
Practical Comprehensive Approach to Current Atrial Fibrillation Challenges: Insights from an Expert Panel

 , , , and
, , , and
Abstract

1. Introduction
2. Materials and Methods
3. Results
3.1. Participants
3.2. Questionnaire Results
3.3. Practical Recommendations
4. Discussion
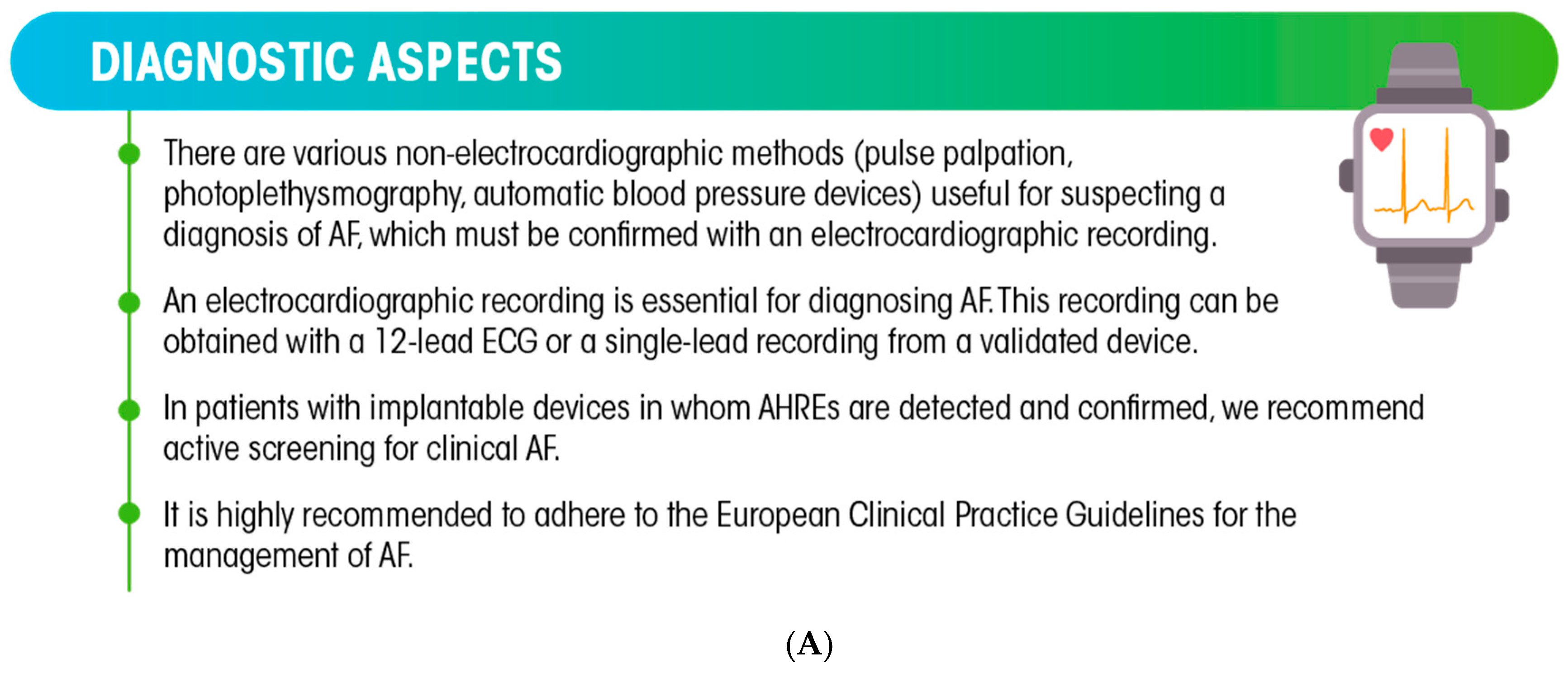
4.1. Diagnostic Aspects
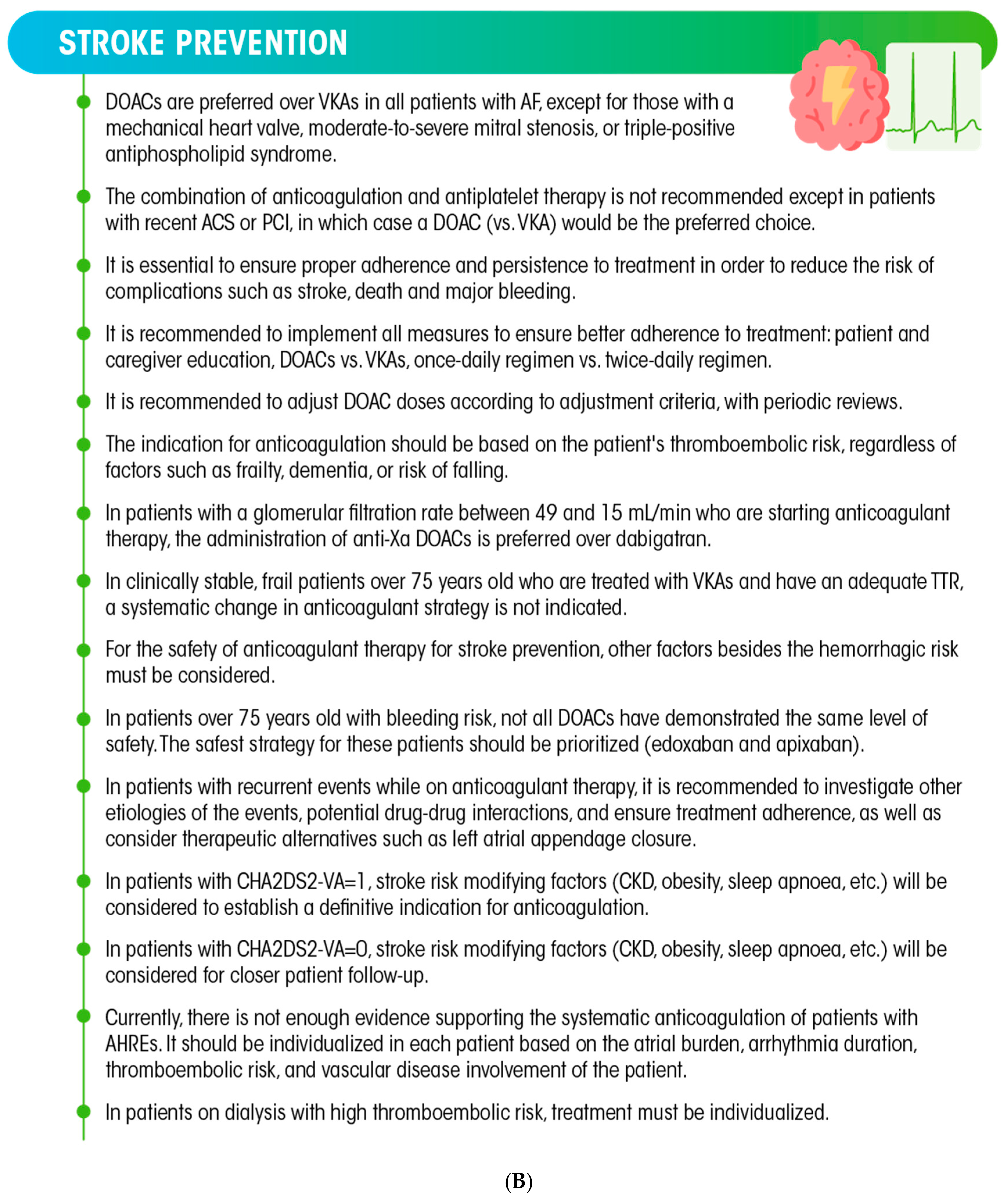
4.2. Stroke Prevention
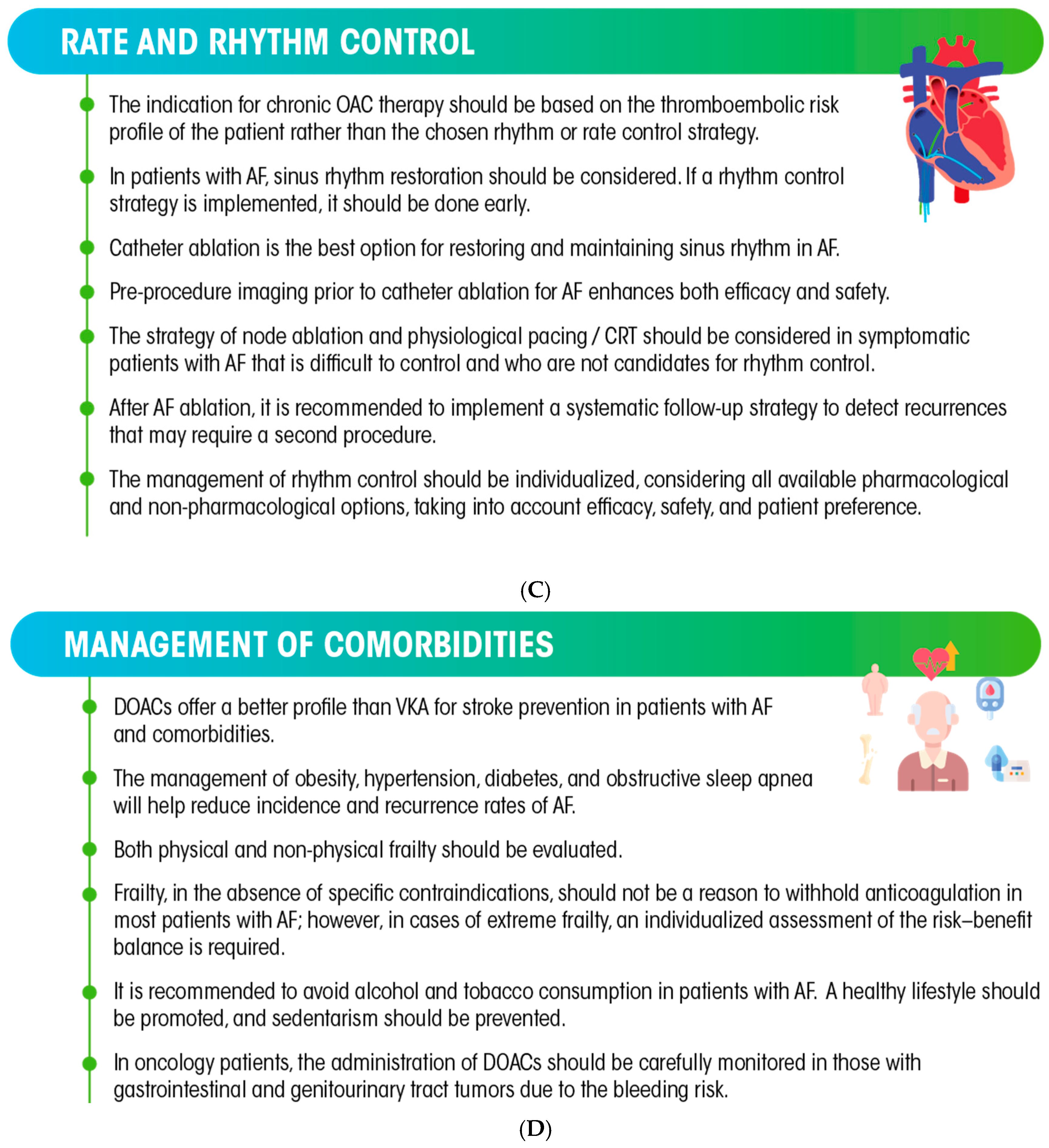
4.3. Rate and Rhythm Control
4.4. Management of Comorbidities
4.5. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barrios, V.; Calderón, A.; Escobar, C.; de la Figuera, M. Patients With Atrial Fibrillation in a Primary Care Setting: Val-FAAP Study. Rev. Esp. Cardiol. 2012, 65, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Doblas, J.J.; Muñiz, J.; Martin, J.J.A.; Rodríguez-Roca, G.; Lobos, J.M.; Awamleh, P.; Permanyer-Miralda, G.; Chorro, F.J.; Anguita, M.; Roig, E. Prevalence of atrial fibrillation in Spain. OFRECE study results. Rev. Esp. Cardiol. 2014, 67, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Guzmán, J.; Freixa-Pamias, R.; García-Alegría, J.; Cabeza, A.-I.P.; Roldán-Rabadán, I.; Antolin-Fontes, B.; Rebollo, P.; Llorac, A.; Genís-Gironés, M.; Escobar-Cervantes, C. Epidemiology of atrial fibrillation-related ischemic stroke and its association with DOAC uptake in Spain: First national population-based study 2005 to 2018. Rev. Esp. Cardiol. 2022, 75, 496–505. [Google Scholar] [CrossRef] [PubMed]
- López Soto, A.; Formiga, F.; Bosch, X.; García Alegría, J. Prevalence of atrial fibrillation and related factors in hospitalized old patients: ESFINGE study. Med. Clin. 2012, 138, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Sabín, J.; Quintana, M.; Masjuan, J.; Oliva-Moreno, J.; Mar, J.; Gonzalez-Rojas, N.; Becerra, V.; Torres, C.; Yebenes, M. Economic impact of patients admitted to stroke units in Spain. Eur. J. Health Econ. 2017, 18, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; Casado-Arroyo, R.; Caso, V.; Crijns, H.J.G.M.; De Potter, T.J.R.; Dwight, J.; Guasti, L.; Hanke, T.; et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2024, 45, 3314–3414. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1–e156. [Google Scholar] [CrossRef] [PubMed]
