
Robotic-Guided Spine Surgery: Implementation of a System in Routine Clinical Practice—An Update




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
- Preoperative imaging and screw planning. In addition to magnetic resonance imaging (MRI) of the spinal region to be examined and instrumented, all patients received preoperative three-dimensional (3D) CT imaging of the part of the spine that was to be stabilized. The MRI and CT data were exported to the BrainLab navigation software (https://www.brainlab.com/surgery-products/overview-spinal-trauma-products/spinal-navigation/, accessed date 20 June 2025) and fused either rigidly or elastically. The navigation software includes a screw planning application that was used to plan the radius, length, and trajectory of the PS prior to surgery. The software enables automatic identification of the vertebra, followed by automatic screw planning for PSs in the selected vertebra. The proposed preplanned screws were then manually corrected according to the surgeon’s preference. For this step, it was crucial to have an artifact-free, high-resolution 3D CT of the spine, i.e., the area intended for instrumentation. (Figure 1 and Figure 2) [4].
- 2.
- The patient is placed in a prone position on a positioning cushion, with additional pressure protection to the knees and elbows, on a carbon fiber surgical table (Figure 3), connected to the AIRO® iCT scanner (Brainlab, Munich, Germany). All anesthesia cables and lines are routed through the gantry. For surgery of the upper and middle thoracic spine, the arms are positioned at the sides of the body; for surgery on the lower thoracic and lumbar spine, the arms are stretched above the head and padded with gel foam paddies and cushions. In all cases, the Cirq® arm is attached to a metal bracket on the left side of the patient. Installation is performed before the patient is covered with sterile drapes [4].
- 3.
- The spinal levels intended for instrumentation were determined using fluoroscopy to plan the skin incision. Fluoroscopy was not necessary in previous operations in the same area. Adhesive fiducials (usually four) were applied to the left and right from the planned or existing skin incision to check the accuracy of registration. After this step, the surgical area was prepared and covered, and the Cirq® arm was covered [4].
- 4.
- In open surgery cases, the bony structures, laminae, and pedicles were exposed along the area intended for instrumentation. For stabilization of the middle and lower thoracic, lumbar, and sacral spine, a spinous process proximal to the upper vertebra of the planned spinal construct was usually selected for fixation of the carbon reference array. For stabilization of the upper thoracic spine, the reference array was usually placed on the spinous process of the vertebra adjacent to the lowest level of the planned construct. In minimally invasive spine surgery (MISS) involving PS implantation, the reference array was usually attached to the spinous process of the vertebra via a separate small skin incision in the midline with subperiosteal dissection of the muscles of the tip of the spinous process. (Figure 4). It is crucial to position the reference array close enough to the region intended for instrumentation, but also far enough away from the projection of the entry point and screw trajectories of the adjacent instrumented vertebrae to avoid collision of the kinematic unit of the robot arm with the reference array. The skin incision for the percutaneous procedures either a midline incision with exposure of the fascia without opening or multiple skin incisions at the entry points of the screws [4].
- 5.
- After exposing the bone anatomy and fixing the reference array, a registration scan with automatic registration of the patient was performed. The surgical area is covered with a sterile drape so that the reference array is visible to the navigation camera, and the scan length is marked with a sterile pen. The registration scan is performed during apnea so that any respiratory artifacts that may occur do not affect accuracy. The scan takes 7–12 s. All personnel leave the operative room for the scan, so that the radiation exposure for staff is zero. Low-dose protocols were used for the scans. The effective dose is calculated by multiplying the total dose length product (DLP) by ED/DLP conversion factors (17.8 μSv/Gy × cm for thoracic and 19.8 μSv/Gy × cm for lumbar spine scans). After the scan, the image data was automatically transferred to the navigation system (BrainLab, Munich, Germany) without user interaction for automatic patient registration. The entire process of covering the patient with a sterile drape for the scan, as well as the scan itself, takes 10–15 min. The registration accuracy was checked and recorded using a pointer and skin fiducials and by placing the pointer in the fixation area of the registration array. In open cases, additional verification of the bony structures was performed. (Figure 5 and Figure 6).
