

The Impact of Chronic Alcohol Consumption on Cognitive Function in Older People
 ,
,  , and
, and
Abstract
1. Introduction
Objectives and Assumptions
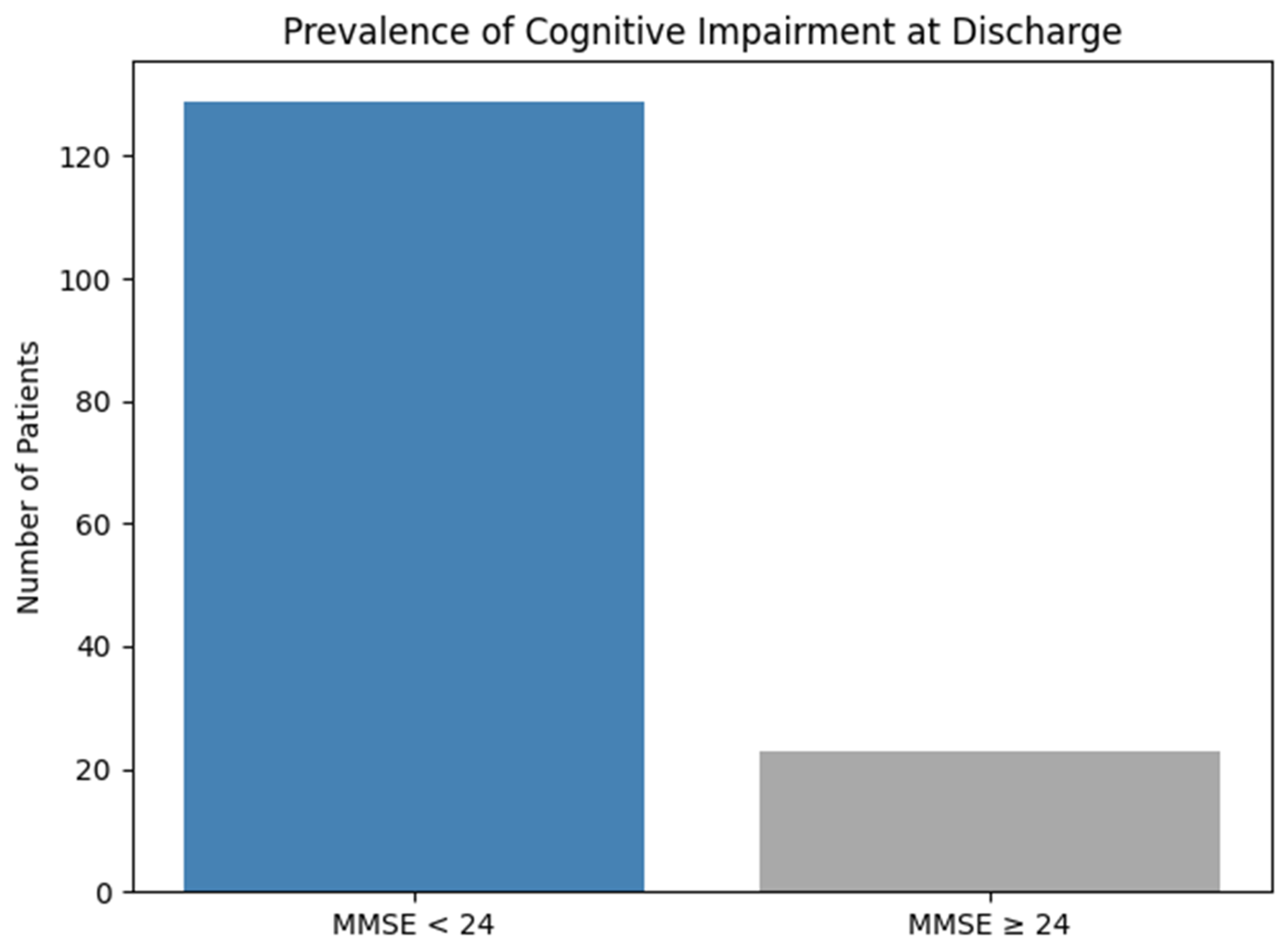
- MMSE score increases significantly at discharge, indicating a reversible component of the cognitive deterioration.
- Patients from rural environments present a lower initial MMSE score than those in the urban environment.
- Higher values of hepatic markers inversely correlate with cognitive performance.
- Older age is associated with lower MMSE scores, independent of hepatic status.
2. Materials and Methods
2.1. Study Design
2.2. Population and Inclusion Criteria
2.3. Data Collection
2.4. MMSE Administration
2.5. Statistical Analysis
