
Pelvic Floor Rehabilitation After Prostatectomy: Baseline Severity as a Predictor of Improvement—A Prospective Cohort Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Rehabilitation Protocol
2.2. Detailed First Session Procedure
- (1)
- Five fast contractions with immediate relaxation.
- (2)
- Five 10-s contractions with 5-s interval.
- (3)
- One 30-s contraction.
- (4)
- Ejection of probe, electrode detachment.
- (5)
- Evaluation and feedback.
- -
- Stage I: 2–10 g
- -
- Stage II: 11–50 g
- -
- Stage III: ≥50 g.
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Physiotherapy Effectiveness by Urinary Incontinence Severity
4.2. Demographic and Clinical Factors
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gacci, M.; De Nunzio, C.; Sakalis, V.; Rieken, M.; Cornu, J.-N.; Gravas, S. Latest Evidence on Post-Prostatectomy Urinary Incontinence. J. Clin. Med. 2023, 12, 1190. [Google Scholar] [CrossRef] [PubMed]
- Averbeck, M.A.; Woodhouse, C.; Comiter, C.; Bruschini, H.; Hanus, T.; Herschorn, S.; Goldman, H.B. Surgical Treatment of Post-Prostatectomy Stress Urinary Incontinence in Adult Men: Report from the 6th International Consultation on Incontinence. Neurourol. Urodyn. 2019, 38, 398–406. [Google Scholar] [CrossRef]
- Mungovan, S.F.; Carlsson, S.V.; Gass, G.C.; Graham, P.L.; Sandhu, J.S.; Akin, O.; Scardino, P.T.; Eastham, J.A.; Patel, M.I. Preoperative Exercise Interventions to Optimize Continence Outcomes Following Radical Prostatectomy. Nat. Rev. Urol. 2021, 18, 259–281. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.J.; Kim, H.J.; Kim, J.H.; Oh, J.J.; Lee, S.C.; Jeong, C.W.; Yoon, C.Y.; Hong, S.K.; Byun, S.-S.; Lee, S.E. Urinary Continence after Radical Prostatectomy: Predictive Factors of Recovery after 1 Year of Surgery. Int. J. Urol. 2012, 19, 1091–1098. [Google Scholar] [CrossRef]
- Rangganata, E.; Rahardjo, H.E. The Effect of Preoperative Pelvic Floor Muscle Training on Incontinence Problems after Radical Prostatectomy: A Meta-Analysis. Urol. J. 2021, 18, 380–388. [Google Scholar] [CrossRef]
