
Association Between Endogenous Equol Production and the Onset of Overactive Bladder in Postmenopausal Women

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
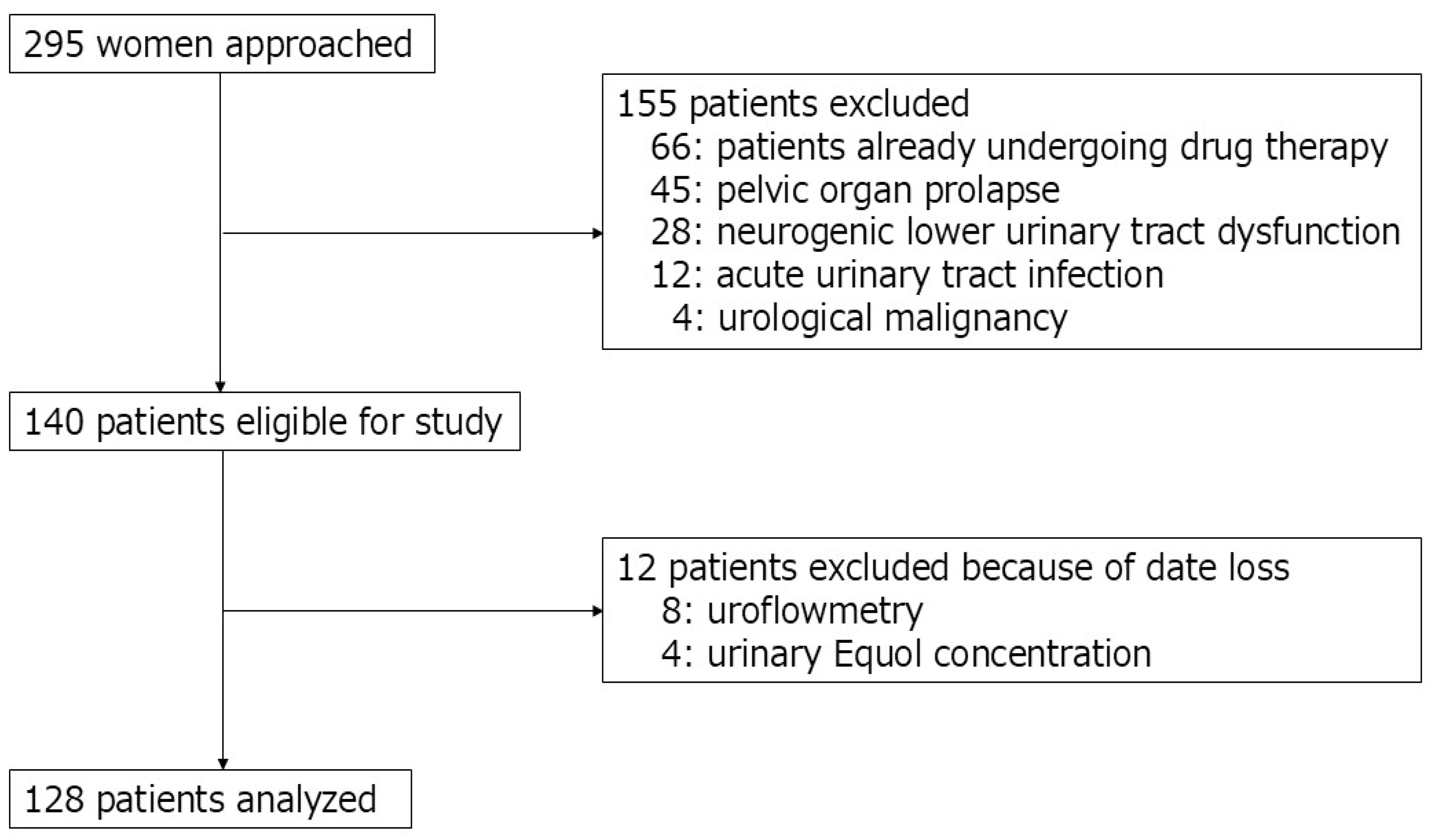
2.2. Patients and Study Design
2.3. Urinary Sample Preparation and Assessment
2.4. Statistical Analysis
2.5. Propensity Score Matching
3. Results
3.1. Differences in Patient Characteristics
3.2. Differences in Urological Parameters
3.3. The Relationship Between the Ability to Produce Equol and the Onset Time of LUTS
3.4. Equol Production Capacity and Factors Associated with the Onset of OAB Based on the Time of Diagnosis
3.5. Correlation Between Urinary Equol Level and Patients’ Backgrounds and Urological Symptoms
3.6. Predictive Factors for Early-Onset LUTS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OAB | overactive bladder |
| OABSS | overactive bladder symptom score |
| LUTS | lower urinary tract symptom |
| ERs | estrogen receptors |
| Q | question |
| P | equol-producing |
| NP | equol-non-producing |
| VV | voided volume |
| Qmax | maximum flow rate |
| PVR | post-void residual urine volume |
| ELISA | enzyme-linked immunosorbent assay |
| ER-β | estrogen receptor beta |
| HRT | hormone replacement therapy |
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; van Kerrebroeck, P.; Victor, A.; Wein, A.; Standardisation Sub-Committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the standardisation sub-committee of the international continence society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Qudah, S.; Abufaraj, M.; Farah, R.; Almazeedi, A.; Ababneh, A.; Alnabulsi, M.; Qatawneh, A.; Hyassat, D.; Ajlouni, K. The prevalence of overactive bladder and its impact on the quality of life: A cross-sectional study. Arab J. Urol. 2024, 22, 39–47. [Google Scholar] [CrossRef]
- Mitsui, T.; Sekido, N.; Masumori, N.; Haga, N.; Omae, K.; Saito, M.; Kubota, Y.; Sakakibara, R.; Yoshida, M.; Takahashi, S. Prevalence and impact on daily life of lower urinary tract symptoms in Japan: Results of the 2023 Japan Community Health Survey (JaCS 2023). Int. J. Urol. 2024, 31, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Angelou, K.; Grigoriadis, T.; Diakosavvas, M.; Zacharakis, D.; Athanasiou, S. The genitourinary syndrome of menopause: An overview of the recent data. Cureus 2020, 12, e7586. [Google Scholar] [CrossRef]
