
The Mental Health of Children with Cerebral Palsy: A Review of the Last Five Years of Research

 and
and 
Abstract
1. Introduction
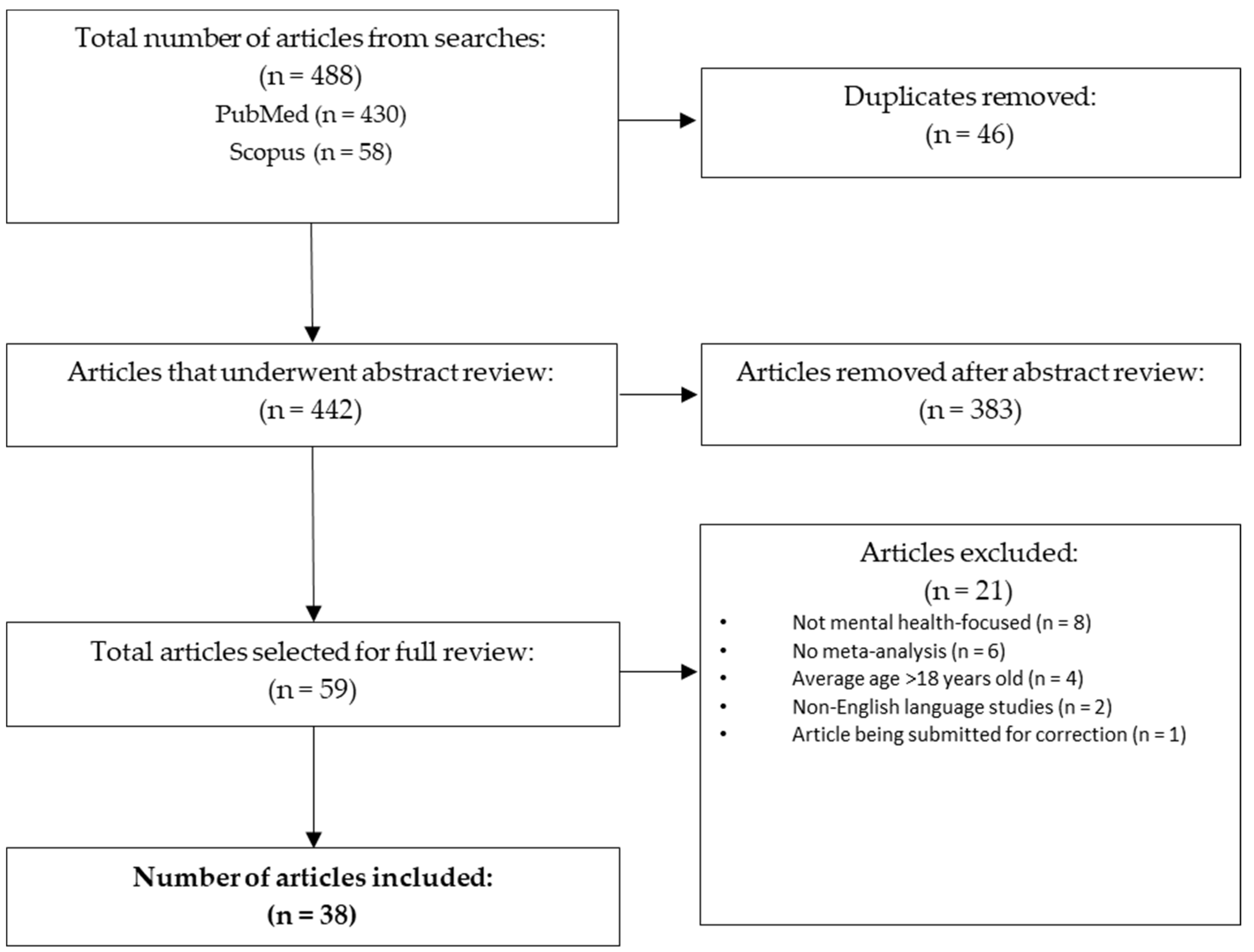
2. Materials and Methods
3. Results
3.1. Overall Prevalence and Trajectory of Mental Health Disorders
3.2. Autism Spectrum Disorder
3.3. Attention-Deficit/Hyperactivity Disorder
3.4. Intellectual Developmental Disorder (Intellectual Disability)
3.5. Anxiety, Depression, and Mood
3.6. Behavioral Concerns and Disorders
3.7. Academic Difficulties and Learning Disorders
3.8. Interventions for Children with CP
3.8.1. Parent-Focused Interventions
3.8.2. Parent- and Child-Focused Interventions
3.8.3. Child-Focused Interventions
4. Discussion
4.1. Specific Mental Health Concerns
4.2. Academic Functioning
4.3. Interventions
4.4. Assessment Concerns
4.5. Limitations
4.6. Implications for Clinical and Academic Practice:
- Children and adolescents with CP should be screened regularly for mental health concerns and disorders, starting as early as the preschool years. This is particularly true for symptoms consistent with ADHD, ASD, and behavioral concerns.
- Considering that early symptoms of mental health are predictive of later mental health concerns and that symptoms are likely to persist, early intervention for mental health concerns should be provided to children and adolescents in addition to preventative care or addressing subclinical mental health symptoms.
- Parenting behavioral interventions should be recommended to families of children with behavioral concerns.
- Caution should be taken when choosing mental and cognitive assessment tools and results interpreted with caution, particularly for children with more severe motor impairments. The Strengths and Difficulties Questionnaire may be a useful screening tool for use with youth with CP.
