
Cardio-Oncology and Multi-Imaging Modalities
 , , , ,
, , , ,
Abstract
1. Introduction
2. Cardiotoxicity and Cardiovascular Implications
2.1. Cancer Therapy-Related Cardiac Dysfunction and Heart Failure
2.2. Myocarditis
2.3. Conduction Disturbances
2.4. Autonomic Dysfunction
2.5. Hypertension
2.6. Vascular Toxicity
3. Cardiac Imaging Techniques in Cardio-Oncology
3.1. Echocardiography
3.2. Cardiac Magnetic Resonance
3.3. Cardiac/Coronary Computed Tomography
3.4. Nuclear Imaging
3.5. Cardiac Masses
4. Imaging for Oncological Therapies at Baseline and Follow-Up
4.1. Anthracyclines
4.2. HER2-Targeted Monoclonal Antibodies
4.3. Proteasome Inhibitors
4.4. Combination Therapy of BRAF and MEK Inhibitors
4.5. Select VEGF Inhibitors
4.6. Tyrosine Kinase Inhibitors
4.7. Immune Checkpoint Inhibitors (ICI)
4.8. CAR T Cell Therapy
4.9. Alkylating Agents
5. Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Computed tomography | (CT) |
| Cardiac magnetic resonance | (CMR) |
| Cancer treatment-related cardiac dysfunction | (CTRCD) |
| Human epidermal growth factor receptor 2 | (HER2) |
| Left-ventricular ejection fraction | (LVEF) |
| Global longitudinal strain | (GLS) |
| Immune checkpoint inhibitor | (ICI) |
| Chimeric antigen receptor T cell | (CAR-T) |
| Vascular endothelial growth factor | (VEGF) |
| Coronary artery disease | (CAD) |
| Transthoracic echocardiography | (TTE) |
| Cardiac/coronary computed tomography | (CCTA) |
| Multi-gated acquisition | (MUGA) |
| Transesophageal echocardiography | (TEE) |
| Right-ventricular ejection fraction | (RVEF) |
| Left-ventricular | (LV) |
| Two-dimensional | (2D) |
| Three-dimensional | (3D) |
| Late gadolinium enhancement | (LGE) |
| Coronary computed tomography angiography | (CCTA) |
| Coronary artery calcification | (CAC) |
| Fractional flow reserve | (FFR) |
| Single-photon-emission computed tomography | (SPECT) |
| Positron emission tomography | (PET) |
| Target kinase inhibitors | (TKI) |
| Cytotoxic T-lymphocyte-associated antigen-4 | (CTLA-4) |
| Programmed cell death-1 | (PD-1) |
| Major adverse cardiovascular events | (MACE) |
| Cytokine release syndrome | (CRS) |
References
- Lenneman, C.G.; Sawyer, D.B. Cardio-Oncology: An Update on Cardiotoxicity of Cancer-Related Treatment. Circ. Res. 2016, 118, 1008–1020. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J.; Lenihan, D.; Armenian, S.; Barac, A.; Blaes, A.; Cardinale, D.; Carver, J.; Dent, S.; Ky, B.; Lyon, A.R.; et al. Defining Cardiovascular Toxicities of Cancer Therapies: An International Cardio-Oncology Society (IC-OS) Consensus Statement. Eur. Heart J. 2022, 43, 280–299. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J.; Lerman, A.; Sandhu, N.P.; Villarraga, H.R.; Mulvagh, S.L.; Kohli, M. Evaluation and Management of Patients with Heart Disease and Cancer: Cardio-Oncology. Mayo Clin. Proc. 2014, 89, 1287–1306. [Google Scholar] [CrossRef] [PubMed]