- 6.
- After selecting a region of interest (ROI), the iCT scan was merged with a preoperative scan. A rigid fusion was performed, and in cases of instability of the spine due to a tumor or fracture, as well as in cases of longer constructs, elastic fusion was performed (Figure 7 and Figure 8). In selected cases with longer thoracolumbosacral constructs, two scans were performed, with repositioning of the reference array to avoid compromising accuracy for levels far from the reference array. After fusion of the scans, the planned screw trajectories were checked and corrected as necessary (Figure 9) [4].
- 7.
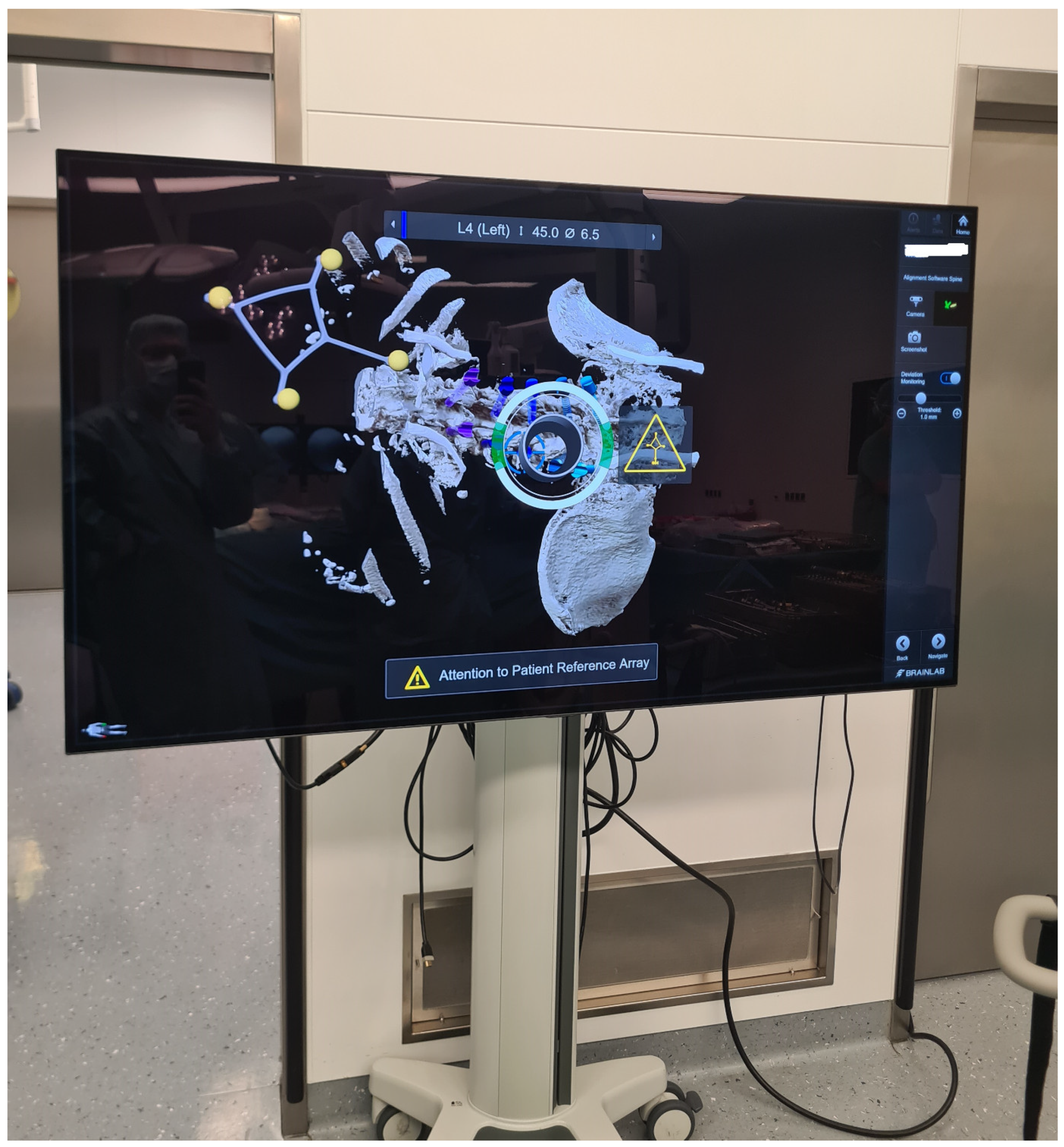
- The kinematic unit of the Cirq® Robotic Alignment Module with the previously calibrated tracking array is positioned over the projection of the screw entry point. The instruments are tracked in real time, and their position is constantly reported back so that the surgeon can observe the movements of the robotic arm and all instruments on a separate monitor. The surgeon is located on the side of the robotic arm, i.e., on the left side of the patient. After positioning the robotic arm over the projection of the trajectory entry point, the robotic arm automatically aligns itself according to preplanned trajectory of the relevant screw. In percutaneous cases, a previously calibrated and registered trocar can be used to open the soft tissue for screw implantation, followed by the attachment of an instrument holder for the drill guide. A drill guide is then inserted through the tracking array with the instrument holder and positioned at the entry point, and attachable snap-on depth control for drilling is then attached. The tracking array is then locked, and drilling begins. In this step, it is crucial that the surgeon additionally stabilizes the instrument holder with sufficient pressure on the entry point to prevent skiving. A K-wire is implanted, and the robotic arm is removed. This workflow is repeated for all trajectories. All K-wires are secured to the cover with clamps to keep them in place. (Figure 10, Figure 11, Figure 12, Figure 13 and Figure 14) [4].
