgery. J. Pers. Med. 2021, 11, 356. [Google Scholar] [CrossRef] [PubMed]
- Mengi, A.; Singh, R.P.; Mengi, N.; Kalgotra, S.; Singh, A. A questionnaire study regarding knowledge, attitude and usage of artificial intelligence and machine learning by the orthodontic fraternity of Northern India. J. Oral. Biol. Craniofac Res. 2024, 14, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Yadalam, P.K.; Anegundi, R.V.; Ardila, C.M. Integrating Artificial Intelligence Into Orthodontic Education and Practice. Int. Dent. J. 2024, 74, 1463. [Google Scholar] [CrossRef]
- Gupta, S.; Verma, S.; Chauhan, A.K.; Roy, M.S.; Rajkumari, W.; Sahgal, C. Knowledge, attitude, and perception of orthodontic students, and orthodontists regarding role of artificial intelligence in field of orthodontics-An online cross-sectional survey. J. World Fed. Orthod. 2025, 14, 3–11. [Google Scholar] [CrossRef]
- Ardila, C.M.; Yadalam, P.K. AI and dental education. Br. Dent. J. 2025, 238, 294. [Google Scholar] [CrossRef]
- Roganović, J. Familiarity with ChatGPT Features Modifies Expectations and Learning Outcomes of Dental Students. Int. Dent. J. 2024, 74, 1456–1462. [Google Scholar] [CrossRef]
- Lin, J.; Liao, Z.; Dai, J.; Wang, M.; Yu, R.; Yang, H.; Liu, C. Digital and artificial intelligence-assisted cephalometric training effectively enhanced students’ landmarking accuracy in preclinical orthodontic education. BMC Oral. Health. 2025, 25, 623. [Google Scholar] [CrossRef]
- Metin, U.; Goymen, M. Information from digital and human sources: A comparison of chatbot and clinician responses to orthodontic questions. Am. J. Orthod. Dentofac. Orthop. 2025, in press. [Google Scholar] [CrossRef]
- Mohseni, S.O.; Schlieve, T. Artificial Intelligence in Medicine: Is Oral and Maxillofacial Surgery Following the Trend? J. Oral. Maxillofac. Surg. 2024, 82, 1189–1190. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Samaniego, C.S.; Sousa Melo, S.L.; Brachvogel, W.A.; Baskaran, K.; Rulli, D. Artificial intelligence (A.I.) in dental curricula: Ethics and responsible integration. J. Dent. Educ. 2023, 87, 1570–1573. [Google Scholar] [CrossRef] [PubMed]
- Hanenkrath, J.; Park, J.H.; Bay, C. Training, use, and modifications related to artificial intelligence in postgraduate orthodontic programs in North America. Am. J. Orthod. Dentofac. Orthop. 2025, 167, 89–94.e2. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Aguayo-Albasini, J.L.; Flores-Pastor, B.; Soria-Aledo, V. GRADE system: Classification of quality of evidence and strength of recommendation. Cir. Esp. 2014, 92, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Tang, B.; Cao, L.; Yan, J.; Zhao, T.; Hua, F.; He, H. The knowledge, experience, and attitude on artificial intelligence-assisted cephalometric analysis: Survey of orthodontists and orthodontic students. Am. J. Orthod. Dentofac. Orthop. 2023, 164, e97–e105. [Google Scholar] [CrossRef]
- Kurt Demirsoy, K.; Buyuk, S.K.; Bicer, T. How reliable is the artificial intelligence product large language model ChatGPT in orthodontics? Angle Orthod. 2024, 94, 602–607. [Google Scholar] [CrossRef]
- Ishida, Y.; Kuwajima, Y.; Kobayashi, T.; Yonezawa, Y.; Asack, D.; Nagai, M.; Kondo, H.; Ishikawa-Nagai, S.; Da Silva, J.; Lee, S.J.; et al. Current Implementation of Digital Dentistry for Removable Prosthodontics in US Dental Schools. Int. J. Dent. 2022, 2022, 7331185. [Google Scholar] [CrossRef]
- Agrawal, P.; Nikhade, P. Artificial Intelligence in Dentistry: Past, Present, and Future. Cureus. 2022, 14, e27405. [Google Scholar] [CrossRef]
- Dipalma, G.; Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Carpentiere, V.; Garofoli, G.; Azzollini, D.; Campanelli, M.; Paduanelli, G.; Palermo, A.; et al. Artificial Intelligence and Its Clinical Applications in Orthodontics: A Systematic Review. Diagnostics 2023, 13, 3677. [Google Scholar] [CrossRef]
- Baxmann, M.; Kárpáti, K.; Baráth, Z. The potentials and challenges of integrating generative artificial intelligence (AI) in dental and orthodontic education: A systematic review. BMC Oral. Health. 2025, 25, 905. [Google Scholar] [CrossRef]
