
Incidence of Sepsis-Induced Coagulopathy (INSIC) Trial: Study Protocol of a Combined Retrospective and Prospective, Multicenter, International, Cross-Sectional, Longitudinal, and Epidemiological Observational Trial
 ,
,  , , ,
, , ,  , ,
, , 
Abstract
1. Introduction
1.1. Objectives
1.2. Trial Design
2. Methods
2.1. Study Setting
2.2. Eligibility Criteria
- The patient must be treated in a participating ICU.
- The patient must be ≥18 years of age.
- The patient must be diagnosed with sepsis or septic shock [2]:
- Definition of sepsis: Acute suspected or confirmed infection plus a sepsis-induced increase in SOFA score by ≥2 points compared with baseline (last-documented value in the ICU or approximate baseline value in cases with known pre-existing conditions, e.g., documented SOFA impairment due to renal insufficiency, COPD, thrombocytopenia, or pre-existing brain damage). In cases where no pre-existing conditions are identified, the pre-existing SOFA score can be assumed to be “0”.
- Definition of septic shock: Sepsis plus persisting hypotension requiring vasopressors to maintain MAP ≥ 65 mm Hg plus lactate ≥ 2 mmol/L after an initial bolus volume of 30 mL/kg body weight (bw).
2.3. Interventions
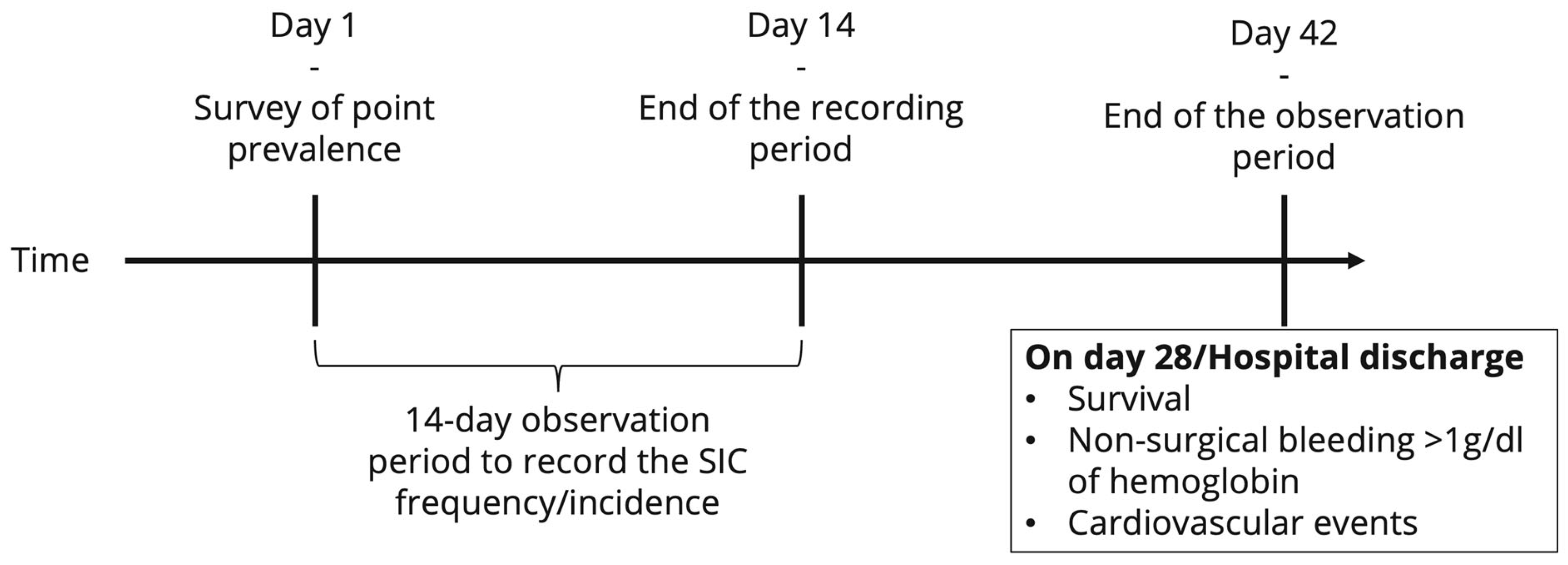
2.4. Outcomes
- (1)
- The incidence rate of SIC within a 14-day observation period (new cases/1000 patient days).