- Litwin, M.S.; Melmed, G.Y.; Nakazon, T. Life after radical prostatectomy: A longitudinal study. J. Urol. 2001, 166, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.A.; Omar, M.I.; Campbell, S.E.; Hunter, K.F.; Cody, J.D.; Glazener, C.M.A. Conservative Management for Postprostatectomy Urinary Incontinence. Cochrane Database Syst. Rev. 2015, 1, CD001843. [Google Scholar] [CrossRef]
- Canning, A.; Raison, N.; Aydin, A.; Cheikh Youssef, S.; Khan, S.; Dasgupta, P.; Ahmed, K. A Systematic Review of Treatment Options for Post-Prostatectomy Incontinence. World J. Urol. 2022, 40, 2617–2626. [Google Scholar] [CrossRef]
- Farraj, H.; Alriyalat, S. Urinary Incontinence Following Robotic-Assisted Radical Prostatectomy: A Literature Review. Cureus 2024, 16, e53058. [Google Scholar] [CrossRef]
- Geng, E.; Yin, S.; Yang, Y.; Ke, C.; Fang, K.; Liu, J.; Wang, D. The Effect of Perioperative Pelvic Floor Muscle Exercise on Urinary Incontinence after Radical Prostatectomy: A Meta-Analysis. Int. Braz. J. Urol. 2023, 49, 441–451. [Google Scholar] [CrossRef]
- Gu, J.; Chen, H.; Gao, C.; Ren, P.; Lu, X.; Cao, J. Clinical Efficacy of a Rehabilitation Management Protocol for Urinary Incontinence after Robot-Assisted Laparoscopic Prostatectomy. Support. Care Cancer 2024, 32, 653. [Google Scholar] [CrossRef] [PubMed]
- Burkhard, F.C.; Nambiar, A.K.; Thiruchelvam, N.; Tubaro, A.; Lombardo, R.; Schneider, M.P. EAU Guidelines on Urinary Incontinence; EAU Guidelines; European Association of Urology: Arnhem, The Netherlands, 2018; ISBN 978-94-92671-01-1. [Google Scholar]
- Lucas, M.G.; Bosch, R.J.L.; Burkhard, F.C.; Cruz, F.; Madden, T.B.; Nambiar, A.K.; Neisius, A.; de Ridder, D.J.M.K.; Tubaro, A.; Turner, W.H.; et al. EAU Guidelines on Assessment and Nonsurgical Management of Urinary Incontinence. Eur. Urol. 2012, 62, 1130–1142. [Google Scholar] [CrossRef] [PubMed]