- Children with CP should be assessed regularly for global and specific learning concerns within academic settings to allow for identification of needs and tailored academic intervention.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CP | Cerebral Palsy |
| ADHD | Attention-Deficit/Hyperactivity Disorder |
| ASD | Autism Spectrum Disorder |
| ID | Intellectual Disability |
| GMFCS | Gross Motor Function Classification System |
| EAA | Equine-Assisted Activities |
| PACT | Parenting Acceptance and Commitment Therapy |
Appendix A. Search Strings
Appendix B

{kind=link}
| Author/Year | Purpose | Study Design | Sample | Relevant Findings |
|---|---|---|---|---|
| Horwood L, Li P, Mok E, Oskoui M, Shevell M, Constantin E (2019) [34] | Determine the prevalence of behavioral challenges in preschool and school-aged children with CP and assess the association between behavioral challenges and sleep problems, nighttime pain, and child characteristics. | Cross-sectional study | Caregivers of 113 children with CP | Approximately 26% of children with CP had behavioral challenges. Sleep problems and nighttime pain were also associated with behavioral challenges. Sleep and behavioral problems were highly associated even when adjusting for nighttime pain and age. |
| Whitney DG, Warschausky SA, Peterson MD. (2019) [11] | Examine the prevalence of mental health disorders among children with and without CP. Examine how physical risk factors in children with CP may mitigate any elevated risk of mental disorders in the population. | Cross-sectional study | 111 children with and without CP | Children with CP had higher odds of developing mental health disorder, with the exception of ADHD. Risk for depression decreased when adjusting for physical factors, but anxiety and behavioral concerns remained high. When assessed individually, risk for depression was no longer increased when controlling for low physical activity and pain. |
| Whitney DG, Peterson MD, Warschausky SA. (2019) [25] | Examine how social factors may mitigate elevated risks of mental health disorders in children with CP. | Cross-sectional study | 111 children with and without CP | Children with CP had a higher likelihood of developing anxiety and behavioral problems after controlling for sociodemographic factors and chronic pain. This risk remained high even after adjusting for being engaged in activities. However, when adjusting for challenges with friendships, the risk for anxiety was no longer increased in children with CP. After adjusting for bullying, the odds of behavioral problems were attenuated but anxiety risk remained high. |
| Påhlman M, Gillberg C, Himmelmann K. (2019) [18] | Describe associated impairments and motor function in children with CP. Examine the association between CP type, motor functioning, and associated impairments in a population group. Compare associated impairment in the same children at school age. | Population-based study | 264 children with CP born between 1999 and 2006 identified through the CP Register of western Sweden (limited to the county of Vastra Gotaland) | Associated impairments were found in 75% of this sample. ID was present in 53%, ASD was present in 18%, and ADHD was present in 21%. Except for ADHD and ASD, all impairments increased with more severe motor impairment. |
| Shahriari, Y., Ghasemzadeh, S., & Vakili, S. (2019) [47] | Examine how effective Child Centered Play Therapy is in improving internalizing and externalizing behaviors for children with CP. | Applied and quasi-experimental with pre- and post-tests | 30 participants with CP and comorbid medical diagnosis of paraplegia and mild to moderate monoplegia, randomly assigned evenly (n = 15) between control and intervention groups | A significant reduction in anxiety, depression, offense, and aggression was observed in the experimental group at both post-test and follow-up, as compared to the control group. There was no change in externalizing offensive behavior. |
| Pereira A, Rosário P, Lopes S, Moreira T, Magalhães P, Núñez JC, Vallejo G, Sampaio A. (2019) [39] | Examine the efficacy of an educational program focused on the promotion of school engagement in children with CP. | Quasi-experimental design (no control group) | 15 children with CP recruited from CP rehab centers in Portugal | Participation in the program improved behavioral engagement, emotional engagement, and cognitive engagement (the dimensions of school engagement). |
| Gardiner E, Miller AR, Lach LM (2020) [33] | Examined the extent to which behavioral problems represent a functional characteristic that crosses diagnostic boundaries. | Cross-sectional study | 179 caregivers of children who have CP, ASD, and global developmental disability/ID | All three groups had matching profile topographies, indicating substantial difficulties with hyperactivity/inattention. |
| Rackauskaite G, Bilenberg N, Uldall P, Bech BH, Østergaard J (2020) [13] | Compare prevalence of mental disorders in a sample of children and adolescents with CP and age/sex matched controls. Examine the association between motor function and mental disorders in youth with CP. | Register-linkage follow-up study | 977 children with CP born between 1997 and 2003 identified from the Danish National Cerebral Palsy Registry and 2627 children without CP matched by age and gender | Prevalence of mental disorders was significantly higher in children with CP compared to controls. ID was associated with motor function. |
| McMahon J, Harvey A, Reid SM, May T, Antolovich G. (2020) [30] | Describe the prevalence of and factors associated with anxiety in children with CP and determine how often providers screen for and manage anxiety in children with CP. | Cross-sectional observational study | 172 families of children with CP participated | A total of 38% of children were found to have clinically significant anxiety based on parent report, and 46% had clinically significant anxiety on child report. Girls were twice as likely to have anxiety. Parent and child reports were highly correlated. Based on reports on the Screen for Child Anxiety Related Disorders measure, 16 children (43%) with clinically significant anxiety were not identified by a provider. |