3. Results
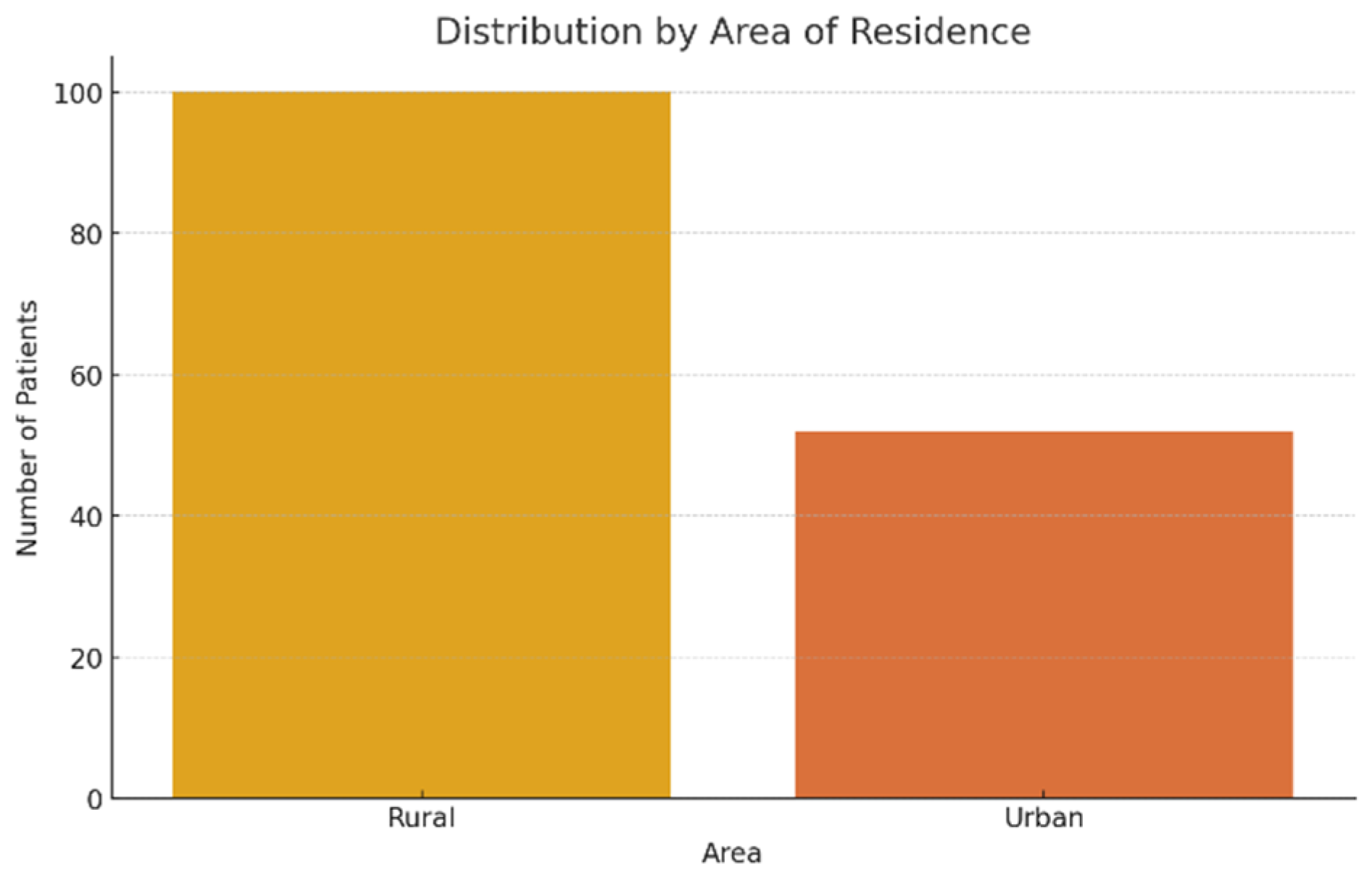
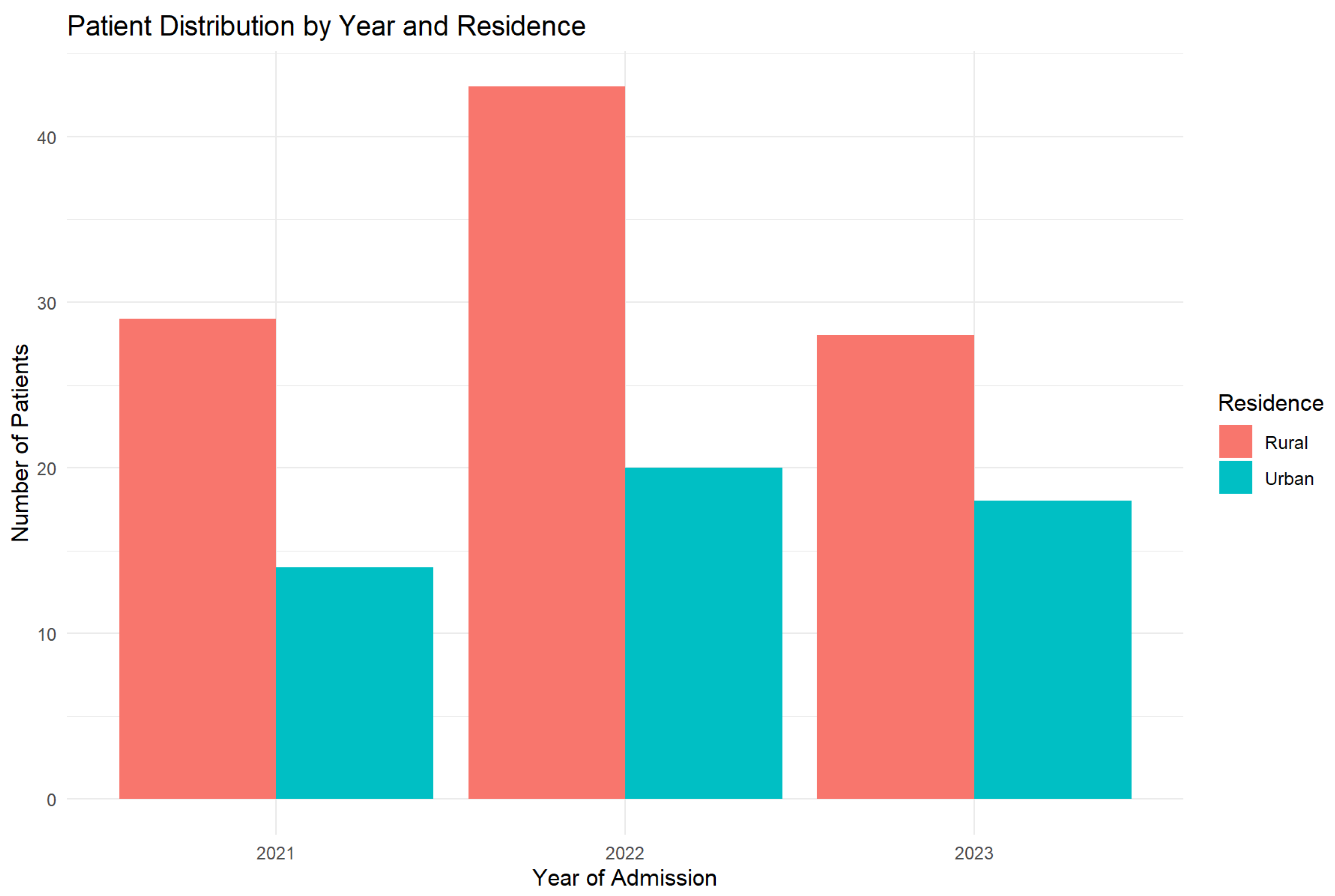
3.1. Demographic Characteristics
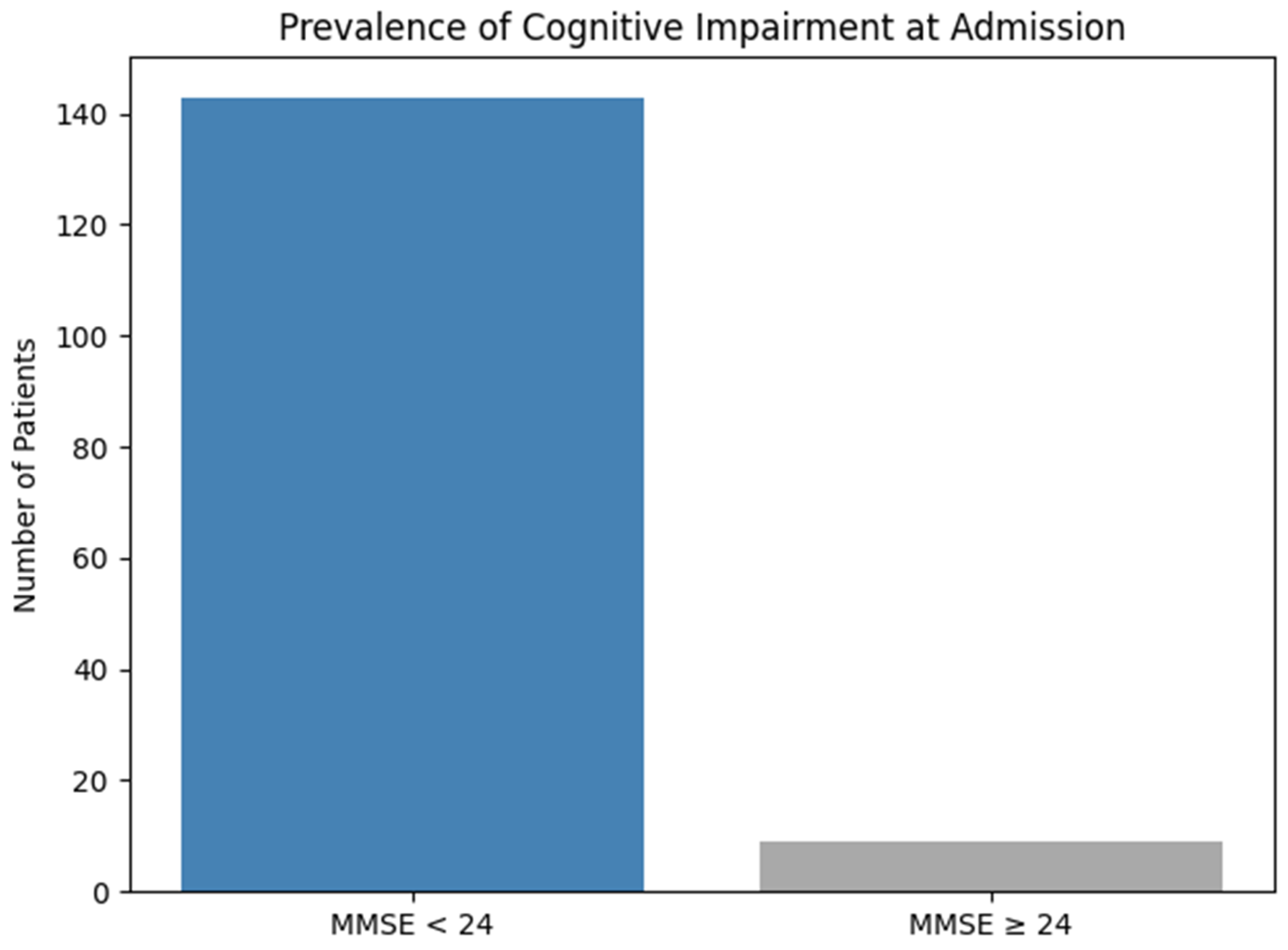
3.2. Cognitive Deficiency Prevalence
3.3. Statistical Associations
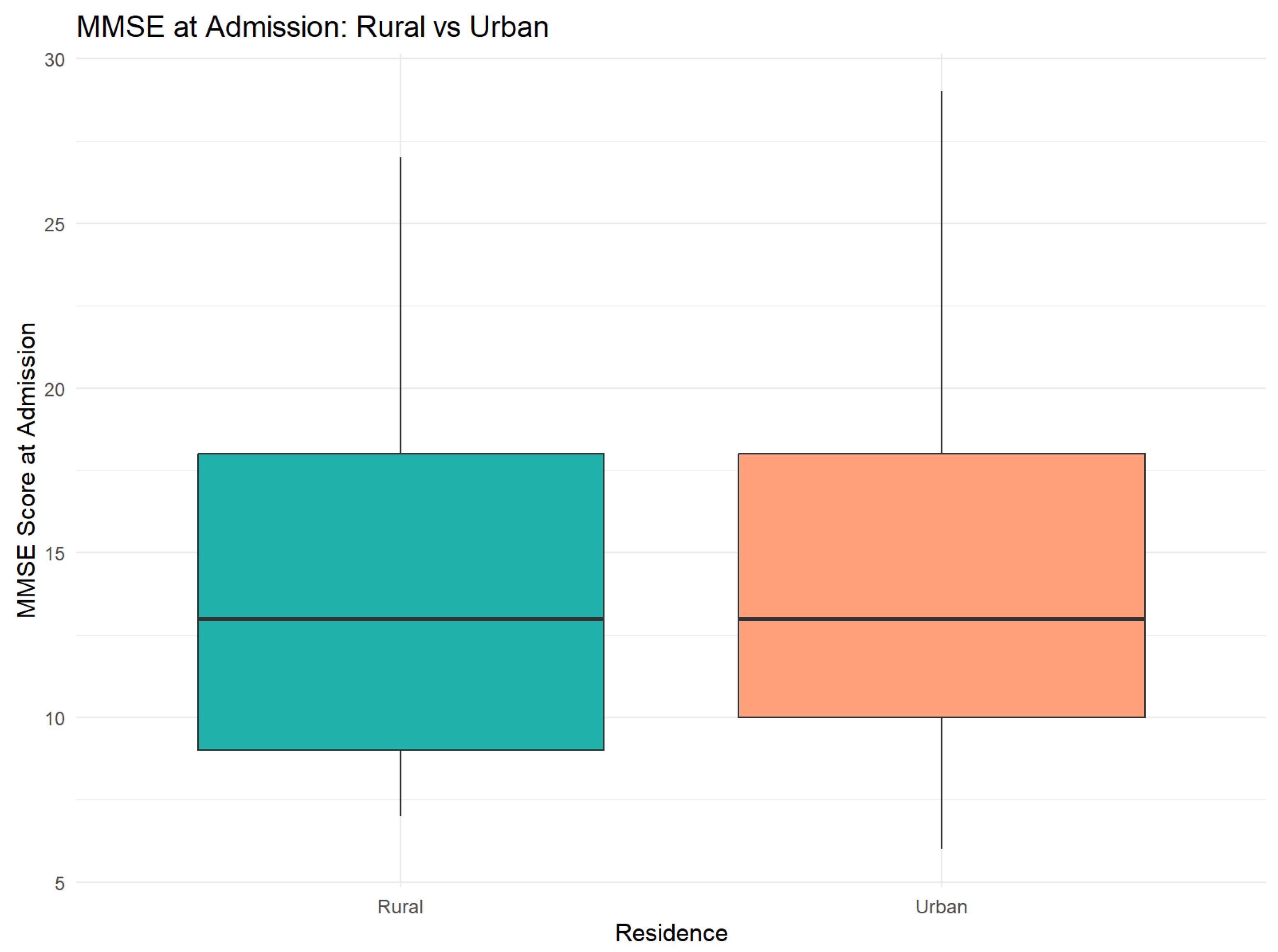
3.3.1. Significant Differences Between Rural and Urban Areas
- At the moment of admission: Insignificant difference (t = −0.06, p = 0.95), with similar areas (Rural: 14.31 vs. Urban: 14.37)
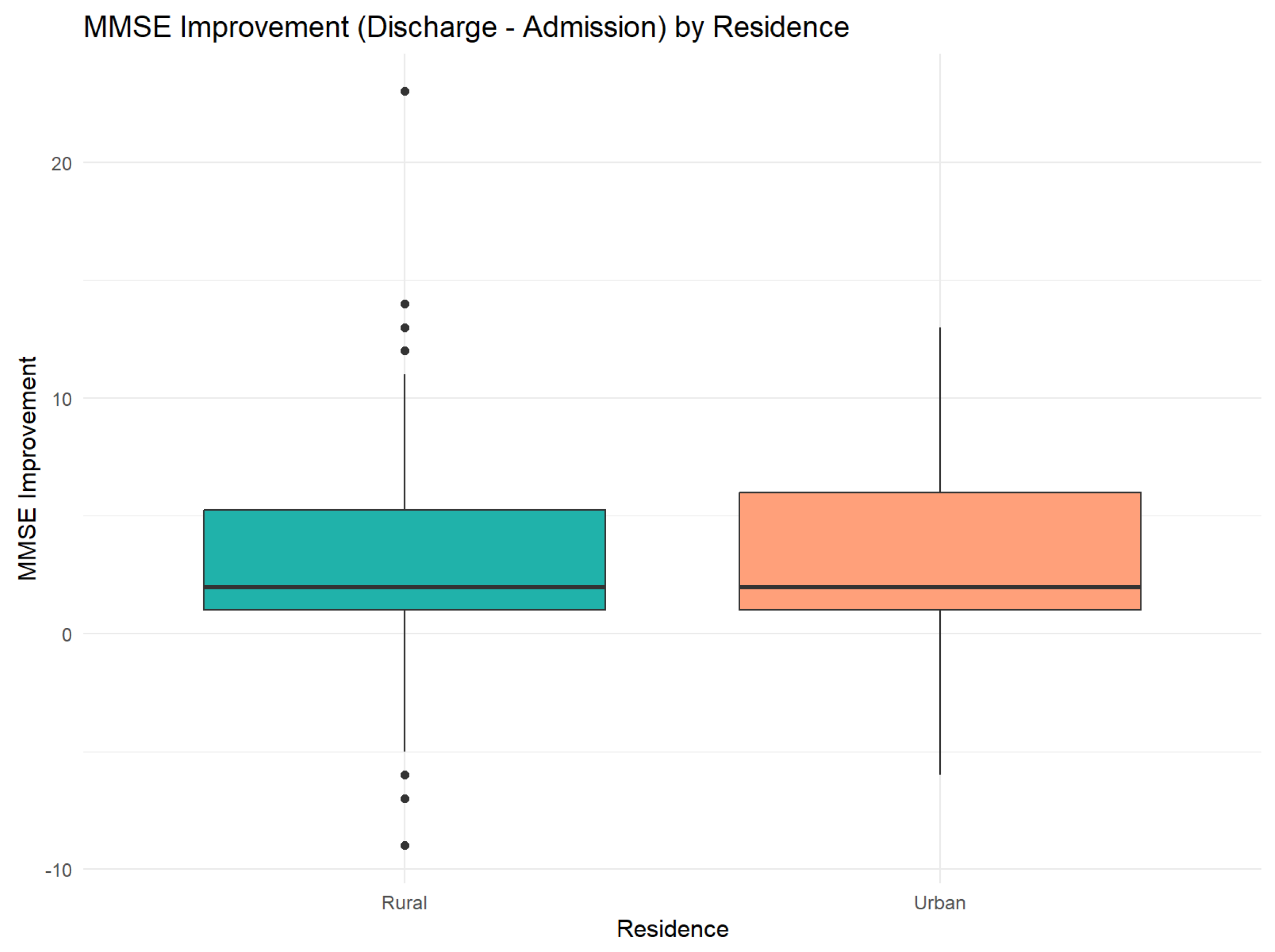
- At the moment of discharge: Average improvement of 3.26 points in both groups, with no significant differences between areas (t = −0.16, p = 0.88)