- Ramezani Tehrani, F.; Mousavi, M.; Saei Ghare Naz, M.; Noroozzadeh, M.; Azizi, F.; Farahmand, M. Endogenous estrogen exposure and hypertension risk; A population-based cohort study with about 2 decades of follow-up. J. Clin. Endocrinol. Metab. 2025, 110, e1125–e1133. [Google Scholar] [CrossRef]
- Baruch, Y.; Torella, M.; De Bastiani, S.; Meschia, M.; Candiani, M.; Colacurci, N.; Salvatore, S. Pre- versus post-Menopausal Onset of overactive bladder and the Response to Vaginal estrogen Therapy: A Prospective Study. Medicina 2023, 59, 245. [Google Scholar] [CrossRef]
- Gold, E.B. The timing of the age at which natural menopause occurs. Obstet. Gynecol. Clin. N. Am. 2011, 38, 425–440. [Google Scholar] [CrossRef]
- Gong, Y.; Lv, J.; Pang, X.; Zhang, S.; Zhang, G.; Liu, L.; Wang, Y.; Li, C. Advances in the metabolic mechanism and functional characteristics of equol. Foods 2023, 12, 2334. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhang, Y.; Li, J.; Tang, J.; Wu, J.; Xie, Z.; Huang, X.; Tao, S.; Xue, T. Identification of metabolites from the gut microbiota in hypertension via network pharmacology and molecular docking. Bioresour. Bioprocess. 2024, 11, 102. [Google Scholar] [CrossRef]
- Cheong, S.H.; Furuhashi, K.; Ito, K.; Nagaoka, M.; Yonezawa, T.; Miura, Y.; Yagasaki, K. Antihyperglycemic effect of equol, a daidzein derivative, in cultured L6 myocytes and ob/ob mice. Mol. Nutr. Food Res. 2014, 58, 267–277. [Google Scholar] [CrossRef]
- Yoshikata, R.; Myint, K.Z.Y.; Ohta, H.; Ishigaki, Y. Effects of an equol-containing supplement on advanced glycation end products, visceral fat and climacteric symptoms in postmenopausal women: A randomized controlled trial. PLoS ONE 2021, 16, e0257332. [Google Scholar] [CrossRef] [PubMed]
- Homma, Y.; Yoshida, M.; Seki, N.; Yokoyama, O.; Kakizaki, H.; Gotoh, M.; Yamanishi, T.; Yamaguchi, O.; Takeda, M.; Nishizawa, O. Symptom assessment tool for overactive bladder syndrome-overactive bladder symptom score. Urology 2006, 68, 318–323. [Google Scholar] [CrossRef]
- Igase, M.; Igase, K.; Tabara, Y.; Ohyagi, Y.; Kohara, K. Cross-sectional study of equol producer status and cognitive impairment in older adults. Geriatr. Gerontol. Int. 2017, 17, 2103–2108. [Google Scholar] [CrossRef]