| Påhlman M, Gillberg C, Wentz E, Himmelmann K. (2020) [19] | Estimate the screen-positive rates of ADHD and ASD in a group of children with CP. | Screening study with parent-completed questionnaires | 264 school-aged children with CP identified through the CP registrar of western Sweden | One-third screened positive for ASD and half screened positive for ADHD. Children with epilepsy, impaired speech, and ID screened positive for ADHD and ASD more often. Severe motor impairment was associated with screening positive for ASD. |
| Leader G, Molina Bonilla P, Naughton K, Maher L, Casburn M, Arndt S, Mannion A (2021) [20] | Identify frequency of GI symptoms, sleep problems, internalizing/externalizing symptoms, and ASD symptoms in a sample of children with CP. Examine impact of comorbidities on frequency and severity of behavioral problems in this sample. | Parent-completed questionnaires | 104 youth with CP | High frequency of behavior problems, sleep problems, gastrointestinal symptoms, ASD symptoms, and internalizing/externalizing symptoms were found in this sample. Relationships were found between the following: sleep problems and behavior problems; GI symptoms and sleep problems; GI symptoms and internalizing/externalizing problems. Behavioral problems were predicted by sleep problems, internalizing/externalizing symptoms, ID, and ASD symptoms. |
| Salie R, Eken MM, Donald KA, Fieggen AG, Langerak NG (2021) [31] | Investigate the prevalence and level of disability due to pain, health-related quality of life, and mental health in adolescents and adults with CP. | Case-control study | 31 adolescents and 30 adults with CP and typically developing peers | Adolescents and adults with CP reported experiencing more frequent pain in their lower limbs with associated higher levels of disability due to the pain, lower health-related quality of life compared to typically developing peers. There were no differences found in mental health outcomes for those with CP compared to typically developing peers. |
| Bjorgaas HM, Elgen IB, Hysing M. (2021) [14] | Examine trajectories of mental health disorders and association with risk factors in children with CP. | Assessment at the age 7 and 11 | 47 children with CP born 2001–2003 living in the Western Health Region of Norway | Significant increase in prevalence of emotional disorders between ages of 7 and 11. Stable prevalence of behavioral disorders. Half of the sample met criteria for a mental health disorder at both time points. Subthreshold mental health disorders at age 7 predicted mental health disorders at age 11. |
| Påhlman M, Gillberg C, Himmelmann K. (2021) [17] | Estimate the prevalence of ASD and ADHD in a population of school aged children with CP. Describe diagnoses in relation to associated characteristics. Compare screening rates to diagnoses. | Screening and assessments | 200 children with CP | A total of 45% of children were diagnosed with ASD, ADHD, or both. ASD was predicted by ID and ADHD. ADHD was predicted by ID and ASD. |
| Cummins D, Kerr C, McConnell K, Perra O. (2021) [27] | Describe the association between spastic CP subtypes and severe ID across gestational age categories, standardized birthweight scores, motor severity of CP, and participants’ sex. Investigate how gestational age categories moderate the association between spastic CP subtypes and severe ID, while controlling for standardized birthweight scores and participant sex. | Population-based, cross-sectional study using data from the Northern Ireland Cerebral Palsy Register (NICPR) | 1452 individuals with prenatal or perinatal spastic CP, data from the Northern Ireland Cerebral Palsy Register (NICPR) | A total of 40.4% of children were diagnosed with ID. Severe ID was more likely in infants born at term compared to those born before 36 weeks. Infants smaller than their gestational age were more at risk of having severe ID compared to those of a normative birth weight. |
| Casseus M, Cheng J. (2021) [22] | Identify the proportion of children with CP who have an unmet need for care coordination. Examine the physical and functional health of this population. Examine if unmet need differs by CP severity or demographic characteristics. | Survey Analysis | 102,341 NSCH respondents from the years of 2016, 2017, and 2018 | Children diagnosed with CP had significantly higher prevalence of all comorbid conditions and functional disabilities. More than half of children with CP had an unmet need for care coordination. |
| Ahn B, Joung YS, Kwon JY, Lee DI, Oh S, Kim BU, Cha JY, Kim JH, Lee JY, Shin HY, Seo YS. (2021) [41] | Examine the effectiveness of equine-assisted activities on attention and quality of life in children with CP. Examine comorbidity between CP and ADHD and the effectiveness of this intervention for children with this comorbidity. | 46 children diagnosed with CP | Children with CP in the excursive group demonstrated improvement in attention. Sub-analysis of children with comorbid CP and ADHD demonstrated improvement in attention and perceived social skills after 16 of equine-assisted activities, compared to the control group. | |
| Jarl J, Alriksson-Schmidt A (2021) [37] | Investigate whether adolescents with CP in Sweden have lower school achievement and if school achievement varies by disability-specific factors | Population-based register study | Children with CP in Sweden, born between 1990 and 1999 with a matched comparison group from the general population; for compulsory school, 1648 cases with CP and 16,838 comparators; for secondary school, (voluntary in Sweden) 2541 cases with CP and 122,999 comparators | Adolescents with CP had a substantial reduction in school outcomes (partly explained by the high presence of ID). Children with CP had lower levels of education when compared to the general population, even after controlling for ID and motor difficulties. |
