
Low-Density Lipoprotein Cholesterol Reduction and Therapeutic Adherence During Cardiac Rehabilitation After Myocardial Infarction
 , ,
, ,  , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
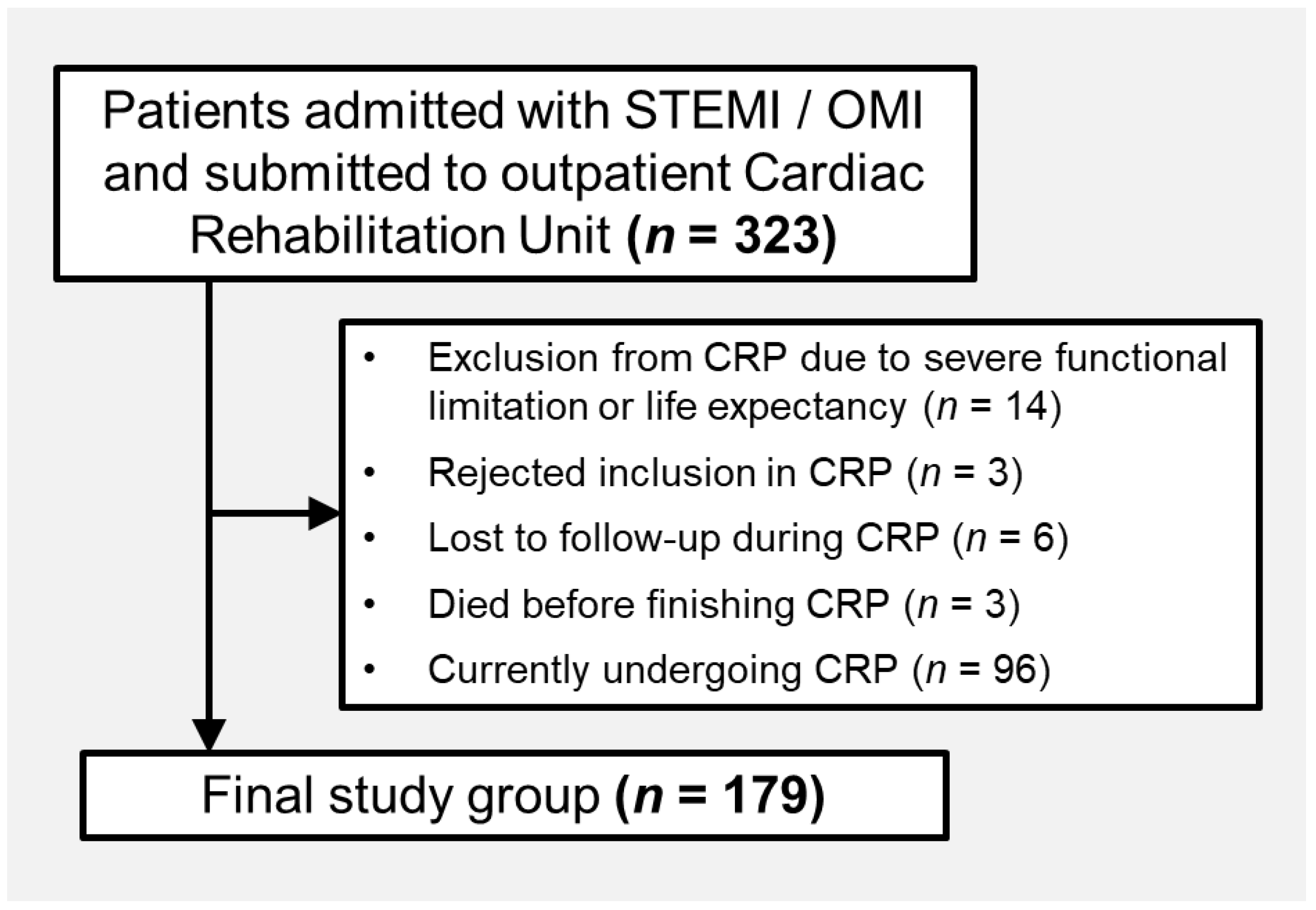
2.1. Population
2.2. Cardiac Rehabilitation Program
2.3. Lipid Profile and LLT Analysis
2.4. Corrected Basal LDL-C and Theoretical Potency of LLT
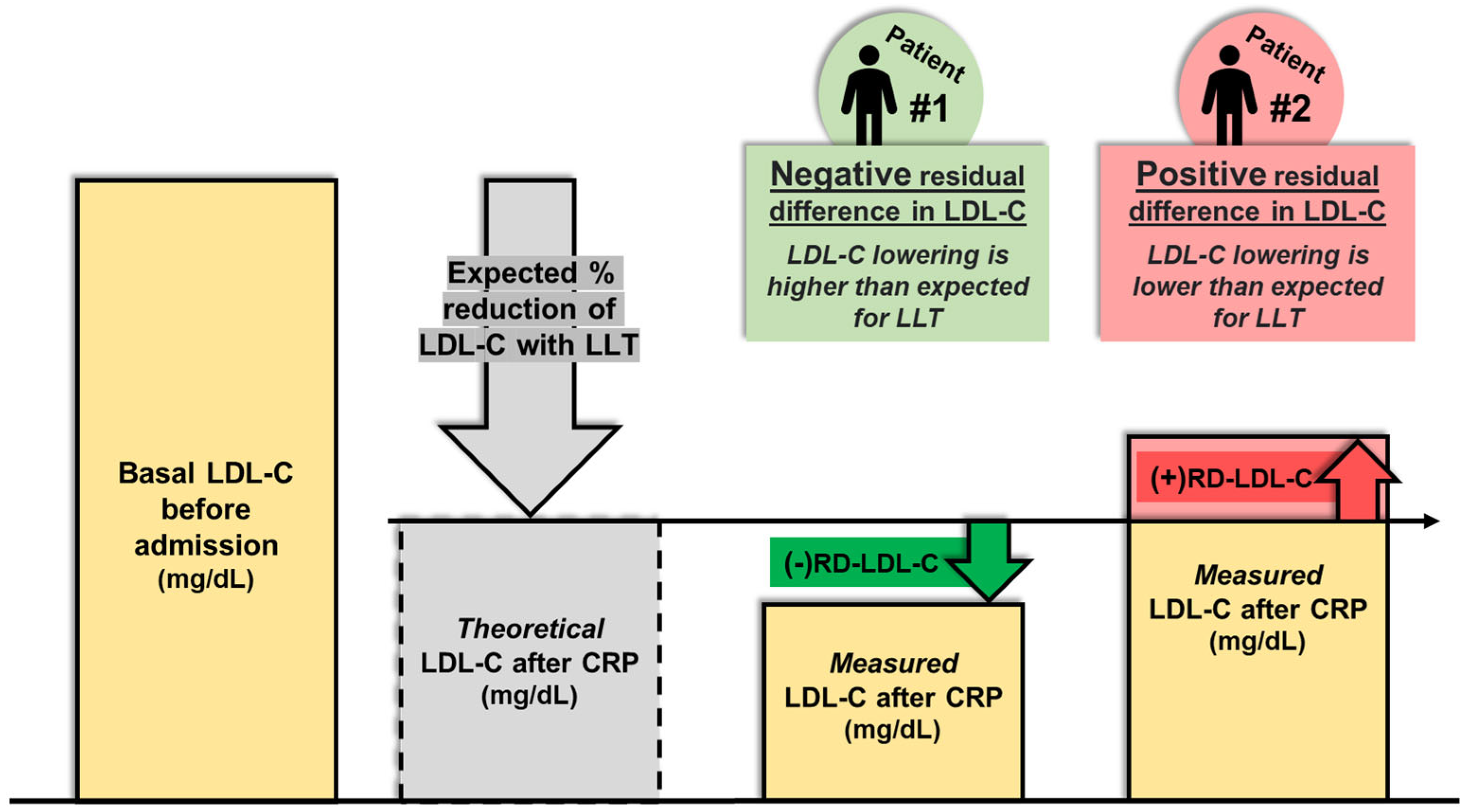
2.5. Residual Difference in LDL-C
2.6. CRP Outcomes
2.7. Objetive of the Study
2.8. Ethics
2.9. Statistical Analysis
3. Results
3.1. Cohort Description
3.2. Lipid-Lowering Therapy Before and After Phase 2 CRP
3.3. Residual Difference in LDL-C
3.4. Predictors of Positive Residual Difference in LDL-C
4. Discussion
4.1. Post-MI LDL-C Goals and Cardiac Rehabilitation
4.2. Lifestyle Habits, Therapeutic Adherence, and Therapeutic Inertia
4.3. Predictors of Positive RD-LDL-C
4.4. Implications for Clinical Practice
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUC | Area under the curve |
| BMI | Body mass index |
| CET | Conventional exercise testing |
| CI | Confidence Interval |
| CPET | Cardiopulmonary exercise testing |
| CRP | Cardiac Rehabilitation Program |
| GAD-2 | Generalized Anxiety Disorder 2-item |
| GRACE | Global Registry of Acute Coronary Events |
| HDL-C | High-density lipoprotein cholesterol |
| HR | Hazard ratio |
| IPAQ | International Physical Activity Questionnaire |
| LDL-C | Low-Density Lipoprotein Cholesterol |
| LLT | Lipid-lowering therapy |
| LVEF | Left Ventricular Ejection Fraction |
| METS | Metabolic equivalents |
| MI | Myocardial Infarction |
| OMI | Occlusion Myocardial Infarction |
| PHQ-2 | Patient Health Questionnaire 2-item |
| RD-LDL-C | Residual difference in LDL-C |
| ROC | Receiver operating characteristic |
| SF-36 | 36-Item Short Form Survey Instrument |
| SPSS | Statistical Package for the Social Sciences |
| STEMI | ST-segment Elevation Myocardial Infarction |
| TG | Triglycerides |
| VO2 | Oxygen consumption |
References
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-Density Lipoproteins Cause Atherosclerotic Cardiovascular Disease. 1. Evidence from Genetic, Epidemiologic, and Clinical Studies. A Consensus Statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef] [PubMed]
- Mensah, G.A.; Roth, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risk Factors. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the Management of Acute Coronary Syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Rao, S.V.; O’Donoghue, M.L.; Ruel, M.; Rab, T.; Tamis-Holland, J.E.; Alexander, J.H.; Baber, U.; Baker, H.; Cohen, M.G.; Cruz-Ruiz, M.; et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2025, 151, e771–e862. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Tsai, J.-C.; Liou, Y.-M.; Chan, P. Effectiveness of Endurance Exercise Training in Patients with Coronary Artery Disease: A Meta-Analysis of Randomised Controlled Trials. Eur. J. Cardiovasc. Nurs. 2017, 16, 397–408. [Google Scholar] [CrossRef]
