
Femtosecond Laser-Assisted Donor and Recipient Preparation for Bowman Layer Transplantation


 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
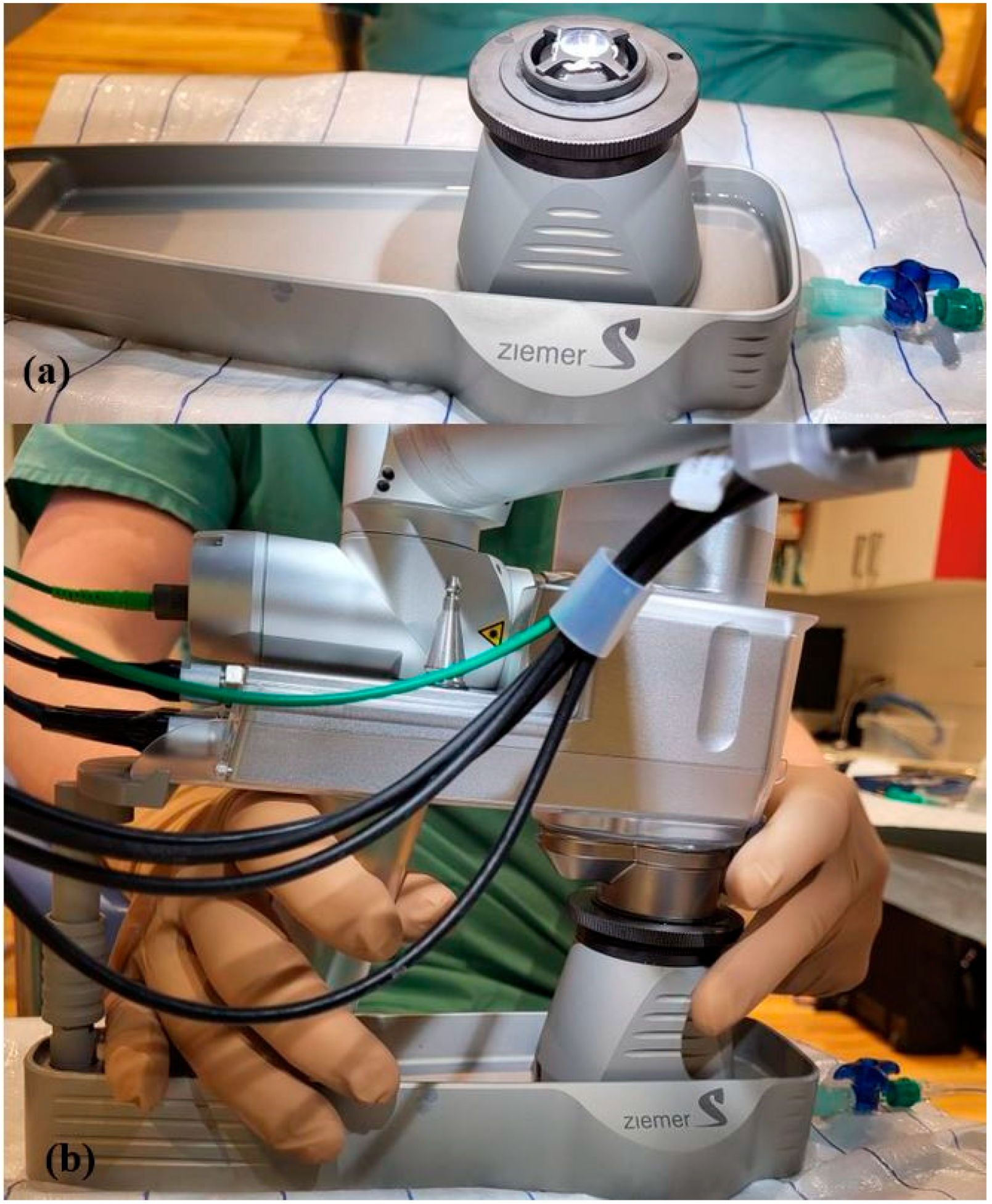
2.2. Donor Bowman Layer
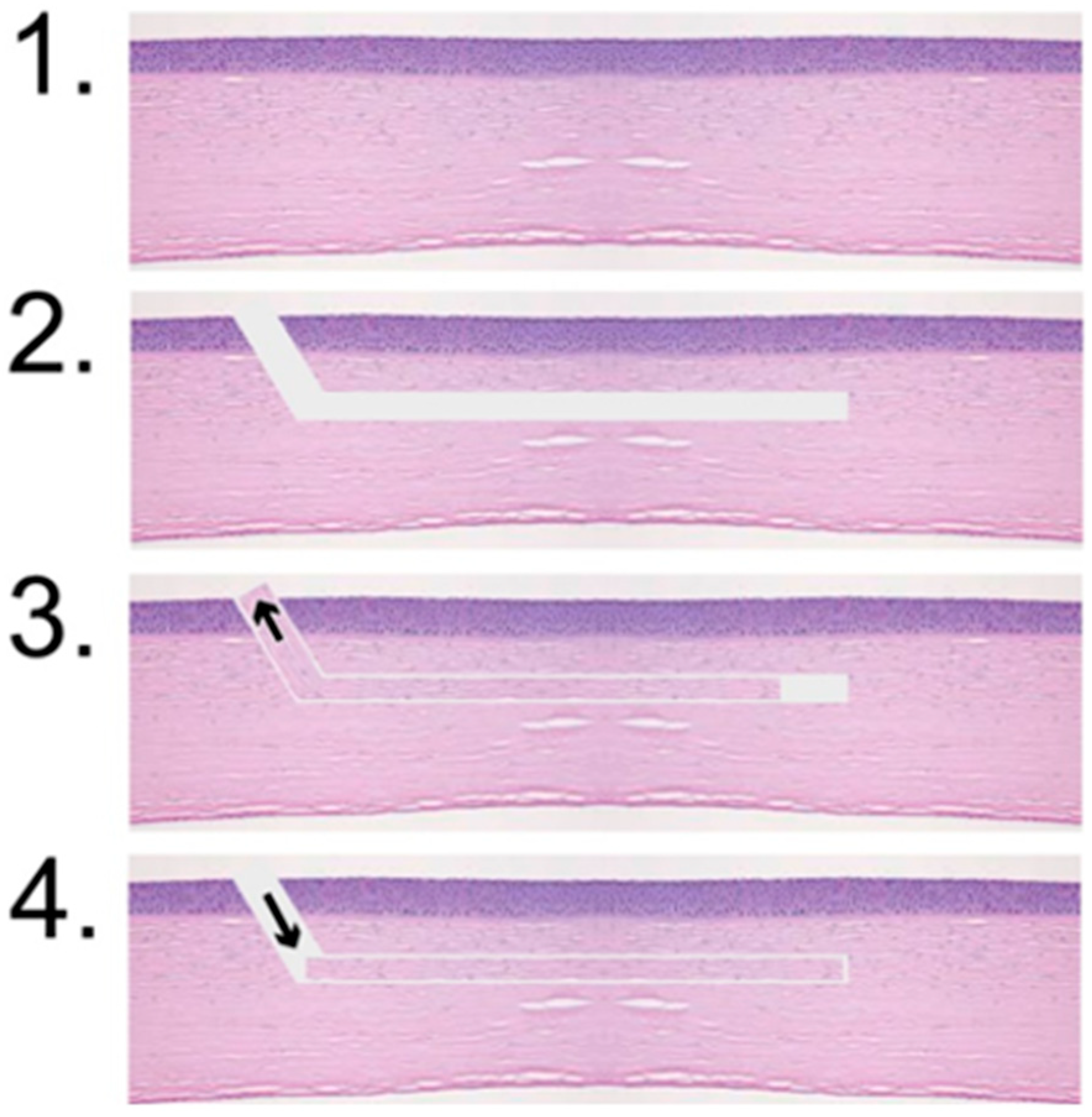
2.3. Recipient Pockets
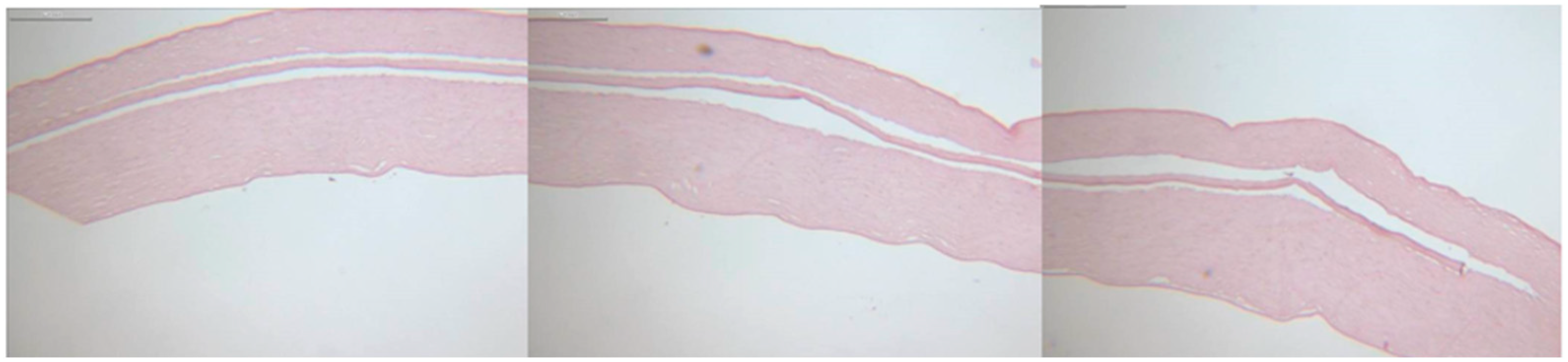
2.4. Histology
3. Results
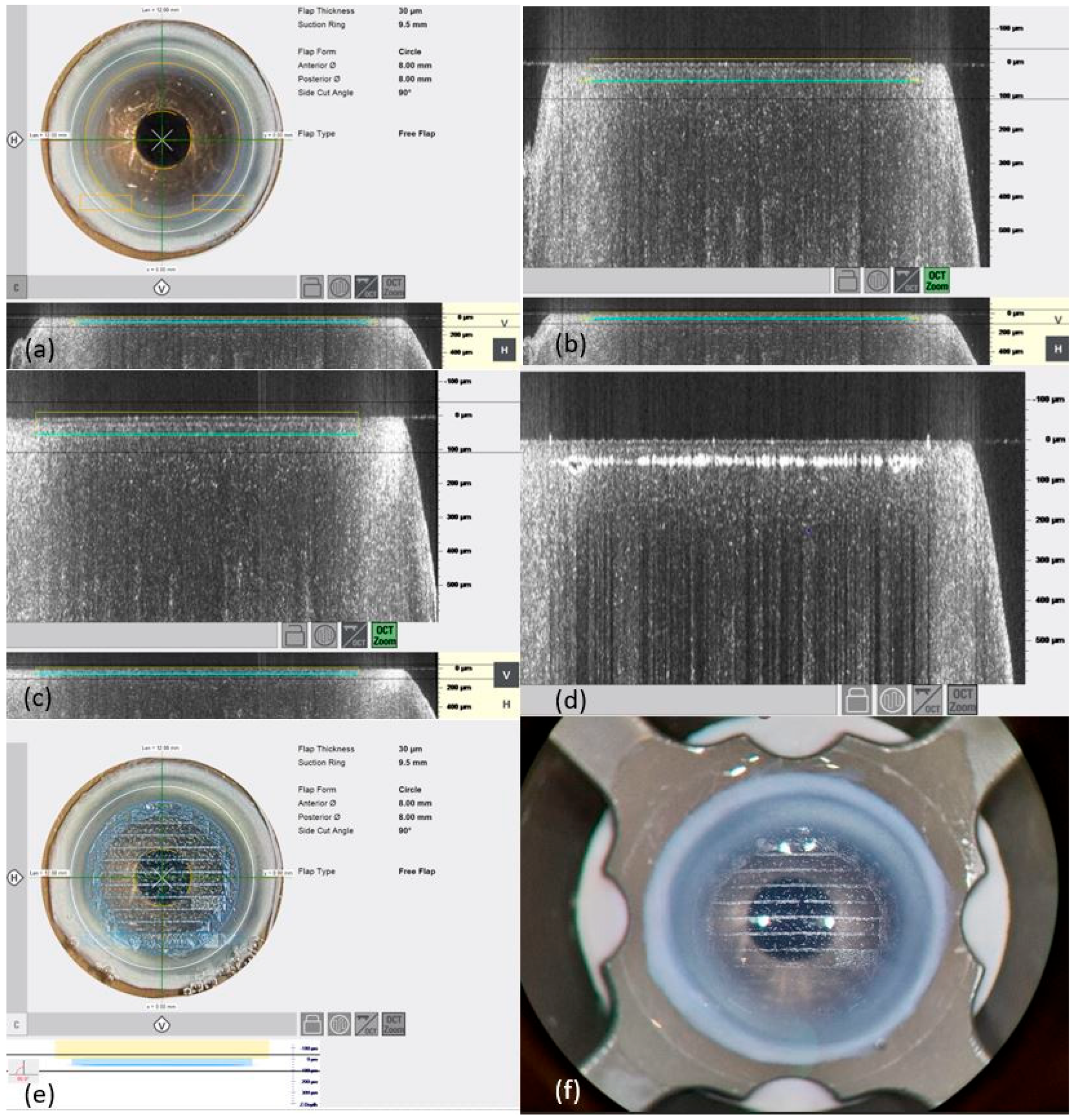
3.1. Preparation of Bowman Layers
3.2. Preparation of Recipient Pockets
3.3. Histology
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grünauer-Kloevekorn, C.; Duncker, G.I. Keratokonus: Epidemiologie, Risikofaktoren und Diagnostik. Klin. Monatsblatter Fur Augenheilkd. 2006, 223, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Jhanji, V.; Sharma, N.; Vajpayee, R.B. Management of keratoconus: Current scenario. Br. J. Ophthalmol. 2011, 95, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Lie, J.; Droutsas, K.; Ham, L.; Dapena, I.; Ververs, B.; Otten, H.; van der Wees, J.; Melles, G.R. Isolated Bowman layer transplantation to manage persistent subepithelial haze after excimer laser surface ablation. J. Cataract Refract. Surg. 2010, 36, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.S.; van Dijk, K.; Melles, G.R.J. Treatment options for advanced keratoconus: A review. Surv. Ophthalmol. 