| de Freitas Feldberg SC, da Silva Gusmão Cardoso T, Santos FH, Muszkat M, Bueno OFA, Berlim de Mello C. (2021) [36] | Investigate aspects of numerical cognition in a sample of bilateral and unilateral CP and whether the cognitive deficits and learning difficulties follow the pattern of primary or secondary dyscalculia. | Exploratory cross-sectional study | 19 children/adolescents recruited from a multidisciplinary center for neurodevelopmental disorders in Sao Paulo, Brazil compared to 31 typically developing children | The unilateral CP group showed significantly lower performance on the writing and reading subtests compared to the traditionally developing group. Both the unilateral and bilateral CP groups had significantly lower arithmetic performance than the traditionally developing group. CP groups had worse performance on tasks of working memory and cognition as well as worse performance on tests involving numerical cognition. Concluded that the mathematics learning disorder was secondary to the neurological disorder and that the impairment in math skills was likely due to global cognitive dysfunctions (i.e., visual-spatial processes and working memory). |
| De Clercq LE, Soenens B, Dieleman LM, Prinzie P, Van der Kaap-Deeder J, Beyers W, De Pauw SSW (2022) [23] | Address the joint contribution of parent-related parenting behaviors and child personality on psychosocial outcomes in children with CP. | Longitudinal study | 118 families of children with CP | Externally controlling and autonomy-supportive parenting behavior remained stable over time. Externally controlling parenting related to increased behavioral problems was found in children who were lower on extraversion, conscientiousness, and imagination. Autonomy-supportive parenting was related to higher levels of psychosocial strengths and was found mostly in children who were higher on emotional stability. |
| Bjorgaas HM, Elgen IB, Hysing M (2022) [15] | Assessed changes in parent-rated mental health problems and differences in mental health problems according to informants. Assessed the validity of the Strengths and Difficulties Questionnaire for psychiatric disorders. | Survey analysis | 67 children with CP from school-starting age to pre-adolescence | Parental scores on the SDQ were elevated on emotional, hyperactivity, and total number of problems. Self-reports of impact of mental health were lower than parent reports. Parents and pre-adolescents reported elevated impact of mental health compared to teacher reports, especially on mood, conduct, and total problems. Strengths and Difficulties Questionnaire was found to be satisfactory in screening for mental health concerns in youth with CP. |
| Laporta-Hoyos, O., Pannek, K., Pagnozzi, A. M., Whittingham, K., Wotherspoon, J., Benfer, K., Fiori, S., Ware, R. S., & Boyd, R. N. (2022) [35] | Determine which combination of clinical scores is associated with psychological outcomes (cognitive, academic, and executive functioning as well as psychological adjustment) in children and adolescents with spastic motor type CP. | Cross-sectional analysis of data | 101 children and adolescents with CP recruited from the Queensland Cerebral Palsy and Rehabilitation Research Centre | Lesions in the medial dorsal thalamus and parietal lobe lesions significantly accounted for poorer verbal proxy IQ ratings. Compared to those with unilateral left-sided lesions, those with bilateral lesions performed better in verbal cognitive functions. Children with CP with ventral posterior lateral thalamus lesions had better parent-related behavioral displays of executive functioning when controlling for the presence of an epilepsy diagnosis. The semi-quantitative scale for structural MRI scoring has implications for personalized interventions for children with CP. |
| PÅhlman M, Gillberg C, Himmelmann K. (2022) [16] | Describe and compare neuroimaging patterns in a group of children with CP and relate findings to ADHD diagnosis, ASD diagnosis, and other associated characteristics. | Population-based study | 184 children with CP born between 1999 and 2006 identified through the CP register of western Sweden | ASD and ADHD were common in all neuroimaging patterns. The highest prevalence of ASD was found in children with predominant white matter injury. The highest prevalence of ADHD was found in children with middle cerebral artery infarction. |
| Mak C, Whittingham K, Cunnington R, Chatfield M, Boyd RN. (2022) [44] | Examine treatment effects at a 6-month follow-up and retention of a RCT of mindfulness-based yoga program (MiYoga) for CP. | 6-month follow-up of a waitlist control randomized controlled trial | 41 parent-child dyads with a child diagnosed with CP participated in initial intervention; 23 of these dyads completed the 6-month follow-up | Child executive and physical function, in addition to parent well-being, improved significantly from pre-intervention to 6-month follow-up, possibly demonstrating a delayed effect of the intervention. No significant changes between pre-intervention or post-intervention to 6-month follow-up on child attention variables or parental mindfulness. |
| Leader G, Mooney A, Chen JL, Whelan S, Naughton K, Maher L, Mannion A. (2022) [21] | Examined the frequency of comorbidities in children with ASD alone, CP alone, and those with comorbid CP and ASD. | Screening study | 96 children with a diagnosis of CP, ASD, or comorbid CP and ASD | Significant group differences in sleep problems, social communication, and adaptive behavior. ID significantly predicted levels of adaptive behavior. |