- Baldassarre, L.A.; Ganatra, S.; Lopez-Mattei, J.; Yang, E.H.; Zaha, V.G.; Wong, T.C.; Ayoub, C.; DeCara, J.M.; Dent, S.; Deswal, A.; et al. Advances in Multimodality Imaging in Cardio-Oncology: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 80, 1560–1578. [Google Scholar] [CrossRef]
- Camilli, M.; Cipolla, C.M.; Dent, S.; Minotti, G.; Cardinale, D.M. Anthracycline Cardiotoxicity in Adult Cancer Patients: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2024, 6, 655–677. [Google Scholar] [CrossRef]
- Dempsey, N.; Rosenthal, A.; Dabas, N.; Kropotova, Y.; Lippman, M.; Bishopric, N.H. Trastuzumab-Induced Cardiotoxicity: A Review of Clinical Risk Factors, Pharmacologic Prevention, and Cardiotoxicity of Other HER2-Directed Therapies. Breast Cancer Res. Treat. 2021, 188, 21–36. [Google Scholar] [CrossRef]
- Wu, Q.; Bai, B.; Tian, C.; Li, D.; Yu, H.; Song, B.; Li, B.; Chu, X. The Molecular Mechanisms of Cardiotoxicity Induced by HER2, VEGF, and Tyrosine Kinase Inhibitors: An Updated Review. Cardiovasc. Drugs Ther. 2022, 36, 511–524. [Google Scholar] [CrossRef]
- Lyon, A.R.; Lopez-Fernandez, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on Cardio-Oncology Developed in Collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Zhang, L.; Awadalla, M.; Mahmood, S.S.; Nohria, A.; Hassan, M.Z.O.; Thuny, F.; Zlotoff, D.A.; Murphy, S.P.; Stone, J.R.; Golden, D.L.A.; et al. Cardiovascular Magnetic Resonance in Immune Checkpoint Inhibitor-Associated Myocarditis. Eur. Heart J. 2020, 41, 1733–1743. [Google Scholar] [CrossRef]
- Frascaro, F.; Bianchi, N.; Sanguettoli, F.; Marchini, F.; Meossi, S.; Zanarelli, L.; Tonet, E.; Serenelli, M.; Guardigli, G.; Campo, G.; et al. Immune Checkpoint Inhibitors-Associated Myocarditis: Diagnosis, Treatment and Current Status on Rechallenge. J. Clin. Med. 2023, 12, 7737. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Abu-Sbeih, H.; Ascierto, P.A.; Brufsky, J.; Cappelli, L.C.; Cortazar, F.B.; Gerber, D.E.; Hamad, L.; Hansen, E.; Johnson, D.B.; et al. Society for Immunotherapy of Cancer (SITC) Clinical Practice Guideline on Immune Checkpoint Inhibitor-Related Adverse Events. J. Immunother. Cancer 2021, 9, e002435. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Olenchock, B.A.; Salem, J.E.; Wiviott, S.D.; Ederhy, S.; Cohen, A.; Stewart, G.C.; Choueiri, T.K.; Di Carli, M.; Allenbach, Y.; et al. Myocarditis in the Setting of Cancer Therapeutics: Proposed Case Definitions for Emerging Clinical Syndromes in Cardio-Oncology. Circulation 2019, 140, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J. Adverse Cardiac Effects of Cancer Therapies: Cardiotoxicity and Arrhythmia. Nat. Rev. Cardiol. 2020, 17, 474–502. [Google Scholar] [CrossRef]
- Fradley, M.G.; Beckie, T.M.; Brown, S.A.; Cheng, R.K.; Dent, S.F.; Nohria, A.; Patton, K.K.; Singh, J.P.; Olshansky, B. Recognition, Prevention, and Management of Arrhythmias and Autonomic Disorders in Cardio-Oncology: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e41–e55. [Google Scholar] [CrossRef]
- Touyz, R.M.; Herrmann, J. Cardiotoxicity with Vascular Endothelial Growth Factor Inhibitor Therapy. NPJ Precis. Oncol. 2018, 2, 13. [Google Scholar] [CrossRef]
- Li, W.; Cornell, R.F.; Lenihan, D.; Slosky, D.; Jagasia, M.; Piazza, G.; Moslehi, J. Cardiovascular Complications of Novel Multiple Myeloma Treatments. Circulation 2016, 133, 908–912. [Google Scholar] [CrossRef]
- More, L.A.; Lane, S.; Asnani, A. 5-FU Cardiotoxicity: Vasospasm, Myocarditis, and Sudden Death. Curr. Cardiol. Rep. 2021, 23, 17. [Google Scholar] [CrossRef]
- Ell, P.; Martin, J.M.; Cehic, D.A.; Ngo, D.T.M.; Sverdlov, A.L. Cardiotoxicity of Radiation Therapy: Mechanisms, Management, and Mitigation. Curr. Treat. Options Oncol. 2021, 22, 70. [Google Scholar] [CrossRef]
- Giza, D.E.; Boccalandro, F.; Lopez-Mattei, J.; Iliescu, G.; Karimzad, K.; Kim, P.; Iliescu, C. Ischemic Heart Disease: Special Considerations in Cardio-Oncology. Curr. Treat. Options Cardiovasc. Med. 2017, 19, 37. [Google Scholar] [CrossRef]
- Dobson, R.; Ghosh, A.K.; Ky, B.; Marwick, T.; Stout, M.; Harkness, A.; Steeds, R.; Robinson, S.; Oxborough, D.; Adlam, D.; et al. BSE and BCOS Guideline for Transthoracic Echocardiographic Assessment of Adult Cancer Patients Receiving Anthracyclines and/or Trastuzumab. JACC CardioOncol. 2021, 3, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Sartorio, A.; Cristin, L.; Pont, C.D.; Farzaneh-Far, A.; Romano, S. Global Longitudinal Strain as an Early Marker of Cardiac Damage after Cardiotoxic Medications, a State of the Art Review. Prog. Cardiovasc. Dis. 2025, 89, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Poulin, F.; Lim, K.D.; Plana, J.C.; Woo, A.; Marwick, T.H. Use of Myocardial Strain Imaging by Echocardiography for the Early Detection of Cardiotoxicity in Patients during and after Cancer Chemotherapy: A Systematic Review. J. Am. Coll. Cardiol. 