2015, 60, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Dapena, I.; Parker, J.S.; Melles, G.R. Potential benefits of modified corneal tissue grafts for keratoconus: Bowman layer ‘inlay’ and ‘onlay’ transplantation, and allogenic tissue ring segments. Curr. Opin. Ophthalmol. 2020, 31, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Luceri, S.; Parker, J.; Dapena, I.; Baydoun, L.; Oellerich, S.; Van Dijk, K.; Melles, G.R. Corneal Densitometry and Higher Order Aberrations After Bowman Layer Transplantation: 1-Year Results. Cornea 2016, 35, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.S.; Huls, F.; Cooper, E.; Graves, P.; Groeneveld-van Beek, E.A.; Lie, J.; Melles, G.R. Technical feasibility of isolated Bowman layer graft preparation by femtosecond laser: A pilot study. Eur. J. Ophthalmol. 2017, 27, 675–677. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Dubey, A.; Prakash, G.; Vajpayee, R.B. Bowman’s layer transplantation: Evidence to date. Clin. Ophthalmol. 2018, 12, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Soong, H.K.; Malta, J.B. Femtosecond lasers in ophthalmology. Am. J. Ophthalmol. 2009, 147, 189–197.e2. [Google Scholar] [CrossRef] [PubMed]
- Schärer, L. Histologische Techniken. In Histopathologie der Haut; Cerroni, L., Garbe, C., Metze, D., Kutzner, H., Kerl, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 3–13. [Google Scholar]
- van Dijk, K.; Parker, J.; Tong, C.M.; Ham, L.; Lie, J.T.; Groeneveld-van Beek, E.A.; Melles, G.R. Midstromal isolated Bowman layer graft for reduction of advanced keratoconus: A technique to postpone penetrating or deep anterior lamellar keratoplasty. JAMA Ophthalmol. 2014, 132, 495–501. [Google Scholar] [CrossRef] [PubMed]
- García de Oteyza, G.; González Dibildox, L.A.; Vázquez-Romo, K.A.; Vázquez, A.T.; Alquisiras, J.H.D.; Martínez-Báez, B.E.; García-Albisua, A.M.; Ramírez, M.; Hernandez-Quintela, E. Bowman layer transplantation using a femtosecond laser. J. Cataract Refract. Surg. 2019, 45, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.S.; Dockery, P.W.; Melles, G.R.J. Bowman Layer Transplantation-A Review. Asia-Pac. J. Ophthalmol. 