
Personalized Treatment Modalities for Rectal Cancer: Advances in Neoadjuvant Treatment
 ,
,
Abstract
1. Introduction
2. Key Considerations in Personalized Treatment Modalities in LARC
2.1. Tumor Characteristics
2.1.1. Tumor Staging (Clinical T and N Stage)
2.1.2. Tumor Location
2.1.3. Extramural Vascular Invasion
2.2. Molecular Characteristics
2.3. Patient-Related Factors
2.3.1. Patient Symptoms
2.3.2. Age, Comorbidities, and Functional Status
2.3.3. Patient Preferences
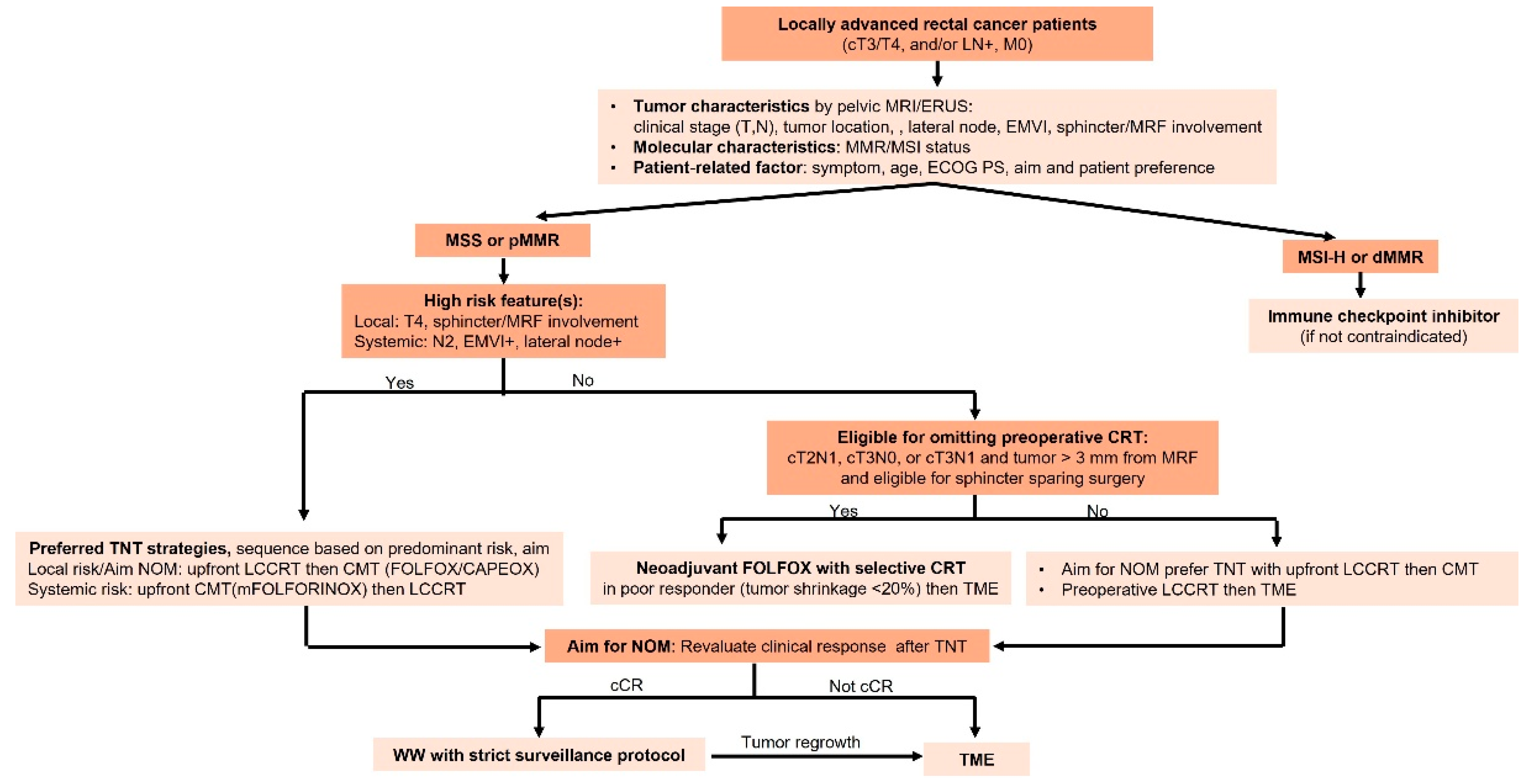
2.4. Risk-Adapted Treatment Strategies
2.4.1. Treatment Intensification
2.4.2. Treatment De-Escalation
2.4.3. Omitting Preoperative Radiation
2.4.4. Non-Operative Management (NOM)/Watch and Wait (WW)
- Flexible sigmoidoscopy and digital rectal examination (DRE) conducted every four months during the initial two years, followed by assessments every six months for the subsequent three years.