- Lévy, S.; Steinbeck, G.; Santini, L.; Nabauer, M.; Penela-Maceda, D.; Kantharia, B.K.; Saksena, S.; Cappato, R. Management of atrial fibrillation: Two decades of progress—A scientific statement from the European Cardiac Arrhythmia Society. J. Interv. Card. Electrophysiol. 2022, 65, 287–326. [Google Scholar] [CrossRef] [PubMed]
- Shiga, T.; Kimura, T.; Fukushima, N.; Yoshiyama, Y.; Iwade, K.; Mori, F.; Ajiro, Y.; Haruta, S.; Yamada, Y.; Sawada, E.; et al. Electronic monitoring of adherence to once-daily and twice-daily direct oral anticoagulants in patients with atrial fibrillation: Baseline data from the SMAAP-AF trial. J. Arrhythmia 2021, 37, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Grymonprez, M.; Capiau, A.; Steurbaut, S.; Mehuys, E.; Boussery, K.; De Backer, T.L.; Lahousse, L. Adherence and persistence to oral anticoagulants in patients with atrial fibrillation: A Belgian nationwide cohort study. Front. Cardiovasc. Med. 2022, 9, 994085. [Google Scholar] [CrossRef] [PubMed]
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 22, 55. [Google Scholar]
- Chen, W.; Zheng, P.; Bu, Y.; Xu, Y.; Lai, D. Achieving Real-Time Prediction of Paroxysmal Atrial Fibrillation Onset by Convolutional Neural Network and Sliding Window on R-R Interval Sequences. Bioengineering 2024, 11, 903. [Google Scholar] [CrossRef] [PubMed]
- Parks, A.L.; Frankel, D.S.; Kim, D.H.; Ko, D.; Kramer, D.B.; Lydston, M.; Fang, M.C.; Shah, S.J. Management of atrial fibrillation in older adults. BMJ 2024, 386, e076246. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Waalen, J.; Edwards, A.M.; Ariniello, L.M.; Mehta, R.R.; Ebner, G.S.; Carter, C.; Baca-Motes, K.; Felicione, E.; Sarich, T.; et al. Effect of a Home-Based Wearable Continuous ECG Monitoring Patch on Detection of Undiagnosed Atrial Fibrillation: The mSToPS Randomized Clinical Trial. JAMA 2018, 320, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-R.; Choi, E.