- Khanagar, S.B.; Al-Ehaideb, A.; Vishwanathaiah, S.; Maganur, P.C.; Patil, S.; Naik, S.; Baeshen, H.A.; Sarode, S.S. Scope and performance of artificial intelligence technology in orthodontic diagnosis, treatment planning, and clinical decision-making—A systematic review. J. Dent. Sci. 2021, 16, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Salari, B.; Amini, M. The Impact of Different Teaching Methods on Clinical Reasoning and Clinical Decision-making of Dentistry Students: A Systematic Review. J. Dent. Educ. 2025, e13930. [Google Scholar] [CrossRef] [PubMed]
- Boccuzzi, M.; Cosola, S.; Butera, A.; Genovesi, A.; Laborante, T.; Castaldo, A.; Zizza, A.; Oldoini, G.; Nota, A.; Tecco, S. Predictability of ClinCheck in overbite correction with aligners: A systematic review. Appl. Sci. 2025, 15, 7268. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year) | Outcome Type | Tools/Measures Used | Objective vs. Subjective | Key Findings |
|---|---|---|---|---|
| Lin et al. (2025) [10] | Skill improvement | Landmarking accuracy tests | Objective | Improved cephalometric accuracy |
| Hanenkrath et al. (2025) [14] | Curricular readiness | Survey among directors | Subjective | Limited integration, lack of training |
| Gupta et al. (2025) [7] | Perceptions, attitudes | Online survey (Likert) | Subjective | High expectations, limited training |
| Metin et al. (2025) [11] | Knowledge retention and perception | AI chatbot, comparison tests, GQS | Both | Comparable satisfaction and diagnostic performance |
| Mengi et al. (2024) [5] | Faculty/student attitudes | Questionnaire | Subjective | Academicians more favorable than clinicians |
| Kurt et al. (2024) [19] | Perceived quality | ChatGPT evaluations, DISCERN, GQS | Subjective | Patients rated highest; experts most critical |
| Lin et al. (2023) [18] | Skill improvement | Pre/post cephalometric training | Objective | Significant increase in diagnostic accuracy |
| Author (Year) | Country | Study Design | Participants | AI Application |
|---|---|---|---|---|
| Lin et al. (2025) [10] | China | Quasi-experimental | 40 students, 24 trainees | Digital and AI-assisted cephalometry |
| Hanenkrath et al. (2025) [14] | USA/Canada | Cross-sectional | 41 program directors | AI integration in curricula (research, diagnosis) |
| Gupta et al. (2025) [7] | India | Cross-sectional | 117 postgraduate students and 149 faculty members | Knowledge, attitude, and perception (KAP) |
| Metin et al. (2025) [11] | Turkey | Cross-sectional | 30 dentists, 30 students, 30 orthodontists | Chatbot vs. human response comparison |
| Mengi et al. (2024) [5] | India | Cross-sectional | 50 orthodontists (academicians and clinicians) and 50 postgraduate students | Knowledge and perception on AI |
| Kurt et al. (2024) [19] | Turkey | Cross-sectional | 30 students, 30 orthodontists | Knowledge and perception on AI |
| Lin et al. (2023) [18] | China | Quasi-experimental | 182 orthodontic students, 298 orthodontists | AI tool in landmark training |
| Study | AI Tool | Educational Use Context | Participant Group | Key Findings on Instructional Role |
|---|---|---|---|---|
| Lin et al. [10] | AI-assisted cephalometry | Landmarking accuracy with real-time feedback | Students, trainees | Improved accuracy and autonomous learning |
| Metin et al. [11] | Chatbot vs. human tutor | Query-based learning and clinical reasoning | Students, clinicians | Comparable satisfaction and performance |
| Kurt et al. [19] | ChatGPT (AI chatbot) | Response accuracy on clinical topics | Students, orthodontists | Rated moderate-to-good quality; educational utility |
| Lin et al. [18] | Digital cephalometry training | Iterative training cycles with feedback | Orthodontic students | Pre/post skill enhancement and increased confidence |
| Study | AI Tool | Objective Performance Measured | Outcome Summary |
|---|---|---|---|
| Lin et al. [10] | AI-assisted cephalometry | Yes | Improved landmarking accuracy. |
| Gupta et al. [7] | Perceptions on AI utility | No direct measure | High expectations for decision support. 74% faculty agreed on AI for cephalometrics; limited training. |