- Baumann, F.T.; Reimer, N.; Gockeln, T.; Reike, A.; Hallek, M.; Ricci, C.; Zopf, E.M.; Schmid, D.; Taaffe, D.; Newton, R.U.; et al. Supervised Pelvic Floor Muscle Exercise Is More Effective than Unsupervised Pelvic Floor Muscle Exercise at Improving Urinary Incontinence in Prostate Cancer Patients Following Radical Prostatectomy—A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2022, 44, 5374–5385. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, J.S.; Breyer, B.; Comiter, C.; Eastham, J.A.; Gomez, C.; Kirages, D.J.; Kittle, C.; Lucioni, A.; Nitti, V.W.; Stoffel, J.T.; et al. Incontinence after Prostate Treatment: AUA/SUFU Guideline. J. Urol. 2019, 202, 369–378. [Google Scholar] [CrossRef]
- Soto González, M.; Da Cuña Carrera, I.; Gutiérrez Nieto, M.; López García, S.; Ojea Calvo, A.; Lantarón Caeiro, E.M. Early 3-Month Treatment with Comprehensive Physical Therapy Program Restores Continence in Urinary Incontinence Patients after Radical Prostatectomy: A Randomized Controlled Trial. Neurourol. Urodyn. 2020, 39, 1529–1537. [Google Scholar] [CrossRef]
- Chen, G.-D.; Lin, T.-L.; Hu, S.-W.; Chen, Y.-C.; Lin, L.-Y. Prevalence and Correlation of Urinary Incontinence and Overactive Bladder in Taiwanese Women. Neurourol. Urodyn. 2003, 22, 109–117. [Google Scholar] [CrossRef]
- Szczygielska, D.; Knapik, A.; Pop, T.; Rottermund, J.; Saulicz, E. The Effectiveness of Pelvic Floor Muscle Training in Men after Radical Prostatectomy Measured with the Insert Test. Int. J. Environ. Res. Public Health 2022, 19, 2890. [Google Scholar] [CrossRef]
- Tillier, C.N.; Vromans, R.D.; Boekhout, A.H.; Veerman, H.; Wollersheim, B.M.; van Muilekom, H.A.M.; Boellaard, T.N.; van Leeuwen, P.J.; van de Poll-Franse, L.V.; van der Poel, H.G. Individual Risk Prediction of Urinary Incontinence after Prostatectomy and Impact on Treatment Choice in Patients with Localized Prostate Cancer. Neurourol. Urodyn. 2021, 40, 1550–1558. [Google Scholar] [CrossRef]
- Mata, L.R.F.D.; Azevedo, C.; Izidoro, L.C.D.R.; Ferreira, D.F.; Estevam, F.E.B.; Amaral, F.M.A.; Chianca, T.C.M. Prevalence and Severity Levels of Post-Radical Prostatectomy Incontinence: Different Assessment Instruments. Rev. Bras. Enferm. 2021, 74, e20200692. [Google Scholar] [CrossRef]