- 8.
- The screws were inserted using a fluoroscopic (first 12 operations) or navigated technique (subsequent surgeries) technique. During screw implantation, micromovements in the surgical field due to screw implantation can impair navigation accuracy, so screws were first implanted where misplacement could cause the most damage (e.g., thoracic screws vs. lumbar screws or thin pedicles vs. thick pedicles). In all cases, particular care must be taken to avoid collisions and disturbances of the reference array (Figure 15 and Figure 16) [4].
- 9.
- After placing the PSs, the surgical site was covered so that the reference array was visible for the navigation camera, and an iCT scan was performed to check the screw position (Figure 17). For longer constructs and spinal instability, the reference array for the second scan was repositioned so that the new scan could serve as both a control iCT scan for implanted screws and a registration scan for screws to be implanted. The second iCT scan is fused with the first registration scan to check the accuracy of screw placements and verify the deviation of the actual screws from the planned trajectories [4]. If the screws are misplaced, the misaligned screws can be segmented into the software to improve visualization after removal and implantation of new screws using the navigated technique. Repeated iCT scans show the visualization of the position of misplaced, repositioned, and corrected screws (Figure 18).
- 10.
- In cases where additional surgical steps were necessary, such as decompression of the spinal canal, tumor resection, or implantation of a cage, the reference array was removed and the operation continued. After the completion of these surgical steps, the rods were implanted, and the wound was closed in layers.