- Pelvic MRI performed every six months for the initial two years, transitioning to annual imaging thereafter.
2.5. Multidisciplinary Team Involvement
3. Emerging Trends and Future Directions
3.1. Intensified Chemotherapy to Avoid Radiation and Enhance NOM in LARC
- (1)
- Can good responders after preoperative FOLFIRINOX safely omit preoperative CRT, such as in the PROSPECT trial explored in patients receiving FOLFOX?
- (2)
- Will a consolidation triplet regimen with FOLFORINOX achieve higher cCR rates and improve organ preservation than a doublet regimen followed by CRT in a TNT strategy?
3.2. Role of Circulating Tumor DNA in Personalizing Non-Operative Strategies
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Cancer Facts & Figures 2025. Atlanta: American Society. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2025/2025-cancer-facts-and-figures-acs.pdf (accessed on 27 January 2025).
- Shulman, R.M.; Deng, M.; Handorf, E.A.; Meyer, J.E.; Lynch, S.M.; Arora, S. Factors Associated with Racial and Ethnic Disparities in Locally Advanced Rectal Cancer Outcomes. JAMA Netw Open 2024, 7, e240044. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Wagle, N.S.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 233–254. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- AlZaabi, A.; AlHarrasi, A.; AlMusalami, A.; AlMahyijari, N.; Al Hinai, K.; Aladawi, H.; Al-Shamsi, H.O. Early onset colorectal cancer: Challenges across the cancer care continuum. Ann. Med. Surg. 2022, 82, 104453. [Google Scholar] [CrossRef]
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; van Krieken, J.H.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef]
- Sebag-Montefiore, D.; Stephens, R.J.; Steele, R.; Monson, J.; Grieve, R.; Khanna, S.; Quirke, P.; Couture, J.; de Metz, C.; Myint, A.S.; et al. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): A multicentre, randomised trial. Lancet 2009, 373, 811–820. [Google Scholar] [CrossRef]
- Gérard, J.P.; Conroy, T.; Bonnetain, F.; Bouché, O.; Chapet, O.; Closon-Dejardin, M.T.; Untereiner, M.; Leduc, B.; Francois, E.; Maurel, J.; et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: Results of FFCD 9203. J. Clin. Oncol. 2006, 24, 4620–4625. [Google Scholar] [CrossRef]
- Bosset, J.F.; Collette, L.; Calais, G.; Mineur, L.; Maingon, P.; Radosevic-Jelic, L.; Daban, A.; Bardet, E.; Beny, A.; Ollier, J.C. Chemotherapy with preoperative radiotherapy in rectal cancer. N. Engl. J. Med. 2006, 355, 1114–1123. [Google Scholar] [CrossRef]
- Breugom, A.J.; Swets, M.; Bosset, J.F.; Collette, L.; Sainato, A.; Cionini, L.; Glynne-Jones, R.; Counsell, N.; Bastiaannet, E.; van den Broek, C.B.; et al. Adjuvant chemotherapy after preoperative (chemo)radiotherapy and surgery for patients with rectal cancer: A systematic review and meta-analysis of individual patient data. Lancet Oncol. 2015, 16, 200–207. [Google Scholar] [CrossRef]
- Fokas, E.; Schlenska-Lange, A.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.L.; et al. Chemoradiotherapy Plus Induction or Consolidation Chemotherapy as Total Neoadjuvant Therapy for Patients with Locally Advanced Rectal Cancer: Long-term Results of the CAO/ARO/AIO-12 Randomized Clinical Trial. JAMA Oncol. 2022, 8, e215445. [Google Scholar] [CrossRef]