- (2)
- The point prevalence of SIC on day 1 of the study period and on three reference days in the 4th quarter of each year from 2019 to 2023.
- (1)
- Length of stay in the ICU until transfer to a normal ward.
- (2)
- ICU mortality rate (in all patients and in the subgroups of patients with sepsis, septic shock, SIC, or SAC (mild, moderate, severe) according to the different scores).
- (3)
- Mortality rate until day 28, hospital death, or hospital discharge (whatever occurs first, in all patients and in the subgroups of patients with sepsis, septic shock, SIC, or SAC (mild, moderate, severe) according to the different scores).
- (4)
- SIC and SAC (mild, moderate, severe) recovery rate 72 h after SIC or SAC onset. The time point was chosen as the 72 h period reflects a critical window during which early death in sepsis or a clinical response to sepsis therapy can be expected [15].
- (5)
- Thromboembolic events after sepsis onset (in sepsis, septic shock, SIC, or SAC (mild, moderate, severe)) up to day 28, death, or hospital discharge (whichever occurs first).
- (6)
- Relevant bleeding without surgical trauma (hemoglobin loss >1 g/dL within 24 h, due to bleeding rather than dilution) after sepsis onset (in sepsis, septic shock, SIC, or SAC (mild, moderate, severe)) until day 28, death, or hospital discharge (whichever occurs first).
2.5. Procedure and Data Collection
2.6. Evaluation of the Change in SIC Prevalence
2.7. Sample Size
2.8. Data Collection Methods
2.9. Data Management
2.10. Statistical Methods
2.11. Data Monitoring
2.12. Harms
2.13. Auditing
2.14. Ethics
2.15. Approval of the Institutional Review Board
2.16. Protocol Amendments
2.17. Consent or Assent
2.18. Confidentiality
3. Discussion
3.1. Justification for Enrolment of Participants Not Capable of Giving Consent
3.1.1. Trial Status
3.1.2. Trial Registration
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| AE | adverse event |
| aPTT | activated partial thromboplastin time |
| BDSG | Federal Data Protection Act |
| CNER | Comité National d’Ethique de Recherche |
| COPD | chronic obstructive pulmonary disease |
| CRP | C-reactive protein |
| DRKS | Deutsches Register Klinikscher Studien (German Clinical Trials Register) |
| DVT | deep vein thrombosis |
| eCRF | electronic case report form |
| F1.2 | thrombin fragment 1.2 |
| Hb | hemoglobin |
| ICU | intensive care unit |
| IL | interleukin |
| INR | international normalized ratio |
| INSIC | incidence of sepsis-induced coagulopathy |
| INSEP | incidence of severe sepsis and septic shock |
| IMISE | Institute for Medical Informatics, Statistics and Epidemiology |
| IU | international units |
| LAE | lung artery embolism |
| LBP | lipopolysaccharide-binding protein |
| MAP | mean arterial pressure |
| PCT | procalcitonin |
| PI | primary investigator |
| RBC | red blood cells |
| RCT | randomized controlled trial |
| SAE | serious adverse event |
| SAC | sepsis-associated coagulopathy |
| SIC | sepsis-induced coagulopathy |
| SOFA | sepsis-related organ failure assessment |
| TAT | thrombin–antithrombin complex |
| TC | thrombocyte concentrate |
References
- Foley Jonathan, H.; Conway Edward, M. Cross Talk Pathways Between Coagulation and Inflammation. Circ. Res. 2016, 118, 1392–1408. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Schmoch, T.; Weigand, M.; Möhnle, P.; Briegel, J.; Brenner, T. Sepsis-Induzierte Koagulopathie: Zu häufig Missachtete Komplikation der Sepsis. INTENSIV-News [Internet]. 2023. Available online: https://medicom.cc/de/publikationen/intensiv-news/202306/entries/03-Sepsis-induzierte-Koagulopathie.php (accessed on 8 June 2025).