- In improvement: Patients from urban areas presented a more pronounced improvement tendency (+3.31 vs. +3.23), but the difference did not reach the statistical significance of 5. A detailed comparison of MMSE scores by residence is provided in Table 1.
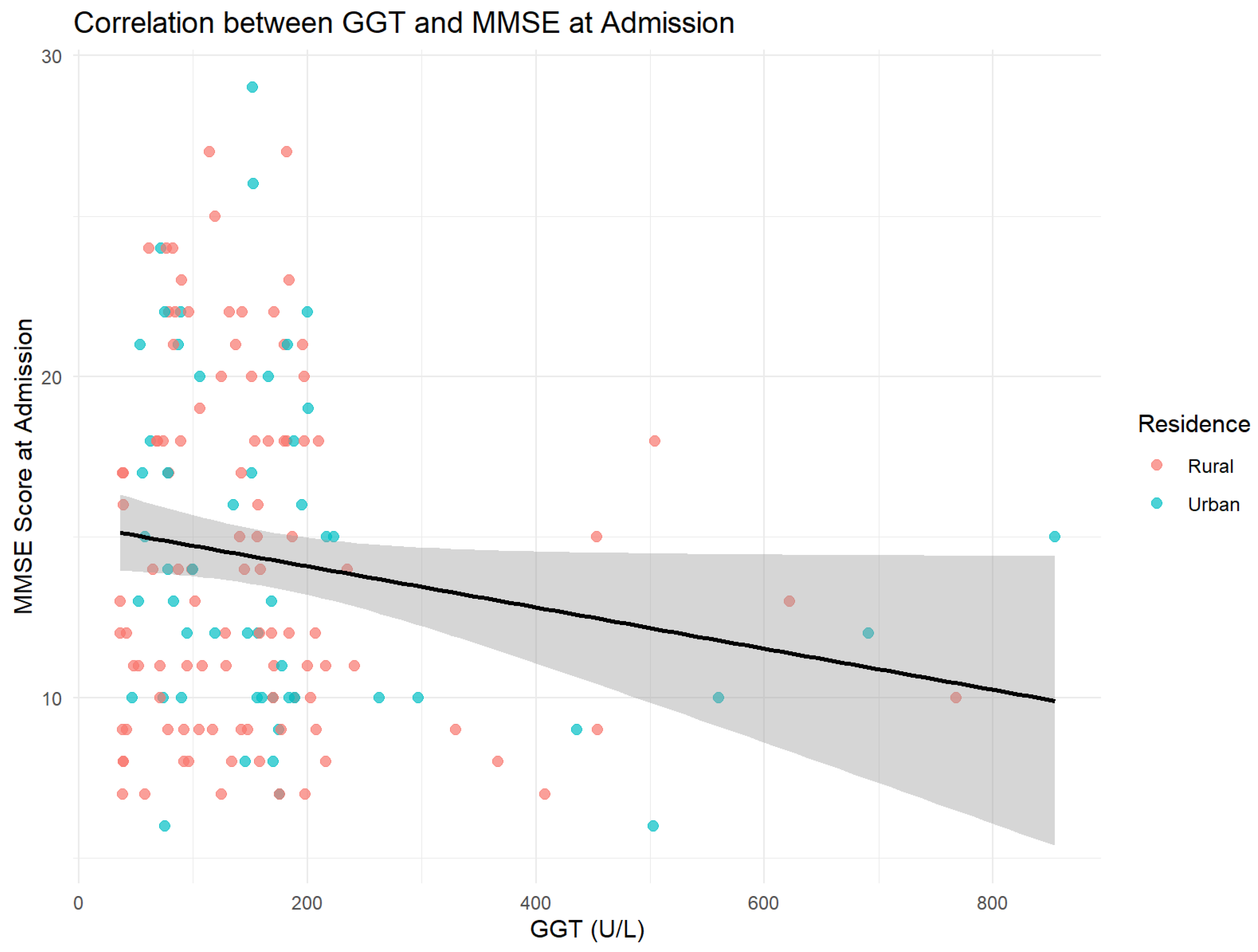
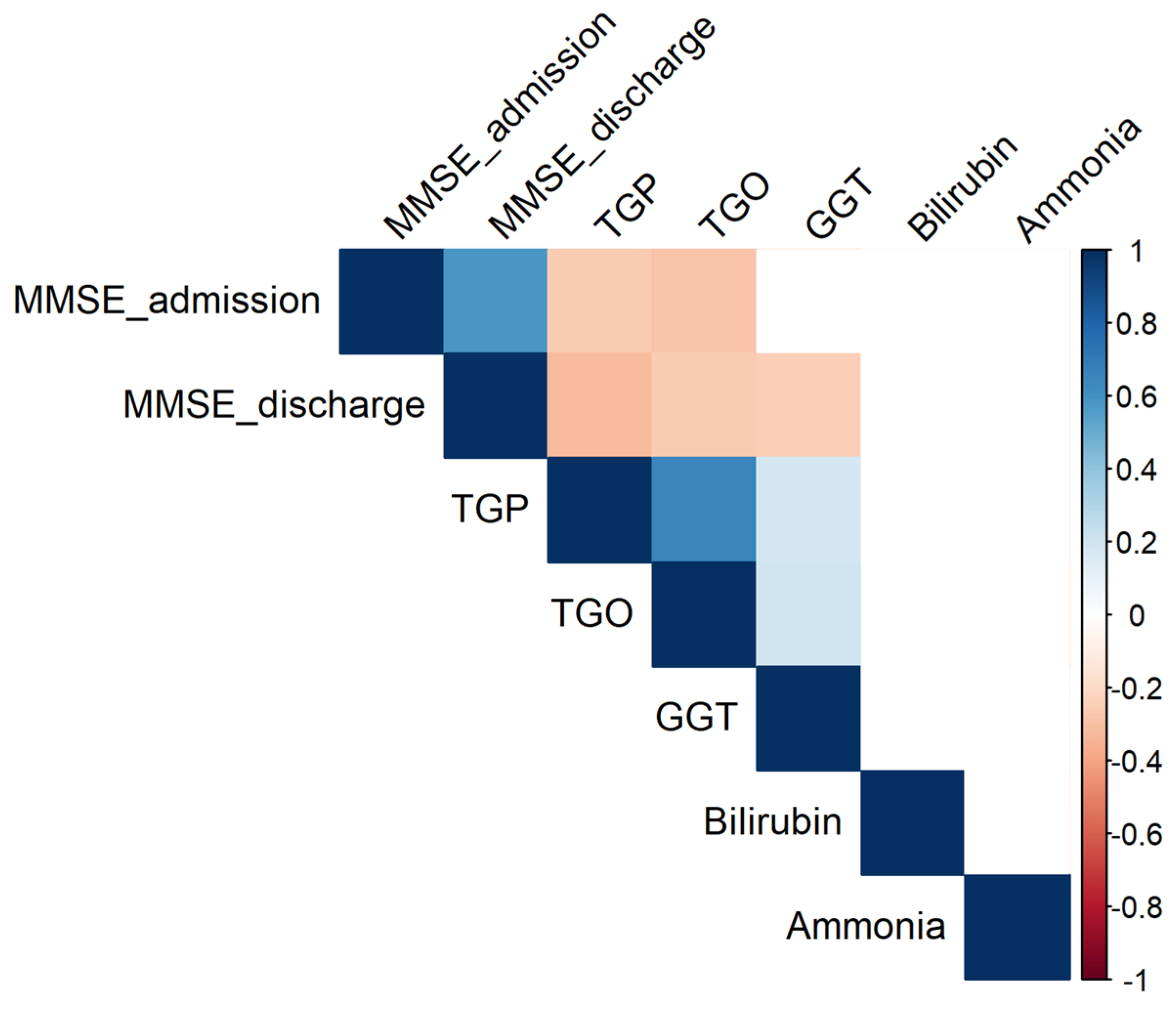
3.3.2. Correlations with Hepatic Parameters
- TGP: r = −0.26 (p = 0.0013)
- TGO: r = −0.29 (p = 0.0003);
- GGT: r = −0.16 (p = 0.05).
4. Discussion
- Interpreting the Main Findings
- Comparison with Literature
4.1. Rural–Urban Disparities
4.2. Hepatic Biomarkers and Cognition
4.3. Consumption Intensity and Non-Linear Model
4.4. Cognitive Recovery After Abstinence
- ○
- Support the literature linking chronic alcohol abuse with severe cognitive deterioration;