- Takeda, T.; Shiina, M.; Chiba, Y. Effectiveness of natural S-equol supplement for premenstrual symptoms: Protocol of a randomised, double-blind, placebo-controlled trial. BMJ Open 2018, 8, e023314. [Google Scholar] [CrossRef]
- Setchell, K.D.R.; Clerici, C. Equol: History, chemistry, and formation. J. Nutr. 2010, 140, 1355S–1362S. [Google Scholar] [CrossRef] [PubMed]
- Setchell, K.D.R.; Brown, N.M.; Lydeking-Olsen, E. The clinical importance of the metabolite equol—A clue to the effectiveness of soy and its isoflavones. J. Nutr. 2002, 132, 3577–3584. [Google Scholar] [CrossRef]
- Yuan, J.P.; Wang, J.H.; Liu, X. Metabolism of dietary soy isoflavones to equol by human intestinal microflora—Implications for health. Mol. Nutr. Food Res. 2007, 51, 765–781. [Google Scholar] [CrossRef]
- Robinson, D.; Cardozo, L.D. The role of estrogens in female lower urinary tract dysfunction. Urology 2003, 62 (Supp. S1), 45–51. [Google Scholar] [CrossRef] [PubMed]
- Ishiwata, N.; Melby, M.K.; Mizuno, S.; Watanabe, S. New equol supplement for relieving menopausal symptoms: Randomized, placebo-controlled trial of Japanese women. Menopause 2009, 16, 141–148. [Google Scholar] [CrossRef]
- Uesugi, S.; Watanabe, S.; Ishiwata, N.; Uehara, M.; Ouchi, K. Effects of isoflavone supplements on bone metabolic markers and climacteric symptoms in Japanese women. BioFactors 2004, 22, 221–228. [Google Scholar] [CrossRef]
- Temml, C.; Heidler, S.; Ponholzer, A.; Madersbacher, S. Prevalence of the overactive bladder syndrome by applying the International Continence Society definition. Eur. Urol. 2005, 48, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.L.; Jackson, E.A.; Churchill, L.; Lampe, J.W.; Leung, K.; Ockene, J.K. Impact of dose, frequency of administration, and equol production on efficacy of isoflavones for menopausal hot flashes: A pilot randomized trial. Menopause 2013, 20, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Oka, J.; Ezaki, J.; Ohtomo, T.; Ueno, T.; Uchiyama, S.; Toda, T.; Uehara, M.; Ishimi, Y. Possible role of equol status in the effects of isoflavone on bone and fat mass in postmenopausal Japanese women: A double-blind, randomized, controlled trial. Menopause 2007, 14, 866–874. [Google Scholar] [CrossRef]
- Fan, W.; Ding, C.; Liu, S.; Gao, X.; Shen, X.; De Boevre, M.; Gao, Z.; Li, M.; Zhang, S.; Miao, Y.; et al. Estrogen receptor β activation inhibits colitis by promoting NLRP6-mediated autophagy. Cell Rep. 2022, 41, 111454. [Google Scholar] [CrossRef]