2014, 63, 2751–2768. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.K.; Kokkinidis, D.G.; Kampaktsis, P.N.; Amir, E.A.; Marwick, T.H.; Gupta, D.; Thavendiranathan, P. Assessment of Prognostic Value of Left Ventricular Global Longitudinal Strain for Early Prediction of Chemotherapy-Induced Cardiotoxicity: A Systematic Review and Meta-Analysis. JAMA Cardiol. 2019, 4, 1007–1018. [Google Scholar] [CrossRef]
- Liu, J.E.; Barac, A.; Thavendiranathan, P.; Scherrer-Crosbie, M. Strain Imaging in Cardio-Oncology. JACC CardioOncol. 2020, 2, 677–689. [Google Scholar] [CrossRef]
- Nazir, M.S.; Okafor, J.; Murphy, T.; Andres, M.S.; Ramalingham, S.; Rosen, S.D.; Chiribiri, A.; Plein, S.; Prasad, S.; Mohiaddin, R.; et al. Echocardiography versus Cardiac MRI for Measurement of Left Ventricular Ejection Fraction in Individuals with Cancer and Suspected Cardiotoxicity. Radiol. Cardiothorac. Imaging 2024, 6, e230048. [Google Scholar] [CrossRef]
- Lorenzo-Esteller, L.; Ramos-Polo, R.; Pons Riverola, A.; Morillas, H.; Berdejo, J.; Pernas, S.; Pomares, H.; Asiain, L.; Garay, A.; Martinez Perez, E.; et al. Pericardial Disease in Patients with Cancer: Clinical Insights on Diagnosis and Treatment. Cancers 2024, 16, 3466. [Google Scholar] [CrossRef]
- Yalta, K.; Yilmaztepe, M.; Zorkun, C. Left Ventricular Dysfunction in the Setting of Takotsubo Cardiomyopathy: A Review of Clinical Patterns and Practical Implications. Card. Fail. Rev. 2018, 4, 14–20. [Google Scholar] [CrossRef]
- Addison, D.; Neilan, T.G.; Barac, A.; Scherrer-Crosbie, M.; Okwuosa, T.M.; Plana, J.C.; Reding, K.W.; Taqueti, V.R.; Yang, E.H.; Zaha, V.G.; et al. Cardiovascular Imaging in Contemporary Cardio-Oncology: A Scientific Statement from the American Heart Association. Circulation 2023, 148, 1271–1286. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Zhang, L.; Zafar, A.; Drobni, Z.D.; Mahmood, S.S.; Cabral, M.; Awadalla, M.; Nohria, A.; Zlotoff, D.A.; Thuny, F.; et al. Myocardial T1 and T2 Mapping by Magnetic Resonance in Patients with Immune Checkpoint Inhibitor-Associated Myocarditis. J. Am. Coll. Cardiol. 2021, 77, 1503–1516. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.K.M.; Jellis, C.L.; Cremer, P.C.; Bolen, M.A.; Flamm, S.D.; Klein, A.L. Cardiac Magnetic Resonance Imaging Techniques and Applications for Pericardial Diseases. Circ. Cardiovasc. Imaging 2022, 15, e014283. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Mattei, J.C.; Yang, E.H.; Ferencik, M.; Baldassarre, L.A.; Dent, S.; Budoff, M.J. Cardiac Computed Tomography in Cardio-Oncology. JACC CardioOncol. 2021, 3, 635–649. [Google Scholar] [CrossRef] [PubMed]