- ○
- Confirm the supplemental vulnerability of the rural residents;
- ○
- Reproduce the negative association between GGT and cognitive function;
- ○
- Break away from the studies suggesting benefits of moderate consumption, a discrepancy that can be explained by the severe consumption in our sample.
4.5. Study Limitations
4.6. Clinical Implications and Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MMSE | Mini-Mental State Examination |
| TGO | Aspartate transaminase (AST) |
| TGP | Alanine transaminase (ALT) |
| GGT | Gamma-glutamyl transferase (GGT) |
| NIAAA | National Institute on Alcohol Abuse and Alcoholism |
| EASL | The European Association for the Study of the Liver |
References
- Buzdugan, C.; Dincă, M. Controversa Demenței Asociate Consumului de Alcool. Rev. Psihol. 2022, 68, 297–308. [Google Scholar]
- Justo, A.F.O.; Paradela, R.; Goncalves, N.G.; Paes, V.R.; Leite, R.E.P.; Nitrini, R.; Pasqualucci, C.A.; Ferriolli, E.; Grinberg, L.T.; Suemoto, C.K. Association Between Alcohol Consumption, Cognitive Abilities, and Neuropathologic Changes. Neurology 2025, 104, e213555. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Hasan, O.S.M.; Black, S.E.; Shield, K.D.; Schwarzinger, M. Alcohol Use and Dementia: A Systematic Scoping Review. Alzheimer’s Res. Ther. 2019, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Global Aging. Available online: https://www.nia.nih.gov/research/dbsr/global-aging (accessed on 12 May 2025).