- Javaherian, M.; Dabbaghipour, N.; Mohammadpour, Z.; Attarbashi Moghadam, B. The Role of the Characteristics of Exercise-Based Cardiac Rehabilitation Program in the Improvement of Lipid Profile Level: A Systematic Review and Meta-Analysis. ARYA Atheroscler. 2020, 16, 192–207. [Google Scholar] [CrossRef]
- Wu, G.; Hu, Y.; Ding, K.; Li, X.; Li, J.; Shang, Z. The Effect of Cardiac Rehabilitation on Lipid Levels in Patients with Coronary Heart Disease. A Systematic Review and Meta-Analysis. Glob. Heart 2022, 17, 83. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef]
- Salzwedel, A.; Jensen, K.; Rauch, B.; Doherty, P.; Metzendorf, M.-I.; Hackbusch, M.; Völler, H.; Schmid, J.-P.; Davos, C.H. Effectiveness of Comprehensive Cardiac Rehabilitation in Coronary Artery Disease Patients Treated According to Contemporary Evidence Based Medicine: Update of the Cardiac Rehabilitation Outcome Study (CROS-II). Eur. J. Prev. Cardiol. 2020, 27, 1756–1774. [Google Scholar] [CrossRef] [PubMed]
- Van Halewijn, G.; Deckers, J.; Tay, H.Y.; Van Domburg, R.; Kotseva, K.; Wood, D. Lessons from Contemporary Trials of Cardiovascular Prevention and Rehabilitation: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2017, 232, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Santiago De Araújo Pio, C.; Marzolini, S.; Pakosh, M.; Grace, S.L. Effect of Cardiac Rehabilitation Dose on Mortality and Morbidity: A Systematic Review and Meta-Regression Analysis. Mayo Clin. Proc. 2017, 92, 1644–1659. [Google Scholar] [CrossRef]
- Bertolín-Boronat, C.; Marcos-Garcés, V.; Merenciano-González, H.; Martínez Mas, M.L.; Climent Alberola, J.I.; Perez, N.; López-Bueno, L.; Esteban Argente, M.C.; Valls Reig, M.; Arizón Benito, A.; et al. Depression, Anxiety, and Quality of Life in a Cardiac Rehabilitation Program Without Dedicated Mental Health Resources Post-Myocardial Infarction. J. Cardiovasc. Dev. Dis. 2025, 12, 92. [Google Scholar] [CrossRef]
- Cosin-Sales, J.; Sidelnikov, E.; Villamayor, S.; Fernández, M.; Merino-Montero, S.; Zamora, A. Identification of Secondary Prevention Patients Eligible for PCSK9 Inhibitors Therapy According to the Routine Clinical Practice in Spain. Adv. Ther. 2023, 40, 2710–2724. [Google Scholar] [CrossRef]
- Ray, K.K.; Molemans, B.; Schoonen, W.M.; Giovas, P.; Bray, S.; Kiru, G.; Murphy, J.; Banach, M.; De Servi, S.; Gaita, D.; et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DA VINCI Study. Eur. J. Prev. Cardiol. 2021, 28, 1279–1289. [Google Scholar] [CrossRef]
- De Backer, G.; Jankowski, P.; Kotseva, K.; Mirrakhimov, E.; Reiner, Ž.; Rydén, L.; Tokgözoğlu, L.; Wood, D.; De Bacquer, D.; De Backer, G.; et al. Management of Dyslipidaemia in Patients with Coronary Heart Disease: Results from the ESC-EORP EUROASPIRE V Survey in 27 Countries. Atherosclerosis 2019, 285, 135–146. [Google Scholar] [CrossRef]