- Erthal, F.; Premaratne, M.; Yam, Y.; Chen, L.; Lamba, J.; Keenan, M.; Haddad, T.; Pharasi, K.; Anand, S.; Beanlands, R.S.; et al. Appropriate Use Criteria for Cardiac Computed Tomography: Does Computed Tomography Have Incremental Value in All Appropriate Use Criteria Categories? J. Thorac. Imaging 2018, 33, 132–137. [Google Scholar] [CrossRef]
- Milazzo, V.; Cosentino, N.; Campodonico, J.; Lucci, C.; Cardinale, D.; Cipolla, C.M.; Marenzi, G. Characteristics, Management, and Outcomes of Acute Coronary Syndrome Patients with Cancer. J. Clin. Med. 2020, 9, 3642. [Google Scholar] [CrossRef]
- Driessen, R.S.; Danad, I.; Stuijfzand, W.J.; Raijmakers, P.G.; Schumacher, S.P.; Van Diemen, P.A.; Leipsic, J.A.; Knuuti, J.; Underwood, S.R.; Van De Ven, P.M.; et al. Comparison of Coronary Computed Tomography Angiography, Fractional Flow Reserve, and Perfusion Imaging for Ischemia Diagnosis. J. Am. Coll. Cardiol. 2019, 73, 161–173. [Google Scholar] [CrossRef]
- Tyebally, S.; Chen, D.; Bhattacharyya, S.; Mughrabi, A.; Hussain, Z.; Manisty, C.; Westwood, M.; Ghosh, A.K.; Guha, A. Cardiac Tumors. JACC CardioOncol. 2020, 2, 293–311. [Google Scholar] [CrossRef]
- Angeli, F.; Bodega, F.; Bergamaschi, L.; Armillotta, M.; Amicone, S.; Canton, L.; Fedele, D.; Suma, N.; Cavallo, D.; Foà, A.; et al. Multimodality Imaging in the Diagnostic Work-Up of Patients with Cardiac Masses. JACC CardioOncol. 2024, 6, 847–862. [Google Scholar] [CrossRef]
- Zhang, K.W.; Finkelman, B.S.; Gulati, G.; Narayan, H.K.; Upshaw, J.; Narayan, V.; Plappert, T.; Englefield, V.; Smith, A.M.; Zhang, C.; et al. Abnormalities in 3-Dimensional Left Ventricular Mechanics with Anthracycline Chemotherapy Are Associated with Systolic and Diastolic Dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1059–1068. [Google Scholar] [CrossRef]
- Camilli, M.; Ferdinandy, P.; Salvatorelli, E.; Menna, P.; Minotti, G. Anthracyclines, Diastolic Dysfunction and the Road to Heart Failure in Cancer Survivors: An Untold Story. Prog. Cardiovasc. Dis. 2024, 86, 38–47. [Google Scholar] [CrossRef]
- Sawyer, D.B.; Zuppinger, C.; Miller, T.A.; Eppenberger, H.M.; Suter, T.M. Modulation of Anthracycline-Induced Myofibrillar Disarray in Rat Ventricular Myocytes by Neuregulin-1beta and Anti-erbB2: Potential Mechanism for Trastuzumab-Induced Cardiotoxicity. Circulation 2002, 105, 1551–1554. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulos, G.; Makris, N.; Laina, A.; Theodorakakou, F.; Briasoulis, A.; Trougakos, I.P.; Dimopoulos, M.A.; Kastritis, E.; Stamatelopoulos, K. Cardiovascular Toxicity of Proteasome Inhibitors: Underlying Mechanisms and Management Strategies: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2023, 5, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Senechal, I.; Andres, M.S.; Tong, J.; Ramalingam, S.; Nazir, M.S.; Rosen, S.D.; Young, K.; Idaikkadar, P.; Larkin, J.; Lyon, A.R. Risk Stratification, Screening and Treatment of BRAF/MEK Inhibitors-Associated Cardiotoxicity. Curr. Oncol. Rep. 2024, 26, 1431–1441. [Google Scholar] [CrossRef] [PubMed]
- Mincu, R.I.; Mahabadi, A.A.; Michel, L.; Mrotzek, S.M.; Schadendorf, D.; Rassaf, T.; Totzeck, M. Cardiovascular Adverse Events Associated with BRAF and MEK Inhibitors: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2019, 2, e198890. [Google Scholar] [CrossRef]
- Chu, T.F.; Rupnick, M.A.; Kerkela, R.; Dallabrida, S.M.; Zurakowski, D.; Nguyen, L.; Woulfe, K.; Pravda, E.; Cassiola, F.; Desai, J.; et al. Cardiotoxicity Associated with Tyrosine Kinase Inhibitor Sunitinib. Lancet 2007, 370, 2011–2019. [Google Scholar] [CrossRef]
- Santoni, M.; Guerra, F.; Conti, A.; Lucarelli, A.; Rinaldi, S.; Belvederesi, L.; Capucci, A.; Berardi, R. Incidence and Risk of Cardiotoxicity in Cancer Patients Treated with Targeted Therapies. Cancer Treat Rev 2017, 59, 123–131. [Google Scholar] [CrossRef]
- Webster, R.M. The Immune Checkpoint Inhibitors: Where Are We Now? Nat Rev Drug Discov 2014, 13, 883–884. [Google Scholar] [CrossRef]
- Sterner, R.C.; Sterner, R.M. CAR-T Cell Therapy: Current Limitations and Potential Strategies. Blood Cancer J. 2021, 11, 69. [Google Scholar] [CrossRef]
- Lefebvre, B.; Kang, Y.; Smith, A.M.; Frey, N.V.; Carver, J.R.; Scherrer-Crosbie, M. Cardiovascular Effects of CAR T Cell Therapy: A Retrospective Study. JACC CardioOncol. 2020, 2, 193–203. [Google Scholar] [CrossRef]
- Bayraktar, U.D.; Bashir, Q.; Qazilbash, M.; Champlin, R.E.; Ciurea, S.O. Fifty Years of Melphalan Use in Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2013, 19, 344–356. [Google Scholar] [CrossRef]
- Feliz, V.; Saiyad, S.; Ramarao, S.M.; Khan, H.; Leonelli, F.; Guglin, M. Melphalan-Induced Supraventricular Tachycardia: Incidence and Risk Factors. Clin. Cardiol. 2011, 34, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Dhesi, S.; Chu, M.P.; Blevins, G.; Paterson, I.; Larratt, L.; Oudit, G.Y.; Kim, D.H. Cyclophosphamide-Induced Cardiomyopathy: A Case Report, Review, and Recommendations for Management. J. Investig. Med. High Impact Case Rep. 2013, 1, 2324709613480346. [Google Scholar] [CrossRef] [PubMed]