3. Results
3.1. General Characteristics of the Patients
3.2. Mortality
3.3. Invasiveness of Surgery
3.4. Operative Time, Robotic Time and Time-per-K-Wire
3.5. PS Accuracy
3.6. Robot Abandonment
3.7. Complications
3.8. Learning Curve
3.9. Radiation Exposure
3.10. Illustrative Cases
3.10.1. Case 1
3.10.2. Case 2
3.10.3. Case 3
3.10.4. Screw Revision Case
3.10.5. Robot Abandonment Case
4. Discussion
4.1. Learning Curve in RG Spine Surgery
4.2. Studies Applying the Cirq® Robotic Arm
4.3. Pedicle Screw Accuracy Placement and Robotic Time
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RG | robotic guided |
| PS | pedicle screw |
| iCT | intraoperative computer tomography |
| GRS | Gertzbein Robbins system |
| FDA | Food and Drug Administration |
| OR | operative room |
| 3D | three-dimensional |
| MRI | magnetic resonance imaging |
| K-wire | Kirschner wire |
| DXA | dual-energy x-ray absorptiometry |
| HU | Hounsfield unit |
| ED | effective dose |
References
- D’Souza, M.; Gendreau, J.; Feng, A.; Kim, L.H.; Ho, A.L.; Veeravagu, A. Robotic-Assisted Spine Surgery: History, Efficacy, Cost, And Future Trends. Robot. Surg. 2019, 6, 9–23. [Google Scholar]
- Ong, V.; Swan, A.R.; Sheppard, J.P.; Ng, E.; Faung, B.; Diaz-Aguilar, L.D.; Pham, M.H. A Comparison of Spinal Robotic Systems and Pedicle Screw Accuracy Rates: Review of Literature and Meta-Analysis. Asian J. Neurosurg. 2022, 17, 547–556. [Google Scholar] [CrossRef]
- Shafi, K.A.; Pompeu, Y.A.; Vaishnav, A.S.; Mai, E.; Sivaganesan, A.; Shahi, P.; Qureshi, S.A. Does robot-assisted navigation influence pedicle screw selection and accuracy in minimally invasive spine surgery? Neurosurg. Focus 2022, 52, E4. [Google Scholar] [CrossRef]
- Pojskić, M.; Bopp, M.; Nimsky, C.; Carl, B.; Saβ, B. Initial Intraoperative Experience with Robotic-Assisted Pedicle Screw Placement with Cirq. J. Clin. Med. 2021, 10, 5725. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Pooler, B.D.; Lauder, T.; del Rio, A.M.; Bruce, R.J.; Binkley, N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann. Intern. Med. 2013, 158, 588–595. [Google Scholar] [CrossRef]
- Desai, M.J.; Kapural, L.; Petersohn, J.D.; Vallejo, R.; Menzies, R.; Creamer, M.; Gofeld, M. A Prospective, Randomized, Multicenter, Open-label Clinical Trial Comparing Intradiscal Biacuplasty to Conventional Medical Management for Discogenic Lumbar Back Pain. Spine 2016, 41, 1065–1074. [Google Scholar] [CrossRef]
- Gabrovsky, N.; Ilkov, P.; Laleva, M. Cirq® robotic assistance for thoracolumbar pedicle screw placement-feasibility, accuracy, and safety. Brain Spine 2023, 3, 101717. [Google Scholar] [CrossRef]
- Siddiqui, M.I.; Wallace, D.J.; Salazar, L.M.; Vardiman, A.B. Robot-Assisted Pedicle Screw Placement: Learning Curve Experience. World Neurosurg. 2019, 130, e417–e422. [Google Scholar] [CrossRef]
- Avrumova, F.; Morse, K.W.; Heath, M.; Widmann, R.F.; Lebl, D.R. Evaluation of K-wireless robotic and navigation assisted pedicle screw placement in adult degenerative spinal surgery: Learning curve and technical notes. J. Spine Surg. 2021, 7, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Srinivasa, V.; Thirugnanam, B.; Pai Kanhangad, M.; Soni, A.; Kashyap, A.; Vidyadhara, A.; Rao, S.K. Flattening the learning curve-Early experience of robotic-assisted pedicle screw placement in spine surgery. J. Orthop. 2024, 57, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Feng, F.; Chen, X.; Liu, Z.; Han, Y.; Chen, H.; Li, Q.; Lao, L.; Shen, H. Learning curve of junior surgeons in robot-assisted pedicle screw placement: A comparative cohort study. Eur. Spine J. 2024, 33, 314–323. [Google Scholar] [CrossRef]