-K.; Kwon, S.; Han, K.-D.; Jung, J.-H.; Cha, M.-J.; Oh, S.; Lip, G.Y. Effectiveness and Safety of Contemporary Oral Anticoagulants Among Asians With Nonvalvular Atrial Fibrillation. Stroke 2019, 50, 2245–2249. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Karthikeyan, G.; Ntsekhe, M.; Haileamlak, A.; El Sayed, A.; El Ghamrawy, A.; Damasceno, A.; Avezum, A.; Dans, A.M.L.; Gitura, B.; et al. Rivaroxaban in Rheumatic Heart Disease-Associated Atrial Fibrillation. N. Engl. J. Med. 2022, 387, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Connolly, S.J.; Brueckmann, M.; Granger, C.B.; Kappetein, A.P.; Mack, M.J.; Blatchford, J.; Devenny, K.; Friedman, J.; Guiver, K.; et al. Dabigatran versus warfarin in patients with mechanical heart valves. N. Engl. J. Med. 2013, 369, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Pengo, V.; Hoxha, A.; Andreoli, L.; Tincani, A.; Silvestri, E.; Prisco, D.; Fierro, T.; Gresele, P.; Cafolla, A.; De Micheli, V.; et al. Trial of Rivaroxaban in AntiPhospholipid Syndrome (TRAPS): Two-year outcomes after the study closure. J. Thromb. Haemost. 2021, 19, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Joosten, L.P.T.; van Doorn, S.; van de Ven, P.M.; Köhlen, B.T.G.; Nierman, M.C.; Koek, H.L.; Hemels, M.E.W.; Huisman, M.V.; Kruip, M.; Faber, L.M.; et al. Safety of Switching From a Vitamin K Antagonist to a Non-Vitamin K Antagonist Oral Anticoagulant in Frail Older Patients With Atrial Fibrillation: Results of the FRAIL-AF Randomized Controlled Trial. Circulation 2024, 149, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Grymonprez, M.; Steurbaut, S.; Capiau, A.; Vauterin, D.; Van Vaerenbergh, F.; Mehuys, E.; Boussery, K.; De Backer, T.L.; Lahousse, L. Minimal Adherence Threshold to Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation to Reduce the Risk of Thromboembolism and Death: A Nationwide Cohort Study. Cardiovasc. Drugs