2020, 9, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Steven, P.; Hos, D.; Heindl, L.M.; Bock, F.; Cursiefen, C. Immunreaktionen nach DMEK, DSAEK und DALK. Klin. Monatsblatter Fur Augenheilkd. 2013, 230, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, S.; Kumari, M.; Bhatnagar, N. Advancements in keratoplasty: Exploring newer techniques and imaging modalities for enhanced surgical outcomes. Saudi J. Ophthalmol. 2024. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Thickness of Bowman layer (µm) | 30 |
| Diameter of suction ring (mm) | 9.5 |
| Anterior diamter (mm) | 8 |
| Posterior diamter (mm) | 8 |
| Angle of side cut (°) | 90 |
| Velocity of side cut (mm/s) | 40 |
| Energy of side cut (%) | 80 |
| Velocity of stromal cut (mm/s) | 14 |
| Energy of stromal cut (%) | 75 |
| Posterior surface (µm) | 5 |
| Resection depth (µm) | 150 |
| Incision diamter (mm) | 9.5 |
| Width of tunnel (mm) | 5 |
| Pocket diameter (mm) | 9 |
| Angle of side cut (°) | 30 |
| Input position (°) | sup |
| Energy of incision cut (%) | 130 |
| Velocity of incision cut (%) | 40 |
| Energy of stromal cut (%) | 80 |