- Perdomo-Pantoja, A.; Ishida, W.; Zygourakis, C.; Holmes, C.; Iyer, R.R.; Cottrill, E.; Theodore, N.; Witham, T.F.; Lo, S.F.L. Accuracy of Current Techniques for Placement of Pedicle Screws in the Spine: A Comprehensive Systematic Review and Meta-Analysis of 51,161 Screws. World Neurosurg. 2019, 126, 664–678.e3. [Google Scholar] [CrossRef] [PubMed]
- Urakov, T.M.; Chang, K.H.; Burks, S.S.; Wang, M.Y. Initial academic experience and learning curve with robotic spine instrumentation. Neurosurg. Focus 2017, 42, E4. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Meyers, J.E.; Siasios, I.; Pollina, J. Next-Generation Robotic Spine Surgery: First Report on Feasibility, Safety, and Learning Curve. Oper. Neurosurg. 2019, 17, 61–69. [Google Scholar] [CrossRef]
- Vardiman, A.B.; Wallace, D.J.; Booher, G.A.; Crawford, N.R.; Riggleman, J.R.; Greeley, S.L.; Ledonio, C.G. Does the accuracy of pedicle screw placement differ between the attending surgeon and resident in navigated robotic-assisted minimally invasive spine surgery? J. Robot. Surg. 2020, 14, 567–572. [Google Scholar] [CrossRef]
- Ueno, J.; Torii, Y.; Umehra, T.; Iinuma, M.; Yoshida, A.; Tomochika, K.; Niki, H.; Akazawa, T. Robotics is useful for less-experienced surgeons in spinal deformity surgery. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 1805–1810. [Google Scholar] [CrossRef]
- Torii, Y.; Ueno, J.; Iinuma, M.; Yoshida, A.; Niki, H.; Akazawa, T. Accuracy of robotic-assisted pedicle screw placement comparing junior surgeons with expert surgeons: Can junior surgeons place pedicle screws as accurately as expert surgeons? J. Orthop. Sci. 2023, 28, 961–965. [Google Scholar] [CrossRef]
- Epstein, N.E. Perspective on robotic spine surgery: Who’s doing the thinking? Surg. Neurol. Int. 2021, 12, 520. [Google Scholar] [CrossRef]
- Kam, J.K.T.; Gan, C.; Dimou, S.; Awad, M.; Kavar, B.; Nair, G.; Morokoff, A. Learning Curve for Robot-Assisted Percutaneous Pedicle Screw Placement in Thoracolumbar Surgery. Asian Spine J. 2019, 13, 920–927. [Google Scholar] [CrossRef]
- Fayed, I.; Tai, A.; Triano, M.; Sayah, A.; Makariou, E.; Voyadzis, J.M.; Sandhu, F.A. Robot-Assisted Percutaneous Pedicle Screw Placement: Evaluation of Accuracy of the First 100 Screws and Comparison with Cohort of Fluoroscopy-guided Screws. World Neurosurg. 2020, 143, e492–e502. [Google Scholar] [CrossRef]
- McCormick, B.; Asdourian, P.L.; Johnson, D.C.; Moatz, B.W.; Duvall, G.T.; Soda, M.T.; Beaufort, A.R.; Chotikul, L.G.; McAfee, P.C. 100 Complex posterior spinal fusion cases performed with robotic instrumentation. J. Robot Surg. 2023, 17, 2749–2756. [Google Scholar] [CrossRef] [PubMed]
- Jiang, K.; Hersh, A.M.; Bhimreddy, M.; Weber-Levine, C.; Davidar, A.D.; Menta, A.K.; Routkevitch, D.; Alomari, S.; Judy, B.F.; Lubelski, D.; et al. Learning Curves for Robot-Assisted Pedicle Screw Placement: Analysis of Operative Time for 234 Cases. Oper. Neurosurg. 2023, 25, 482–488. [Google Scholar] [CrossRef]