- Cvoro, A.; Tatomer, D.; Tee, M.K.; Zogovic, T.; Harris, H.A.; Leitman, D.C. Selective estrogen receptor-β agonists repress transcription of proinflammatory genes. J. Immunol. 2008, 180, 630–636. [Google Scholar] [CrossRef]
- Yang, X.; Li, Y.Z.; Mao, Z.; Gu, P.; Shang, M. Effects of estrogen and tibolone on bladder histology and estrogen receptors in rats. Chin. Med. J. 2009, 122, 381–385. [Google Scholar] [CrossRef]
- Sánchez-Ortiz, R.F.; Wang, Z.; Menon, C.; DiSanto, M.E.; Wein, A.J.; Chacko, S. Estrogen modulates the expression of myosin heavy chain in detrusor smooth muscle. Am. J. Physiol. Cell Physiol. 2001, 280, C433–C440. [Google Scholar] [CrossRef]
- Russo, E.; Misasi, G.; Montt-Guevara, M.M.; Giannini, A.; Simoncini, T. Effects of ospemifene on overactive bladder in postmenopausal women with vulvovaginal atrophy. Climacteric 2023, 26, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Setchell, K.D.R.; Clerici, C.; Lephart, E.D.; Cole, S.J.; Heenan, C.; Castellani, D.; Wolfe, B.E.; Nechemias-Zimmer, L.; Brown, N.M.; Lund, T.D.; et al. S-equol, a potent ligand for estrogen receptor β, is the exclusive enantiomeric form of the soy isoflavone metabolite produced by human intestinal bacterial flora. Am. J. Clin. Nutr. 2005, 81, 1072–1079. [Google Scholar] [CrossRef]
- Oñate, F.P.; Chamignon, C.; Burz, S.D.; Lapaque, N.; Monnoye, M.; Philippe, C.; Bredel, M.; Chêne, L.; Farin, W.; Paillarse, J.M.; et al. Adlercreutzia equolifaciens is an anti-inflammatory commensal bacterium with decreased abundance in gut microbiota of patients with metabolic liver disease. Int. J. Mol. Sci. 2023, 24, 12232. [Google Scholar] [CrossRef]
- Ghimire, S.; Cady, N.M.; Lehman, P.; Peterson, S.R.; Shahi, S.K.; Rashid, F.; Giri, S.; Mangalam, A.K. Dietary isoflavones alter gut microbiota and lipopolysaccharide biosynthesis to reduce inflammation. Gut Microbes 2022, 14, 2127446. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Entire | P Group | NP Group | p Value | |
|---|---|---|---|---|
| Number of patients (%) | 128 (100) | 59 (46.1) | 69 (53.9) | - |
| Age (years) | 71.6 ± 10.3 | 73.2 ± 9.8 | 70.2 ± 10.6 | 0.094 |
| Age of onset of LUTS (years) | 65.5 ± 11.2 | 68.7 ± 10.9 | 62.7 ± 10.7 | 0.002 |
| Urinary equol concentration (μmol/L) | 11.7 ± 38.2 | 37.4 ± 176.4 | 0.2 ± 0.3 | <0.001 |