| Olusanya BO, Gladstone M, Wright SM, Hadders-Algra M, Boo NY… (2022) [28] | Report the best available evidence on the global and regional prevalence of CP and developmental ID and the associated “years lived with disability” among children under five years of age in 2019. | Cross-sectional analysis of data | GBD-WHO Rehabilitation Database-data from 204 countries | CP has the highest prevalence in low- and middle-income countries. Of the 662.8 million children under five, 8.1 million (or 1.2%) were estimated to have CP and 16.11 million (or 2.4%) were estimated to have ID. |
| Ödek, Uğur & Özcan, kürşat & Ozyurt, Gonca & Akpinar, Selcuk. (2022) [45] | Examine the benefits of equine-facilitated activities on symptoms of anxiety, aggression, empathy, and emotional regulation in children with CP. Examine the impact of equine facilitated activities on maternal depression and anxiety. | Between-groups design | 20 children with CP and their mothers | Eight weeks of adaptive riding was associated with decreases in the children’s anxiety and aggression, in addition to decreased maternal depression. The intervention was associated with improvements in emotional regulation and empathy. |
| Whittingham K, Sheffield J, Mak C, Wright A, Boyd RN. (2022) [48] | Examine the effectiveness of Parenting Acceptance and Commitment Therapy in improving the emotional availability of the parent/child relationship, parental psych well-being, child psych adjustment, and quality of life. | RCT with waitlist control | 67 parents of children with CP | Two components of parental emotional availability (parental non-intrusiveness and child involvement) significantly improved with intervention. Parents reported improved comfort with their child’s CP diagnosis, higher likelihood to seek help, higher likelihood to connect with others, and greater meaningful living. |
| Samijn B, Van den Broeck C, Plasschaert F, Pascal A, Deschepper E, Hoebeke P, Van Laecke E. (2022) [46] | Examine the effectiveness of incontinence training with urotherapy in a sample of children with CP. | Populated-based case-control study | 21 children with CP and 24 typically developing children with either daytime-only or both daytime and nocturnal enuresis | For children with CP, the effectiveness rate of incontinence training is lower. Compared to typically developing peers, changes from incontinence training are slower to occur in children with CP. |
| Cribb CF, Keko M, Creveling S, Rochani HD, Modlesky CM, Colquitt G (2023) [12] | Determine the relationship between prevalence of mental health disorders and participation in physical activity and sports. | Survey analysis | 458 children with CP and 40,091 typically developing children whose parents participated in the 2016–2020 NSCH | Children with CP had a higher prevalence of mental health disorders and were more likely to receive mental health care. Children with CP had higher rates of anxiety, depression, behavioral disorders, and ADHD. Participation in sports and daily physical activity was associated with reduced likelihood of some conditions. |
| Alibakhshi, H., Simin ghalamaval, M., Ayoubi Avaz, K., Salmani, M., Pahlavanian, A., Motaharinezhad, F., Kanani, Z (2023) [42] | Examine the effectiveness of teaching communication skills to mothers of children with CP and evaluate child behavioral problems. | Semi-experimental design with pre- and post-test assessment | 42 mothers of children with CP who were displaying behavioral problems | Communication skills group demonstrated significant reduction in the following areas of measurement: aggression & hyperactivity, social incompatibility, antisocial behaviors, anxiety and depression, and general behavioral problems. |
| Testani D, McMorris CA, Clark CA, Sanguino H, Condliffe EG, Noel ME, Kopala Sibley DC, Brunton LK (2024) [32] | Examine individual and cumulative impacts of physiological symptoms on anxiety and depression in youth with CP. | Cross-sectional observational study | 40 youth with CP and their caregivers | Youth with CP experienced elevated levels of physiological symptoms and elevated anxiety and depression symptoms. Factors also contributing to caregiver reports of the child’s anxiety and depression included fatigue, severe pain, sleep efficiency, and level of physical activity. |
| Fitneva SA, Corbett BA, Prasad AN. (2024) [29] | Analyze behavioral outcomes who had severe epilepsy, CP, and ID compared to typically developing peers. | Review and analysis of longitudinal survey | 10,879 2–3-year-old children from 3 cycles of Canada’s National Longitudinal Survey of Children and Youth | Children with neurodevelopmental disabilities and significant differences in behavioral outcomes at younger ages (higher levels of hyperactivity/inattention, challenges with prosocial behaviors, separation anxiety, and mood/anxiety concerns) when compared to typically developing peers. |
| Chen Q, Chen M, Bao W, Strathearn L, Zang X, Meng L, Xu G. (2024) [24] | Examine associations between CP with ADHD and ASD. | Large-scale nationwide population-based study | 177,899 children between the ages of 3 and 17 years old. Data taken from the National Health Interview Survey from 1997–2003 and 2008–2018 | Children with CP had a higher prevalence of ADHD and ASD. |
| Casseus M, Cheng J, Reichman NE. (2024) [26] | Estimate associations between clinical and functional characteristics and a diagnosis of ADHD in a sample of children and young adults with CP. | Retrospective, cross-sectional studying using electronic health records | 1145 children and young adults with CP | A total of 18.1% of the sample had a diagnosis of ADHD. Those with bilateral spastic CP had lower odds of ADHD. GMFCS levels III-IV were associated with a lower odds of ADHD. |
| Chen YC, Chang WP, Liang KJ, Chen CL, Chen HY, Chen SP, Chan PS (2024) [43] | Examine the effects of neurofeedback training on attention task performance in children with CP and attention deficits. | Two-arm parallel design randomized trial | 19 children with both CP and attention deficits | The neurofeedback intervention group demonstrated decreased theta/beta ratios at post-training compared to the control group and within-group improvement during the training intervention. Neurofeedback group demonstrated a trend for decreased omission rates on an assessment of attention related problems. |