- Grau, M.; Elosua, R.; Cabrera De León, A.; Guembe, M.J.; Baena-Díez, J.M.; Vega Alonso, T.; Javier Félix, F.; Zorrilla, B.; Rigo, F.; Lapetra, J.; et al. Factores de riesgo cardiovascular en España en la primera década del siglo xxi: Análisis agrupado con datos individuales de 11 estudios de base poblacional, estudio DARIOS. Rev. Esp. Cardiol. 2011, 64, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Cosín Sales, J.; Escobar Cervantes, C.; Gómez-Barrado, J.J.; Andreu Cayuelas, J.M.; García Del Egido, A.; Castro Martín, J.J.; Huelmos Rodrigo, A.I.; Corbi-Pascual, M.; Varela Cancelo, A.; Vidal-Pérez, R.; et al. Impact of Therapeutic Inertia in Lipid-Lowering Therapy in Patients at Very High Cardiovascular Risk. Clin. Investig. Arterioscler. 2025, 500773. [Google Scholar] [CrossRef]
- Faggiano, A.; Gualeni, A.; Barbieri, L.; Mureddu, G.F.; Venturini, E.; Giallauria, F.; Ambrosetti, M.; Ruzzolini, M.; Maranta, F.; Silverii, M.V.; et al. Therapeutic Inertia in Dyslipidemia Management for Secondary Cardiovascular Prevention: Results from the Italian ITACARE-P Network. J. Clin. Med. 2025, 14, 493. [Google Scholar] [CrossRef]
- Dixon, D.L.; Sharma, G.; Sandesara, P.B.; Yang, E.; Braun, L.T.; Mensah, G.A.; Sperling, L.S.; Deedwania, P.C.; Virani, S.S. Therapeutic Inertia in Cardiovascular Disease Prevention. J. Am. Coll. Cardiol. 2019, 74, 1728–1731. [Google Scholar] [CrossRef] [PubMed]
- Zheng, E.; Madura, P.; Grandos, J.; Broncel, M.; Pawlos, A.; Woźniak, E.; Gorzelak-Pabiś, P. When the Same Treatment Has Different Response: The Role of Pharmacogenomics in Statin Therapy. Biomed. Pharmacother. 2024, 170, 115966. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, S.; Pollevick, M.E.; Lara-Breitinger, K.M.; Stone, N.J. Inter-Individual Variability in Lipid Response: A Narrative Review. Am. J. Med. 2022, 135, 1427–1433.e7. [Google Scholar] [CrossRef]
- Velasco (Coordinador), J.A.; Cosín, J.; Maroto, J.M.; Muñiz, J.; Casasnovas, J.A.; Plaza, I.; Tomás Abadal, L. Guías de práctica clínica de la Sociedad Española de Cardiología en prevención cardiovascular y rehabilitación cardíaca. Rev. Esp. Cardiol. 2000, 53, 1095–1120. [Google Scholar] [CrossRef]
- Ambrosetti, M.; Abreu, A.; Corrà, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.E.; Schmid, J.-P.; Vigorito, C.; et al. Secondary Prevention through Comprehensive Cardiovascular Rehabilitation: From Knowledge to Implementation. 2020 Update. A Position Paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef]
- AACVPR Stratification Algorithm for Risk of Event. Available online: https://www.aacvpr.org/Portals/0/2014_AACVPR-Risk-Stratification-Algorithm.pdf (accessed on 12 May 2025).