| Hypertension (%) | 64 (50.0) | 36 (61.0) | 28 (40.6) | 0.033 |
| Diabetes mellitus (%) | 23 (18.0) | 13 (22.0) | 10 (14.5) | 0.356 |
| Dyslipidemia (%) | 34 (26.6) | 17 (28.8) | 17 (24.6) | 0.689 |
| Chronic kidney disease (%) | 47 (36.7) | 18 (30.5) | 29 (42.0) | 0.201 |
| Subjective symptoms (OABSS) | ||||
| Q1. Daytime frequency | 1.0 ± 0.6 | 1.0 ± 0.6 | 1.0 ± 0.6 | 0.930 |
| Q2. Nocturia | 1.9 ± 1.0 | 1.9 ± 1.0 | 1.9 ± 1.1 | 0.958 |
| Q3. Urgency | 3.3 ± 1.1 | 3.2 ± 1.1 | 3.5 ± 1.1 | 0.104 |
| Q4. Urgency incontinence | 2.2 ± 1.8 | 2.08 ± 1.7 | 2.2 ± 1.9 | 0.711 |
| Total OABSS | 8.4 ± 3.0 | 8.2 ± 3.0 | 8.6 ± 3.1 | 0.429 |
| Severity of OAB | 0.845 | |||
| Mild (%) | 13 (15.5) | 10 (16.9) | 14 (20.3) | |
| Moderate (%) | 42 (50.0) | 39 (66.1) | 42 (60.9) | |
| Severe (%) | 29 (34.5) | 10 (16.9) | 13 (18.8) | |
| Objective findings | ||||
| Voided volume (mL) | 219.9 ± 131.0 | 201.4 ± 118.8 | 236.7 ± 140.4 | 0.231 |
| Maximum flow rate (mL/s) | 21.0 ± 12.4 | 20.3 ± 12.3 | 21.7 ± 12.6 | 0.610 |
| Post-void residual urine (mL) | 35.6 ± 36.0 | 23.4 ± 33.2 | 27.7 ± 38.8 | 0.577 |
| Early-Onset | Late-Onset | p Value | |
|---|---|---|---|
| Number of patients (%) | 58 (45.3) | 70 (54.7) | - |
| Equol producing (%) | 18 (31.0) | 41 (58.6) | 0.002 |
| Age at diagnosis of OAB (years) | 68.7 ± 9.0 | 78.1 ± 5.7 | <0.001 |
| Age of onset of LUTS (years) | 55.3 ± 6.6 | 73.9 ± 5.8 | <0.001 |
| Urinary equol concentration (μmol/L) | 3.6 ± 8.5 | 29.3 ± 163.8 | 0.014 |
| Hypertension (%) | 24 (41.4) | 40 (57.1) | 0.110 |
| Diabetes mellitus (%) | 11 (19.0) | 12 (17.1) | 0.820 |
| Dyslipidemia (%) | 12 (20.7) | 22 (31.4) | 0.228 |
| Chronic kidney disease (%) | 21 (36.2) | 26 (37.1) | >0.999 |
| Subjective symptoms (OABSS) | |||
| Q1. Daytime frequency | 1.0 ± 0.6 | 0.9 ± 0.6 | 0.342 |
| Q2. Nocturia | 1.7 ± 1.1 | 2.1 ± 1.0 | 0.052 |
| Q3. Urgency | 3.3 ± 1.1 | 3.3 ± 1.2 | 0.996 |
| Q4. Urgency incontinence | 1.9 ± 1.8 | 2.4 ± 1.8 | 0.148 |
| Total OABSS | 8.0 ± 2.9 | 8.7 ± 3.1 | 0.175 |
| Severity of OAB | 0.159 | ||
| Mild (%) | 14 (24.1) | 10 (14.3) | |
| Moderate (%) | 37 (63.8) | 44 (62.9) | |
| Severe (%) | 7 (12.1) | 16 (22.9) | |
| Objective findings | |||
| Voided volume (mL) | 222.3 ± 136.7 | 217.8 ± 127.5 | 0.880 |
| Maximum flow rate (mL/s) | 21.2 ± 11.7 | 20.8 ± 13.1 | 0.906 |
| Post-void residual urine (mL) | 17.5 ± 29.0 | 32.5 ± 40.1 | 0.048 |
