
Integrating CT-Based Lung Fibrosis and MRI-Derived Right Ventricular Function for the Detection of Pulmonary Hypertension in Interstitial Lung Disease

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
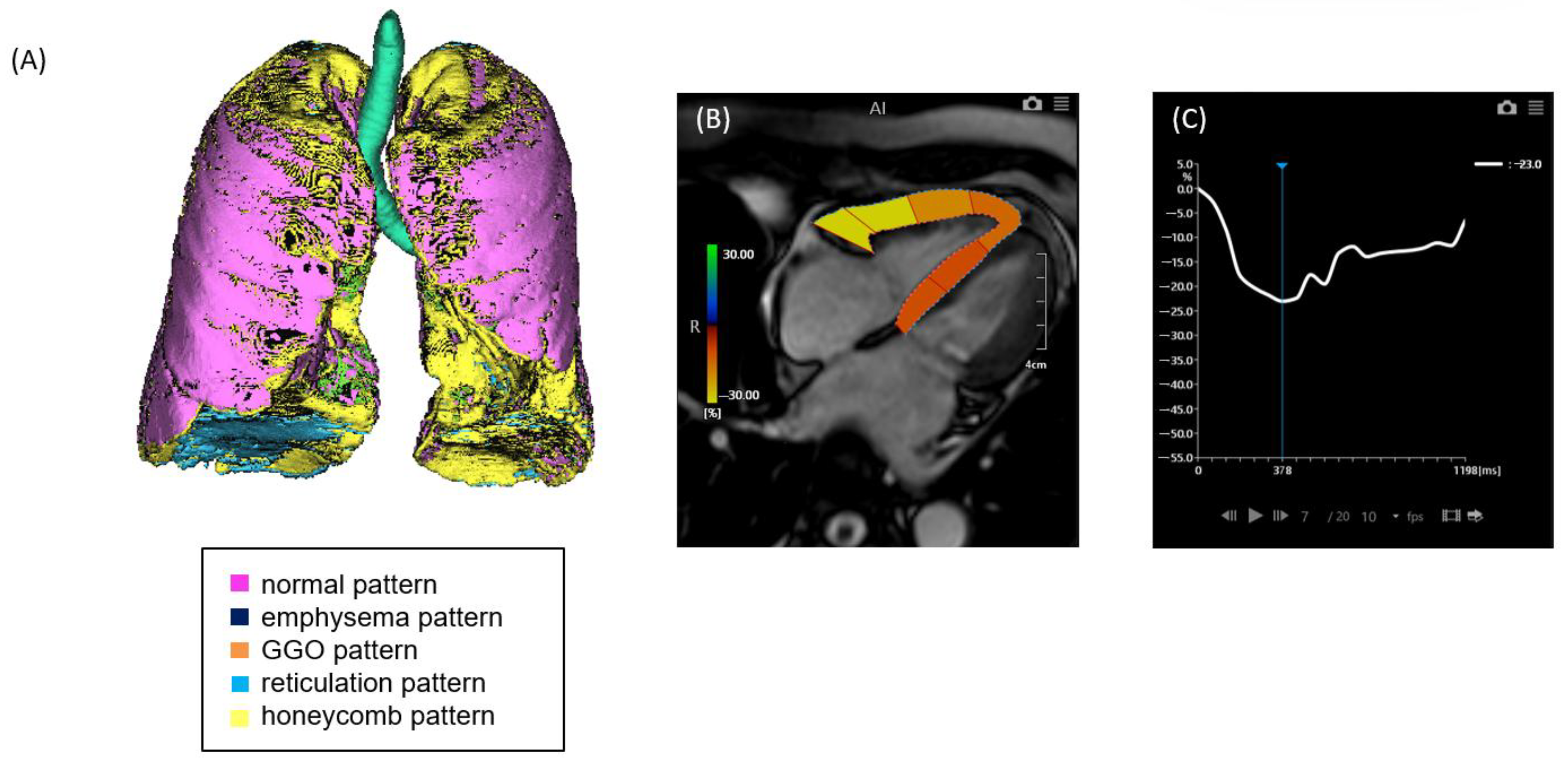
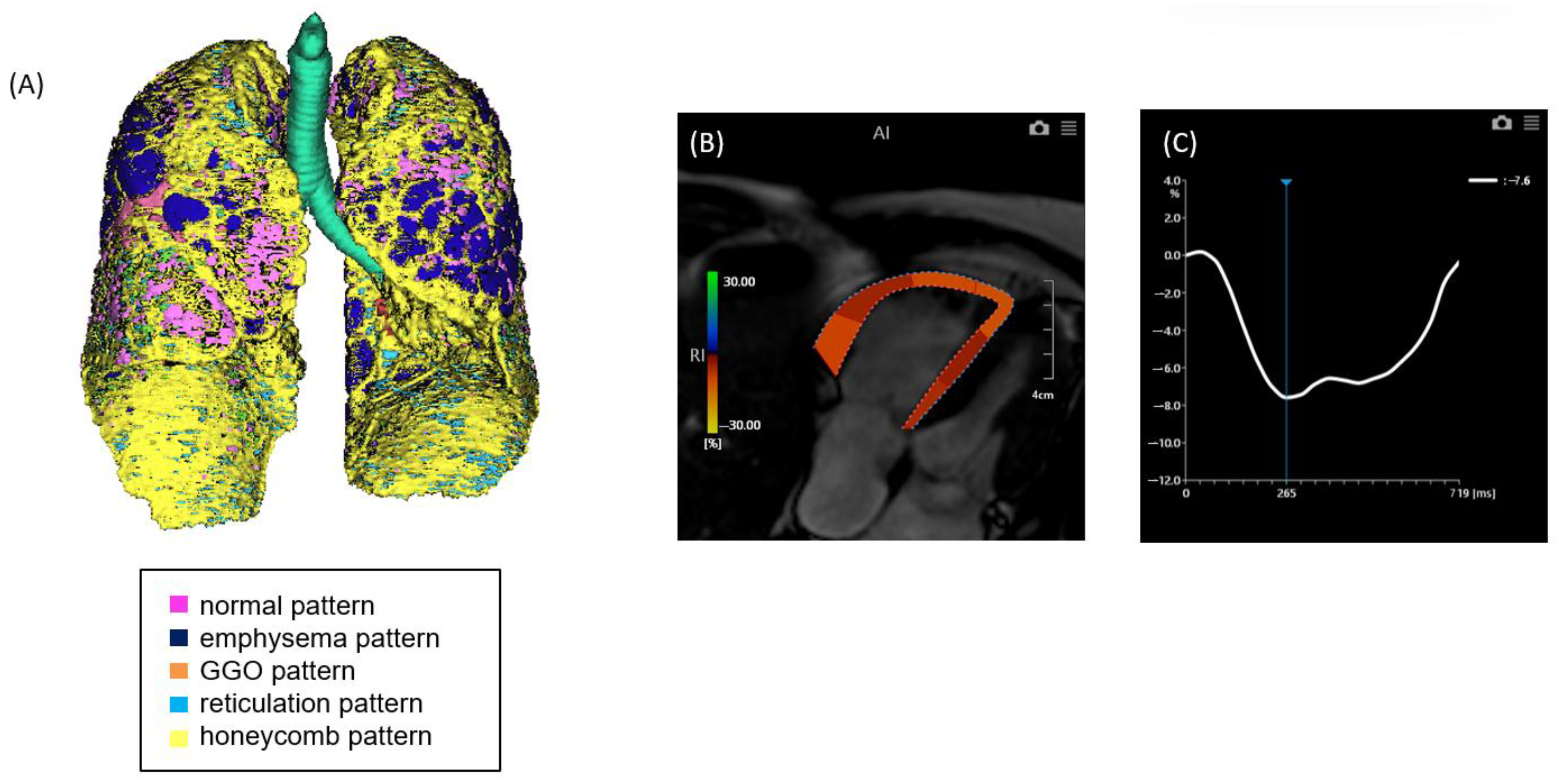
2.2. CT Image Acquisition and Analysis
2.3. MRI Image Acquisition and Analysis
2.4. Right Heart Catheterization
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of Chest CT and Cardiac MRI Parameters of ILD with and Without PH
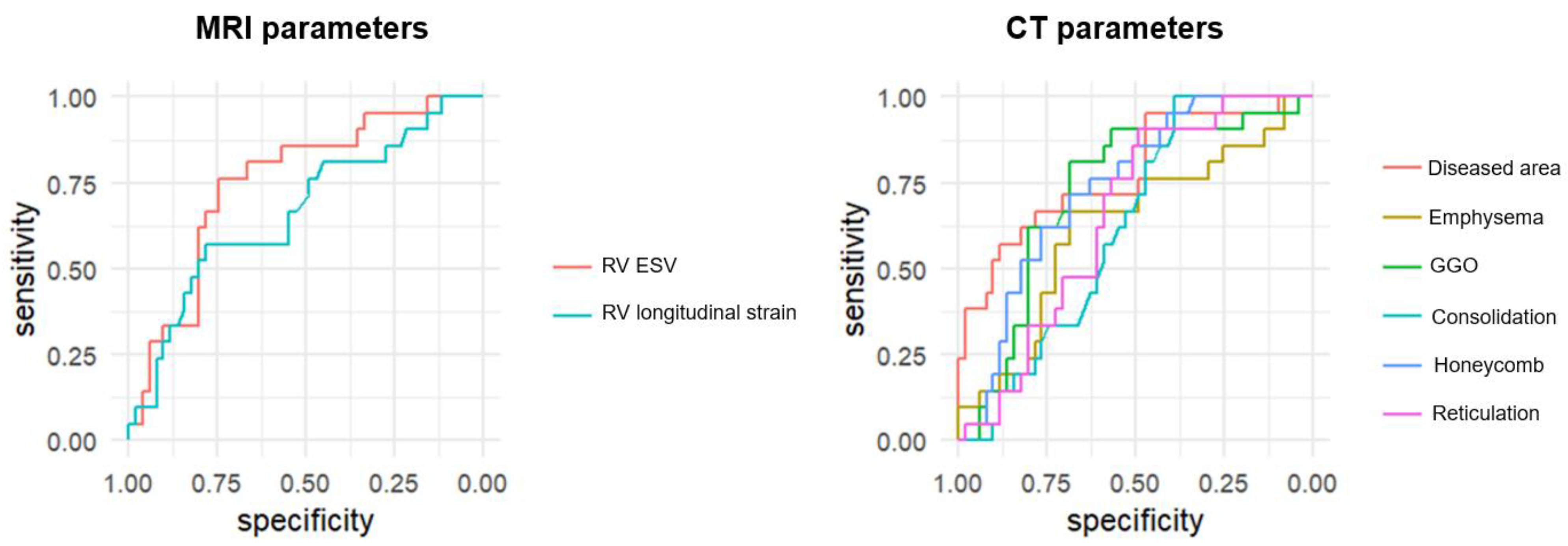
3.3. Diagnostic Performance of CT and MRI Parameters
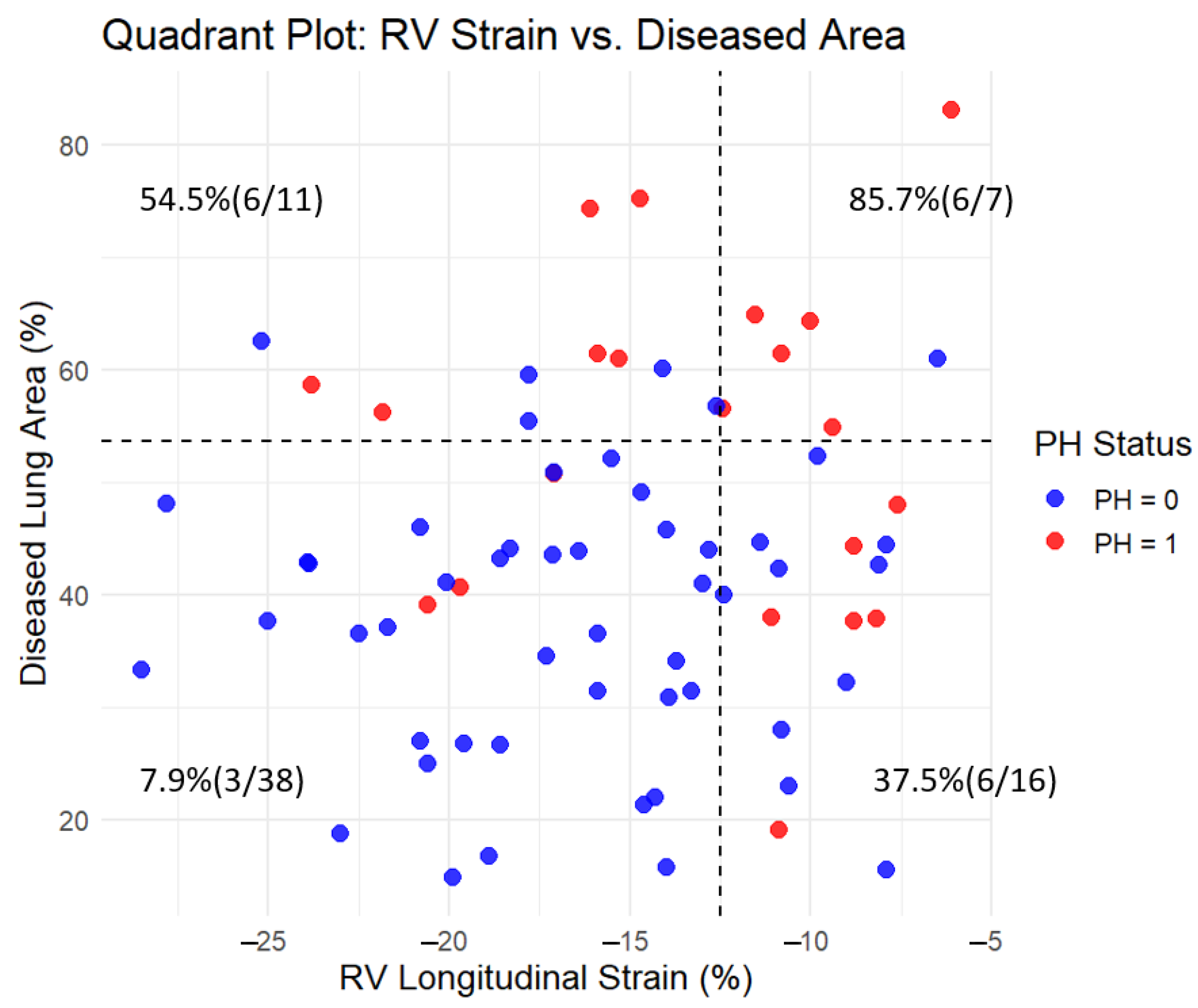
3.4. Incremental Value of Combining CT and MRI Parameters
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ki, M.S.; Kim, S.Y.; Kim, E.Y.; Jung, J.Y.; Kang, Y.A.; Park, M.S.; Kim, Y.S.; Park, S.Y.; Lee, S.H. Clinical Outcomes and Prognosis of Patients With Interstitial Lung Disease Undergoing Lung Cancer Surgery: A Propensity Score Matching Study. Clin. Lung Cancer 2023, 24, e27–e38. [Google Scholar] [CrossRef] [PubMed]
- Hilberg, O.; Bendstrup, E.; Løkke, A.; Ibsen, R.; Fløe, A.; Hyldgaard, C. Co-morbidity and mortality among patients with interstitial lung diseases: A population-based study. Respirology 2018, 23, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [PubMed]
- Alhamad, E.H.; Cal, J.G.; Alrajhi, N.N.; Alharbi, W.M. Predictors of Mortality in Patients with Interstitial Lung Disease-Associated Pulmonary Hypertension. J. Clin. Med. 2020, 9, 3828. [Google Scholar] [CrossRef]