- Marcos-Garcés, V.; Merenciano-González, H.; Martínez Mas, M.L.; Palau, P.; Climent Alberola, J.I.; Perez, N.; López-Bueno, L.; Esteban Argente, M.C.; Valls Reig, M.; Muñoz Alcover, R.; et al. Short-Course High-Intensity Statin Treatment during Admission for Myocardial Infarction and LDL-Cholesterol Reduction—Impact on Tailored Lipid-Lowering Therapy at Discharge. J. Clin. Med. 2023, 13, 127. [Google Scholar] [CrossRef] [PubMed]
- Bertolín-Boronat, C.; Merenciano-González, H.; Marcos-Garcés, V.; Martínez-Mas, M.L.; Climent Alberola, J.I.; Pérez, N.; López-Bueno, L.; Esteban-Argente, M.C.; Valls Reig, M.; Arizón Benito, A.; et al. Dynamics of HDL-Cholesterol Following a Post-Myocardial Infarction Cardiac Rehabilitation Program. Rev. Cardiovasc. Med. 2025, 26, 25399. [Google Scholar] [CrossRef]
- Bertolín-Boronat, C.; Marcos-Garcés, V.; Merenciano-González, H.; Martínez Mas, M.L.; Climent Alberola, J.I.; Perez, N.; López Bueno, L.; Esteban Argente, M.C.; Valls Reig, M.; Arizón Benito, A.; et al. Familial Hypercholesterolemia Screening in a Cardiac Rehabilitation Program After Myocardial Infarction. Cardiogenetics 2025, 15, 6. [Google Scholar] [CrossRef]
- Masana, L.; Ibarretxe, D.; Plana, N. Reasons Why Combination Therapy Should Be the New Standard of Care to Achieve the LDL-Cholesterol Targets: Lipid-Lowering Combination Therapy. Curr. Cardiol. Rep. 2020, 22, 66. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (Ctt) Collaboration; Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; et al. Efficacy and Safety of More Intensive Lowering of LDL Cholesterol: A Meta-Analysis of Data from 170 000 Participants in 26 Randomised Trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (Ctt) Collaborators; Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R.; et al. The Effects of Lowering LDL Cholesterol with Statin Therapy in People at Low Risk of Vascular Disease: Meta-Analysis of Individual Data from 27 Randomised Trials. Lancet 2012, 380, 581–590. [Google Scholar] [CrossRef]
- Leening, M.J.G. Overcoming Therapeutic Inertia in LDL Cholesterol-Lowering Treatment with Education and Simplified Treatment Algorithms. Neth. Heart J. 2024, 32, 198–199. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.S.; Branch, W.T.; Cook, C.B.; Doyle, J.P.; El-Kebbi, I.M.; Gallina, D.L.; Miller, C.D.; Ziemer, D.C.; Barnes, C.S. Clinical Inertia. Ann. Intern. Med. 2001, 135, 825–834. [Google Scholar] [CrossRef]
- Lavoie, K.L.; Rash, J.A.; Campbell, T.S. Changing Provider Behavior in the Context of Chronic Disease Management: Focus on Clinical Inertia. Annu. Rev. Pharmacol. Toxicol. 2017, 57, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Descamps, O.; Tomassini, J.E.; Lin, J.; Polis, A.B.; Shah, A.; Brudi, P.; Hanson, M.E.; Tershakovec, A.M. Variability of the LDL-C Lowering Response to Ezetimibe and Ezetimibe + Statin Therapy in Hypercholesterolemic Patients. Atherosclerosis 2015, 240, 482–489. [Google Scholar] [CrossRef]
- Makhmudova, U.; Schatz, U.; Perakakis, N.; Kassner, U.; Schumann, F.; Axthelm, C.; Stürzebecher, P.; Sinning, D.L.; Doevelaar, A.; Rohn, B.; et al. High Interindividual Variability in LDL-Cholesterol Reductions after Inclisiran Administration in a Real-World Multicenter Setting in Germany. Clin. Res. Cardiol. 2023, 112, 1639–1649. [Google Scholar] [CrossRef]
- Ouyang, M.; Li, C.; Hu, D.; Peng, D.; Yu, B. Mechanisms of Unusual Response to Lipid-Lowering Therapy: PCSK9 Inhibition. Clin. Chim. Acta 2023, 538, 113–123. [Google Scholar] [CrossRef]
- Smith, J.R.; Thomas, R.J.; Bonikowske, A.R.; Hammer, S.M.; Olson, T.P. Sex Differences in Cardiac Rehabilitation Outcomes. Circ. Res. 2022, 130, 552–565. [Google Scholar] [CrossRef] [PubMed]
- Samayoa, L.; Grace, S.L.; Gravely, S.; Scott, L.B.; Marzolini, S.; Colella, T.J.F. Sex Differences in Cardiac Rehabilitation Enrollment: A Meta-Analysis. Can. J. Cardiol. 2014, 30, 793–800. [Google Scholar] [CrossRef]
- Oosenbrug, E.; Marinho, R.P.; Zhang, J.; Marzolini, S.; Colella, T.J.F.; Pakosh, M.; Grace, S.L. Sex Differences in Cardiac Rehabilitation Adherence: A Meta-Analysis. Can. J. Cardiol. 2016, 32, 1316–1324. [Google Scholar] [CrossRef]
- Peters, S.A.E.; Colantonio, L.D.; Zhao, H.; Bittner, V.; Dai, Y.; Farkouh, M.E.; Monda, K.L.; Safford, M.M.; Muntner, P.; Woodward, M. Sex Differences in High-Intensity Statin Use Following Myocardial Infarction in the United States. J. Am. Coll. Cardiol. 2018, 71, 1729–1737. [Google Scholar] [CrossRef] [PubMed]