- Iba, T.; Nisio, M.D.; Levy, J.H.; Kitamura, N.; Thachil, J. New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: A retrospective analysis of a nationwide survey. BMJ Open 2017, 7, e017046. [Google Scholar] [CrossRef] [PubMed]
- Taylor, F.B.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M.; Scientific Subcommittee on Disseminated Intravascular Coagulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH). Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef]
- Lyons, P.G.; Micek, S.T.; Hampton, N.; Kollef, M.H. Sepsis-Associated Coagulopathy Severity Predicts Hospital Mortality. Crit. Care Med. 2018, 46, 736–742. [Google Scholar] [CrossRef]
- Bloos, F.; Trips, E.; Nierhaus, A.; Briegel, J.; Heyland, D.K.; Jaschinski, U.; Moerer, O.; Weyland, A.; Marx, G.; Gründling, M.; et al. Effect of Sodium Selenite Administration and Procalcitonin-Guided Therapy on Mortality in Patients With Severe Sepsis or Septic Shock: A Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 1266–1276. [Google Scholar] [CrossRef]
- Keh, D.; Trips, E.; Marx, G.; Wirtz, S.P.; Abduljawwad, E.; Bercker, S.; Bogatsch, H.; Briegel, J.; Engel, C.; Gerlach, H.; et al. Effect of Hydrocortisone on Development of Shock Among Patients With Severe Sepsis: The HYPRESS Randomized Clinical Trial. JAMA 2016, 316, 1775–1785. [Google Scholar] [CrossRef]
- Schmoch, T.; Möhnle, P.; Weigand, M.A.; Briegel, J.; Bauer, M.; Bloos, F.; Meybohm, P.; Keh, D.; Löffler, M.; Elke, G.; et al. The prevalence of sepsis-induced coagulopathy in patients with sepsis—A secondary analysis of two German multicenter randomized controlled trials. Ann. Intensive Care 2023, 13, 3. [Google Scholar] [CrossRef]
- Tanaka, C.; Tagami, T.; Kudo, S.; Takehara, A.; Fukuda, R.; Nakayama, F.; Kaneko, J.; Ishiki, Y.; Sato, S.; Kuno, M.; et al. Validation of sepsis-induced coagulopathy score in critically ill patients with septic shock: Post hoc analysis of a nationwide multicenter observational study in Japan. Int. J. Hematol. 2021, 114, 164–171. [Google Scholar] [CrossRef]
- Helms, J.; Severac, F.; Merdji, H.; Clere-Jehl, R.; François, B.; Mercier, E.; Quenot, J.P.; Meziani, F.; CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). Performances of disseminated intravascular coagulation scoring systems in septic shock patients. Ann. Intensive Care 2020, 10, 92. [Google Scholar] [CrossRef]
- Marik, P.E. Drotrecogin alfa (activated) in severe sepsis. Lancet Infect. Dis. 2013, 13, 107. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Thompson, B.T.; Barie, P.S.; Dhainaut, J.F.; Douglas, I.S.; Finfer, S.; Gårdlund, B.; Marshall, J.C.; Rhodes, A.; Artigas, A.; et al. Drotrecogin Alfa (Activated) in Adults with Septic Shock. N. Engl. J. Med. 2012, 366, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Francois, B.; Zabolotskikh, I.; Daga, M.K.; Lascarrou, J.B.; Kirov, M.Y.; Pettilä, V.; Wittebole, X.; Meziani, F.; Mercier, E.; et al. Effect of a Recombinant Human Soluble Thrombomodulin on Mortality in Patients with Sepsis-Associated Coagulopathy: The SCARLET Randomized Clinical Trial. JAMA 2019, 321, 1993–2002. [Google Scholar] [CrossRef]
- Daviaud, F.; Grimaldi, D.; Dechartres, A.; Charpentier, J.; Geri, G.; Marin, N.; Chiche, J.D.; Cariou, A.; Mira, J.P.; Pène, F. Timing and causes of death in septic shock. Ann. Intensive Care 2015, 5, 16. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Doyle, D.J.; Goyal, A.; Garmon, E.H. American Society of Anesthesiologists Classification. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK441940/ (accessed on 1 June 2022).