| Early-Onset | Late-Onset | |||||
|---|---|---|---|---|---|---|
| P Group | NP Group | p Value | P Group | NP Group | p Value | |
| Number of patients (%) | 18 (31.0) | 40 (69.0) | - | 41 (58.6) | 29 (41.4) | - |
| Age (years) | 62.2 ± 8.1 | 64.4 ± 9.4 | 0.400 | 78.1 ± 5.7 | 78.1 ± 6.0 | 0.963 |
| Age of onset of LUTS (years) | 55.1 ± 6.0 | 55.4 ± 6.7 | 0.866 | 74.7 ± 6.0 | 72.8 ± 5.5 | 0.171 |
| Urinary equol concentration (μmol/L) | 10.7 ± 12.2 | 0.2 ± 0.3 | <0.001 | 49.2 ± 211.2 | 0.2 ± 0.2 | <0.001 |
| Hypertension (%) | 11 (61.1) | 13 (32.5) | 0.049 | 25 (61.0) | 15 (51.7) | 0.472 |
| Diabetes mellitus (%) | 5 (27.8) | 6 (15.0) | 0.290 | 8 (19.5) | 4 (13.8) | 0.749 |
| Dyslipidemia (%) | 5 (27.8) | 7 (17.5) | 0.486 | 12 (29.3) | 10 (34.5) | 0.794 |
| Chronic kidney disease (%) | 3 (16.7) | 18 (45.0) | 0.044 | 15 (36.6) | 11 (37.9) | 1.000 |
| Subjective symptoms (OABSS) | ||||||
| Q1. Daytime frequency | 1.1 ± 0.5 | 1.0 ± 0.6 | 0.750 | 0.9 ± 0.7 | 0.9 ± 0.6 | 0.839 |
| Q2. Nocturia | 1.6 ± 1.0 | 1.8 ± 1.1 | 0.544 | 2.1 ± 1.0 | 2.1 ± 1.0 | 0.788 |
| Q3. Urgency | 3.0 ± 0.9 | 3.5 ± 1.1 | 0.123 | 3.2 ± 1.2 | 3.5 ± 1.1 | 0.360 |
| Q4. Urgency incontinence | 1.4 ± 1.4 | 2.1 ± 1.9 | 0.201 | 2.4 ± 1.7 | 2.3 ± 1.9 | 0.961 |
| Total OABSS | 7.1 ± 2.0 | 8.4 ± 3.2 | 0.127 | 8.6 ± 3.3 | 8.9 ± 2.9 | 0.741 |
| Severity of OAB | 0.649 | 1.000 | ||||
| Mild (%) | 4 (22.2) | 10 (25.0) | 6 (14.6) | 4 (13.8) | ||
| Moderate (%) | 13 (72.2) | 24 (60.0) | 26 (63.4) | 18 (62.1) | ||
| Severe (%) | 1 (5.6) | 6 (15.0) | 9 (22.0) | 7 (24.1) | ||
| Objective findings | ||||||
| Voided volume (mL) | 193.1 ± 100.2 | 236.3 ± 151.0 | 0.376 | 205.1 ± 128.2 | 237.2 ± 127.8 | 0.426 |
| Maximum flow rate (mL/s) | 16.8 ± 4.9 | 23.3 ± 13.4 | 0.089 | 21.9 ± 14.2 | 43.4 ± 48.2 | 0.467 |
| Post-void residual volume (mL) | 17.5 ± 32.4 | 17.5 ± 27.9 | 0.819 | 26.1 ± 33.8 | 43.4 ± 48.2 | 0.147 |
| r | 95% CI | p Value | |
|---|---|---|---|
| Age (years) | 0.062 | −0.116–0.236 | 0.495 |
| Age of onset of LUTS (years) | 0.043 | −0.135–0.217 | 0.637 |
| Subjective symptoms (OABSS) | |||
| Q1. Daytime frequency | −0.006 | −0.183–0.170 | 0.943 |
| Q2. Nocturia | 0.109 | −0.069–0.280 | 0.228 |
| Q3. Urgency | 0.137 | −0.041–0.306 | 0.130 |
| Q4. Urgency incontinence | −0.088 | −0.260–0.090 | 0.332 |
| Total OABSS | 0.035 | −0.142–0.210 | 0.696 |