Ther. 2025, 39, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Komen, J.J.; Heerdink, E.R.; Klungel, O.H.; Mantel-Teeuwisse, A.K.; Forslund, T.; Wettermark, B.; Hjemdahl, P. Long-term persistence and adherence with non-vitamin K oral anticoagulants in patients with atrial fibrillation and their associations with stroke risk. Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, f72–f80. [Google Scholar] [CrossRef] [PubMed]
- López, R.Q.; Pérez, F.F.; Beyer-Westendorf, J. Adherence and persistence with direct oral anticoagulants by dose regimen: A systematic review. Br. J. Clin. Pharmacol. 2025, 91, 1096–1113. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Cools, F.; Virdone, S.; Bassand, J.-P.; Fitzmaurice, D.A.; Fox, K.A.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Mantovani, L.G.; et al. Mortality in Patients With Atrial Fibrillation Receiving Nonrecommended Doses of Direct Oral Anticoagulants. J. Am. Coll. Cardiol. 2020, 76, 1425–1436. [Google Scholar] [CrossRef] [PubMed]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef] [PubMed]
- Munoz, F.D.-C.; Gharacholou, S.M.; Munger, T.M.; Friedman, P.A.; Asirvatham, S.J.; Packer, D.L.; Noseworthy, P.A. Meta-Analysis of Renal Function on the Safety and Efficacy of Novel Oral Anticoagulants for Atrial Fibrillation. Am. J. Cardiol. 2016, 117, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Brachmann, J.; Sohns, C.; Andresen, D.; Siebels, J.; Sehner, S.; Boersma, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Schunkert, H.; et al. Atrial Fibrillation Burden and Clinical Outcomes in Heart Failure: The CASTLE-AF Trial. JACC Clin. Electrophysiol. 2021, 7, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Pierucci, N.; La Fazia, V.M.; Mohanty, S.; Schiavone, M.; Doty, B.; Gabrah, K.; Della Rocca, D.G.; Burkhardt, J.D.; Al-Ahmad, A.; Di Biase, L.; et al. Results of ICE-Guided Isolation of the Superior Vena Cava With Pulsed Field Ablation. JACC Clin. Electrophysiol. 2025, 11, 752–760. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Gerstenfeld, E.P.; Natale, A.; Whang, W.; Cuoco, F.A.; Patel, C.; Mountantonakis, S.E.; Gibson, D.N.; Harding, J.D.; Ellis, C.R.; et al. Pulsed Field or Conventional Thermal Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2023, 389, 1660–1671. [Google Scholar] [CrossRef] [PubMed]