- Conroy, T.; Bosset, J.F.; Etienne, P.L.; Rio, E.; François, É.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Ciseł, B.; Pietrzak, L.; Michalski, W.; Wyrwicz, L.; Rutkowski, A.; Kosakowska, E.; Cencelewicz, A.; Spałek, M.; Polkowski, W.; Jankiewicz, M.; et al. Long-course preoperative chemoradiation versus 5 × 5 Gy and consolidation chemotherapy for clinical T4 and fixed clinical T3 rectal cancer: Long-term results of the randomized Polish II study. Ann. Oncol. 2019, 30, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Tang, Y.; Hu, C.; Jiang, L.M.; Jiang, J.; Li, N.; Liu, W.Y.; Chen, S.L.; Li, S.; Lu, N.N.; et al. Multicenter, Randomized, Phase III Trial of Short-Term Radiotherapy Plus Chemotherapy Versus Long-Term Chemoradiotherapy in Locally Advanced Rectal Cancer (STELLAR). J. Clin. Oncol. 2022, 40, 1681–1692. [Google Scholar] [CrossRef]
- Garcia-Aguilar, J.; Patil, S.; Gollub, M.J.; Kim, J.K.; Yuval, J.B.; Thompson, H.M.; Verheij, F.S.; Omer, D.M.; Lee, M.; Dunne, R.F.; et al. Organ Preservation in Patients with Rectal Adenocarcinoma Treated with Total Neoadjuvant Therapy. J. Clin. Oncol. 2022, 40, 2546–2556. [Google Scholar] [CrossRef]
- Kang, S.B.; Cho, J.R.; Jeong, S.Y.; Oh, J.H.; Ahn, S.; Choi, S.; Kim, D.W.; Lee, B.H.; Youk, E.G.; Park, S.C.; et al. Quality of life after sphincter preservation surgery or abdominoperineal resection for low rectal cancer (ASPIRE): A long-term prospective, multicentre, cohort study. Lancet Reg. Health West. Pac. 2021, 6, 100087. [Google Scholar] [CrossRef]
- Peeters, K.C.; van de Velde, C.J.; Leer, J.W.; Martijn, H.; Junggeburt, J.M.; Kranenbarg, E.K.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Marijnen, C.A. Late side effects of short-course preoperative radiotherapy combined with total mesorectal excision for rectal cancer: Increased bowel dysfunction in irradiated patients--a Dutch colorectal cancer group study. J. Clin. Oncol. 2005, 23, 6199–6206. [Google Scholar] [CrossRef]
- Balyasnikova, S.; Brown, G. Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management. Curr. Treat. Options Oncol. 2016, 17, 32. [Google Scholar] [CrossRef]
- Klessen, C.; Rogalla, P.; Taupitz, M. Local staging of rectal cancer: The current role of MRI. Eur. Radiol. 2007, 17, 379–389. [Google Scholar] [CrossRef]
- Bipat, S.; Glas, A.S.; Slors, F.J.; Zwinderman, A.H.; Bossuyt, P.M.; Stoker, J. Rectal cancer: Local staging and assessment of lymph node involvement with endoluminal US, CT, and MR imaging--a meta-analysis. Radiology 2004, 232, 773–783. [Google Scholar] [CrossRef]
- Zhang, G.; Cai, Y.Z.; Xu, G.H. Diagnostic Accuracy of MRI for Assessment of T Category and Circumferential Resection Margin Involvement in Patients with Rectal Cancer: A Meta-Analysis. Dis. Colon Rectum 2016, 59, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Beets-Tan, R.G.; Beets, G.L. Rectal cancer: Review with emphasis on MR imaging. Radiology 2004, 232, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Lahaye, M.J.; Engelen, S.M.; Nelemans, P.J.; Beets, G.L.; van de Velde, C.J.; van Engelshoven, J.M.; Beets-Tan, R.G. Imaging for predicting the risk factors--the circumferential resection margin and nodal disease--of local recurrence in rectal cancer: A meta-analysis. Semin. Ultrasound CT MR 2005, 26, 259–268. [Google Scholar] [CrossRef]
- Xie, H.; Zhou, X.; Zhuo, Z.; Che, S.; Xie, L.; Fu, W. Effectiveness of MRI for the assessment of mesorectal fascia involvement in patients with rectal cancer: A systematic review and meta-analysis. Dig. Surg. 2014, 31, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Bartram, C.; Brown, G. Endorectal ultrasound and magnetic resonance imaging in rectal cancer staging. Gastroenterol. Clin. 2002, 31, 827–839. [Google Scholar] [CrossRef]