| Objective findings | |||
| Voided volume (mL) | 0.211 | −0.012–0.414 | 0.063 |
| Maximum flow rate (mL/s) | 0.106 | −0.106–0.308 | 0.327 |
| Post-void residual urine (mL) | −0.007 | −0.215–0.202 | 0.951 |
| Univariate Analysis | |||
|---|---|---|---|
| OR | 95% CI | p Value | |
| Hypertension | 1.890 | 0.933–3.820 | 0.077 |
| Diabetes mellitus | 0.884 | 0.358–2.180 | 0.789 |
| Dyslipidemia | 1.760 | 0.781–3.950 | 0.173 |
| Chronic kidney disease | 1.040 | 0.506–2.140 | 0.913 |
| Equol production | 3.140 | 1.610–6.530 | 0.002 |
| Early-Onset | Late-Onset | p Value | Standardized Mean Differences | |
|---|---|---|---|---|
| Hypertension (%) | 24 (46.2) | 23 (44.4) | >0.999 | 0.019 |
| Diabetes mellitus (%) | 6 (11.5) | 6 (11.5) | >0.999 | 0.011 |
| Dyslipidemia (%) | 12 (23.1) | 13 (25.0) | >0.999 | 0.017 |
| Chronic kidney disease (%) | 18 (34.6) | 19 (36.5) | >0.999 | 0.015 |
| Early-Onset N = 52 | Late-Onset N = 52 | p Value | |
|---|---|---|---|
| Equol production; positive (%) | 16 (30.8) | 24 (46.2) | 0.014 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Honda, H.; Matsuo, T.; Ito, H.; Kakita, S.; Mori, S.; Araki, K.; Mitsunari, K.; Ohba, K.; Mochizuki, Y.; Imamura, R. Association Between Endogenous Equol Production and the Onset of Overactive Bladder in Postmenopausal Women. J. Clin. Med. 2025, 14, 4183. https://doi.org/10.3390/jcm14124183
Honda H, Matsuo T, Ito H, Kakita S, Mori S, Araki K, Mitsunari K, Ohba K, Mochizuki Y, Imamura R. Association Between Endogenous Equol Production and the Onset of Overactive Bladder in Postmenopausal Women. Journal of Clinical Medicine. 2025; 14(12):4183. https://doi.org/10.3390/jcm14124183
Chicago/Turabian StyleHonda, Hiroyuki, Tomohiro Matsuo, Hidenori Ito, Shota Kakita, Shintaro Mori, Kyohei Araki, Kensuke Mitsunari, Kojiro Ohba, Yasushi Mochizuki, and Ryoichi Imamura. 2025. "Association Between Endogenous Equol Production and the Onset of Overactive Bladder in Postmenopausal Women" Journal of Clinical Medicine 14, no. 12: 4183. https://doi.org/10.3390/jcm14124183
APA StyleHonda, H., Matsuo, T., Ito, H., Kakita, S., Mori, S., Araki, K., Mitsunari, K., Ohba, K., Mochizuki, Y., & Imamura, R. (2025). Association Between Endogenous Equol Production and the Onset of Overactive Bladder in Postmenopausal Women. Journal of Clinical Medicine, 14(12), 4183. https://doi.org/10.3390/jcm14124183