- Seeger, W.; Adir, Y.; Barberà, J.A.; Champion, H.; Coghlan, J.G.; Cottin, V.; De Marco, T.; Galiè, N.; Ghio, S.; Gibbs, S.; et al. Pulmonary hypertension in chronic lung diseases. J. Am. Coll. Cardiol. 2013, 62 (Suppl. S25), D109–D116. [Google Scholar] [CrossRef]
- Parikh, R.; Konstantinidis, I.; O’Sullivan, D.M.; Farber, H.W. Pulmonary hypertension in patients with interstitial lung disease: A tool for early detection. Pulm. Circ. 2022, 12, e12141. [Google Scholar] [CrossRef]
- Iwasawa, T.; Asakura, A.; Sakai, F.; Kanauchi, T.; Gotoh, T.; Ogura, T.; Yazawa, T.; Nishimura, J.; Inoue, T. Assessment of prognosis of patients with idiopathic pulmonary fibrosis by computer-aided analysis of CT images. J. Thorac. Imaging 2009, 24, 216–222. [Google Scholar] [CrossRef]
- Iwasawa, T.; Matsushita, S.; Hirayama, M.; Baba, T.; Ogura, T. Quantitative Analysis for Lung Disease on Thin-Section CT. Diagnostics 2023, 13, 2988. [Google Scholar] [CrossRef]
- Iwasawa, T.; Okudela, K.; Takemura, T.; Fukuda, T.; Matsushita, S.; Baba, T.; Ogura, T.; Tajiri, M.; Yoshizawa, A. Computer-aided Quantification of Pulmonary Fibrosis in Patients with Lung Cancer: Relationship to Disease-free Survival. Radiology 2019, 292, 489–498. [Google Scholar] [CrossRef]
- Iwasawa, T.; Takemura, T.; Okudera, K.; Gotoh, T.; Iwao, Y.; Kitamura, H.; Baba, T.; Ogura, T.; Oba, M.S. The importance of subpleural fibrosis in the prognosis of patients with idiopathic interstitial pneumonias. Eur. J. Radiol. 2017, 90, 106–113. [Google Scholar] [CrossRef]