- Zwart, W.H.; Hotca, A.; Hospers, G.A.P.; Goodman, K.A.; Garcia-Aguilar, J. The Multimodal Management of Locally Advanced Rectal Cancer: Making Sense of the New Data. Am. Soc. Clin. Oncol. Educ. Book 2022, 42, 1–14. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Zhang, Y.-Z.; Song, M.; Geng, J.-H.; Zhu, X.-G.; Li, S.; Li, Y.-H.; Cai, Y.; Wang, W.-H. Patterns of failure and implications for clinical target volume definition of locally advanced T4b rectal cancer identified with magnetic resonance imaging and treated using neoadjuvant chemoradiotherapy and surgery. Radiother. Oncol. 2021, 161, 132–139. [Google Scholar] [CrossRef]
- Sluckin, T.C.; Couwenberg, A.M.; Lambregts, D.M.J.; Hazen, S.-M.J.A.; Horsthuis, K.; Meijnen, P.; Beets-Tan, R.G.H.; Tanis, P.J.; Marijnen, C.A.M.; Kusters, M. Lateral Lymph Nodes in Rectal Cancer: Do we all Think the Same? A Review of Multidisciplinary Obstacles and Treatment Recommendations. Clin. Color. Cancer 2022, 21, 80–88. [Google Scholar] [CrossRef]
- Ueno, H.; Mochizuki, H.; Hashiguchi, Y.; Hase, K. Prognostic determinants of patients with lateral nodal involvement by rectal cancer. Ann. Surg. 2001, 234, 190–197. [Google Scholar] [CrossRef]
- Khan, M.A.S.; Ang, C.W.; Hakeem, A.R.; Scott, N.; Saunders, R.N.; Botterill, I. The Impact of Tumour Distance From the Anal Verge on Clinical Management and Outcomes in Patients Having a Curative Resection for Rectal Cancer. J. Gastrointest. Surg. 2017, 21, 2056–2065. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Swets, M.; Breugom, A.J.; Gelderblom, H.; van de Velde, C.J.H. Should rectal cancer located 10-15 cm from the anal verge be defined as colon cancer. Ann. Oncol. 2017, 28, 664–665. [Google Scholar] [CrossRef]
- Miyakita, H.; Kamei, Y.; Chan, L.F.; Okada, K.; Kayano, H.; Yamamoto, S. Classification of rectal cancer according to recurrence types—Comparison of Japanese guidelines and Western guidelines. World J. Clin. Cases 2022, 10, 13284–13292. [Google Scholar] [CrossRef] [PubMed]
- Schrag, D.; Shi, Q.; Weiser, M.R.; Gollub, M.J.; Saltz, L.B.; Musher, B.L.; Goldberg, J.; Baghdadi, T.A.; Goodman, K.A.; McWilliams, R.R.; et al. Preoperative Treatment of Locally Advanced Rectal Cancer. N. Engl. J. Med. 2023, 389, 322–334. [Google Scholar] [CrossRef]
- Xynos, E.; Tekkis, P.; Gouvas, N.; Vini, L.; Chrysou, E.; Tzardi, M.; Vassiliou, V.; Boukovinas, I.; Agalianos, C.; Androulakis, N.; et al. Clinical practice guidelines for the surgical treatment of rectal cancer: A consensus statement of the Hellenic Society of Medical Oncologists (HeSMO). Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2016, 29, 103–126. [Google Scholar] [CrossRef]
- Varela, C.; Kim, N.K. Surgical Treatment of Low-Lying Rectal Cancer: Updates. Ann. Coloproctol. 2021, 37, 395–424. [Google Scholar] [CrossRef] [PubMed]
- Socha, J.; Kairevice, L.; Kępka, L.; Michalski, W.; Spałek, M.; Paciorek, K.; Bujko, K. Should Short-Course Neoadjuvant Radiation Therapy Be Applied for Low-Lying Rectal Cancer? A Systematic Review and Meta-Analysis of the Randomized Trials. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 1257–1264. [Google Scholar] [CrossRef]
- Adam, I.J.; Mohamdee, M.O.; Martin, I.G.; Scott, N.; Finan, P.J.; Johnston, D.; Dixon, M.F.; Quirke, P. Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet 1994, 344, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Quirke, P. What is the role for the circumferential margin in the modern treatment of rectal cancer? J. Clin. Oncol. 2008, 26, 303–312. [Google Scholar] [CrossRef]
- Emile, S.H.; Horesh, N.; Freund, M.R.; Parlade, A.; Nagarajan, A.; Garoufalia, Z.; Gefen, R.; Silva-Alvarenga, E.; Dasilva, G.; Wexner, S.D. Assessment of mesorectal fascia status in MRI compared with circumferential resection margin after total mesorectal excision and predictors of involved margins. Surgery 2022, 172, 1085–1092. [Google Scholar] [CrossRef]