- Van Oortmerssen, J.A.E.; Mulder, J.W.C.M.; Van Der Bijl, M.F.; Mijnster, R.J.M.; Kavousi, M.; Roeters Van Lennep, J.E. on behalf of the IMPRESS consortium Lipid Lowering Therapy Utilization and Lipid Goal Attainment in Women. Curr. Atheroscler. Rep. 2025, 27, 29. [Google Scholar] [CrossRef]
- Colantonio, L.D.; Huang, L.; Monda, K.L.; Bittner, V.; Serban, M.-C.; Taylor, B.; Brown, T.M.; Glasser, S.P.; Muntner, P.; Rosenson, R.S. Adherence to High-Intensity Statins Following a Myocardial Infarction Hospitalization Among Medicare Beneficiaries. JAMA Cardiol. 2017, 2, 890. [Google Scholar] [CrossRef] [PubMed]
- Bots, S.H.; Inia, J.A.; Peters, S.A.E. Medication Adherence After Acute Coronary Syndrome in Women Compared with Men: A Systematic Review and Meta-Analysis. Front. Glob. Womens Health 2021, 2, 637398. [Google Scholar] [CrossRef]
- O’Donoghue, M.L.; Morrow, D.A.; Tsimikas, S.; Sloan, S.; Ren, A.F.; Hoffman, E.B.; Desai, N.R.; Solomon, S.D.; Domanski, M.; Arai, K.; et al. Lipoprotein(a) for Risk Assessment in Patients with Established Coronary Artery Disease. J. Am. Coll. Cardiol. 2014, 63, 520–527. [Google Scholar] [CrossRef]
- Afshar, M.; Pilote, L.; Dufresne, L.; Engert, J.C.; Thanassoulis, G. Lipoprotein(a) Interactions with Low-Density Lipoprotein Cholesterol and Other Cardiovascular Risk Factors in Premature Acute Coronary Syndrome (ACS). J. Am. Heart Assoc. 2016, 5, e003012. [Google Scholar] [CrossRef]
- Sheashaa, H.; Mousa, H.; Abbas, M.T.; Farina, J.M.; Awad, K.; Pereyra, M.; Scalia, I.G.; Ali, N.B.; Javadi, N.; Bismee, N.N.; et al. Interaction Between Lipoprotein(a) and Other Lipid Molecules: A Review of the Current Literature. Biomolecules 2025, 15, 162. [Google Scholar] [CrossRef] [PubMed]
- Arnold, N.; Blaum, C.; Goßling, A.; Brunner, F.J.; Bay, B.; Zeller, T.; Ferrario, M.M.; Brambilla, P.; Cesana, G.; Leoni, V.; et al. Impact of Lipoprotein(a) Level on Low-Density Lipoprotein Cholesterol– or Apolipoprotein B–Related Risk of Coronary Heart Disease. J. Am. Coll. Cardiol. 2024, 84, 165–177. [Google Scholar] [CrossRef]
- Chait, A.; Eckel, R.H.; Vrablik, M.; Zambon, A. Lipid-Lowering in Diabetes: An Update. Atherosclerosis 2024, 394, 117313. [Google Scholar] [CrossRef]
- Armillotta, M.; Angeli, F.; Paolisso, P.; Belmonte, M.; Raschi, E.; Di Dalmazi, G.; Amicone, S.; Canton, L.; Fedele, D.; Suma, N.; et al. Cardiovascular Therapeutic Targets of Sodium-Glucose Co-Transporter 2 (SGLT2) Inhibitors beyond Heart Failure. Pharmacol. Ther. 2025, 270, 108861. [Google Scholar] [CrossRef]
- Velidakis, N.; Stachteas, P.; Gkougkoudi, E.; Papadopoulos, C.; Kadoglou, N.P.E. Classical and Novel Lipid-Lowering Therapies for Diabetic Patients with Established Coronary Artery Disease or High Risk of Coronary Artery Disease—A Narrative Clinical Review. Pharmaceuticals 2024, 17, 568. [Google Scholar] [CrossRef]
- Wittlinger, T.; Schwaab, B.; Völler, H.; Bongarth, C.; Heinze, V.; Eckrich, K.; Guha, M.; Richter, M.; Schlitt, A. Efficacy of Lipid-Lowering Therapy during Cardiac Rehabilitation in Patients with Diabetes Mellitus and Coronary Heart Disease. J. Cardiovasc. Dev. Dis. 2021, 8, 105. [Google Scholar] [CrossRef]
- Schwaab, B.; Waldmann, A.; Katalinic, A.; Sheikhzadeh, A.; Raspe, H. In-Patient Cardiac Rehabilitation versus Medical Care—A Prospective Multicentre Controlled 12 Months Follow-up in Patients with Coronary Heart Disease. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Mänttäri, M.; Tenkanen, L.; Mäenpää, H.; Manninen, V.; Huttunen, J.K. High-Density Lipoprotein Cholesterol Elevation with Gemfibrozil: Effects of Baseline Level and Modifying Factors. Clin. Pharmacol. Ther. 1993, 54, 437–447. [Google Scholar] [CrossRef]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation: A Scientific Statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation 2019, 140, e69–e89. [Google Scholar] [CrossRef]
- Hama, T.; Chacin Suarez, A.S.; Bissen, T.G.; Bonikowske, A.R.; Smith, J.R.; Taylor, B.J.; Wheatley-Guy, C.M.; Scales, R.; Rogers, M.J.; Ahlskog, A.L.; et al. Home-Based Cardiac Rehabilitation Among Attendees from a Large Health Care System During the Covid-19 Pandemic. JACC Adv. 2024, 3, 101403. [Google Scholar] [CrossRef] [PubMed]