- Kamide, H.; Kato, S.; Hayakawa, K.; Fukui, K.; Kitamura, H.; Ogura, T.; Iwasawa, T.; Kimura, K.; Tamura, K.; Utsunomiya, D. Impairment of right ventricular strain evaluated by cardiovascular magnetic resonance feature tracking in patients with interstitial lung disease. Int. J. Cardiovasc. Imaging 2021, 37, 1073–1083. [Google Scholar] [CrossRef]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef]
- Caminati, A.; Cassandro, R.; Harari, S. Pulmonary hypertension in chronic interstitial lung diseases. Eur. Respir. Rev. 2013, 22, 292–301. [Google Scholar] [CrossRef]
- Waxman, A.B.; Elia, D.; Adir, Y.; Humbert, M.; Harari, S. Recent advances in the management of pulmonary hypertension with interstitial lung disease. Eur. Respir. Rev. 2022, 31, 210220. [Google Scholar] [CrossRef] [PubMed]
- Hur, D.J.; Sugeng, L. Non-invasive Multimodality Cardiovascular Imaging of the Right Heart and Pulmonary Circulation in Pulmonary Hypertension. Front. Cardiovasc. Med. 2019, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Dorfmüller, P.; Shlobin, O.A.; Ventetuolo, C.E. Group 3 Pulmonary Hypertension: From Bench to Bedside. Circ. Res. 2022, 130, 1404–1422. [Google Scholar] [CrossRef] [PubMed]
- Nathan, S.D.; Barbera, J.A.; Gaine, S.P.; Harari, S.; Martinez, F.J.; Olschewski, H.; Olsson, K.M.; Peacock, A.J.; Pepke-Zaba, J.; Provencher, S.; et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur. Respir. J. 2019, 53, 1801914. [Google Scholar] [CrossRef]