- Kurimura, Y.; Haga, N.; Yanagida, T.; Tanji, R.; Onagi, A.; Honda, R.; Matsuoka, K.; Hoshi, S.; Hata, J.; Onoda, M.; et al. The Preoperative Pad Test as a Predictor of Urinary Incontinence and Quality of Life after Robot-Assisted Radical Prostatectomy: A Prospective, Observational, Clinical Study. Int. Urol. Nephrol. 2020, 52, 67–76. [Google Scholar] [CrossRef]
- Kataoka, M.; Meguro, S.; Tanji, R.; Onagi, A.; Matsuoka, K.; Honda-Takinami, R.; Hoshi, S.; Hata, J.; Sato, Y.; Akaihata, H.; et al. Role of Puboperinealis and Rectourethralis Muscles as a Urethral Support System to Maintain Urinary Continence after Robot-Assisted Radical Prostatectomy. Sci. Rep. 2023, 13, 14126. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Li, C.; Liu, H.-Y.; Zhu, Z.-Y. Relationship between Abnormal Pelvic Floor Electromyography and Obstetric Factors in Postpartum Women: A Cross-Sectional Study. BMC Women’s Health 2024, 24, 239. [Google Scholar] [CrossRef] [PubMed]
- Tienza, A.; Robles, J.E.; Hevia, M.; Algarra, R.; Diez-Caballero, F.; Pascual, J.I. Prevalence Analysis of Urinary Incontinence after Radical Prostatectomy and Influential Preoperative Factors in a Single Institution. Aging Male 2018, 21, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Pinkhasov, R.M.; Lee, T.; Huang, R.; Berkley, B.; Pinkhasov, A.M.; Dodge, N.; Loecher, M.S.; James, G.; Pop, E.; Attwood, K.; et al. Prediction of Incontinence after Robot-Assisted Radical Prostatectomy: Development and Validation of a 24-Month Incontinence Nomogram. Cancers 2022, 14, 1644. [Google Scholar] [CrossRef]
- Thüroff, J.W.; Abrams, P.; Andersson, K.-E.; Artibani, W.; Chapple, C.R.; Drake, M.J.; Hampel, C.; Neisius, A.; Schröder, A.; Tubaro, A. EAU Guidelines on Urinary Incontinence. Eur. Urol. 2011, 59, 387–400. [Google Scholar] [CrossRef]
- García-Sánchez, C.; García Obrero, I.; Muñoz-Calahorro, C.; Rodríguez-Pérez, A.J.; Medina-López, R.A. Efficacy of Preoperative-Guided Pelvic Floor Exercises on Urinary Incontinence and Quality of Life after Robotic Radical Prostatectomy. Actas Urológicas Españolas 2025, 49, 501702. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, D.; Jones, M.K.; Ghosal, S.; Lawton, J.; Greene, K.L.; Rapp, D.E. Comparison of In-Person Versus Online Comprehensive Pelvic Floor Rehabilitation Program Following Prostatectomy. Urology 2024, 190, 90–96. [Google Scholar] [CrossRef]