- Husaini, M.; Deych, E.; Waken, R.J.; Sells, B.; Lai, A.; Racette, S.B.; Rich, M.W.; Joynt Maddox, K.E.; Peterson, L.R. Intensive Versus Traditional Cardiac Rehabilitation: Mortality and Cardiovascular Outcomes in a 2016–2020 Retrospective Medicare Cohort. Circ. Cardiovasc. Qual. Outcomes 2023, 16, e010131. [Google Scholar] [CrossRef] [PubMed]
- Merenciano-Gonzalez, H.; Marcos Garces, V.; Martinez Mas, M.L.; Palau, P.; Climent Alberola, J.I.; Perez, N.; Lopez-Bueno, L.; Esteban Argente, M.C.; Valls Reig, M.; Munoz Alcover, R.; et al. Residual Difference in LDL Cholesterol as an Indicator of Adherence to Lifestyle Changes during Cardiac Rehabilitation. Eur. Heart J. 2023, 44 (Suppl. S2), ehad655.2592. [Google Scholar] [CrossRef]
- Merenciano-González, H.; Marcos-Garcés, V.; Martínez Mas, M.L.; Palau Sampío, P.; Climent Alberola, J.I.; Pérez Solé, N.; López Bueno, L.; Esteban Argente, M.C.; Valls Reig, M.; Muñoz Alcover, R.; et al. Diferencia Residual en Colesterol LDL como Indicador de Adherencia a Cambios en el Estilo de Vida Durante un Programa Ambulatorio de Rehabilitación Cardiaca. Rev. Esp. Cardiol. 2023, 76 (Suppl. S1), 99. Available online: https://www.revespcardiol.org/es-congresos-sec--el-congreso-de-la-salud-cardiovascu-157-sesion-rehabilitacion-cardiaca-y-adherencia-7567-diferencia-residual-en-colesterol-ldl-co-92384 (accessed on 10 April 2025). [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 179) | Negative RD-LDL-C (n = 125) | Positive RD-LDL-C (n = 54) | p-Value |
|---|---|---|---|---|
| Clinical variables | ||||
| Age (years) | 63.04 ± 10.56 | 61.83 ± 9.8 | 65.84 ± 11.77 | 0.03 |
| Male sex (%) | 152 (84.9) | 99 (79.2) | 53 (98.1) | 0.001 |
| Hypercholesterolemia (%) | 160 (89.4) | 115 (92) | 45 (83.3) | 0.08 |
| Hypertension (%) | 102 (57) | 65 (52) | 37 (68.5) | 0.04 |
| Diabetes mellitus (%) | 42 (23.5) | 36 (28.8) | 6 (11.1) | 0.01 |
| Killip class ≥ 2 (%) | 51 (28.5) | 31 (24.8) | 20 (37) | 0.1 |
| GRACE risk score | 118.3 ± 28.88 | 114.72 ± 26.2 | 126.61 ± 33.08 | 0.02 |
| Infarct location | 0.46 | |||
| Anterior (%) | 80 (44.7) | 51 (40.8) | 29 (53.7) | |
| Inferior (%) | 78 (43.6) | 58 (46.4) | 20 (37) | |
| Lateral (%) | 12 (6.7) | 9 (7.2) | 3 (5.6) | |
| OMI (%) | 9 (5) | 7 (5.6) | 2 (3.7) | |
| LVEF (%) | 52.29 ± 10.57 | 52.74 ± 10.7 | 51.26 ± 10.28 | 0.39 |
| LVEF < 50% (%) | 63 (35.2) | 44 (35.2) | 19 (35.2) | 1 |
| Exercise training modality during CRP | 0.02 | |||
| Ambulatory training (%) | 142 (79.3) | 93 (74.4) | 49 (90.7) | |
| Supervised in-hospital training (%) | 37 (20.7) | 32 (25.6) | 5 (9.3) | |
| Lipid and metabolic profile before admission | ||||
| Fasting blood glucose (mg/dL) | 99.59 ± 23.69 | 103.27 ± 24.66 | 91.15 ± 18.95 | 0.002 |
| Total cholesterol (mg/dL) | 199.83 ± 54.72 | 205.78 ± 54.13 | 186.04 ± 54.05 | 0.03 |
| Triglycerides (mg/dL) | 124 [90, 169] | 156.76 [97, 184] | 117.54 [84, 150.25] | 0.002 |
| HDL-C (mg/dL) | 46.25 ± 11.1 | 45.99 ± 9.99 | 46.85 ± 13.41 | 0.67 |
| Non-HDL-C (mg/dL) | 153.58 ± 51.4 | 159.79 ± 51.92 | 139.19 ± 47.58 | 0.01 |
| LDL-C (mg/dL) | 131.66 ± 45.02 | 136.06 ± 45.36 | 121.46 ± 42.91 | 0.04 |
| Corrected basal LDL-C (mg/dL) # | 159.72 ± 45.14 | 166.9 ± 44.69 | 143.09 ± 42.03 | 0.001 |
| LLT before admission (%) | 64 (35.8) | 47 (37.6) | 17 (31.5) | 0.43 |
| HbA1c (%) * | 6.25 ± 1.51 | 6.5 ± 1.33 | 5.32 ± 1.81 | 0.01 |
| Lipid and metabolic profile after CRP | ||||
| Fasting blood glucose (mg/dL) | 94.91 ± 18.7 | 97.33 ± 20.08 | 89.41 ± 13.72 | 0.009 |
| Median change (mg/dL) | −4.5 [−12.8, 5.75] | −5.5 [−13.25, 5.5] | −3 [−12, 6] | 0.47 |
| Total cholesterol (mg/dL) | 102.63 ± 17.85 | 99.44 ± 17.81 | 109.96 ± 15.79 | <0.001 |
| Mean change (mg/dL) | −97.31 ± 52.44 | −106.56 ± 50.23 | −76.07 ± 51.68 | <0.001 |
| Triglycerides (mg/dL) | 86.5 [65–118] | 93 [68.25, 122.5] | 78 [59.5, 103] | 0.02 |
| Median change (mg/dL) | −36.5 [−73.25, −6.75] | −40 [−75.5, −12.5] | −27 [−67.25, 0] | 0.1 |
| HDL-C (mg/dL) | 43.28 ± 9.03 | 42.76 ± 8.71 | 44.48 ± 9.71 | 0.24 |
| Median change (mg/dL) | −3 [−8, 2] | −3 [−8, 2] | −3 [−7.25, 2.5] | 0.99 |
| Non-HDL-C (mg/dL) | 59.35 ± 16.17 | 56.69 ± 16.64 | 65.48 ± 13.24 | 0.001 |
| Mean change (mg/dL) | −94.26 ± 49.72 | −103.22 ± 48.24 | −73.7 ± 47.3 | <0.001 |
| LDL-C (mg/dL) | 43.05 ± 13.8 | 39.3 ± 13.52 | 51.72 ± 10.13 | <0.001 |
| Mean change (mg/dL) | −88.61 ± 42.71 | −96.76 ± 41.13 | −69.74 ± 40.62 | <0.001 |
| Theoretical LDL-C after CRP (mg/dL) | 50.82 ± 16.18 | 54.79 ± 16.24 | 41.64 ± 11.8 | <0.001 |
| RD-LDL-C (mg/dL) | −7.54 [−16.8, 2.8] | −13.6 [−20.12, −6.91] | 8.92 [3.97, 14.39] | <0.001 |