| Metin et al. [11] | Chatbot vs. Human Tutor | Yes | Comparable performance. |
| Mengi et al. [5] | CBCT analysis tools | Yes | 90% faculty endorsed AI for complex diagnostics. |
| Kurt et al. [19] | ChatGPT | Yes | Patients rated AI responses highest (GQS > 4); orthodontists more critical. |
| Lin et al. [18] | Digital cephalometric training | Yes | Significant pre/post accuracy gain. |
| Study | Stakeholder Group | Key Findings |
|---|---|---|
| Lin et al. [10] | Clinical Students | AI tools improved skills and engagement; readiness inferred via improved autonomy. |
| Hanenkrath et al. [14] | Program Directors | AI integration planned in 56% of programs, but 87.8% lacked structured seminars. |
| Gupta et al. [7] | Faculty and Postgraduates | Favorable attitudes (72%), hindered by cost and lack of technical training. |
| Metin et al. [11] | Students, General Dentists, Orthodontists | Students and general dentists showed moderate-to-high confidence in chatbot responses; orthodontists more skeptical. |
| Mengi et al. [5] | Academicians and Clinicians | Academicians supportive (84%), clinicians less engaged due to workflow barriers. |
| Kurt et al. [19] | Students, Patients, Experts | Patients rated AI responses highly; orthodontists more critical; dental students moderate. |
| Lin et al. [18] | Orthodontic Students | Repeated AI-assisted training increased confidence and accuracy; readiness inferred. |
| Study | Bias due to Confounding | Bias in Selection of Participants | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of Reported Result | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Lin et al. [10] | Moderate | Low | Low | Low | Low | Low | Low | Moderate |
| Gupta et al. [7] | Moderate | Moderate | Low | Low | Low | Low | Low | Moderate |
| Metin et al. [11] | Serious | Serious | Moderate | Moderate | Low | Serious | Low | Serious |
| Hanenkrath et al. [14] | Low | Low | Low | Low | Low | Low | Low | Low |
| Mengi et al. [5] | Low | Low | Low | Low | Low | Low | Low | Low |
| Kurt et al. [19] | Moderate | Moderate | Low | Low | Low | Low | Low | Moderate |
| Lin et al. [18] | Low | Low | Low | Low | Low | Low | Low | Low |
| Study | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Quality |
|---|---|---|---|---|---|---|
| Lin et al. [10] | Moderate | Not Serious | Not Serious | Serious | Undetected | Low |
| Gupta et al. [7] | Moderate | Not Serious | Not Serious | Not Serious | Undetected | Moderate |
| Metin et al. [11] | Serious | Not Serious | Not Serious | Serious | Undetected | Low |
| Hanenkrath et al. [14] | Low | Not Serious | Not Serious | Not Serious | Undetected | Moderate |
| Mengi et al. [5] | Low | Not Serious | Not Serious | Not Serious | Undetected | Moderate |
| Kurt et al. [19] | Moderate | Serious | Not Serious | Serious | Undetected | Low |
| Lin et al. [18] | Low | Not Serious | Not Serious | Not Serious | Undetected | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardila, C.M.; Pineda-Vélez, E.; Vivares Builes, A.M. Integrating Artificial Intelligence into Orthodontic Education: A Systematic Review and Meta-Analysis of Clinical Teaching Application. J. Clin. Med. 2025, 14, 5487. https://doi.org/10.3390/jcm14155487
Ardila CM, Pineda-Vélez E, Vivares Builes AM. Integrating Artificial Intelligence into Orthodontic Education: A Systematic Review and Meta-Analysis of Clinical Teaching Application. Journal of Clinical Medicine. 2025; 14(15):5487. https://doi.org/10.3390/jcm14155487
Chicago/Turabian StyleArdila, Carlos M., Eliana Pineda-Vélez, and Anny Marcela Vivares Builes. 2025. "Integrating Artificial Intelligence into Orthodontic Education: A Systematic Review and Meta-Analysis of Clinical Teaching Application" Journal of Clinical Medicine 14, no. 15: 5487. https://doi.org/10.3390/jcm14155487
APA StyleArdila, C. M., Pineda-Vélez, E., & Vivares Builes, A. M. (2025). Integrating Artificial Intelligence into Orthodontic Education: A Systematic Review and Meta-Analysis of Clinical Teaching Application. Journal of Clinical Medicine, 14(15), 5487. https://doi.org/10.3390/jcm14155487