- Ford, M.K.; Beattie, W.S.; Wijeysundera, D.N. Systematic review: Prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Ann. Intern. Med. 2010, 152, 26–35. [Google Scholar] [CrossRef]
- SepNet Critical Care Trials Group. Incidence of severe sepsis and septic shock in German intensive care units: The prospective, multicentre INSEP study. Intensive Care Med. 2016, 42, 1980–1989. [Google Scholar] [CrossRef]
- Saito, S.; Uchino, S.; Hayakawa, M.; Yamakawa, K.; Kudo, D.; Iizuka, Y.; Sanui, M.; Takimoto, K.; Mayumi, T.; Sasabuchi, Y. Epidemiology of disseminated intravascular coagulation in sepsis and validation of scoring systems. J. Crit. Care 2019, 50, 23–30. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. Available online: https://pubmed.ncbi.nlm.nih.gov/31078660/ (accessed on 14 October 2024). [CrossRef]
- Federal Law Gazette. Ordinance on the implementation of Good Clinical Practice in the conduct of clinical trials on medicinal products for use in humans (GCP Ordinance-GCP-V). Fed. Law Gaz. 2004, 2004, 19. [Google Scholar]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). ICH Official Web Site: ICH. 2021. Available online: https://www.ich.org/ (accessed on 6 February 2021).
- The World Medical Association (WMA). Declaration of Helsinki–Ethical Principles for Medical Research Involving Human Subjects. 2018. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 15 August 2019).
- The European Parliament and of the Council. General Data Protection Regulation (GDPR). Regulation (EU) 2016/679 of the European Parliament and of the Council. 27 April 2016. Available online: https://gdpr-info.eu (accessed on 8 June 2025).
- Peng, J.C.; Nie, F.; Li, Y.J.; Xu, Q.Y.; Xing, S.P.; Li, W.; Gao, Y. Favorable Outcomes of Anticoagulation With Unfractioned Heparin in Sepsis-Induced Coagulopathy: A Retrospective Analysis of MIMIC-III Database. Front. Med. 2022, 8, 773339. Available online: https://www.frontiersin.org/articles/10.3389/fmed.2021.773339 (accessed on 3 May 2023). [CrossRef] [PubMed]
- Yamakawa, K.; Umemura, Y.; Hayakawa, M.; Kudo, D.; Sanui, M.; Takahashi, H.; Yoshikawa, Y.; Hamasaki, T.; Fujimi, S. Benefit profile of anticoagulant therapy in sepsis: A nationwide multicentre registry in Japan. Crit. Care 2016, 20, 229. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Vincent, J.L.; Tanaka, K.; Radford, A.H.; Kayanoki, T.; Fineberg, D.A.; Hoppensteadt, D.; Fareed, J. Effect of a Recombinant Human Soluble Thrombomodulin on Baseline Coagulation Biomarker Levels and Mortality Outcome in Patients with Sepsis-Associated Coagulopathy. Crit. Care Med. 2020, 48, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Warren, B.L.; Eid, A.; Singer, P.; Pillay, S.S.; Carl, P.; Novak, I.; Chalupa, P.; Atherstone, A.; Pénzes, I.; Kübler, A.; et al. Caring for the critically ill patient. High-dose antithrombin III in severe sepsis: A randomized controlled trial. JAMA 2001, 286, 1869–1878. [Google Scholar] [CrossRef]
- Abraham, E.; Laterre, P.F.; Garg, R.; Levy, H.; Talwar, D.; Trzaskoma, B.L.; François, B.; Guy, J.S.; Brückmann, M.; Rea-Neto, Á.; et al. Drotrecogin Alfa (Activated) for Adults with Severe Sepsis and a Low Risk of Death. N. Engl. J. Med. 2005, 353, 1332–1341. [Google Scholar] [CrossRef]