| LDL-C < 55 mg/dL after CRP (%) | 153 (85.5) | 117 (93.6) | 36 (66.7) | <0.001 |
| HbA1c (%) | 6 ± 0.6 | 6.06 ± 0.66 | 5.86 ± 0.39 | 0.04 |
| Median change (%) | 0.1 [−0.3, 0.4] | 0 [−0.4, 0.28] | 0.3 [0.2, 0.4] | 0.13 |
| HbA1c < 7% after CRP (%) | 168 (94.9) | 116 (93.5) | 52 (98.1) | 0.21 |
| Other cardiovascular risk factors | ||||
| Lipoprotein (a) (mg/dL) | 28 [12.25, 76.75] | 25 [12, 60] | 49 [15, 90] | 0.03 |
| Smoking habit before CRP (%) | 87 (48.6) | 61 (48.8) | 26 (48.1) | 0.94 |
| Smoking habit after CRP (%) | 12 (6.7) | 6 (4.8) | 6 (11.1) | 0.12 |
| Systolic pressure before CRP (mmHg) | 124.6 ± 15.42 | 125 ± 15.52 | 123.67 ± 15.28 | 0.6 |
| Systolic pressure after CRP (mmHg) | 115.14 ± 9.69 | 115.02 ± 9.44 | 115.43 ± 10.35 | 0.8 |
| Median change (mmHg) | −10 [−20, 0] | −10 [−20, −4] | −6 [−16, 0] | 0.2 |
| Diastolic pressure before CRP (mmHg) | 77.6 ± 8.51 | 78.22 ± 7.78 | 76.15 ± 9.1 | 0.71 |
| Diastolic pressure after CRP (mmHg) | 73.54 ± 7.12 | 74.36 ± 6.87 | 72.95 ± 7.56 | 0.82 |
| Median change (mmHg) | −4 [−7, 0] | −4 [−8, −2] | −4 [−6, 0] | 0.87 |
| Weight before CRP (kg) | 79.85 ± 13.4 | 79.93 ± 13.99 | 79.68 ± 12.06 | 0.91 |
| Weight after CRP (kg) | 78.03 ± 12.78 | 78.18 ±13.14 | 77.68 ± 12 | 0.81 |
| Median change (kg) | −1 [−4, 1.5] | −1.5 [−4, 1.5] | −0.7 [−4.63, 1.25] | 0.81 |
| BMI before CRP | 27.47 ± 4.2 | 27.8 ± 4.48 | 26.7 ± 3.41 | 0.11 |
| BMI after CRP | 26.87 ± 3.98 | 27.22 ± 4.18 | 26.08 ± 3.39 | 0.08 |
| Median change | −0.33 [−1.49, 0.37] | −0.41 [−1.48, 0.47] | −0.24 [−1.53, 0.21] | 0.92 |
| BMI ≥ 30 before CRP (%) | 39 (21.8) | 31 (24.8) | 8 (14.8) | 0.14 |
| BMI ≥ 30 after CRP (%) | 34 (19) | 27 (21.6) | 7 (13) | 0.18 |
| Adherence to Mediterranean diet after CRP (≥8 points in PREDIMED) | 155 (88.1) | 106 (86.2) | 49 (92.5) | 0.24 |
| Therapeutic adherence after CRP (4 points in Morisky–Green) | 158 (89.8) | 109 (88.6) | 49 (92.5) | 0.44 |
| Quality of life outcomes | ||||
| SF-36 (mean) before CRP (points) | 64 ± 19.4 | 64.19 ± 18.7 | 63.54 ± 21.09 | 0.84 |
| SF-36 (mean) after CRP (points) | 71.27 ± 18.88 | 71.01 ± 19.04 | 71.88 ± 18.66 | 0.78 |
| Median change (points) | 5.61 [−3.66, 18.38] | 5.28 [−3.73, 15.48] | 5.88 [−3.08, 21.48] | 0.49 |
| PHQ-2 before CRP (points) | 1 [0, 2] | 1 [0, 2] | 1 [0, 2] | 0.74 |
| PHQ-2 after CRP (points) | 0 [0, 2] | 0 [0, 2] | 0 [0, 2] | 0.43 |
| Median change (points) | 0 [−1, 0] | 0 [−1, 0] | 0 [−1, 0] | 0.22 |
| GAD-2 before CRP (points) | 2 [0, 3] | 2 [0, 3] | 2 [0, 3] | 0.74 |
| GAD-2 after CRP (points) | 1 [0, 2] | 1 [0, 2] | 1 [0, 2] | 0.94 |
| Median change (points) | 0 [−2, 0] | 0 [−1, 0] | 0 [−2, 0] | 0.99 |
| Physical fitness variables | ||||
| IPAQ before CRP (METS/week) | 1386 [641.25, 2772] | 1386 [495, 2772] | 1386 [693, 2826.75] | 0.5 |
| IPAQ after CRP (METS/week) | 3545 [1980, 6132] | 3339 [1980, 5670] | 4531 [1998, 6774] | 0.1 |
| Median change (METS/week) | 1636 [461.75, 3572.63] | 1565 [489, 3031.5] | 2528.75 [373.88, 5311.5] | 0.19 |
| Peak VO2 before CRP (mL/kg/min) | 25.66 ± 9.26 | 26.39 ± 9.47 | 23.96 ± 8.6 | 0.11 |
| Peak VO2 after CRP (mL/kg/min) | 29.25 ± 10.43 | 30.03 ± 10.6 | 27.44 ± 9.89 | 0.13 |
| Mean change (mL/kg/min) | 3.6 ± 4.73 | 3.64 ± 4.77 | 3.49 ± 4.67 | 0.84 |
| All Patients (n = 179) | Negative RD-LDL-C (n = 125) | Positive RD-LDL-C (n = 54) | p-Value | |
|---|---|---|---|---|
| LLT at discharge | ||||
| Statins | 0.74 | |||
| No statin | 6 (3.4) | 4 (3.2) | 2 (3.7) | |
| Fluvastatin 80 mg o.d. | 1 (0.6) | 1 (0.8) | 0 (0) | |
| Pitavastatin 4 mg o.d. | 1 (0.6) | 1 (0.8) | 0 (0) | |
| Atorvastatin 20 mg o.d. | 2 (1.1) | 2 (1.6) | 0 (0) | |
| Atorvastatin 40 mg o.d. | 20 (11.2) | 16 (12.8) | 4 (7.4) | |
| Atorvastatin 60 mg o.d. | 3 (1.7) | 2 (1.6) | 1 (1.9) | |
| Atorvastatin 80 mg o.d. | 63 (35.2) | 39 (31.2) | 24 (44.4) | |
| Rosuvastatin 10 mg o.d. | 9 (5) | 7 (5.6) | 2 (3.7) | |
| Rosuvastatin 15 mg o.d. | 2 (1.1) | 1 (0.8) | 1 (1.9) | |
| Rosuvastatin 20 mg o.d. | 71 (39.7) | 51 (40.8) | 20 (37) | |
| Rosuvastatin 30 mg o.d. | 1 (0.6) | 1 (0.8) | 0 (0) | |
| Ezetimibe 10 mg o.d. | 97 (54.2) | 72 (57.6) | 25 (46.3) | 0.16 |
| Bempedoic acid 180 mg o.d. | 1 (0.6) | 1 (0.8) | 0 (0) | 0.51 |
| PCSK9 inhibitors | 1 (0.6) | 1 (0.8) | 0 (0) | 0.51 |
| Inclisiran | 0 (0) | 0 (0) | 0 (0) | - |
| Fibrates | 0 (0) | 0 (0) | 0 (0) | - |
| Theoretical potency of LLT at discharge (% reduction of LDL-C) | 58.99 ± 10.96 | 59.41 ± 11.03 | 58.04 ± 10.83 | 0.44 |