- Jarzebski, M.P.; Elmqvist, T.; Gasparatos, A.; Fukushi, K.; Eckersten, S.; Haase, D.; Goodness, J.; Khoshkar, S.; Saito, O.; Takeuchi, K.; et al. Ageing and Population Shrinking: Implications for Sustainability in the Urban Century. NPJ Urban Sustain. 2021, 1, 1–11. [Google Scholar] [CrossRef]
- Ageing: Global Population. Available online: https://www.who.int/news-room/questions-and-answers/item/population-ageing (accessed on 12 May 2025).
- Romania Proportion of Population Aged 65 and over 2025 Data 2026 Forecast 2010–2024 Historical. Available online: https://tradingeconomics.com/romania/proportion-of-population-aged-65-over-eurostat-data.html (accessed on 12 May 2025).
- Demography of Europe—An Ageing Population. Available online: https://ec.europa.eu/eurostat/cache/beta/demography/ee_et/bloc-1c.html?lang=en (accessed on 12 May 2025).
- Romania to Enter UN List of Super-Aged Societies in 2025. Available online: https://www.romania-insider.com/romania-un-list-super-aged-societies-2025 (accessed on 12 May 2025).
- Romania. Available online: https://data.who.int/countries/642 (accessed on 12 May 2025).
- O’Connell, H.; Chin, A.-V.; Cunningham, C.; Lawlor, B. Alcohol Use Disorders Elderly People–Redefining Age Old Problem in Old Age. BMJ 2003, 327, 664–667. [Google Scholar] [CrossRef]
- No Level of Alcohol Consumption Is Safe for Our Health. Available online: https://www.who.int/europe/news/item/04-01-2023-no-level-of-alcohol-consumption-is-safe-for-our-health (accessed on 12 May 2025).
- Religa, D.; Tsevis, T.; Wahlund, L.-O. Alcohol Abuse and Addiction in Older People. In Psychogeriatrics: A Clinical Guide; Veronese, N., Marseglia, A., Eds.; Springer International Publishing: Cham, Switzerland, 2024; pp. 31–55. ISBN 978-3-031-58488-6. [Google Scholar]
- Health, T.L.P. Reinvigorating the Public Health Response to Dementia. Lancet Public Health 2021, 6, e696. [Google Scholar] [CrossRef]
- Aye, S.; Bouteloup, V.; Tate, A.; Wimo, A.; Handels, R.; Jean, D.; Winblad, B.; Jönsson, L. Health-Related Quality of Life in Subjective Cognitive Decline and Mild Cognitive Impairment: A Longitudinal Cohort Analysis. Alzheimer’s Res. Ther. 2023, 15, 200. [Google Scholar] [CrossRef]
- MacLeod, C.A.; Bu, F.; Rutherford, A.C.; Phillips, J.; Woods, R. Cognitive Impairment Negatively Impacts Allied Health Service Uptake: Investigating the Association between Health and Service Use. SSM Popul. 2021, 13, 100720. [Google Scholar] [CrossRef]
- ADI-WHO Launches Global Status Report on Public Health Response to Dementia. Available online: https://www.alzheimer-europe.org/policy/global-action/who-global-status-report-dementia (accessed on 12 May 2025).
- Landeiro, F.; Mughal, S.; Walsh, K.; Nye, E.; Morton, J.; Williams, H.; Ghinai, I.; Castro, Y.; Leal, J.; Roberts, N.; et al. Health-Related Quality of Life in People with Predementia Alzheimer’s Disease, Mild Cognitive Impairment or Dementia Measured with Preference-Based Instruments: A Systematic Literature Review. Alzheimer’s Res. Ther. 2020, 12, 154. [Google Scholar] [CrossRef]
- Moroianu, M.; Moroianu, L.-A.; Ciubară, A.; Matei, M.N. Persistent Depressive Disorder: The Clinical Approach of the Patient Associating Depression and Dental Pathology—Case Report and Clinical Considerations. BRAIN Broad Res. Artif. Intell. Neurosci. 2022, 13, 229–238. [Google Scholar] [CrossRef]
- Moroianu, L.-A.; Curis, C.; Moroianu, M.; Stefanescu, C.; Ciubara, A. Optimism as a Resource and form of Manifesting Positive Affectiveness in the Elderly and Young Adults Pre-Pandemic vs. Pandemic—Comparative Study. BRAIN Broad Res. Artif. Intell. Neurosci. 2024, 15, 240–257. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Lee, D.Y.; Lee, B.C.; Jung, M.H.; Kim, H.; Choi, Y.S.; Choi, I.-G. Alcohol and Cognition in the Elderly: A Review. Psychiatry Investig. 2012, 9, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.C.; Wang, L.; Manning, K.J.; Holzhauer, C.G. Alcohol Use Disorder in Older Adults A Review of Recent Literature on Epidemiology, Cognitive Outcomes, and Neuroimaging Finding sand Treatment. Am. J. Geriatr. Psychiatry: Open Sci. Educ. Pract. 2024, 1, 39–51. [Google Scholar] [CrossRef]
- Ridley, N.J.; Draper, B.; Withall, A. Alcohol-Related Dementia: An Update of the Evidence. Alzheimer’s Res. Ther. 2013, 5, 3. [Google Scholar] [CrossRef]
- Koch, M.; Fitzpatrick, A.L.; Rapp, S.R.; Nahin, R.L.; Williamson, J.D.; Lopez, O.L.; DeKosky, S.T.; Kuller, L.H.; Mackey, R.H.; Mukamal, K.J.; et al. Alcohol Consumption and Risk of Dementia and Cognitive Decline Among Older Adults With or Without Mild Cognitive Impairment. JAMA Netw. Open 2019, 2, e1910319. [Google Scholar] [CrossRef]
- Hulse, G.K.; Lautenschlager, N.T.; Tait, R.J.; Almeida, O.P. Dementia Associated with Alcoholand Other Drug Use. Int. Psychogeriatr. 2005, 17, S109–S127. [Google Scholar] [CrossRef]
- Eva, L.; Brehar, F.-M.; Florian, I.-A.; Covache-Busuioc, R.-A.; Costin, H.P.; Dumitrascu, D.-I.; Bratu, B.-G.; Glavan, L.-A.; Ciurea, A.V. Neuropsychiatric and Neuropsychological Aspects of Alcohol-Related Cognitive Disorders: An In-Depth Review of Wernicke’s Encephalopathy and Korsakoff’s Syndrome. J. Clin. Med. 2023, 12, 6101. [Google Scholar] [CrossRef]