- Tsuchida, T.; Makino, Y.; Wada, T.; Ushio, N.; Totoki, T.; Fujie, N.; Yasuo, S.; Matsuoka, T.; Koami, H.; Yamakawa, K.; et al. Efficacy of antithrombin administration for patients with sepsis: A systematic review, meta-analysis, and meta-regression. Acute Med. Surg. 2024, 11, e950. [Google Scholar] [CrossRef]
- Ding, R.; Wang, Z.; Lin, Y.; Liu, B.; Zhang, Z.; Ma, X. Comparison of a new criteria for sepsis-induced coagulopathy and International Society on Thrombosis and Haemostasis disseminated intravascular coagulation score in critically ill patients with sepsis 3.0: A retrospective study. Blood Coagul Fibrinolysis 2018, 29, 551–558. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 49, e1063–e1143. [Google Scholar]


{kind=link}
{kind=link}
| SIC Score Iba et al. [4] | SAC Score Lyons et al. [6] | ||
|---|---|---|---|
| Points | |||
| Platelet count SIC subscore (PSSC) (platelet count (PLC) [1/nL] | >150/nL | 0 | Mild SAC 1.2 ≤ INR < 1.4 and 100 > PLC ≤ 150 |
| 100 to <150/nL | 1 | ||
| <100/nL | 2 | ||
| International Normalized Ratio (INR) SIC subscore (ISSC) [ ] | 0 | ||
| ≥1.2 to <1.4 | 1 | ||
| ≥1.4 | 2 | ||
| SOFA subscore (truncated SOFA score, including the respiratory, cardiocirculatory, hepatic, and renal subscore) [Points] | 0 | 0 | |
| 1 | 1 | ||
| ≥2 | 2 | Moderate SAC: 1.4 ≤ INR < 1.6 or 80 ≥ PLC ≤ 100; | |
| No SIC | <4 points | Severe SAC INR ≥ 1.6 or PLC < 80 | |
| SIC | ≥4 points (with PT-INR plus platelet count exceeding 2) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmoch, T.; Möhnle, P.; Weigand, M.A.; Dietrich, M.; Gregorius, J.; Frank, S.; Briegel, J.; Radke, D.I.; Bauer, M.; Bloos, F.; et al. Incidence of Sepsis-Induced Coagulopathy (INSIC) Trial: Study Protocol of a Combined Retrospective and Prospective, Multicenter, International, Cross-Sectional, Longitudinal, and Epidemiological Observational Trial. J. Clin. Med. 2025, 14, 4222. https://doi.org/10.3390/jcm14124222
Schmoch T, Möhnle P, Weigand MA, Dietrich M, Gregorius J, Frank S, Briegel J, Radke DI, Bauer M, Bloos F, et al. Incidence of Sepsis-Induced Coagulopathy (INSIC) Trial: Study Protocol of a Combined Retrospective and Prospective, Multicenter, International, Cross-Sectional, Longitudinal, and Epidemiological Observational Trial. Journal of Clinical Medicine. 2025; 14(12):4222. https://doi.org/10.3390/jcm14124222
Chicago/Turabian StyleSchmoch, Thomas, Patrick Möhnle, Markus A. Weigand, Maximilian Dietrich, Jonas Gregorius, Sandra Frank, Josef Briegel, David I. Radke, Michael Bauer, Frank Bloos, and et al. 2025. "Incidence of Sepsis-Induced Coagulopathy (INSIC) Trial: Study Protocol of a Combined Retrospective and Prospective, Multicenter, International, Cross-Sectional, Longitudinal, and Epidemiological Observational Trial" Journal of Clinical Medicine 14, no. 12: 4222. https://doi.org/10.3390/jcm14124222
APA StyleSchmoch, T., Möhnle, P., Weigand, M. A., Dietrich, M., Gregorius, J., Frank, S., Briegel, J., Radke, D. I., Bauer, M., Bloos, F., Meybohm, P., Bogatsch, H., & Brenner, T., on behalf of the SepNet Critical Care Trials Group. (2025). Incidence of Sepsis-Induced Coagulopathy (INSIC) Trial: Study Protocol of a Combined Retrospective and Prospective, Multicenter, International, Cross-Sectional, Longitudinal, and Epidemiological Observational Trial. Journal of Clinical Medicine, 14(12), 4222. https://doi.org/10.3390/jcm14124222