| LLT after CRP | ||||
| Statins | 0.04 | |||
| No statin | 1 (0.6) | 1 (0.8) | 0 (0) | |
| Pitavastatin 1 mg o.d. | 1 (0.6) | 0 (0) | 1 (1.9) | |
| Pitavastatin 4 mg o.d. | 2 (1.1) | 2 (1.6) | 0 (0) | |
| Atorvastatin 20 mg o.d. | 1 (0.6) | 0 (0) | 1 (1.9) | |
| Atorvastatin 40 mg o.d. | 23 (12.8) | 18 (14.4) | 5 (9.3) | |
| Atorvastatin 80 mg o.d. | 45 (25.1) | 27 (21.6) | 18 (33.3) | |
| Rosuvastatin 10 mg o.d. | 9 (5) | 8 (6.4) | 1 (1.9) | |
| Rosuvastatin 20 mg o.d. | 85 (47.5) | 65 (52) | 20 (37) | |
| Rosuvastatin 30 mg o.d. | 5 (2.8) | 2 (1.6) | 3 (5.6) | |
| Rosuvastatin 40 mg o.d. | 7 (3.9) | 2 (1.6) | 5 (9.3) | |
| Ezetimibe 10 mg o.d. | 164 (91.6) | 111 (88.8) | 53 (98.1) | 0.04 |
| Bempedoic acid 180 mg o.d. | 19 (10.6) | 8 (6.4) | 11 (20.4) | 0.005 |
| PCSK9 inhibitors | 24 (13.4) | 15 (12) | 9 (16.7) | 0.5 |
| Inclisiran | 6 (3.4) | 5 (4) | 1 (1.9) | 0.52 |
| Fibrates | 1 (0.6) | 1 (0.8) | 0 (0) | 0.54 |
| Theoretical potency of LLT after CRP (% reduction of LDL-C) | 67.44 ± 7.51 | 66.41 ± 7.48 | 69.81 ± 7.07 | 0.005 |
| Median change (%) | 6 [0, 15] | 0 [0, 13] | 9 [3.75, 16.25] | <0.001 |
| Variable | HR [95% CI] | Change in Model’s Nagelkerke’s R2 | Change in Model’s Chi-Squared | p-Value |
|---|---|---|---|---|
| Model 1—clinical variables | ||||
| Age (years) | 1.02 [0.97, 1.08] | - | - | 0.4 |
| Male sex (%) | 16.02 [2.08, 123.34] | 0.107 | 14.07 | 0.008 |
| Hypercholesterolemia (%) | 0.4 [0.13, 1.27] | - | - | 0.12 |
| Hypertension (%) | 1.87 [0.86, 4.07] | - | - | 0.11 |
| Diabetes mellitus (%) | 0.26 [0.1, 0.69] | 0.056 | 7.87 | 0.006 |
| GRACE risk score | 1.01 [0.99, 1.03] | - | - | 0.43 |
| Supervised in-hospital training | 0.26 [0.09, 0.73] | 0.055 | 7.96 | 0.01 |
| Model 2—clinical variables and lipid and metabolic profile variables before admission | ||||
| Male sex | 17.96 [2.15, 149.92] | 0.117 | 14.79 | 0.008 |
| Diabetes mellitus | 0.17 [0.06, 0.51] | 0.07 | 10.85 | 0.002 |
| Supervised in-hospital training | 0.28 [0.09, 0.86] | 0.035 | 5.69 | 0.03 |
| Fasting blood glucose (mg/dL) | 1 [0.98, 1.02] | - | - | 0.91 |
| Total cholesterol (mg/dL) | 0.99 [0.94, 1.05] | - | - | 0.82 |
| Triglycerides (mg/dL) | 0.99 [0.97, 1.01] | - | - | 0.22 |
| Non-HDL-C (mg/dL) | 1.04 [0.94, 1.15] | - | - | 0.43 |
| LDL-C (mg/dL) | 0.98 [0.89, 1.07] | - | - | 0.61 |
| Corrected basal LDL-C (mg/dL) | 0.98 [0.97, 0.99] | 0.077 | 11.2 | 0.001 |
| HbA1c (%) | 0.58 [0.17, 1.92] | - | - | 0.37 |
| Lipoprotein (a) (mg/dL) | 1.02 [1.01, 1.03] | 0.077 | 10.53 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolín-Boronat, C.; Merenciano-González, H.; Marcos-Garcés, V.; Martínez Mas, M.L.; Climent Alberola, J.I.; Civera, J.M.; Valls Reig, M.; Ruiz Hueso, M.; Castro Carmona, P.; Perez, N.; et al. Low-Density Lipoprotein Cholesterol Reduction and Therapeutic Adherence During Cardiac Rehabilitation After Myocardial Infarction. J. Clin. Med. 2025, 14, 4242. https://doi.org/10.3390/jcm14124242
Bertolín-Boronat C, Merenciano-González H, Marcos-Garcés V, Martínez Mas ML, Climent Alberola JI, Civera JM, Valls Reig M, Ruiz Hueso M, Castro Carmona P, Perez N, et al. Low-Density Lipoprotein Cholesterol Reduction and Therapeutic Adherence During Cardiac Rehabilitation After Myocardial Infarction. Journal of Clinical Medicine. 2025; 14(12):4242. https://doi.org/10.3390/jcm14124242
Chicago/Turabian StyleBertolín-Boronat, Carlos, Héctor Merenciano-González, Víctor Marcos-Garcés, María Luz Martínez Mas, Josefa Inés Climent Alberola, José Manuel Civera, María Valls Reig, Marta Ruiz Hueso, Patricia Castro Carmona, Nerea Perez, and et al. 2025. "Low-Density Lipoprotein Cholesterol Reduction and Therapeutic Adherence During Cardiac Rehabilitation After Myocardial Infarction" Journal of Clinical Medicine 14, no. 12: 4242. https://doi.org/10.3390/jcm14124242
APA StyleBertolín-Boronat, C., Merenciano-González, H., Marcos-Garcés, V., Martínez Mas, M. L., Climent Alberola, J. I., Civera, J. M., Valls Reig, M., Ruiz Hueso, M., Castro Carmona, P., Perez, N., López-Bueno, L., Díaz Díaz, B., Miñano Martínez, I., Payá Rubio, A., Ríos-Navarro, C., de Dios, E., Gavara, J., Jiménez-Navarro, M. F., Sanchis, J., & Bodi, V. (2025). Low-Density Lipoprotein Cholesterol Reduction and Therapeutic Adherence During Cardiac Rehabilitation After Myocardial Infarction. Journal of Clinical Medicine, 14(12), 4242. https://doi.org/10.3390/jcm14124242