- Palamà, Z.; Robles, A.G.; Paoletti, M.; Nesti, M.; De Ruvo, E.; Scarà, A.; Borrelli, A.; Luca, G.D.M.D.; Rillo, M.; Calò, L.; et al. Long-Term Follow-Up In Paroxysmal Atrial Fibrillation Patients With Documented Isolated Trigger. Front. Cardiovasc. Med. 2023, 10, 1115328. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Toennis, T.; Goette, A.; Camm, A.J.; Diener, H.C.; Becher, N.; Bertaglia, E.; Lundqvist, C.B.; Borlich, M.; Brandes, A.; et al. Anticoagulation with Edoxaban in Patients with Atrial High-Rate Episodes. N. Engl. J. Med. 2023, 389, 1167–1179. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.S.; Lopes, R.D.; Granger, C.B.; Alings, M.; Rivard, L.; McIntyre, W.F.; Atar, D.; Birnie, D.H.; Boriani, G.; Camm, A.J.; et al. Apixaban for Stroke Prevention in Subclinical Atrial Fibrillation. N. Engl. J. Med. 2024, 390, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Nalliah, C.J.; Wong, G.R.; Lee, G.; Voskoboinik, A.; Kee, K.; Goldin, J.; Watts, T.; Linz, D.; Parameswaran, R.; Sugumar, H.; et al. Impact of CPAP on the Atrial Fibrillation Substrate in Obstructive Sleep Apnea: The SLEEP-AF Study. JACC Clin. Electrophysiol. 2022, 8, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; De Caterina, R.; Manu, M.C.; Souza, J.; Pecen, L.; Kirchhof, P. Impact of Weight on Clinical Outcomes of Edoxaban Therapy in Atrial Fibrillation Patients Included in the ETNA-AF-Europe Registry. J. Clin. Med. 2021, 10, 2879. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Response | Number of Panelists n (%) | |
|---|---|---|
| Specialty | Cardiology | 33 (94%) |
| Internal medicine | 2 (6%) | |
| Type of institution | Hospital | 33 (94%) |
| Outpatient clinic | 2 (6%) | |
| Working group member in a scientific society | Yes | 23 (66%) |