- Dong, Z.; Dai, L.; Song, Y.; Ma, X.; Wang, J.; Yu, S.; Yang, S.; Yang, K.; Zhao, K.; Lu, M.; et al. Right Ventricular Strain Derived from Cardiac MRI Feature Tracking for the Diagnosis and Prognosis of Arrhythmogenic Right Ventricular Cardiomyopathy. Radiol. Cardiothorac. Imaging 2024, 6, e230292. [Google Scholar] [CrossRef]
- Lu, G.; Cao, L.; Ye, W.; Wei, X.; Xie, J.; Du, Z.; Zhang, X.; Luo, X.; Ou, J.; Zhang, Q.; et al. Incremental Prognostic Value of Cardiac MRI Feature Tracking and T1 Mapping in Arrhythmogenic Right Ventricular Cardiomyopathy. Radiol. Cardiothorac. Imaging 2024, 6, e230430. [Google Scholar] [CrossRef]
- Iwasawa, T.; Iwao, Y.; Takemura, T.; Okudela, K.; Gotoh, T.; Baba, T.; Ogura, T.; Oba, M.S. Extraction of the subpleural lung region from computed tomography images to detect interstitial lung disease. Jpn. J. Radiol. 2017, 35, 681–688. [Google Scholar] [CrossRef]
- Iwasawa, T.; Kato, S.; Ogura, T.; Kusakawa, Y.; Iso, S.; Baba, T.; Fukui, K.; Oba, M.S. Low-normal lung volume correlates with pulmonary hypertension in fibrotic idiopathic interstitial pneumonia: Computer-aided 3D quantitative analysis of chest CT. AJR Am. J. Roentgenol. 2014, 203, W166–W173. [Google Scholar] [CrossRef]
- King, T.E., Jr.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef]