- Devabhaktuni, S.; Patkar, P.; Pooja, V.; Dhamija, S.; Gupta, N.; Chaudhury, S.; Saldanha, D. Differentiation of Hepatic Encephalopathy from Delirium Tremens: A Case Seriesand Review. Ind. Psychiatry J. 2021, 30, S214. [Google Scholar] [CrossRef]
- Cordova-Gallardo, J.; Vargas-Beltran, A.M.; Armendariz-Pineda, S.M.; Ruiz-Manriquez, J.; Ampuero, J.; Torre, A. Brain Reserve in Hepatic Encephalopathy: Pathways of Damage and Preventive Strategies through Lifestyle and Therapeutic Interventions. Ann. Hepatol. 2025, 30, 101740. [Google Scholar] [CrossRef]
- Subramaniyan, V.; Chakravarthi, S.; Jegasothy, R.; Seng, W.Y.; Fuloria, N.K.; Fuloria, S.; Hazarika, I.; Das, A. Alcohol-Associated Liver Disease: A Review on Its Pathophysiology, Diagnosis and Drug Therapy. Toxicol. Rep. 2021, 8, 376–385. [Google Scholar] [CrossRef]
- Ciobanu, A.M.; Petrescu, C.; Anghele, C.; Manea, M.C.; Ciobanu, C.A.; Petrescu, D.M.; Antonia, M.O.; Riga, S. Severe Vitamin D Deficiency—A Possible Cause of Resistance to Treatment in Psychiatric Pathology. Medicina 2023, 59, 2056. [Google Scholar] [CrossRef]
- Curis, C.; Moroianu, M.; Moroianu, L.-A.; Pintilei, D.R.; Ardeleanu, V.; Bobirca, A.; Mahler, B.; Stoian, A.P. Intuitive Nutrition Co-Factor of Emotional Equilibrium for Maintaining Nutritional Balance: A Prospective Study. Mediterr. J. Clin. 2023, 11, 1–26. [Google Scholar] [CrossRef]
- Mitincu-Caramfil, S.D.; Moroianu, L.-A.; Bradeanu, A.V.; Isailă, O.-M.; Curis, C.; Drima, E. The Correlation Between Emotionality Changes and Alcohol Consumption in Young Persons: A Pilot Study. Healthcare 2025, 13, 987. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Elbaz, A.; Britton, A.; Bell, S.; Dugravot, A.; Shipley, M.; Kivimaki, M.; Singh-Manoux, A. Alcohol Consumption and Cognitive Decline in Early Old Age. Neurology 2014, 82, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Mende, M.A. Alcohol in the Aging Brain—The Interplay Between Alcohol Consumption, Cognitive Decline and the Cardiovascular System. Front. Neurosci. 2019, 13, 713. [Google Scholar] [CrossRef]
- Topiwala, A.; Wang, C.; Ebmeier, K.P.; Burgess, S.; Bell, S.; Levey, D.F.; Zhou, H.; McCracken, C.; Roca-Fernández, A.; Petersen, S.E.; et al. Associations between Moderate Alcohol Consumption, Brain Iron, and Cognition in UK Biobank Participants: Observational and Mendelian Randomization Analyses. PLoS Med. 2022, 19, e1004039. [Google Scholar] [CrossRef]
- Zarezadeh, M.; Mahmoudinezhad, M.; Faghfouri, A.H.; Honarvar, N.M.; Regestein, Q.R.; Papatheodorou, S.I.; Mekary, R.A.; Willett, W.C. Alcohol Consumption in Relation to Cognitive Dysfunction and Dementia: A Systematic Review and Dose-Response Meta-Analysis of Comparative Longitudinal Studies. Ageing Res. Rev. 2024, 100, 102419. [Google Scholar] [CrossRef]
- Chen, K.; Li, Y.; Yue, R.; Jin, Z.; Cui, S.; Zhang, X.; Zhu, D.; Li, Q. A Nonlinear Relationship between Alcohol Consumption and Cognitive Function in Elderly People: A Population-Based Study from NHANES 2011–2014. Front. Aging Neurosci. 2024, 16, 1458274. [Google Scholar] [CrossRef]
- Díaz-Camargo, E.; Hernández-Lalinde, J.; Sánchez-Rubio, M.; Chaparro-Suárez, Y.; Álvarez-Caicedo, L.; Fierro-Zarate, A.; Gravini-Donado, M.; García-Pacheco, H.; Rojas-Quintero, J.; Bermúdez, V. NHANES 2011–2014 Reveals Decreased Cognitive Performance in U.S. Older Adults with Metabolic Syndrome Combinations. Int. J. Environ. Public Health 2023, 20, 5257. [Google Scholar] [CrossRef]
- Jeon, K.H.; Han, K.; Jeong, S.-M.; Park, J.; Yoo, J.E.; Yoo, J.; Lee, J.; Kim, S.; Shin, D.W. Changes in Alcohol Consumption and Risk of Dementia in a Nationwide Cohort in South Korea. JAMA Netw. Open 2023, 6, e2254771. [Google Scholar] [CrossRef]
- Sabia, S.; Fayosse, A.; Dumurgier, J.; Dugravot, A.; Akbaraly, T.; Britton, A.; Kivimäki, M.; Singh-Manoux, A. Alcohol Consumption and Risk of Dementia: 23 Year Follow-up of Whitehall II Cohort Study. BMJ 2018, 362, k2927. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Si, W.; Zhu, C.; Zhao, Q. Alcohol Consumption and Mild Cognitive Impairment: A Mendelian Randomization Study from Rural China. Nutrients 2022, 14, 3596. [Google Scholar] [CrossRef] [PubMed]
- Morega, S.; Ionele, C.-M.; Podeanu, M.-A.; Florescu, D.-N.; Rogoveanu, I. Assessment of Cognitive Function in Romanian Patients with Chronic Alcohol Consumption. Gastroenterol. Insights 2024, 15, 433–446. [Google Scholar] [CrossRef]
- Weden, M.M.; Shih, R.A.; Kabeto, M.U.; Langa, K.M. Secular Trends in Dementiaand Cognitive Impairment of U.S. Rural and Urban Older Adults. Am. J. Prev. Med. 2018, 54, 164–172. [Google Scholar] [CrossRef]
- Xu, W.Y.; Jung, J.; Retchin, S.M.; Li, Y.; Roy, S. Rural-Urban Disparities in Diagnosis of Early-Onset Dementia. JAMA Netw. Open 2022, 5, e2225805. [Google Scholar] [CrossRef]
- Steinberg, N.; Parisi, J.M.; Feger, D.M.; Clay, O.J.; Willis, S.L.; Ball, K.K.; Marsiske, M.; Harrell, E.R.; Sisco, S.M.; Rebok, G.W. Rural-Urban Differences in Cognition: Findings from the Advanced Cognitive Training for Independent and Vital Elderly Trial. J. Aging Health 2023, 35, 107S–118S. [Google Scholar] [CrossRef]
- Liu, C.-C.; Liu, C.-H.; Sun, Y.; Lee, H.-J.; Tang, L.-Y.; Chiu, M.-J. Rural-Urban Disparities in the Prevalence of Mild Cognitive Impairment and Dementia in Taiwan: A Door-to-Door Nationwide Study. J. Epidemiol. 2022, 32, 502–509. [Google Scholar] [CrossRef]
