
Infection Associated with Global Cerebral Edema and Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Ethics
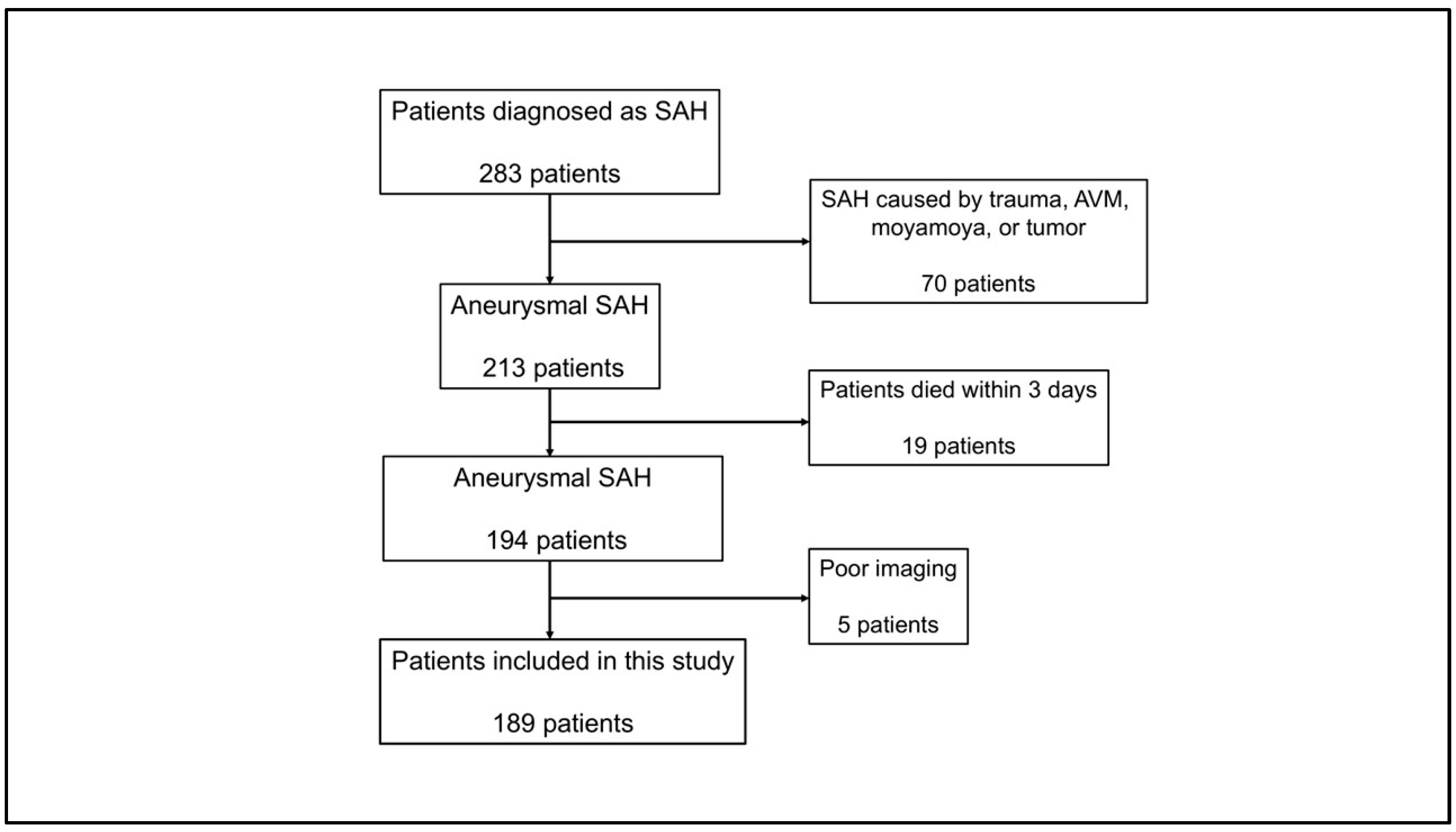
2.2. Study Design and Population