- Ouchi, M.; Kitta, T.; Chiba, H.; Higuchi, M.; Abe-Takahashi, Y.; Togo, M.; Kusakabe, N.; Murai, S.; Kikuchi, H.; Matsumoto, R.; et al. Physiotherapy for Continence and Muscle Function in Prostatectomy: A Randomised Controlled Trial. BJU Int. 2024, 134, 398–406. [Google Scholar] [CrossRef]
- Smither, A.R.; Guralnick, M.L.; Davis, N.B.; See, W.A. Quantifying the Natural History of Post-Radical Prostatectomy Incontinence Using Objective Pad Test Data. BMC Urol. 2007, 7, 2. [Google Scholar] [CrossRef]
- Trofimenko, V.; Myers, J.B.; Brant, W.O. Post-Prostatectomy Incontinence: How Common and Bothersome Is It Really? Sex. Med. Rev. 2017, 5, 536–543. [Google Scholar] [CrossRef]
- Teo, J.L.; Zheng, Z.; Bird, S.R. Identifying the Factors Affecting ‘Patient Engagement’ in Exercise Rehabilitation. BMC Sports Sci. Med. Rehabil. 2022, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Hout, M.; Gurayah, A.; Arbelaez, M.C.S.; Blachman-Braun, R.; Shah, K.; Herrmann, T.R.W.; Shah, H.N. Incidence and Risk Factors for Postoperative Urinary Incontinence after Various Prostate Enucleation Procedures: Systemic Review and Meta-Analysis of PubMed Literature from 2000 to 2021. World J. Urol. 2022, 40, 2731–2745. [Google Scholar] [CrossRef] [PubMed]
- Marino, F.; Moretto, S.; Rossi, F.; Bizzarri, F.P.; Gandi, C.; Filomena, G.B.; Gavi, F.; Russo, P.; Campetella, M.; Totaro, A.; et al. Robot-Assisted Radical Prostatectomy with the Hugo RAS and Da Vinci Surgical Robotic Systems: A Systematic Review and Meta-Analysis of Comparative Studies. Eur. Urol. Focus, 2024; in press. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Group (n = 182) |
|---|---|
| Age (years), mean (SD) | 66.1 (6.5) |
| BMI (kg/m2), mean (SD) | 28.2 (3.6) |
| Preoperative PSA (ng/mL), mean (SD) | 9.2 (7.8) |
| Postoperative PSA (ng/mL), mean (SD) | 0.2 (1.5) |
| Urinary incontinence stage (at baseline), n (%) | |