- Hsu, B.H.; Liu, H.W.; Lee, K.L.; Lin, M.C.; Chen, G.; Yu, J.; Chen, C.-L.; Su, I.-C.S.; Lin, C.-M. Learning Curve of ROSA ONE Spine System for Transpedicular Screw Placement. Neurospine 2022, 19, 367–375. [Google Scholar] [CrossRef]
- MacLean, L.; Hersh, A.M.; Bhimreddy, M.; Jiang, K.; Davidar, A.D.; Weber-Levine, C.; Alomari, S.; Judy, B.F.; Lubelski, D.; Theodore, N. Comparison of accuracy, revision, and perioperative outcomes in robot-assisted spine surgeries: Systematic review and meta-analysis. J. Neurosurg. Spine 2024, 42, 519–531. [Google Scholar] [CrossRef]
- Gabrovsky, N.; Ilkov, P.; Laleva, M. Cirq Robotic Assistance for Thoracolumbar Pedicle Screw Placement: Overcoming the Disadvantages of Minimally Invasive Spine Surgery. Acta Neurochir. Suppl. 2023, 135, 389–392. [Google Scholar]
- Desai, S.K.; Adams, J.P. Initial single surgeon evaluation comparing C-arm fluoroscopy with the Cirq robotic assistance device for instrumentation of the thoracolumbar spine. BMC Surg. 2022, 22, 434. [Google Scholar] [CrossRef]
- Ringel, F.; Stüer, C.; Reinke, A.; Preuss, A.; Behr, M.; Auer, F.; Stoffel, M.; Meyer, B. Accuracy of robot-assisted placement of lumbar and sacral pedicle screws: A prospective randomized comparison to conventional freehand screw implantation. Spine 2012, 37, E496–E501. [Google Scholar] [CrossRef] [PubMed]
- Asada, T.; Simon, C.Z.; Lu, A.Z.; Adida, S.; Dupont, M.; Parel, P.M.; Zhang, J.; Bhargava, S.; Morse, K.W.; Dowdell, J.E.; et al. Robot-navigated pedicle screw insertion can reduce intraoperative blood loss and length of hospital stay: Analysis of 1633 patients utilizing propensity score matching. Spine J. 2024, 24, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Tian, W.; Sun, Y.; Liu, Y.; Wei, Y. Effect of Robot-Assisted Surgery on Lumbar Pedicle Screw Internal Fixation in Patients with Osteoporosis. World Neurosurg. 2019, 125, e1057–e1062. [Google Scholar] [CrossRef]
- Jiang, B.; Pennington, Z.; Azad, T.; Liu, A.; Ahmed, A.K.; Zygourakis, C.C.; Westbroek, E.M.; Zhu, A.; Cottrill, E.; Theodore, N. Robot-Assisted versus Freehand Instrumentation in Short-Segment Lumbar Fusion: Experience with Real-Time Image-Guided Spinal Robot. World Neurosurg. 2020, 136, e635–e645. [Google Scholar] [CrossRef]
- Gautschi, O.P.; Schatlo, B.; Schaller, K.; Tessitore, E. Clinically relevant complications related to pedicle screw placement in thoracolumbar surgery and their management: A literature review of 35,630 pedicle screws. Neurosurg. Focus 2011, 31, E8. [Google Scholar] [CrossRef]
- Perna, A.; Velluto, C.; Smakaj, A.; Tamburrelli, F.; Borruto, M.I.; Santagada, D.A.; Gorgoglione, F.L.; Liuzza, F.; Proietti, L. Positioning accuracy and facet joints violation after percutaneous pedicle screws placement with robot-assisted versus fluoroscopy-guided technique: Systematic review and meta-analysis. J. Neurosci. Rural Pract. 2023, 14, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.; Smith, A.D.; Shaffer, A.; Krist, D.T.; Moawad, C.M.; MacInnis, B.R.; Teal, K.; Hassaneen, W.; Arnold, P.M. Evaluating robotic pedicle screw placement against conventional modalities: A systematic review and network meta-analysis. Neurosurg. Focus 2022, 52, E10. [Google Scholar] [CrossRef] [PubMed]