| Micheletti S, Galli J, Vezzoli M, Scaglioni V, Agostini S, Calza S, Merabet LB, Fazzi E. (2024) [38] | Investigate the prevalence and clinical manifestations of learning disorders (reading, writing, and mathematics disorders) in a group of children with CP with normal verbal IQ and reduced motor involvement; explore how the clinical profile from a group of children with CP and learning disorders differs from that of children with CP without learning disorders and children with SLDs. | Prospective cross-sectional study | 42 children with CP and 60 children with SLDs | A total of 59% of the children with CP had reading, writing, or mathematics disorders. Children with CP with learning disorders had a low performance IQ, normal phonological awareness, and working memory difficulties. Children with SLDs had normal performance IQ, impaired phonological awareness, and mild working memory difficulties. |
| Wotherspoon J, Whittingham K, Sheffield J, Boyd RN. (2024) [40] | Test the efficacy of a novel web-based cognitive rehabilitation program (Strengthening Mental Abilities through Relational Training) for children between 8 and 12 years old with mild to moderate congenital CP. | Mixed methods sequential explanatory design | 21 Australian children with CP | No group differences found between the experimental group and the control group (perhaps due to specific challenges in engaging with and completing the training). |
References
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.P.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral Palsy. Nat. Rev. Dis. Primers 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Hines, M.; Goldsmith, S.; Barclay, R. Clinical Prognostic Messages from a Systematic Review on Cerebral Palsy. Pediatrics 2012, 130, e1285–e1312. [Google Scholar] [CrossRef] [PubMed]
- Downs, J.; Blackmore, A.M.; Epstein, A.; Skoss, R.; Langdon, K.; Jacoby, P.; Whitehouse, A.J.O.; Leonard, H.; Rowe, P.W.; Glasson, E.J. The Prevalence of Mental Health Disorders and Symptoms in Children and Adolescents with Cerebral Palsy: A Systematic Review and Meta-Analysis. Dev. Med. Child Neurol. 2018, 60, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Bjorgaas, H.M.; Hysing, M.; Elgen, I. Psychiatric Disorders among Children with Cerebral Palsy at School Starting Age. Res. Dev. Disabil. 2012, 33, 1287–1293. [Google Scholar] [CrossRef]
- Parkes, J.; White-Koning, M.; Dickinson, H.O.; Thyen, U.; Arnaud, C.; Beckung, E.; Fauconnier, J.; Marcelli, M.; McManus, V.; Michelsen, S.I.; et al. Psychological Problems in Children with Cerebral Palsy: A Cross-Sectional European Study. J. Child Psychol. Psychiatry 2008, 49, 405–413. [Google Scholar] [CrossRef]
- Craig, F.; Savino, R.; Trabacca, A. A Systematic Review of Comorbidity between Cerebral Palsy, Autism Spectrum Disorders and Attention Deficit Hyperactivity Disorder. Eur. J. Paediatr. Neurol. 2019, 23, 31–42. [Google Scholar] [CrossRef]
- Gorter, J.W.; Fehlings, D.; Ferro, M.A.; Gonzalez, A.; Green, A.D.; Hopmans, S.N.; McCauley, D.; Palisano, R.J.; Rosenbaum, P.; Speller, B. Correlates of Mental Health in Adolescents and Young Adults with Cerebral Palsy: A Cross-Sectional Analysis of the MyStory Project. J. Clin. Med. 2022, 11, 3060. [Google Scholar] [CrossRef]
- Sigurdardottir, S.; Indredavik, M.S.; Eiriksdottir, A.; Einarsdottir, K.; Gudmundsson, H.S.; Vik, T. Behavioural and Emotional Symptoms of Preschool Children with Cerebral Palsy: A Population-Based Study. Dev. Med. Child Neurol. 2010, 52, 1056–1061. [Google Scholar] [CrossRef]
- Fluss, J.; Lidzba, K. Cognitive and Academic Profiles in Children with Cerebral Palsy: A Narrative Review. Ann. Phys. Rehabil. Med. 2020, 63, 447–456. [Google Scholar] [CrossRef]
- Whittingham, K.; Sanders, M.; McKinlay, L.; Boyd, R.N. Interventions to Reduce Behavioral Problems in Children with Cerebral Palsy: An RCT. Pediatrics 2014, 133, e1249–e1257. [Google Scholar] [CrossRef]
- Whitney, D.G.; Warschausky, S.A.; Peterson, M.D. Mental Health Disorders and Physical Risk Factors in Children with Cerebral Palsy: A Cross-Sectional Study. Dev. Med. Child Neurol. 2019, 61, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Cribb, C.F.; Keko, M.; Creveling, S.; Rochani, H.D.; Modlesky, C.M.; Colquitt, G. Mental Health, Physical Activity, and Sports among Children with Cerebral Palsy. Child Care Health Dev. 2023, 49, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Rackauskaite, G.; Bilenberg, N.; Uldall, P.; Bech, B.H.; Østergaard, J. Prevalence of Mental Disorders in Children and Adolescents with Cerebral Palsy: Danish Nationwide Follow-up Study. Eur. J. Paediatr. Neurol. 2020, 27, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Bjorgaas, H.M.; Elgen, I.B.; Hysing, M. Trajectories of Psychiatric Disorders in a Cohort of Children with Cerebral Palsy across Four Years. Disabil. Health J. 2021, 14, 100992. [Google Scholar] [CrossRef]
- Bjorgaas, H.M.; Elgen, I.B.; Hysing, M. Mental Health in Pre-Adolescents with Cerebral Palsy: Exploring the Strengths and Difficulties Questionnaire as a Screening Tool in a Follow-Up Study Including Multi-Informants. Children 2022, 9, 1009. [Google Scholar] [CrossRef]
- PÅhlman, M.; Gillberg, C.; Himmelmann, K. Neuroimaging Findings in Children with Cerebral Palsy with Autism and/or Attention-Deficit/Hyperactivity Disorder: A Population-Based Study. Dev. Med. Child Neurol. 2022, 64, 63–69. [Google Scholar] [CrossRef]
- Påhlman, M.; Gillberg, C.; Himmelmann, K. Autism and Attention-Deficit/Hyperactivity Disorder in Children with Cerebral Palsy: High Prevalence Rates in a Population-Based Study. Dev. Med. Child Neurol. 2021, 63, 320–327. [Google Scholar] [CrossRef]
- Påhlman, M.; Gillberg, C.; Himmelmann, K. One-Third of School-Aged Children with Cerebral Palsy Have Neuropsychiatric Impairments in a Population-Based Study. Acta Paediatr. 2019, 108, 2048–2055. [Google Scholar] [CrossRef]