- Richeldi, L.; du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 72) | Patients with PH (n = 21) | Patients Without PH (n = 51) | * p-Value | |
|---|---|---|---|---|
| Age | 70.5 ± 7.4 | 71.9 ± 6.1 | 70.0 ± 8.0 | 0.27 |
| Sex (Male) | 44 (61%) | 14 (67%) | 30 (59%) | |
| MRC dyspnea scale | 1.9 ± 1.1 | 2.8 ± 0.9 | 1.5 ± 0.9 | <0.001 |
| BMI (kg/m2) | 23.0 ± 3.1 | 23.2 ± 2.9 | 23.0 ± 3.2 | 0.77 |
| Systolic blood pressure (mmHg) | 136 ± 17 | 138 ± 15 | 135 ± 18 | 0.44 |
| Diastolic blood pressure (mmHg) | 77 ± 9.5 | 81 ± 9.8 | 76 ± 9.0 | 0.033 |
| Heart rate (bpm) | 74 ± 14 | 80 ± 16 | 72 ± 12 | 0.06 |
| BNP (pg/mL) | 59 ± 123 | 129 ± 211 | 30 ± 23 | 0.044 |
| Creatinine (mg/dL) | 1.0 ± 1.2 | 1.4 ± 2.2 | 0.8 ± 0.2 | 0.309 |
| KL-6 (U/mL) | 1025 ± 645 | 1057 ± 572 | 1011 ± 677 | 0.773 |
| LDH (IU/L) | 244 ± 54 | 249 ± 59 | 242 ± 52 | 0.645 |
| CRP (mg/dL) | 0.39 ± 0.55 | 0.51 ± 0.65 | 0.34 ± 0.50 | 0.296 |
| FVC, % predicted | 82 ± 23 | 72 ± 15 | 85 ± 25 | 0.01 |
| FEV1, % predicted | 78 ± 20 | 70 ± 19 | 81 ± 20 | 0.037 |
| DLco, % predicted | 65 ± 23 | 47 ± 17 | 71 ± 22 | <0.001 |
| Modality | Parameter | PH Present (n = 21) | PH Absent (n = 51) | * p-Value |
|---|---|---|---|---|
| MRI (Heart) | RV strain | −13.4 ± 5.1 | −16.4 ± 5.2 | 0.026 |
| RVESV | 74.2 ± 18.3 | 59.5 ± 14.2 | 0.003 | |
| CT (Lung) | Diseased area | 56.4 ± 17.2 | 38.4 ± 12.5 | <0.001 |
| GGO | 11.8 ± 3.6 | 8.65 ± 4.3 | 0.005 | |
| Emphysema | 17.4 ± 17.2 | 10.6 ± 12.9 | 0.12 | |
| Honeycomb | 17.7 ± 4.9 | 12.8 ± 6.4 | 0.0027 | |