- Riewruja, K.; Tanasansomboon, T.; Yingsakmongkol, W.; Kotheeranurak, V.; Limthongkul, W.; Chokesuwattanaskul, R.; Kerr, S.J.; Singhatanadgige, W. A Network Meta-Analysis Comparing the Efficacy and Safety of Pedicle Screw Placement Techniques Using Intraoperative Conventional, Navigation, Robot-Assisted, and Augmented Reality Guiding Systems. Int. J. Spine Surg. 2024, 18, 551–570. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Li, H.; Su, J.; Wang, Z.; Li, D.; Tian, Y.; Yuan, S.; Wang, L.; Liu, X. Comparison of the Accuracy of Pedicle Screw Placement Using a Fluoroscopy-Assisted Free-Hand Technique with Robotic-Assisted Navigation Using an O-Arm or 3D C-Arm in Scoliosis Surgery. Glob. Spine J. 2024, 14, 1337–1346. [Google Scholar] [CrossRef]
- Guan, J.; Feng, N.; Yu, X.; Yang, K. Comparison of robot-assisted versus fluoroscopy-guided transforaminal lumbar interbody fusion (TLIF) for lumbar degenerative diseases: A systematic review and meta-analysis of randomized controlled trails and cohort studies. Syst. Rev. 2024, 13, 170. [Google Scholar] [CrossRef]
- Hyun, S.J.; Kim, K.J.; Jahng, T.A.; Kim, H.J. Minimally Invasive Robotic Versus Open Fluoroscopic-guided Spinal Instrumented Fusions: A Randomized Controlled Trial. Spine 2017, 42, 353–358. [Google Scholar] [CrossRef]
- Cammarata, G.; Scalia, G.; Costanzo, R.; Umana, G.E.; Furnari, M.; Ponzo, G.; Giuffrida, M.; Maugeri, R.; Iacopino, D.G.; Nicoletti, G.F.; et al. Fluoroscopy-Assisted Freehand Versus 3D-Navigated Imaging-Assisted Pedicle Screw Insertion: A Multicenter Study. Acta Neurochir. Suppl. 2023, 135, 425–430. [Google Scholar]
- Nagata, K.; Glassman, S.D.; Brown, M.E.; Daniels, C.L.; Schmidt, G.O.; Carreon, L.Y.; Hines, B.; Gum, J.L. Risk Factors of Screw Malposition in Robot-Assisted Cortical Bone Trajectory: Analysis of 1344 Consecutive Screws in 256 Patients. Spine 2024, 49, 780–787. [Google Scholar] [CrossRef]
- Zhang, Q.; Fan, M.X.; Han, X.G.; Liu, Y.J.; He, D.; Liu, B.; Tian, W. Risk Factors of Unsatisfactory Robot-Assisted Pedicle Screw Placement: A Case-Control Study. Neurospine 2021, 18, 839–844. [Google Scholar] [CrossRef]
- Gautam, D.; Vivekanandan, S.; Mazur, M.D. Robotic Spine Surgery: Systematic Review of Common Error Types and Best Practices. Oper. Neurosurg. 2024, 28, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Ha, B.J.; Lee, J.M.; Yoon, S.J.; Kim, B.K.; Lee, J.; Lee, S.; Ryu, S.; Cha, Y.; Hwang, S.; Woo, D.; et al. Three-Dimensional Quantitative Assessment of Pedicle Screw Accuracy in Clinical Utilization of a New Robotic System in Spine Surgery: A Multicenter Study. Neurospine 2023, 20, 1028–1039. [Google Scholar] [CrossRef]
- Al-Naseem, A.O.; Al-Muhannadi, A.; Ramadhan, M.; Alfadhli, A.; Marwan, Y.; Shafafy, R.; Abd-El-Barr, M.M. Robot-assisted pedicle screw insertion versus navigation-based and freehand techniques for posterior spinal fusion in scoliosis: A systematic review and meta-analysis. Spine Deform. 2024, 12, 1203–1215. [Google Scholar] [CrossRef] [PubMed]
- Altorfer, F.C.S.; Kelly, M.J.; Avrumova, F.; Burkhard, M.D.; Zhu, J.; Abel, F.; Cammisa, F.P.; Sama, A.; Farshad, M.; Lebl, D.R. Pedicle Screw Placement with Augmented Reality Versus Robotic-Assisted Surgery. Spine 2024. ahead of print. [Google Scholar] [CrossRef]
- Toossi, N.; Vardiman, A.B.; Benech, C.A.; Kanaly, C.W.; Maltenfort, M.G.; Backes, D.M.; Bucklen, B. Factors Affecting the Accuracy of Pedicle Screw Placement in Robot-Assisted Surgery: A Multicenter Study. Spine 2022, 47, 1613–1619. [Google Scholar] [CrossRef]