- Kamphuis, J.A.M.; Linschoten, M.; Cramer, M.J.; Gort, E.H.; van Rhenen, A.; Asselbergs, F.W.; Doevendans, P.A.; Teske, A.J. Cancer Therapy-Related Cardiac Dysfunction of Nonanthracycline Chemotherapeutics: What Is the Evidence? JACC CardioOncol. 2019, 1, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Gongora, C.A. Are Sodium-Glucose Cotransporter-2 Inhibitors the Cherry on Top of Cardio-Oncology Care? Cardiovasc. Drugs Ther. 2024, 1–8. [Google Scholar] [CrossRef]
- Gongora, C.A.; Drobni, Z.D.; Quinaglia Araujo Costa Silva, T.; Zafar, A.; Gong, J.; Zlotoff, D.A.; Gilman, H.K.; Hartmann, S.E.; Sama, S.; Nikolaidou, S.; et al. Sodium-Glucose Co-Transporter-2 Inhibitors and Cardiac Outcomes Among Patients Treated with Anthracyclines. J. Am. Coll. Cardiol. Heart Fail. 2022, 10, 559–567. [Google Scholar] [CrossRef]
- Maamari, D.J.; Biddinger, K.J.; Jurgens, S.J.; Rämö, J.T.; Zheng, A.; Hayes, D.; Gongora, C.A.; Choi, S.H.; Arany, Z.; Thavendiranathan, P.; et al. Polygenic Susceptibility to Dilated Cardiomyopathy Underlies Peripartum, Alcohol-Induced, and Cancer Therapy-Related Cardiomyopathies. medRxiv 2025. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Therapeutic | Cardiotoxicity | Baseline and Follow-Up |
|---|---|---|
| Anthracyclines | Heart failure *, cardiomyopathy, arrhythmias | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: Repeat TTE when cumulative dose >250 mg/m2 doxorubicin-equivalence and after every 50 mg/m2. Then, serial imaging from 1-5 years after therapy. |
| HER2-targeted monoclonal antibodies | Heart failure *, cardiomyopathy | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: Repeat TTE every 3 months |
| Proteasome inhibitors | Heart failure *, ischemic heart disease, dysrhythmias | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: Repeat if symptomatic. For carfilzomib, repeat TTE every 3 cycles |
| Combination therapy with BRAF + MEK inhibitors | Hypertension *, heart failure, QT prolongation, pulmonary embolus | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: Repeat TTE one month after initiation of treatment, then every 2-4 months |
| VEGF inhibitors | Heart failure *, ischemic heart disease, hypertension | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: Reassessment of LVEF after cycle 1 and cycle 3. Repeat if symptomatic |
| Tyrosine kinase inhibitors | Heart failure *, atrial fibrillation, ventricular arrhythmias, or QT prolongation | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: 1) Osimertinib, repeat TTE every 3 months. 2) Ibrutinib, repeat only if symptomatic |
| Immune checkpoint inhibitors | Arrhythmias *, myocarditis, pericarditis | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: Only if symptomatic |