| Velocity of stromal cut (mm/s) | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlosser, R.; Rickmann, A.; Szurman, P.; Wahl, S.; Seitz, B.; Wakili, P.; Müller, L.J.; Roberts, P.K.; Boden, K.T. Femtosecond Laser-Assisted Donor and Recipient Preparation for Bowman Layer Transplantation. J. Clin. Med. 2025, 14, 4362. https://doi.org/10.3390/jcm14124362
Schlosser R, Rickmann A, Szurman P, Wahl S, Seitz B, Wakili P, Müller LJ, Roberts PK, Boden KT. Femtosecond Laser-Assisted Donor and Recipient Preparation for Bowman Layer Transplantation. Journal of Clinical Medicine. 2025; 14(12):4362. https://doi.org/10.3390/jcm14124362
Chicago/Turabian StyleSchlosser, Rosemarie, Annekatrin Rickmann, Peter Szurman, Silke Wahl, Berthold Seitz, Philip Wakili, Lisa Julia Müller, Philipp Ken Roberts, and Karl Thomas Boden. 2025. "Femtosecond Laser-Assisted Donor and Recipient Preparation for Bowman Layer Transplantation" Journal of Clinical Medicine 14, no. 12: 4362. https://doi.org/10.3390/jcm14124362
APA StyleSchlosser, R., Rickmann, A., Szurman, P., Wahl, S., Seitz, B., Wakili, P., Müller, L. J., Roberts, P. K., & Boden, K. T. (2025). Femtosecond Laser-Assisted Donor and Recipient Preparation for Bowman Layer Transplantation. Journal of Clinical Medicine, 14(12), 4362. https://doi.org/10.3390/jcm14124362