| Reticulation | 8.10 ± 8.04 | 5.66 ± 5.75 | 0.23 | |
| Consolidation | 1.48 ± 3.20 | 0.662 ± 0.798 | 0.27 |
| Modality | Parameter | AUC | 95% CI | p-Value | Threshold | Sensitivity, % | Specificity, % |
|---|---|---|---|---|---|---|---|
| MRI (Heart) | RV strain | 0.665 | 0.522–0.808 | 0.022 | −12.5 | 57.1 | 78.4 |
| RVESV | 0.754 | 0.631–0.876 | <0.001 | 67.2 | 76.2 | 74.5 | |
| CT (Lung) | Diseased area | 0.778 | 0.685–0.921 | <0.001 | 53.6 | 57.1 | 88.2 |
| Emphysema | 0.622 | 0.451–0.755 | 0.101 | 9.93 | 66.7 | 68.6 | |
| GGO | 0.724 | 0.610–0.864 | 0.001 | 9.77 | 81.0 | 68.6 | |
| Consolidation | 0.622 | 0.526–0.775 | 0.058 | 0.21 | 100 | 39.2 | |
| Honeycomb | 0.738 | 0.634–0.864 | <0.001 | 14.8 | 71.4 | 68.6 | |
| Reticulation | 0.654 | 0.536–0.788 | 0.017 | 3.68 | 90.5 | 49.0 | |
| MRI + CT | Diseased area + RVESV | 0.846 | 0.748–0.944 | <0.001 | 0.186 | 90.5 | 68.6 |
| Diseased area + RVESV + RV strain | 0.860 | 0.767–0.953 | <0.001 | 0.361 | 76.2 | 84.3 |
| Improvement in Discrimination—AUC and NRI | ||||
|---|---|---|---|---|
| Model | AUC | NRI (Continuous) | 95% CI | p-Value |
| Diseased area only | 0.778 | |||
| Diseased area + RVESV | 0.847 | 0.700 | 0.247–1.154 | 0.002 |
| Diseased area + RVESV + RV strain | 0.854 | 0.6835 | 0.2147–1.1523 | 0.004 |
| Improvement in Reclassification—AUC and IDI | ||||
| Model | AUC | NRI (Continuous) | 95% CI | p-value |
| Diseased area only | 0.778 | |||
| Diseased area + RVESV | 0.847 | 0.0887 | 0.0097–0.1678 | 0.03 |