- Guner, O.S.; Tumay, L.V. Persistent extramural vascular invasion positivity on magnetic resonance imaging after neoadjuvant chemoradiotherapy predicts poor outcome in rectal cancer. Asian J. Surg. 2021, 44, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.R.S.; Simillis, C.; Hunter, C.; Chand, M.; Bhoday, J.; Garant, A.; Vuong, T.; Artho, G.; Rasheed, S.; Tekkis, P.; et al. A meta-analysis comparing the risk of metastases in patients with rectal cancer and MRI-detected extramural vascular invasion (mrEMVI) vs mrEMVI-negative cases. Br. J. Cancer 2017, 116, 1513–1519. [Google Scholar] [CrossRef]
- Cercek, A.; Lumish, M.; Sinopoli, J.; Weiss, J.; Shia, J.; Lamendola-Essel, M.; Dika, I.H.E.; Segal, N.; Shcherba, M.; Sugarman, R.; et al. PD-1 Blockade in Mismatch Repair–Deficient, Locally Advanced Rectal Cancer. N. Engl. J. Med. 2022, 386, 2363–2376. [Google Scholar] [CrossRef] [PubMed]
- Ostwal, V.; Pande, N.S.; Engineer, R.; Saklani, A.; deSouza, A.; Ramadwar, M.; Sawant, S.; Mandavkar, S.; Shrirangwar, S.; Kataria, P.; et al. Low prevalence of deficient mismatch repair (dMMR) protein in locally advanced rectal cancers (LARC) and treatment outcomes. J. Gastrointest. Oncol. 2018, 10, 19–29. [Google Scholar] [CrossRef]
- Cercek, A.; Dos Santos Fernandes, G.; Roxburgh, C.S.; Ganesh, K.; Ng, S.; Sanchez-Vega, F.; Yaeger, R.; Segal, N.H.; Reidy-Lagunes, D.L.; Varghese, A.M.; et al. Mismatch Repair-Deficient Rectal Cancer and Resistance to Neoadjuvant Chemotherapy. Clin. Cancer Res. 2020, 26, 3271–3279. [Google Scholar] [CrossRef] [PubMed]
- Cercek, A.; Sinopoli, J.C.; Shia, J.; Weiss, J.A.; Temple, L.; Smith, J.J.; Saltz, L.B.; Widmar, M.; Fumo, G.; Aparo, S.; et al. Durable complete responses to PD-1 blockade alone in mismatch repair deficient locally advanced rectal cancer. J. Clin. Oncol. 2024, 42, LBA3512. [Google Scholar] [CrossRef]
- Guyot D’Asnières De Salins, A.; Tachon, G.; Cohen, R.; Karayan-Tapon, L.; Junca, A.; Frouin, E.; Godet, J.; Evrard, C.; Randrian, V.; Duval, A.; et al. Discordance between immunochemistry of mismatch repair proteins and molecular testing of microsatellite instability in colorectal cancer. ESMO Open 2021, 6, 100120. [Google Scholar] [CrossRef]
- Hechtman, J.F.; Rana, S.; Middha, S.; Stadler, Z.K.; Latham, A.; Benayed, R.; Soslow, R.; Ladanyi, M.; Yaeger, R.; Zehir, A.; et al. Retained mismatch repair protein expression occurs in approximately 6% of microsatellite instability-high cancers and is associated with missense mutations in mismatch repair genes. Mod. Pathol. 2020, 33, 871–879. [Google Scholar] [CrossRef]
- Yoo, R.N.; Cho, H.M.; Kye, B.H. Management of obstructive colon cancer: Current status, obstacles, and future directions. World J. Gastrointest. Oncol. 2021, 13, 1850–1862. [Google Scholar] [CrossRef]
- Guan, X.; Wei, R.; Yang, R.; Lu, Z.; Liu, E.; Zhao, Z.; Chen, H.; Yang, M.; Liu, Z.; Jiang, Z.; et al. Association of Radiotherapy for Rectal Cancer and Second Gynecological Malignant Neoplasms. JAMA Netw. Open 2021, 4, e2031661. [Google Scholar] [CrossRef]
- Dracham, C.B.; Shankar, A.; Madan, R. Radiation induced secondary malignancies: A review article. Radiat. Oncol. J. 2018, 36, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Penn, I. Second neoplasms following radiotherapy or chemotherapy for cancer. Am. J. Clin. Oncol. 1982, 5, 83–96. [Google Scholar] [CrossRef]
- Gaetani, R.S.; Ladin, K.; Abelson, J.S. Journey through the Decades: The Evolution in Treatment and Shared Decision Making for Locally Advanced Rectal Cancer. Cancers 2024, 16, 2807. [Google Scholar] [CrossRef]