- Påhlman, M.; Gillberg, C.; Wentz, E.; Himmelmann, K. Autism Spectrum Disorder and Attention-Deficit/Hyperactivity Disorder in Children with Cerebral Palsy: Results from Screening in a Population-Based Group. Eur. Child Adolesc. Psychiatry 2020, 29, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Leader, G.; Molina Bonilla, P.; Naughton, K.; Maher, L.; Casburn, M.; Arndt, S.; Mannion, A. Complex Comorbid Presentations Are Associated with Harmful Behavior Problems among Children and Adolescents with Cerebral Palsy. Dev. Neurorehabil. 2021, 24, 25–34. [Google Scholar] [CrossRef]
- Leader, G.; Mooney, A.; Chen, J.L.; Whelan, S.; Naughton, K.; Maher, L.; Mannion, A. The Co-Occurrence of Autism Spectrum Disorder and Cerebral Palsy and Associated Comorbid Conditions in Children and Adolescents. Dev. Neurorehabil. 2022, 25, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Casseus, M.; Cheng, J. Children with Cerebral Palsy and Unmet Need for Care Coordination. J. Dev. Behav. Pediatr. 2021, 42, 605–612. [Google Scholar] [CrossRef]
- De Clercq, L.E.; Soenens, B.; Dieleman, L.M.; Prinzie, P.; Van der Kaap-Deeder, J.; Beyers, W.; De Pauw, S.S.W. Parenting and Child Personality as Modifiers of the Psychosocial Development of Youth with Cerebral Palsy. Child Psychiatry Hum. Dev. 2022, 53, 137–155. [Google Scholar] [CrossRef]
- Chen, Q.; Chen, M.; Bao, W.; Strathearn, L.; Zang, X.; Meng, L.; Xu, G. Association of Cerebral Palsy with Autism Spectrum Disorder and Attention-Deficit/Hyperactivity Disorder in Children: A Large-Scale Nationwide Population-Based Study. BMJ Paediatr. Open 2024, 8, e002343. [Google Scholar] [CrossRef] [PubMed]
- Whitney, D.G.; Peterson, M.D.; Warschausky, S.A. Mental Health Disorders, Participation, and Bullying in Children with Cerebral Palsy. Dev. Med. Child Neurol. 2019, 61, 937–942. [Google Scholar] [CrossRef]
- Casseus, M.; Cheng, J.; Reichman, N.E. Clinical and Functional Characteristics of Children and Young Adults with Cerebral Palsy and Co-Occurring Attention-Deficit/Hyperactivity Disorder. Res. Dev. Disabil. 2024, 151, 104787. [Google Scholar] [CrossRef] [PubMed]
- Cummins, D.; Kerr, C.; McConnell, K.; Perra, O. Risk Factors for Intellectual Disability in Children with Spastic Cerebral Palsy. Arch. Dis. Child 2021, 106, 975–980. [Google Scholar] [CrossRef]
- Olusanya, B.O.; Gladstone, M.; Wright, S.M.; Hadders-Algra, M.; Boo, N.-Y.; Nair, M.K.C.; Almasri, N.; Kancherla, V.; Samms-Vaughan, M.E.; Kakooza-Mwesige, A.; et al. Cerebral Palsy and Developmental Intellectual Disability in Children Younger than 5 Years: Findings from the GBD-WHO Rehabilitation Database 2019. Front. Public Health 2022, 10, 894546. [Google Scholar] [CrossRef]
- Fitneva, S.A.; Corbett, B.A.; Prasad, A.N. Psychosocial Correlates of Neurodevelopmental Disabilities in 2- to 3-Year-Olds. Epilepsy Behav. 2023, 146, 109370. [Google Scholar] [CrossRef]
- McMahon, J.; Harvey, A.; Reid, S.M.; May, T.; Antolovich, G. Anxiety in Children and Adolescents with Cerebral Palsy. J. Paediatr. Child Health 2020, 56, 1194–1200. [Google Scholar] [CrossRef]
- Salie, R.; Eken, M.M.; Donald, K.A.; Fieggen, A.G.; Langerak, N.G. Pain, Health-Related Quality of Life, and Mental Health of Adolescents and Adults with Cerebral Palsy in Urban South Africa. Disabil. Rehabil. 2022, 44, 4672–4680. [Google Scholar] [CrossRef] [PubMed]
- Testani, D.; McMorris, C.A.; Clark, C.A.; Sanguino, H.; Condliffe, E.G.; Noel, M.E.; Kopala Sibley, D.C.; Brunton, L.K. Investigating Physiological Symptoms Associated with Mental Health Symptoms in Youth with Cerebral Palsy: An Observational Study. Res. Dev. Disabil. 2024, 151, 104783. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, E.; Miller, A.R.; Lach, L.M. Topography of Behavior Problems among Children with Neurodevelopmental Conditions: Profile Differences and Overlaps. Child Care Health Dev. 2020, 46, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Horwood, L.; Li, P.; Mok, E.; Oskoui, M.; Shevell, M.; Constantin, E. Behavioral Difficulties, Sleep Problems, and Nighttime Pain in Children with Cerebral Palsy. Res. Dev. Disabil. 2019, 95, 103500. [Google Scholar] [CrossRef]
- Laporta-Hoyos, O.; Pannek, K.; Pagnozzi, A.M.; Whittingham, K.; Wotherspoon, J.; Benfer, K.; Fiori, S.; Ware, R.S.; Boyd, R.N. Cognitive, Academic, Executive and Psychological Functioning in Children with Spastic Motor Type Cerebral Palsy: Influence of Extent, Location, and Laterality of Brain Lesions. Eur. J. Paediatr. Neurol. 2022, 38, 33–46. [Google Scholar] [CrossRef]
- de Freitas Feldberg, S.C.; da Silva Gusmão Cardoso, T.; Santos, F.H.; Muszkat, M.; Bueno, O.F.A.; Berlim de Mello, C. Numerical Cognition in Children with Cerebral Palsy. Res. Dev. Disabil. 2021, 119, 104086. [Google Scholar] [CrossRef]
- Jarl, J.; Alriksson-Schmidt, A. School Outcomes of Adolescents with Cerebral Palsy in Sweden. Dev. Med. Child Neurol. 2021, 63, 429–435. [Google Scholar] [CrossRef]
- Micheletti, S.; Galli, J.; Vezzoli, M.; Scaglioni, V.; Agostini, S.; Calza, S.; Merabet, L.B.; Fazzi, E. Academic Skills in Children with Cerebral Palsy and Specific Learning Disorders. Dev. Med. Child Neurol. 2024, 66, 778–792. [Google Scholar] [CrossRef]
- Pereira, A.; Rosário, P.; Lopes, S.; Moreira, T.; Magalhães, P.; Núñez, J.C.; Vallejo, G.; Sampaio, A. Promoting School Engagement in Children with Cerebral Palsy: A Narrative Based Program. Int. J. Environ. Res. Public Health 2019, 16, 3634. [Google Scholar] [CrossRef]
- Wotherspoon, J.; Whittingham, K.; Sheffield, J.; Boyd, R.N. Randomised Controlled Trial of an Online Cognitive Training Program in School-Aged Children with Cerebral Palsy. Res. Dev. Disabil. 2024, 150, 104752. [Google Scholar] [CrossRef]
- Ahn, B.; Joung, Y.-S.; Kwon, J.-Y.; Lee, D.I.; Oh, S.; Kim, B.-U.; Cha, J.Y.; Kim, J.-H.; Lee, J.Y.; Shin, H.Y.; et al. Effects of Equine-Assisted Activities on Attention and Quality of Life in Children with Cerebral Palsy in a Randomized Trial: Examining the Comorbidity with Attention-Deficit/Hyperactivity Disorder. BMC Pediatr. 2021, 21, 135. [Google Scholar] [CrossRef] [PubMed]