| Stage 0 | 64 (35.2) |
| Stage 1 | 23 (12.6) |
| Stage 2 | 47 (25.8) |
| Stage 3 | 48 (26.4) |
| Rehabilitated before surgery, n (%) | |
| No | 36 (19.8) |
| Yes | 146 (80.2) |
| Time to rehabilitation (days), mean (SD) | 36.1 (14.0) |
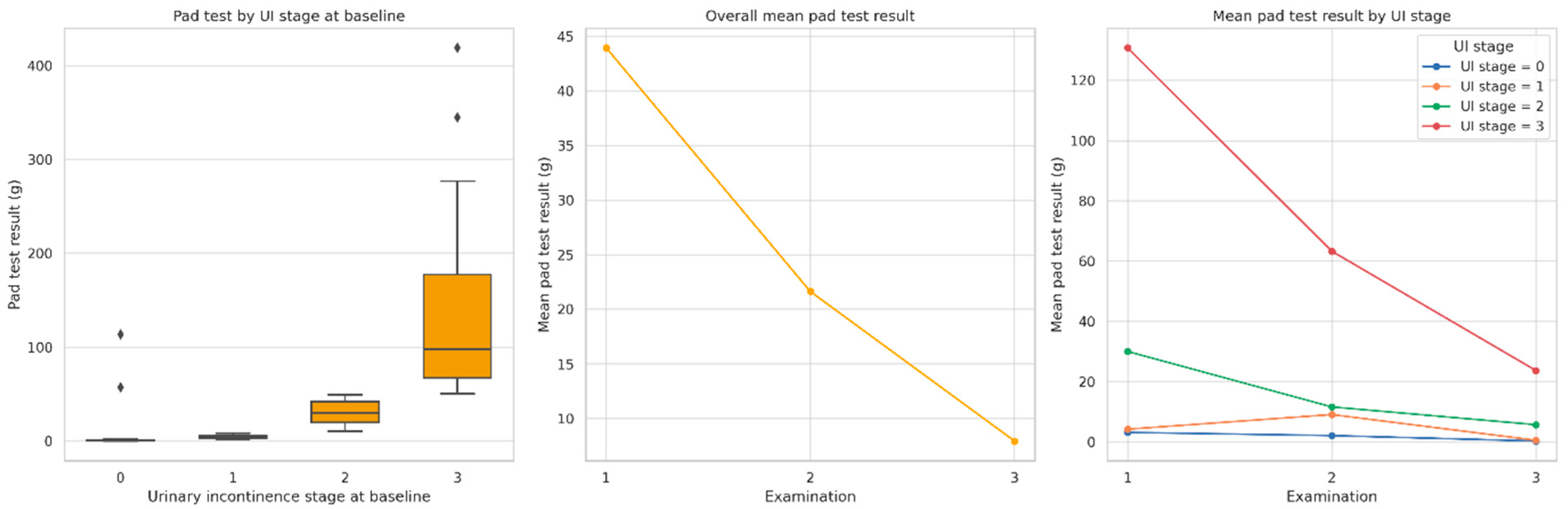
| Pad test result at Examination 1(g), mean (SD) | 43.9 (68.9) |
| Pad test result at Examination 3 (g), mean (SD) | 8.0 (22.9) |
| Δ Pad test result (g), mean (SD) | 36.0 (63.4) |
| Type of surgery, n (%) | |
| LRP | 106 (58.2) |
| RARP | 76 (41.8) |
| pT, n (%) | |
| pT1 | 2 (1.1) |
| pT2 | 126 (69.2) |
| pT3 | 54 (29.7) |
| pN, n (%) | |
| Nx | 17 (9.3) |
| N0 | 163 (89.6) |
| N1 | 2 (1.1) |
| pM, n (%) | |
| M0 | 14 (7.7) |
| Mx | 168 (92.3) |
| GS1, n (%) | |
| GS1 → 3 | 58 (31.9) |
| GS1 → 4 | 121 (66.5) |
| GS1 → 5 | 3 (1.6) |
| GS2, n (%) | |
| GS2 → 3 | 77 (42.3) |
| GS2 → 4 | 89 (48.9) |
| GS2 → 5 | 16 (8.8) |
| GS, n (%) | |
| GS → 6 | 16 (8.8) |
| GS → 7 | 100 (54.9) |
| GS → 8 | 50 (27.5) |
| GS → 9 | 16 (8.8) |
| Persistent PSA, n (%) | |
| No | 158 (86.8) |
| Yes | 24 (13.2) |
| EPE, n (%) | |
| EPE 0 | 129 (70.9) |
| EPE 1 | 47 (25.8) |
| EPE 2 | 6 (3.3) |
| SVI, n (%) | |
| No | 162 (89.0) |
| Yes | 20 (11.0) |
| EAU, n (%) | |
| EAU 1 | 9 (4.9) |
| EAU 2 | 139 (76.4) |
| EAU 3 | 34 (18.7) |
| ISUP, n (%) | |
| ISUP 1 | 16 (8.8) |
| ISUP 2 | 39 (21.4) |
| ISUP 3 | 61 (33.5) |
| ISUP 4 | 50 (27.5) |
| ISUP 5 | 16 (8.8) |
| UI Stageat Baseline | Examination 1 | Examination 2 | Examination 3 | p |
|---|---|---|---|---|
| Stage 0 | 3.2 (15.7) a | 2.2 (14.2) b | 0.4 (1.4) c | 0.0001 |
| Stage 1 | 4.3 (1.7) a | 9.1 (36.2) b | 0.6 (0.7) d | 0.0001 |
| Stage 2 | 30.1 (12.4) a | 11.7 (15.2) b | 5.8 (16.4) c | 0.0001 |
| Stage 3 | 130.8 (83.1) a | 63.3 (72.0) b | 23.7 (37.3) c,d | 0.0001 |
| Number of Pads | Examination | UI Stage 0 | UI Stage 1 | UI Stage 2 | UI Stage 3 | p (Chi2) |
|---|---|---|---|---|---|---|
| 0, n (%) | Examination 1 | 23 (35.9) | 6 (26.1) | 29 (61.7) | 38 (79.2) | <0.0001 |
| Examination 2 | 30 (46.9) | 5 (21.7) | 19 (40.4) | 24 (50.0) | <0.0001 | |