- Karahan, S.N.; Gorgun, E. Modern rectal cancer management: A review of total neoadjuvant therapy and current practices. Am. J. Surg. 2025, 241, 116145. [Google Scholar] [CrossRef]
- Dijkstra, E.A.; Nilsson, P.J.; Hospers, G.A.P.; Bahadoer, R.R.; Meershoek-Klein Kranenbarg, E.; Roodvoets, A.G.H.; Putter, H.; Berglund, Å.; Cervantes, A.; Crolla, R.; et al. Locoregional Failure During and After Short-course Radiotherapy Followed by Chemotherapy and Surgery Compared with Long-course Chemoradiotherapy and Surgery: A 5-Year Follow-up of the RAPIDO Trial. Ann. Surg. 2023, 278, e766–e772. [Google Scholar] [CrossRef]
- Conroy, T.; Castan, F.; Etienne, P.L.; Rio, E.; Mesgouez-Nebout, N.; Evesque, L.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiotherapy in patients with locally advanced rectal cancer: Long-term results of the UNICANCER-PRODIGE 23 trial. Ann. Oncol. 2024, 35, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Downing, A.; Glaser, A.W.; Finan, P.J.; Wright, P.; Thomas, J.D.; Gilbert, A.; Corner, J.; Richards, M.; Morris, E.J.A.; Sebag-Montefiore, D. Functional Outcomes and Health-Related Quality of Life After Curative Treatment for Rectal Cancer: A Population-Level Study in England. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 1132–1142. [Google Scholar] [CrossRef] [PubMed]
- Verheij, F.S.; Omer, D.M.; Williams, H.; Lin, S.T.; Qin, L.X.; Buckley, J.T.; Thompson, H.M.; Yuval, J.B.; Kim, J.K.; Dunne, R.F.; et al. Long-Term Results of Organ Preservation in Patients with Rectal Adenocarcinoma Treated with Total Neoadjuvant Therapy: The Randomized Phase II OPRA Trial. J. Clin. Oncol. 2024, 42, 500–506. [Google Scholar] [CrossRef]
- Berardi, R.; Maccaroni, E.; Onofri, A.; Morgese, F.; Torniai, M.; Tiberi, M.; Ferrini, C.; Cascinu, S. Locally advanced rectal cancer: The importance of a multidisciplinary approach. World J. Gastroenterol. 2014, 20, 17279–17287. [Google Scholar] [CrossRef]
- Obias, V.J.; Reynolds, H.L., Jr. Multidisciplinary teams in the management of rectal cancer. Clin. Colon Rectal Surg. 2007, 20, 143–147. [Google Scholar] [CrossRef]
- Rouanet, P.; Castan, F.; Mazard, T.; Lemanski, C.; Nougaret, S.; Deshayes, E.; Chalbos, P.; Gourgou, S.; Taoum, C. GRECCAR 14—A multicentric, randomized, phase II-III study evaluating the tailored management of locally advanced rectal carcinoma after a favourable response to induction chemotherapy: Study protocol. Color. Dis. 2023, 25, 2078–2086. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Shi, Q.; Dasari, A.; Garcia-Aguilar, J.; Sanoff, H.; George, T.J.; Hong, T.; Yothers, G.; Philip, P.; Nelson, G.; et al. Alliance A022104/NRG-GI010: The Janus Rectal Cancer Trial: A randomized phase II/III trial testing the efficacy of triplet versus doublet chemotherapy regarding clinical complete response and disease-free survival in patients with locally advanced rectal cancer. BMC Cancer 2024, 24, 901. [Google Scholar] [CrossRef]
- Scott, A.J.; Kennedy, E.B.; Berlin, J.; Brown, G.; Chalabi, M.; Cho, M.T.; Cusnir, M.; Dorth, J.; George, M.; Kachnic, L.A.; et al. Management of Locally Advanced Rectal Cancer: ASCO Guideline. J. Clin. Oncol. 2024, 42, 3355–3375. [Google Scholar] [CrossRef]
- Dossa, F.; Chesney, T.R.; Acuna, S.A.; Baxter, N.N. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Pezeshki, P.S.; Ghalehtaki, R. The clinical application of ctDNA to predict response to neoadjuvant chemoradiotherapy in patients with locally-advanced rectal cancer. Biomark Res. 2023, 11, 81. [Google Scholar] [CrossRef]