| CAR T-cell therapy | Heart failure *, tachyarrhythmias, cardiomyopathy | Baseline: TTE with 2D, 3D, GLS, diastolic function Follow-Up: Repeat TTE if there is CRS grade 2 or higher, or if symptomatic |
| Imaging Modality | Sequence | Strengths | Limitations |
|---|---|---|---|
| Echocardiography (TTE, TEE) | 2D, 3D volumetric assessment Diastolic function GLS Valvular assessment Hemodynamic profiles (i.e., pulmonary hypertension) |
|
|
| Cardiac MRI | Cine sequences, LV mass and volume measurements Valvular assessment Multiparametric tissue characterization with T1, T2, ECV Strain techniques and stress LGE CMR available |
|
|
| Cardiac CT | Contrast perfusion for coronary CTA FFR evaluation Non-contrast CT sequences for calcium (coronary calcium) evaluation |
|
|
| Nuclear | MUGA Stress SPECT or PET, Technetium pyrophosphate scan |
|
|
| Imaging Modality | Imaging Illustrations | Description |
|---|---|---|
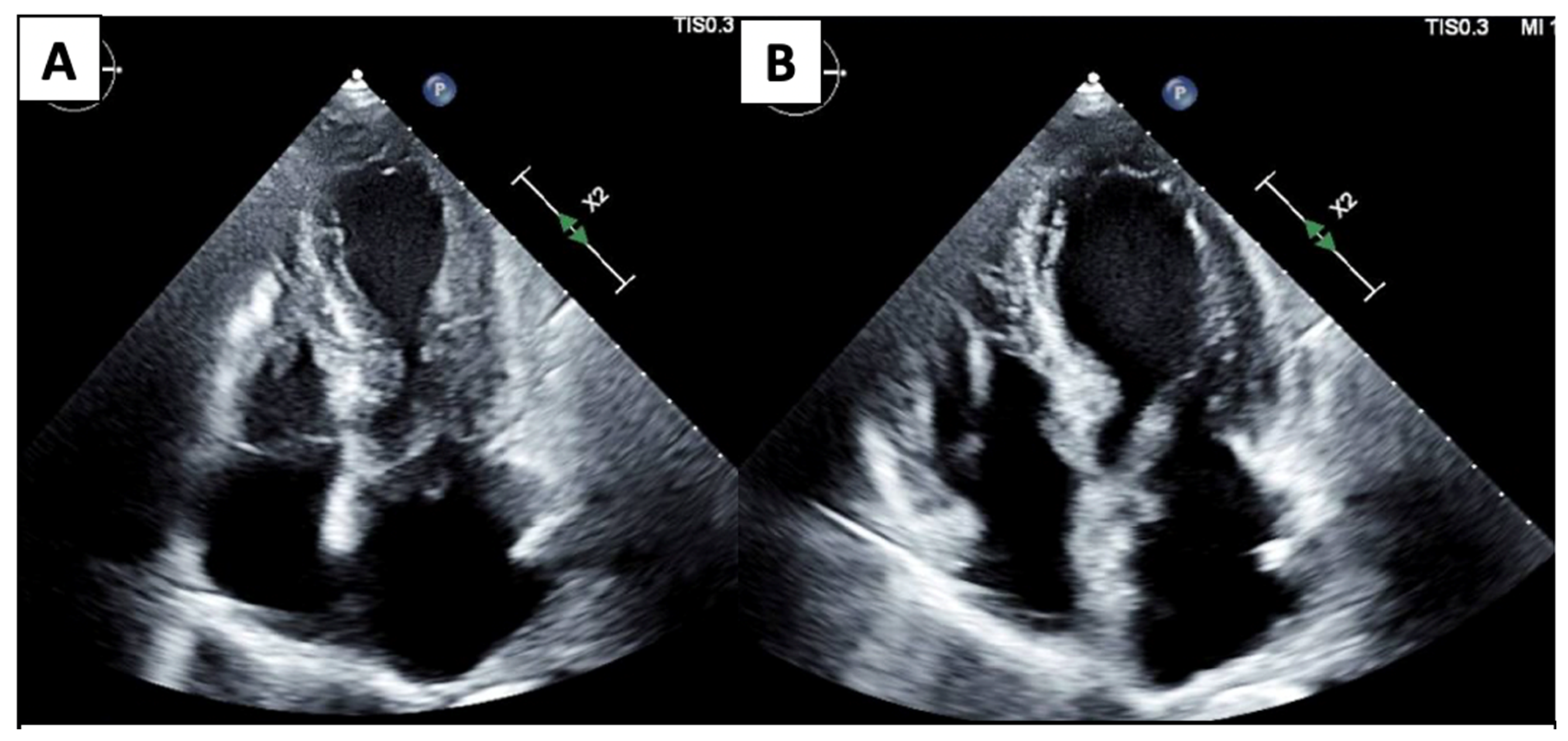
| Echocardiography |  | Mild left-ventricular dilation and systolic dysfunction |
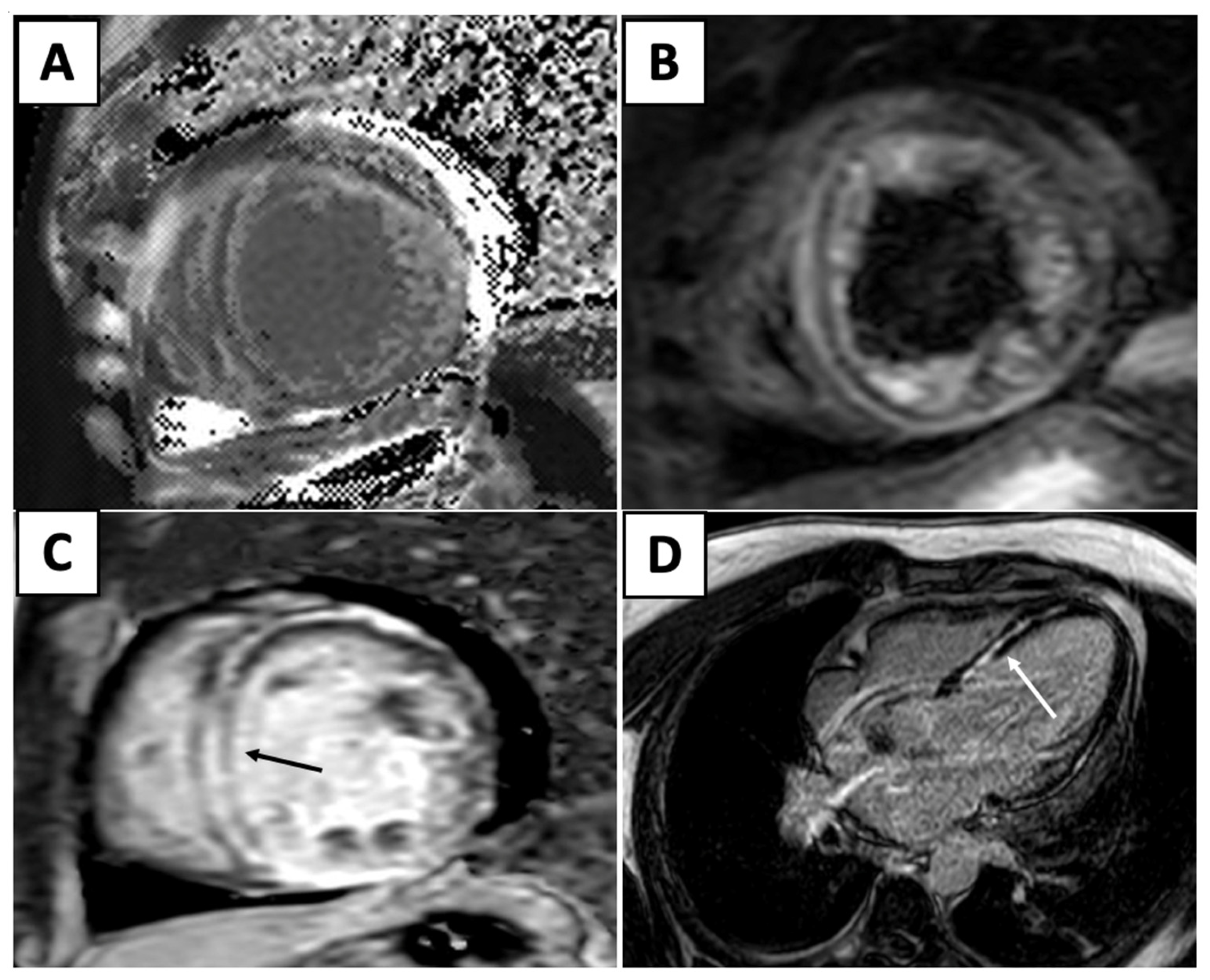
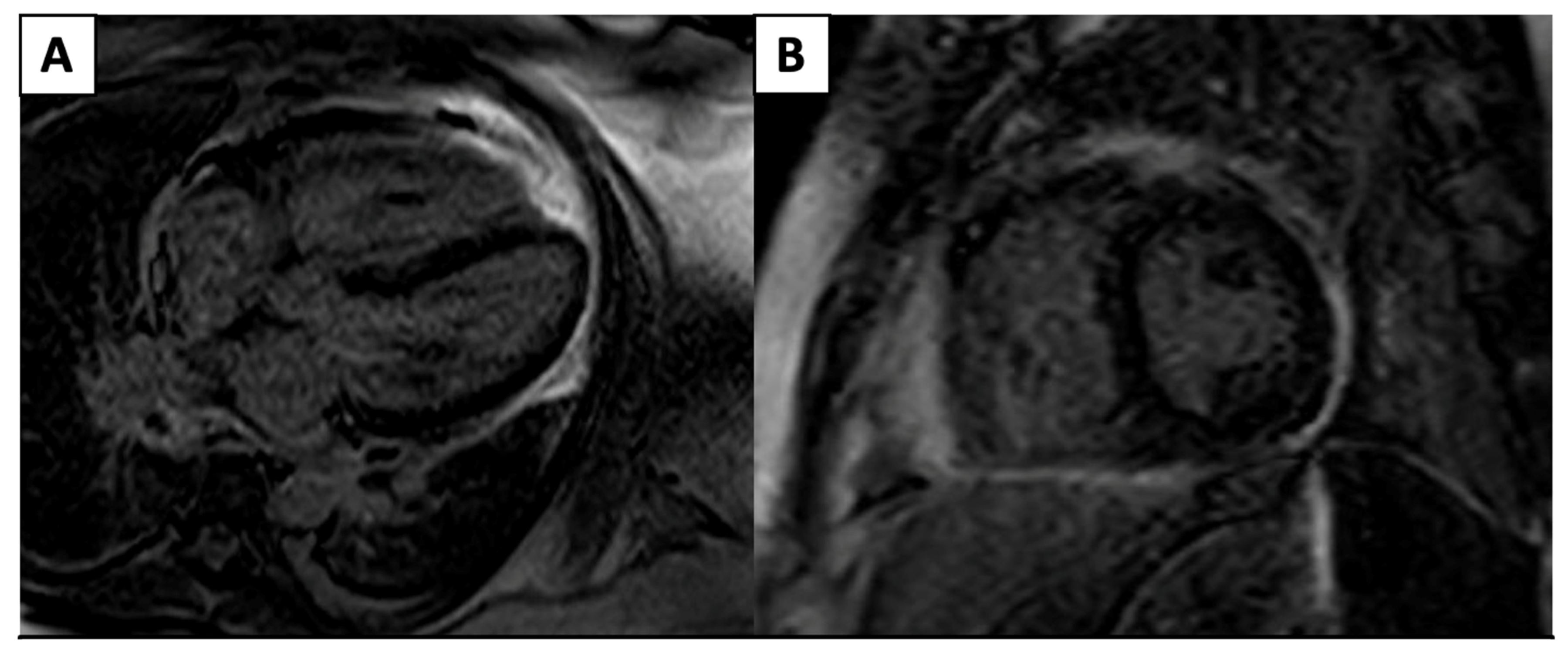
| Cardiac MRI | 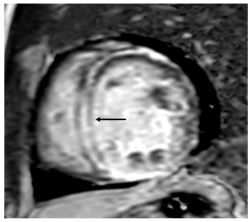 | Short-axis view reveal interventricular mid-myocardial LGE (black arrow). |
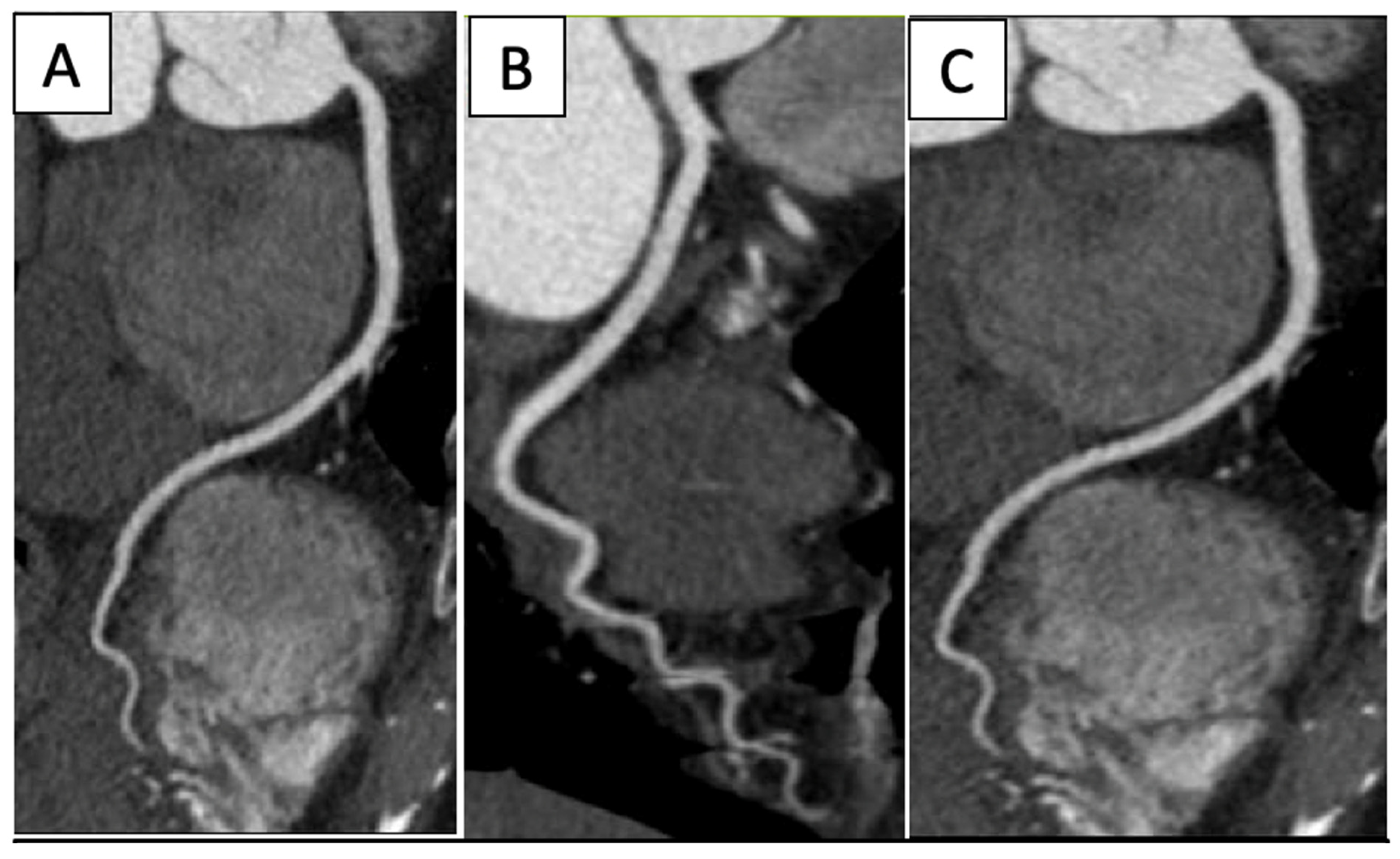
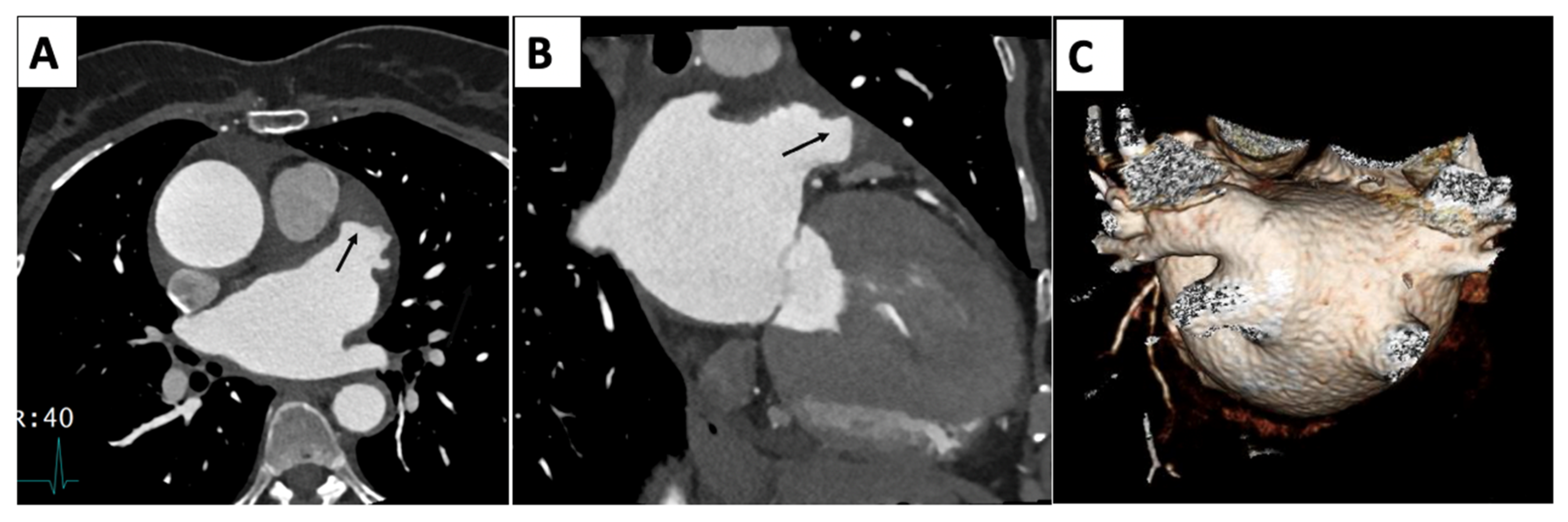
| Cardiac CT | 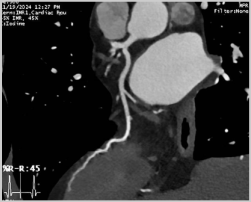 | Left-anterior descending artery on cardiac CT |
| Nuclear |  | Normal fluorodeoxyglucose uptake in the myocardium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.M.; Lerman, B.; Contreras Yametti, F.; Garcia, M.; Slipczuk, L.; Schenone, A.L.; Zhang, L.; Gongora, C.A. Cardio-Oncology and Multi-Imaging Modalities. J. Clin. Med. 2025, 14, 4353. https://doi.org/10.3390/jcm14124353
Park CM, Lerman B, Contreras Yametti F, Garcia M, Slipczuk L, Schenone AL, Zhang L, Gongora CA. Cardio-Oncology and Multi-Imaging Modalities. Journal of Clinical Medicine. 2025; 14(12):4353. https://doi.org/10.3390/jcm14124353
Chicago/Turabian StylePark, Christine M., Ben Lerman, Felipe Contreras Yametti, Mario Garcia, Leandro Slipczuk, Aldo L. Schenone, Lili Zhang, and Carlos A. Gongora. 2025. "Cardio-Oncology and Multi-Imaging Modalities" Journal of Clinical Medicine 14, no. 12: 4353. https://doi.org/10.3390/jcm14124353
APA StylePark, C. M., Lerman, B., Contreras Yametti, F., Garcia, M., Slipczuk, L., Schenone, A. L., Zhang, L., & Gongora, C. A. (2025). Cardio-Oncology and Multi-Imaging Modalities. Journal of Clinical Medicine, 14(12), 4353. https://doi.org/10.3390/jcm14124353