| No | 12 (34%) | |
| Geographical localization | Castile and León | 2 (6%) |
| Castile-La Mancha | 1 (3%) | |
| Madrid | 5 (14%) | |
| Andalusia | 6 (17%) | |
| Valencian Community | 5 (14%) | |
| Catalonia | 5 (14%) | |
| Basque Country | 2 (6%) | |
| Extremadura | 1 (3%) | |
| Aragon | 1 (3%) | |
| Galicia | 3 (9%) | |
| Navarre | 1 (3%) | |
| Canary Islands | 1 (3%) | |
| Murcia | 1 (3%) | |
| Cantabria | 1 (3%) | |
| Years of experience in the management of patients with AF and treatment with OACs | 0–9 | 2 (6%) |
| 10–19 | 14 (40%) | |
| 20–29 | 16 (46%) | |
| ≥30 | 3 (8%) | |
| Monthly number of patients with AF treated with OACs | 25–50 | 17 (49%) |
| ≥50 | 18 (51%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escobar, C.; Camafort, M.; Fortuny, E.; Grymonprez, M.; Pérez-Cabeza, A.I.; de Backer, T.L.; Leaders Connect Group. Practical Comprehensive Approach to Current Atrial Fibrillation Challenges: Insights from an Expert Panel. J. Clin. Med. 2025, 14, 5199. https://doi.org/10.3390/jcm14155199
Escobar C, Camafort M, Fortuny E, Grymonprez M, Pérez-Cabeza AI, de Backer TL, Leaders Connect Group. Practical Comprehensive Approach to Current Atrial Fibrillation Challenges: Insights from an Expert Panel. Journal of Clinical Medicine. 2025; 14(15):5199. https://doi.org/10.3390/jcm14155199
Chicago/Turabian StyleEscobar, Carlos, Miguel Camafort, Elena Fortuny, Maxim Grymonprez, Alejandro Isidoro Pérez-Cabeza, Tine L. de Backer, and Leaders Connect Group. 2025. "Practical Comprehensive Approach to Current Atrial Fibrillation Challenges: Insights from an Expert Panel" Journal of Clinical Medicine 14, no. 15: 5199. https://doi.org/10.3390/jcm14155199
APA StyleEscobar, C., Camafort, M., Fortuny, E., Grymonprez, M., Pérez-Cabeza, A. I., de Backer, T. L., & Leaders Connect Group. (2025). Practical Comprehensive Approach to Current Atrial Fibrillation Challenges: Insights from an Expert Panel. Journal of Clinical Medicine, 14(15), 5199. https://doi.org/10.3390/jcm14155199