- Kotani, D.; Oki, E.; Nakamura, Y.; Yukami, H.; Mishima, S.; Bando, H.; Shirasu, H.; Yamazaki, K.; Watanabe, J.; Kotaka, M.; et al. Molecular residual disease and efficacy of adjuvant chemotherapy in patients with colorectal cancer. Nat. Med. 2023, 29, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Khakoo, S.; Carter, P.D.; Brown, G.; Valeri, N.; Picchia, S.; Bali, M.A.; Shaikh, R.; Jones, T.; Begum, R.; Rana, I.; et al. MRI Tumor Regression Grade and Circulating Tumor DNA as Complementary Tools to Assess Response and Guide Therapy Adaptation in Rectal Cancer. Clin. Cancer Res. 2020, 26, 183–192. [Google Scholar] [CrossRef]
- Murahashi, S.; Akiyoshi, T.; Sano, T.; Fukunaga, Y.; Noda, T.; Ueno, M.; Zembutsu, H. Serial circulating tumour DNA analysis for locally advanced rectal cancer treated with preoperative therapy: Prediction of pathological response and postoperative recurrence. Br. J. Cancer 2020, 123, 803–810. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, L.; Bao, H.; Fan, X.; Xia, F.; Wan, J.; Shen, L.; Guan, Y.; Bao, H.; Wu, X.; et al. Utility of ctDNA in predicting response to neoadjuvant chemoradiotherapy and prognosis assessment in locally advanced rectal cancer: A prospective cohort study. PLoS Med. 2021, 18, e1003741. [Google Scholar] [CrossRef]
- Vidal, J.; Casadevall, D.; Bellosillo, B.; Pericay, C.; Garcia-Carbonero, R.; Losa, F.; Layos, L.; Alonso, V.; Capdevila, J.; Gallego, J.; et al. Clinical Impact of Presurgery Circulating Tumor DNA after Total Neoadjuvant Treatment in Locally Advanced Rectal Cancer: A Biomarker Study from the GEMCAD 1402 Trial. Clin. Cancer Res. 2021, 27, 2890–2898. [Google Scholar] [CrossRef]
- Watanabe, J.; Kagawa, Y.; Ando, K.; Uemura, M.; Fujimoto, Y.; Suwa, Y.; Nishizawa, Y.; Matsuhashi, N.; Izawa, N.; Muto, O.; et al. Circulating tumor DNA for predicting complete response to total neoadjuvant therapy in locally advanced rectal cancer: ENSEMBLE-2. J. Clin. Oncol. 2025, 43, 284. [Google Scholar] [CrossRef]
- Malla, M.; Loree, J.M.; Kasi, P.M.; Parikh, A.R. Using Circulating Tumor DNA in Colorectal Cancer: Current and Evolving Practices. J. Clin. Oncol. 2022, 40, 2846–2857. [Google Scholar] [CrossRef] [PubMed]
- Peking Union Medical College Hospital. Circulating Tumor DNA-Guided Neoadjuvant Treatment Strategy for Locally Advanced Rectal Cancer (CINTS-R). Available online: https://clinicaltrials.gov/study/NCT05601505?term=NCT05601505&rank=1 (accessed on 2 June 2025).
- Helsinki University Central Hospital. Systemic Neoadjuvant and Adjuvant Control by Precision Medicine in Rectal Cancer (SYNCOPE). Available online: https://clinicaltrials.gov/study/NCT04842006?term=NCT04842006%20&rank=1 (accessed on 2 June 2025).
- Cancer Institute and Hospital, CAMS & PUMC, China. MRI Simulation-Guided Boost in Short-Course Preoperative Radiotherapy for Unresectable Rectal Cancer (SUNRISE). Available online: https://clinicaltrials.gov/study/NCT03714490?term=NCT03714490&rank=1 (accessed on 2 June 2025).
- OHSU Knight Cancer Institute. Establishing a ctDNA Biomarker to Improve Organ Preserving Strategies in Patients with Rectal Cancer. Available online: https://clinicaltrials.gov/study/NCT05081024?term=NCT05081024%20&rank=1 (accessed on 2 June 2025).
- Grupo Espanol Multidisciplinario del Cancer Digestivo. GEMCAD-REVEAL STUDY—Circulating Tumor DNA as a Predictor of Relapse in Patients with Locally Advanced Rectal Cancer. (REVEAL). Available online: https://clinicaltrials.gov/study/NCT05674422?term=NCT05674422&rank=1 (accessed on 2 June 2025).
- Sixth Affiliated Hospital of Sun Yat-sen University. Dynamic Multi-Omics Integration Model to Predict Neoadjuvant Therapy Response in Locally Advanced Rectal Cancer. Available online: https://clinicaltrials.gov/study/NCT06364371?term=NCT06364371&rank=1 (accessed on 2 June 2025).