| Diseased area + RVESV + RV strain | 0.854 | 0.1222 | 0.0286–0.2158 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, K.; Kato, S.; Yasuda, N.; Sawamura, S.; Fukui, K.; Iwasawa, T.; Ogura, T.; Utsunomiya, D. Integrating CT-Based Lung Fibrosis and MRI-Derived Right Ventricular Function for the Detection of Pulmonary Hypertension in Interstitial Lung Disease. J. Clin. Med. 2025, 14, 5329. https://doi.org/10.3390/jcm14155329
Ito K, Kato S, Yasuda N, Sawamura S, Fukui K, Iwasawa T, Ogura T, Utsunomiya D. Integrating CT-Based Lung Fibrosis and MRI-Derived Right Ventricular Function for the Detection of Pulmonary Hypertension in Interstitial Lung Disease. Journal of Clinical Medicine. 2025; 14(15):5329. https://doi.org/10.3390/jcm14155329
Chicago/Turabian StyleIto, Kenichi, Shingo Kato, Naofumi Yasuda, Shungo Sawamura, Kazuki Fukui, Tae Iwasawa, Takashi Ogura, and Daisuke Utsunomiya. 2025. "Integrating CT-Based Lung Fibrosis and MRI-Derived Right Ventricular Function for the Detection of Pulmonary Hypertension in Interstitial Lung Disease" Journal of Clinical Medicine 14, no. 15: 5329. https://doi.org/10.3390/jcm14155329
APA StyleIto, K., Kato, S., Yasuda, N., Sawamura, S., Fukui, K., Iwasawa, T., Ogura, T., & Utsunomiya, D. (2025). Integrating CT-Based Lung Fibrosis and MRI-Derived Right Ventricular Function for the Detection of Pulmonary Hypertension in Interstitial Lung Disease. Journal of Clinical Medicine, 14(15), 5329. https://doi.org/10.3390/jcm14155329