- Asada, T.; Subramanian, T.; Simon, C.Z.; Singh, N.; Hirase, T.; Araghi, K.; Lu, A.Z.; Mai, E.; Kim, Y.E.; Tuma, O.; et al. Level-specific comparison of 3D navigated and robotic arm-guided screw placement: An accuracy assessment of 1210 pedicle screws in lumbar surgery. Spine J. 2024, 24, 1872–1880. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Fang, Y.; Zhang, Q.; Zhao, J.; Liu, B.; Tian, W. A prospective cohort study of the accuracy and safety of robot-assisted minimally invasive spinal surgery. BMC Surg. 2022, 22, 47. [Google Scholar] [CrossRef]
- Lee, N.J.; Buchanan, I.A.; Zuckermann, S.L.; Boddapati, V.; Mathew, J.; Geiselmann, M.; Park, P.J.; Leung, E.; Buchholz, A.L.; Khan, A.; et al. What Is the Comparison in Robot Time per Screw, Radiation Exposure, Robot Abandonment, Screw Accuracy, and Clinical Outcomes Between Percutaneous and Open Robot-Assisted Short Lumbar Fusion?: A Multicenter, Propensity-Matched Analysis of 310 Patients. Spine 2022, 47, 42–48. [Google Scholar] [CrossRef]
- Pechlivanis, I.; Kiriyanthan, G.; Engelhardt, M.; Scholz, M.; Lücke, S.; Harders, A.; Schmieder, K. Percutaneous placement of pedicle screws in the lumbar spine using a bone mounted miniature robotic system: First experiences and accuracy of screw placement. Spine 2009, 34, 392–398. [Google Scholar] [CrossRef]
- Bonello, J.P.; Koucheki, R.; Abbas, A.; Lex, J.; Nucci, N.; Yee, A.; Ahn, H.; Finkelstein, J.; Lewis, S.; Larouche, J.; et al. Comparison of major spine navigation platforms based on key performance metrics: A meta-analysis of 16,040 screws. Eur. Spine J. 2023, 32, 2937–2948. [Google Scholar] [CrossRef]
- Caelers, I.J.M.H.; Berendsen, R.C.M.; Droeghaag, R.; Pecasse, N.J.J.; Rijkers, K.; Van Hemert, W.L.W.; De Bie, R.; Van Santbrink, H. Comparing radiation dose of image-guided techniques in lumbar fusion surgery with pedicle screw insertion; A systematic review. N. Am. Spine Soc. J. 2023, 13, 100199. [Google Scholar] [CrossRef]
- Pennington, Z.; Cottrill, E.; Westbroek, E.M.; Goodwin, M.L.; Lubelski, D.; Ahmed, A.K.; Sciubba, D.M. Evaluation of surgeon and patient radiation exposure by imaging technology in patients undergoing thoracolumbar fusion: Systematic review of the literature. Spine J. 2019, 19, 1397–1411. [Google Scholar] [CrossRef] [PubMed]

























Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pojskić, M.; Bopp, M.; Alwakaa, O.; Nimsky, C.; Saß, B. Robotic-Guided Spine Surgery: Implementation of a System in Routine Clinical Practice—An Update. J. Clin. Med. 2025, 14, 4463. https://doi.org/10.3390/jcm14134463
Pojskić M, Bopp M, Alwakaa O, Nimsky C, Saß B. Robotic-Guided Spine Surgery: Implementation of a System in Routine Clinical Practice—An Update. Journal of Clinical Medicine. 2025; 14(13):4463. https://doi.org/10.3390/jcm14134463
Chicago/Turabian StylePojskić, Mirza, Miriam Bopp, Omar Alwakaa, Christopher Nimsky, and Benjamin Saß. 2025. "Robotic-Guided Spine Surgery: Implementation of a System in Routine Clinical Practice—An Update" Journal of Clinical Medicine 14, no. 13: 4463. https://doi.org/10.3390/jcm14134463
APA StylePojskić, M., Bopp, M., Alwakaa, O., Nimsky, C., & Saß, B. (2025). Robotic-Guided Spine Surgery: Implementation of a System in Routine Clinical Practice—An Update. Journal of Clinical Medicine, 14(13), 4463. https://doi.org/10.3390/jcm14134463