{kind=link}
| Trial Name | Study Design | Population | Treatment Arm | Primary Endpoint | Key Findings |
|---|---|---|---|---|---|
| Cercek et al. [45] | Prospective phase 2 | dMMR/MSI-H stage II or III | Neoadjuvant Dostarlimab × 6 months then restaging if cCR → Watch and Wait if non cCR → LCCRT then TME | cCR at 12 months after Dostarlimab | 100% cCR |
| RAPIDO [13] | RCT phase 3 | ≥1 high-risk feature: cT4 or cN2, EMVI, positive MRF, or lateral LN | SCRT → FOLFOX × 9/CAPEOX × 6 → TME vs. LCCRT → TME → with/without FOLFOX × 12/CAPEOX × 8 | 3-year DRTF | 23.7% vs. 30.4% |
| PRODIGE -23 [12] | RCT phase 3 | cT3 or cT4 | FOLFORINOX × 6 → LCCRT → TME → FOLFOX × 6/Capecitabine vs. LCCRT → TME → FOLFOX × 6/Capecitabine | 3-year DFS | 75.7% vs. 68.5% |
| PROSPECT [36] | RCT, noninferiority study | cT2N1, cT3N0, or cT3N1 and candidates for sphincter-sparing surgery | Preoperative FOLFOX × 6 → Restaging if ≥20% response → TME then adjuvant CMT if <20% response → LCCRT → TME then adjuvant CMT vs. LCCRT → TME then adjuvant CMT | DFS | HR 0.92 (90.2% CI: 0.74–1.14) p = 0.005 |
| OPRA [16] | RCT phase 2 | stage II or III | FOLOX × 8/CAPEOX × 5 → LCCRT vs. LCCRT → FOLOX × 8/CAPEOX × 5 restaging both arms if cCR/ncCR → Watch and Wait if incomplete response → TME | DFS | 3-year DFS 76% in both groups |
| Trial ID | Study Design | Population | Treatment/Intervention | Primary Endpoint | ctDNA Application |
|---|---|---|---|---|---|
| NCT05601505 (CINTS-R) [75] | RCT phase 2 | stage II or III | -Control: nCRT then TME -Experimental: if baseline ctDNA VAF < 0.5% → nCRT, VAF ≥ 0.5% or +post-CRT ctDNA → TNT then TME | 2-year DRTF | ctDNA-guided neoadjuvant treatment strategies |
| NCT04842006 (SYNCOPE) [76] | RCT | stage II or III with EMVI | -Control: LCCRT then TME -Experimental: TNT with SCRT then CAPEOX then TME | RFS | Postoperative ctDNA for MRD assessment and its correlation with RFS |
| NCT03714490 (SUNRISE) [77] | RCT phase 2 | stage II or III with cT4b or positive MRF | -Control: LCCRT then TME -Experimental: TNT with SCRT then CAPEOX then TME | R0 resection rate | Correlation of ctDNA clearance or persistence with treatment response and DFS/OS |
| NCT05081024 (ctTRAC) [78] | Prospective observational cohort study | stage II or III planned for TNT | Blood collection for ctDNA at baseline, every 2 months while undergoing TNT, and then every 3 months for up to 3 years after completion of TNT | cCR rate | ctDNA monitoring as biomarker to predict cCR after TNT |
| NCT05674422 (REVEAL) [79] | Prospective observational cohort study | stage II or III planned for TNT then WW if cCR or ncCR | Blood collection for ctDNA up to 2 years after starting TNT | PPV and NPV of post-TNT ctDNA to identify relapses in 2 years after TNT | ctDNA monitoring as biomarker to predict relapse after TNT |
| NCT06364371 [80] | Prospective observational cohort study | stage II or III planned for neoadjuvant treatment | Monitoring MRI scans, histopathology slides, CEA and ctDNA at pre-, during, and post-treatment | Area under curve of prediction model for predicting pCR | ctDNA monitoring as biomarker to predict pCR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pakvisal, N.; Pappas, L.; Caughey, B.A.; Ricciardi, R.; Parikh, A. Personalized Treatment Modalities for Rectal Cancer: Advances in Neoadjuvant Treatment. J. Clin. Med. 2025, 14, 4411. https://doi.org/10.3390/jcm14134411
Pakvisal N, Pappas L, Caughey BA, Ricciardi R, Parikh A. Personalized Treatment Modalities for Rectal Cancer: Advances in Neoadjuvant Treatment. Journal of Clinical Medicine. 2025; 14(13):4411. https://doi.org/10.3390/jcm14134411
Chicago/Turabian StylePakvisal, Nussara, Leontios Pappas, Bennett A. Caughey, Rocco Ricciardi, and Aparna Parikh. 2025. "Personalized Treatment Modalities for Rectal Cancer: Advances in Neoadjuvant Treatment" Journal of Clinical Medicine 14, no. 13: 4411. https://doi.org/10.3390/jcm14134411
APA StylePakvisal, N., Pappas, L., Caughey, B. A., Ricciardi, R., & Parikh, A. (2025). Personalized Treatment Modalities for Rectal Cancer: Advances in Neoadjuvant Treatment. Journal of Clinical Medicine, 14(13), 4411. https://doi.org/10.3390/jcm14134411