| Examination 3 | 46 (71.9) | 13 (56.5) | 20 (42.6) | 20 (41.7) | <0.0001 | |
| 1, n (%) | Examination 1 | 36 (56.2) | 12 (52.2) | 5 (10.6) | 3 (6.2) | <0.0001 |
| Examination 2 | 34 (53.1) | 16 (69.6) | 15 (31.9) | 12 (25.0) | <0.0001 | |
| Examination 3 | 17 (26.6) | 10 (43.5) | 25 (53.2) | 16 (33.3) | <0.0001 | |
| 2, n (%) | Examination 1 | 4 (6.2) | 4 (17.4) | 6 (12.8) | 3 (6.2) | <0.0001 |
| Examination 2 | 0 (0.0) | 2 (8.7) | 9 (19.1) | 5 (10.4) | <0.0001 | |
| Examination 3 | 1 (1.6) | 0 (0.0) | 2 (4.3) | 6 (12.5) | <0.0001 | |
| ≥3, n (%) | Examination 1 | 1 (1.6) | 1 (4.3) | 7 (14.9) | 4 (8.3) | <0.0001 |
| Examination 2 | 0 (0.0) | 0 (0.0) | 4 (8.5) | 7 (14.6) | <0.0001 | |
| Examination 3 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 6 (12.5) | <0.0001 |
| Number of Diapers | Examination | UI Stage 0 | UI Stage 1 | UI Stage 2 | UI Stage 3 | p (Chi2) |
|---|---|---|---|---|---|---|
| 0, n (%) | Examination 1 | 56 (87.5) | 16 (69.6) | 16 (34.0) | 4 (8.3) | <0.0001 |
| Examination 2 | 62 (96.9) | 23 (100.0) | 36 (76.6) | 27 (56.2) | <0.0001 | |
| Examination 3 | 64 (100.0) | 22 (95.7) | 42 (89.4) | 37 (77.1) | 0.0179 | |
| 1, n (%) | Examination 1 | 3 (4.7) | 3 (13.0) | 14 (29.8) | 3 (6.2) | <0.0001 |
| Examination 2 | 0 (0.0) | 0 (0.0) | 6 (12.8) | 2 (4.2) | <0.0001 | |
| Examination 3 | 0 (0.0) | 1 (4.3) | 3 (6.4) | 4 (8.3) | 0.0179 | |
| 2, n (%) | Examination 1 | 3 (4.7) | 4 (17.4) | 9 (19.1) | 9 (18.8) | <0.0001 |
| Examination 2 | 1 (1.6) | 0 (0.0) | 4 (8.5) | 12 (25.0) | <0.0001 | |
| Examination 3 | 0 (0.0) | 0 (0.0) | 1 (2.1) | 4 (8.3) | 0.0179 | |
| ≥3, n (%) | Examination 1 | 2 (3.1) | 0 (0.0) | 8 (17.0) | 32 (66.7) | <0.0001 |
| Examination 2 | 1 (1.6) | 0 (0.0) | 1 (2.1) | 7 (14.6) | <0.0001 | |
| Examination 3 | 0 (0.0) | 0 (0.0) | 1 (2.1) | 3 (6.2) | 0.0179 |
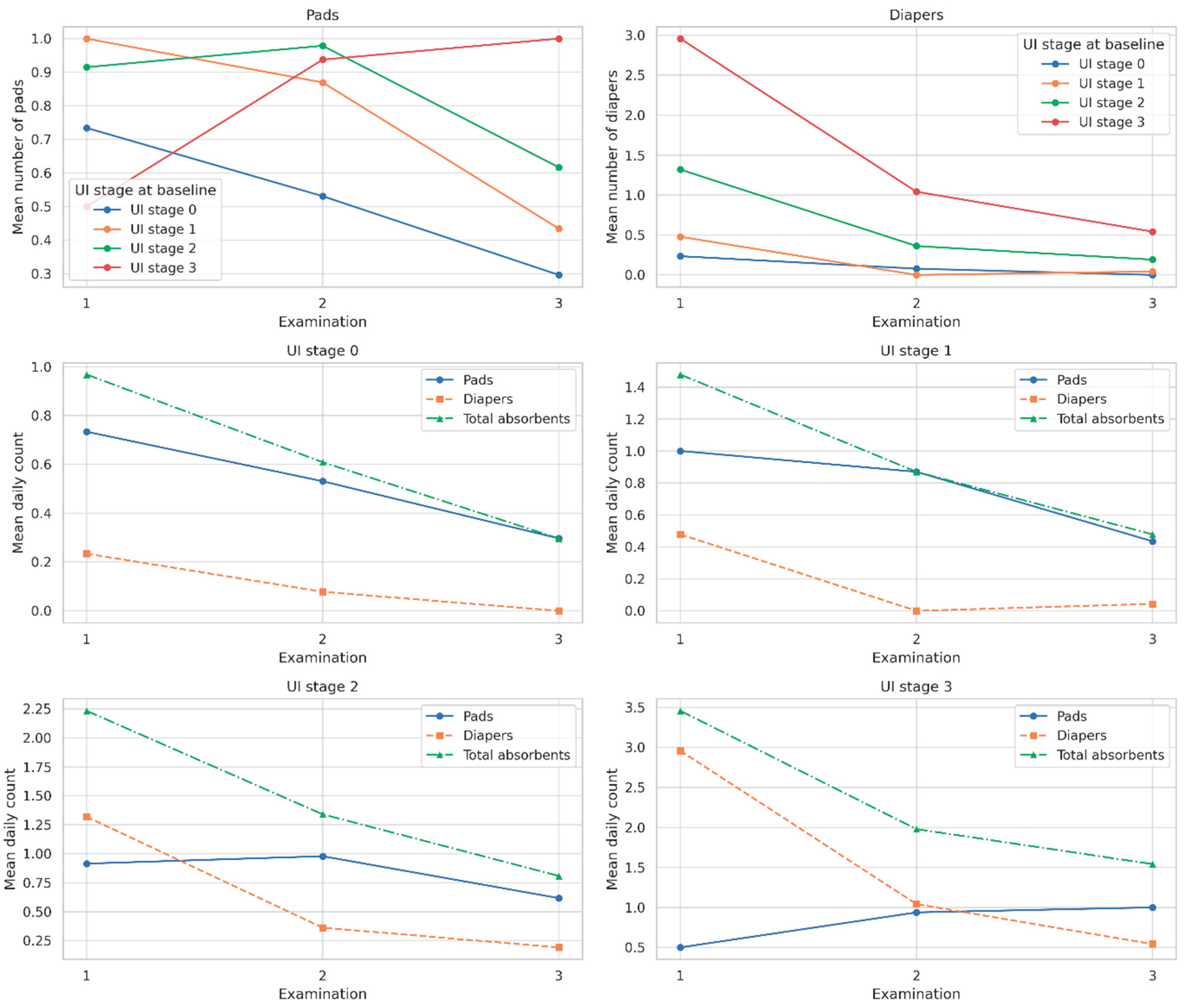
| UI Stage at Baseline | Examination | Mean Number of Pads | Mean Number of Diapers | Mean Number of Total Absorbents |
|---|---|---|---|---|
| Stage 0 | 1 | 0.7 | 0.2 | 1.0 |
| 2 | 0.5 | 0.1 | 0.6 | |
| 3 | 0.3 | 0.0 | 0.3 | |
| Stage 1 | 1 | 1.0 | 0.5 | 1.5 |