- Kramer, M.; Cutty, M.; Knox, S.; Alekseyenko, A.V.; Mollalo, A. Rural–Urban Disparities of Alzheimer’s Disease and Related Dementias: A Scoping Review. Alzheimer’s Dementia Transl. Clin. 2025, 11, e70047. [Google Scholar] [CrossRef]
- Bartley, M.M.; Baer-Benson, H.; Schroeder, D.R.; Sauver, J.L.S.; Khera, N.; Griffin, J.M. Social Determinants of Health among Older Adults with Dementia in Urban and Rural Areas. J. Prev. Alzheimer’s Dis. 2023, 10, 895–902. [Google Scholar] [CrossRef]
- Hahn, L.; Kessler, J. A New Scoring System for Increasing the Sensitivity of the MMSE. Z. Für Gerontol. Und Geriatr. 2020, 53, 156–162. [Google Scholar] [CrossRef]
- Kilian, C.; Klinger, S.; Rehm, J.; Manthey, J. Alcohol Use, Dementia Risk, and Sex: A Systematic Review and Assessment of Alcohol-Attributable Dementia Cases in Europe. BMC Geriatr. 2023, 23, 246. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.-J.; Yu, Y.-X.; Tian, K.; Yong, W.; Yu, W.-L.; Bai, R.-Y.; Wu, L.-E.; Guo, X. Prevalence and Risk Factors of Subjective Cognitive Decline in Older Adults in Baotou, China: A Cross-Sectional Study. Front. Aging Neurosci. 2024, 16, 1422258. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-L.; Jia, S.-Y.; Yang, B.; Miao, J.; Su, C.; Cui, Z.-G.; Yang, L.-M.; Guo, J.-H. Non-Linear Association of Liver Enzymes with Cognitive Performance in the Elderly: A Cross-Sectional Study. PLoS ONE 2024, 19, e0306839. [Google Scholar] [CrossRef] [PubMed]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2020, 323, 764. [Google Scholar] [CrossRef]
- US Preventive Services Task Force; Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W.; Kubik, M.; et al. Screening for Cognitive Impairment in Older Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2020, 323, 757. [Google Scholar] [CrossRef]
- Maciosek, M.V.; LaFrance, A.B.; Dehmer, S.P.; McGree, D.A.; Flottemesch, T.J.; Xu, Z.; Solberg, L.I. Updated Priorities Among Effective Clinical Preventive Services. Ann. Fam. Med. 2017, 15, 14–22. [Google Scholar] [CrossRef]
- Williams, E.C.; Achtmeyer, C.E.; Young, J.P.; Rittmueller, S.E.; Ludman, E.J.; Lapham, G.T.; Lee, A.K.; Chavez, L.J.; Berger, D.; Bradley, K.A. Local Implementation of Alcohol Screening and Brief Intervention at Five Veterans Health Administration Primary Care Clinics: Perspectives of Clinicaland Administrative Staff. J. Subst. Abus. Treat. 2016, 60, 27–35. [Google Scholar] [CrossRef]
- Johnson, M.; Jackson, R.; Guillaume, L.; Meier, P.; Goyder, E. Barrier sand Facilitators to Implementing Screening and Brief Intervention for Alcohol Misuse: A Systematic Review of Qualitative Evidence. J. Public Health 2011, 33, 412–421. [Google Scholar] [CrossRef]
- König, A.; Zeghari, R.; Guerchouche, R.; Tran, M.D.; Bremond, F.; Linz, N.; Lindsay, H.; Langel, K.; Ramakers, I.; Lemoine, P.; et al. Remote Cognitive Assessment of Older Adults in Rural Areas by Telemedicine and Automatic Speech and Video Analysis: Protocol for a Cross-Over Feasibility Study. BMJ Open 2021, 11, e047083. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practical Guidelines: Management of Alcoholic Liver Disease. J. Hepatol. 2012, 57, 399–420. [Google Scholar] [CrossRef]
- Musto, J.A.; Brown, R.; Lucey, M.R. Is There a Safe Limit for Consumption of Alcohol? J. Hepatol. 2025, 82, 535–540. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Rural (N = 97) M ± SD | Urban (N = 55) M ± SD | T(DF) | p-Value |
|---|---|---|---|---|
| MMSE at admission | 22.6 ± 3.9 | 24.8 ± 4.2 | 238 | 2 |
| MMSE at discharge | 25.0 ± 3.7 | 25.2 ± 3.5 | 15 | 88 |
| MMSE improvement (δ) | 2.4 ± 1.9 | 2.3 ± 2.1 | 18 | 86 |
| Hepatic Parameter | Pearson R | p-Value |
|---|---|---|
| TGP | −0.26 | 0.0013 |
| TGO | −0.29 | 0.0003 |
| GGT | −0.41 | <0.001 |
| Total bilirubin | −0.06 | 0.47 |
| Ammonia | −0.06 | 0.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitincu-Caramfil, S.-D.; Plesea-Condratovici, A.; Balta, A.A.S.; Bulza, V.; Bradeanu, A.-V.; Moroianu, L.-A.; Isailă, O.-M.; Drima, E. The Impact of Chronic Alcohol Consumption on Cognitive Function in Older People. J. Clin. Med. 2025, 14, 4595. https://doi.org/10.3390/jcm14134595
Mitincu-Caramfil S-D, Plesea-Condratovici A, Balta AAS, Bulza V, Bradeanu A-V, Moroianu L-A, Isailă O-M, Drima E. The Impact of Chronic Alcohol Consumption on Cognitive Function in Older People. Journal of Clinical Medicine. 2025; 14(13):4595. https://doi.org/10.3390/jcm14134595
Chicago/Turabian StyleMitincu-Caramfil, Simona-Dana, Alina Plesea-Condratovici, Alexia Anastasia Stefania Balta, Valentin Bulza, Andrei-Vlad Bradeanu, Lavinia-Alexandra Moroianu, Oana-Maria Isailă, and Eduard Drima. 2025. "The Impact of Chronic Alcohol Consumption on Cognitive Function in Older People" Journal of Clinical Medicine 14, no. 13: 4595. https://doi.org/10.3390/jcm14134595
APA StyleMitincu-Caramfil, S.-D., Plesea-Condratovici, A., Balta, A. A. S., Bulza, V., Bradeanu, A.-V., Moroianu, L.-A., Isailă, O.-M., & Drima, E. (2025). The Impact of Chronic Alcohol Consumption on Cognitive Function in Older People. Journal of Clinical Medicine, 14(13), 4595. https://doi.org/10.3390/jcm14134595