- Alibakhshi, H.; Siminghalam, M.; Avaz, K.A.; Salmani, M.; Pahlevanian, A.; Motaharinezhad, F.; Kanani, Z. The Impact of Teaching Communication Skills to Mothers on Reducing Behavioral Problems in Children with Cerebral Palsy: A Quasi-Experimental Study. J. Rehabil. Sci. Res. 2023, 10, 222–227. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Chang, W.-P.; Liang, K.-J.; Chen, C.-L.; Chen, H.-Y.; Chen, S.-P.; Chan, P.-Y.S. The Effects of Neurofeedback Training for Children with Cerebral Palsy and Co-Occurring Attention Deficits: A Pilot Study. Child Care Health Dev. 2024, 50, e13231. [Google Scholar] [CrossRef] [PubMed]
- Mak, C.; Whittingham, K.; Cunnington, R.; Chatfield, M.; Boyd, R.N. Six-Month Follow-up of a Mindfulness Yoga Program, MiYoga, on Attention, Executive Function, Behaviour and Physical Outcomes in Cerebral Palsy. Disabil. Rehabil. 2022, 44, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Ödek, U.; Özcan, K.; Özyurt, G.; Akpinar, S. Psychological Benefits of Equine-Facilitated Activities for Children Diagnosed with Cerebral Palsy. Sport Mont. 2022, 20, 31–37. [Google Scholar] [CrossRef]
- Samijn, B.; Van den Broeck, C.; Plasschaert, F.; Pascal, A.; Deschepper, E.; Hoebeke, P.; Van Laecke, E. Incontinence Training in Children with Cerebral Palsy: A Prospective Controlled Trial. J. Pediatr. Urol. 2022, 18, e1–e447. [Google Scholar] [CrossRef]
- Shahriari, Y.; Ghasemzadeh, S.; Vakili, S. The Effectiveness of Child-Centred Play Therapy on Internalization and Extrapolation Behavioral Problems in Children with Cerebral Palsy. Iran. J. Psychiatry Clin. Psychol. 2019, 25, 236–249. [Google Scholar] [CrossRef]
- Whittingham, K.; Sheffield, J.; Mak, C.; Wright, A.; Boyd, R.N. Parenting Acceptance and Commitment Therapy: An RCT of an Online Course with Families of Children with CP. Behav. Res. Ther. 2022, 155, 104129. [Google Scholar] [CrossRef]
- Levy-Zaks, A.; Pollak, Y.; Ben-Pazi, H. Cerebral Palsy Risk Factors and Their Impact on Psychopathology. Neurol. Res. 2014, 36, 92–94. [Google Scholar] [CrossRef]
- McMorris, C.A.; Lake, J.; Dobranowski, K.; McGarry, C.; Lin, E.; Wilton, D.; Lunsky, Y.; Balogh, R. Psychiatric Disorders in Adults with Cerebral Palsy. Res. Dev. Disabil. 2021, 111, 103859. [Google Scholar] [CrossRef]
- Whitney, D.G.; Warschausky, S.A.; Ng, S.; Hurvitz, E.A.; Kamdar, N.S.; Peterson, M.D. Prevalence of Mental Health Disorders among Adults with Cerebral Palsy. Ann. Intern. Med. 2019, 171, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Weber, P.; Bolli, P.; Heimgartner, N.; Merlo, P.; Zehnder, T.; Kätterer, C. Behavioral and Emotional Problems in Children and Adults with Cerebral Palsy. Eur. J. Paediatr. Neurol. 2016, 20, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Ghasemi, H.; Abdoli, N.; Rahmani, A.; Shiri, M.H.; Hashemian, A.H.; Akbari, H.; Mohammadi, M. The Global Prevalence of ADHD in Children and Adolescents: A Systematic Review and Meta-Analysis. Ital. J. Pediatr. 2023, 49, 48. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Rasoulpoor, S.; Rasoulpoor, S.; Shohaimi, S.; Jafarpour, S.; Abdoli, N.; Khaledi-Paveh, B.; Mohammadi, M. The Global Prevalence of Autism Spectrum Disorder: A Comprehensive Systematic Review and Meta-Analysis. Ital. J. Pediatr. 2022, 48, 112. [Google Scholar] [CrossRef]
- Reid, S.M.; Meehan, E.M.; Arnup, S.J.; Reddihough, D.S. Intellectual Disability in Cerebral Palsy: A Population-Based Retrospective Study. Dev. Med. Child Neurol. 2018, 60, 687–694. [Google Scholar] [CrossRef]
- Türkoğlu, G.; Türkoğlu, S.; Çelık, C.; Uçan, H. Intelligence, Functioning, and Related Factors in Children with Cerebral Palsy. Arch. Neuropsychiatry 2017, 54, 33–37. [Google Scholar] [CrossRef]
- Stadskleiv, K. Cognitive Functioning in Children with Cerebral Palsy. Dev. Med. Child Neurol. 2020, 62, 283–289. [Google Scholar] [CrossRef]
- Brossard-Racine, M.; Hall, N.; Majnemer, A.; Shevell, M.I.; Law, M.; Poulin, C.; Rosenbaum, P. Behavioural Problems in School Age Children with Cerebral Palsy. Eur. J. Paediatr. Neurol. 2012, 16, 35–41. [Google Scholar] [CrossRef]
- Cobham, V.E.; Hickling, A.; Kimball, H.; Thomas, H.J.; Scott, J.G.; Middeldorp, C.M. Systematic Review: Anxiety in Children and Adolescents with Chronic Medical Conditions. J. Am. Acad. Child Adolesc. Psychiatry 2020, 5, 595–618. [Google Scholar] [CrossRef]
- Frampton, I.; Yude, C.; Goodman, R. The Prevalence and Correlates of Specific Learning Difficulties in a Representative Sample of Children with Hemiplegia. Br. J. Educ. Psychol. 1998, 68, 39–51. [Google Scholar] [CrossRef]
- Silberg, T.; Kapil, N.; Caven, I.; Levac, D.; Fehlings, D. Cognitive Behavioral Therapies for Individuals with Cerebral Palsy: A Scoping Review. Dev. Med. Child Neurol. 2023, 65, 1012–1028. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rausch, R.; Chahin, S.; Miller, C.; Dopheide, L.; Bovio, N.; Harris, A.; Patel, D. The Mental Health of Children with Cerebral Palsy: A Review of the Last Five Years of Research. J. Clin. Med. 2025, 14, 4364. https://doi.org/10.3390/jcm14124364
Rausch R, Chahin S, Miller C, Dopheide L, Bovio N, Harris A, Patel D. The Mental Health of Children with Cerebral Palsy: A Review of the Last Five Years of Research. Journal of Clinical Medicine. 2025; 14(12):4364. https://doi.org/10.3390/jcm14124364
Chicago/Turabian StyleRausch, Rebecca, Summer Chahin, Caroline Miller, Lindsey Dopheide, Nicholas Bovio, Ann Harris, and Dilip Patel. 2025. "The Mental Health of Children with Cerebral Palsy: A Review of the Last Five Years of Research" Journal of Clinical Medicine 14, no. 12: 4364. https://doi.org/10.3390/jcm14124364
APA StyleRausch, R., Chahin, S., Miller, C., Dopheide, L., Bovio, N., Harris, A., & Patel, D. (2025). The Mental Health of Children with Cerebral Palsy: A Review of the Last Five Years of Research. Journal of Clinical Medicine, 14(12), 4364. https://doi.org/10.3390/jcm14124364