| 2 | 0.9 | 0.0 | 0.9 | |
| 3 | 0.4 | 0.0 | 0.5 | |
| Stage 2 | 1 | 0.9 | 1.3 | 2.2 |
| 2 | 1.0 | 0.4 | 1.3 | |
| 3 | 0.6 | 0.2 | 0.8 | |
| Stage 3 | 1 | 0.5 | 3.0 | 3.5 |
| 2 | 0.9 | 1.0 | 2.0 | |
| 3 | 1.0 | 0.5 | 1.5 |
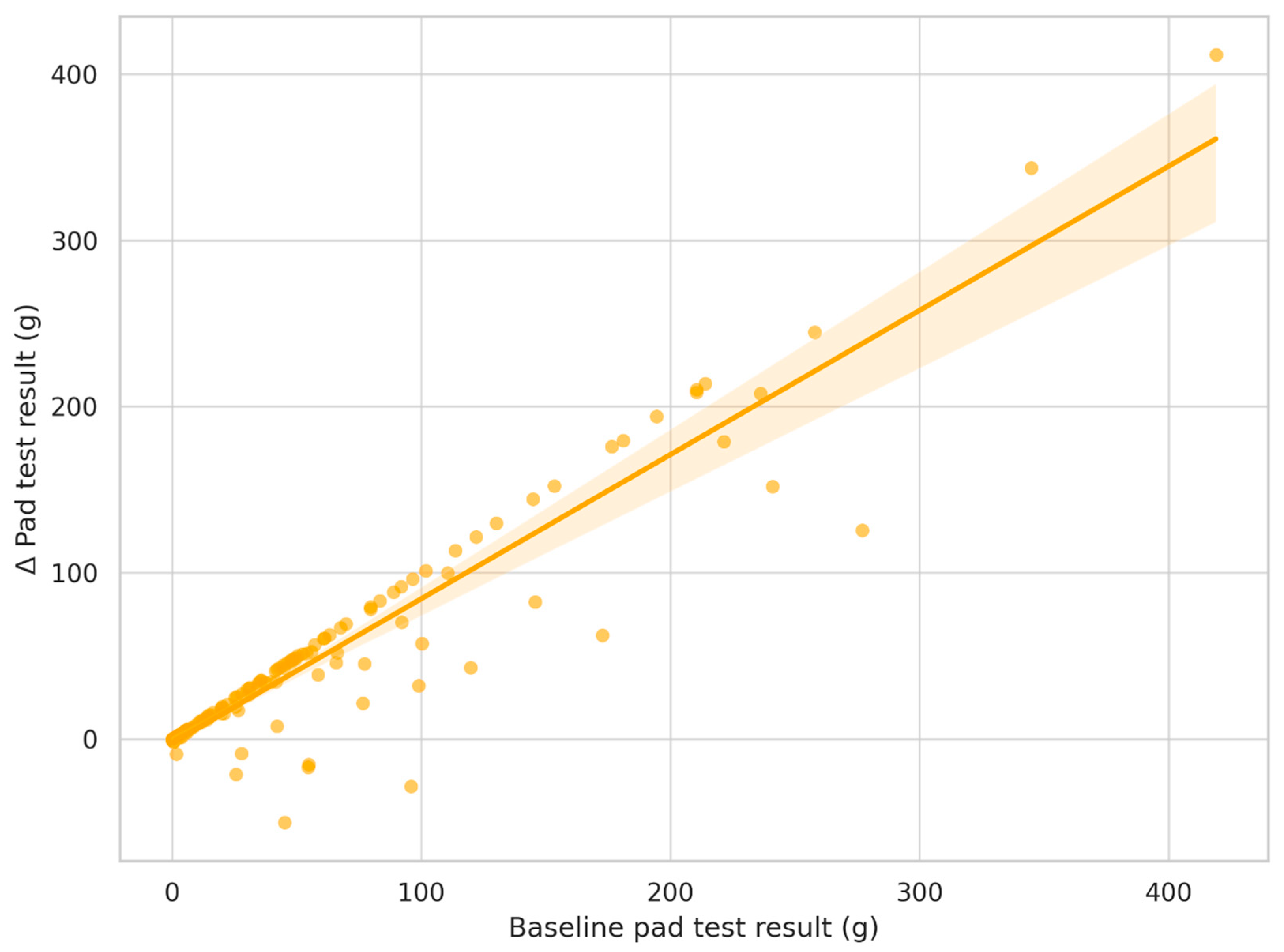
| Characteristic | β | CI 2.5% | CI 97.5% | p |
|---|---|---|---|---|
| Intercept | 28.622 | −15.214 | 72.459 | 0.199 |
| UI stage at baseline | −3.327 | −6.78 | 0.126 | 0.059 |
| Age | −0.306 | −0.794 | 0.182 | 0.218 |
| BMI | −0.174 | −1.03 | 0.683 | 0.69 |
| Time to rehabilitation | −0.075 | −0.295 | 0.145 | 0.503 |
| Baseline pad test result | 0.909 | 0.849 | 0.97 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terek-Derszniak, M.; Biskup, M.; Skowronek, T.; Nowak, M.; Falana, J.; Jaskulski, J.; Obarzanowski, M.; Gozdz, S.; Macek, P. Pelvic Floor Rehabilitation After Prostatectomy: Baseline Severity as a Predictor of Improvement—A Prospective Cohort Study. J. Clin. Med. 2025, 14, 4180. https://doi.org/10.3390/jcm14124180
Terek-Derszniak M, Biskup M, Skowronek T, Nowak M, Falana J, Jaskulski J, Obarzanowski M, Gozdz S, Macek P. Pelvic Floor Rehabilitation After Prostatectomy: Baseline Severity as a Predictor of Improvement—A Prospective Cohort Study. Journal of Clinical Medicine. 2025; 14(12):4180. https://doi.org/10.3390/jcm14124180
Chicago/Turabian StyleTerek-Derszniak, Małgorzata, Małgorzata Biskup, Tomasz Skowronek, Mariusz Nowak, Justyna Falana, Jarosław Jaskulski, Mateusz Obarzanowski, Stanislaw Gozdz, and Pawel Macek. 2025. "Pelvic Floor Rehabilitation After Prostatectomy: Baseline Severity as a Predictor of Improvement—A Prospective Cohort Study" Journal of Clinical Medicine 14, no. 12: 4180. https://doi.org/10.3390/jcm14124180
APA StyleTerek-Derszniak, M., Biskup, M., Skowronek, T., Nowak, M., Falana, J., Jaskulski, J., Obarzanowski, M., Gozdz, S., & Macek, P. (2025). Pelvic Floor Rehabilitation After Prostatectomy: Baseline Severity as a Predictor of Improvement—A Prospective Cohort Study. Journal of Clinical Medicine, 14(12), 4180. https://doi.org/10.3390/jcm14124180