2.3. Demographic Data and Laboratory Data
2.4. Clinical and Radiographic Assessment
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Infectious Complications
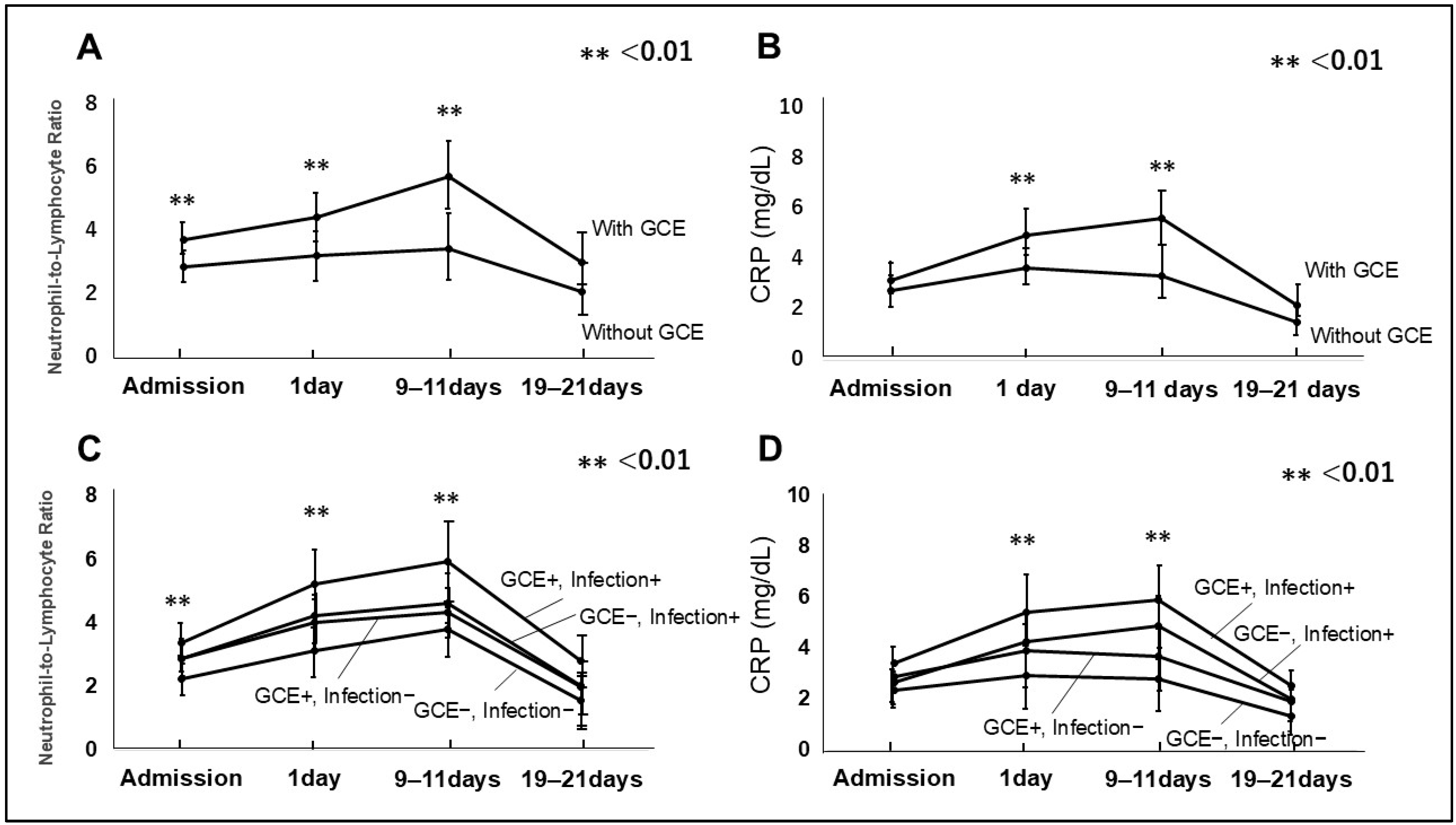
3.3. GCE and Infection
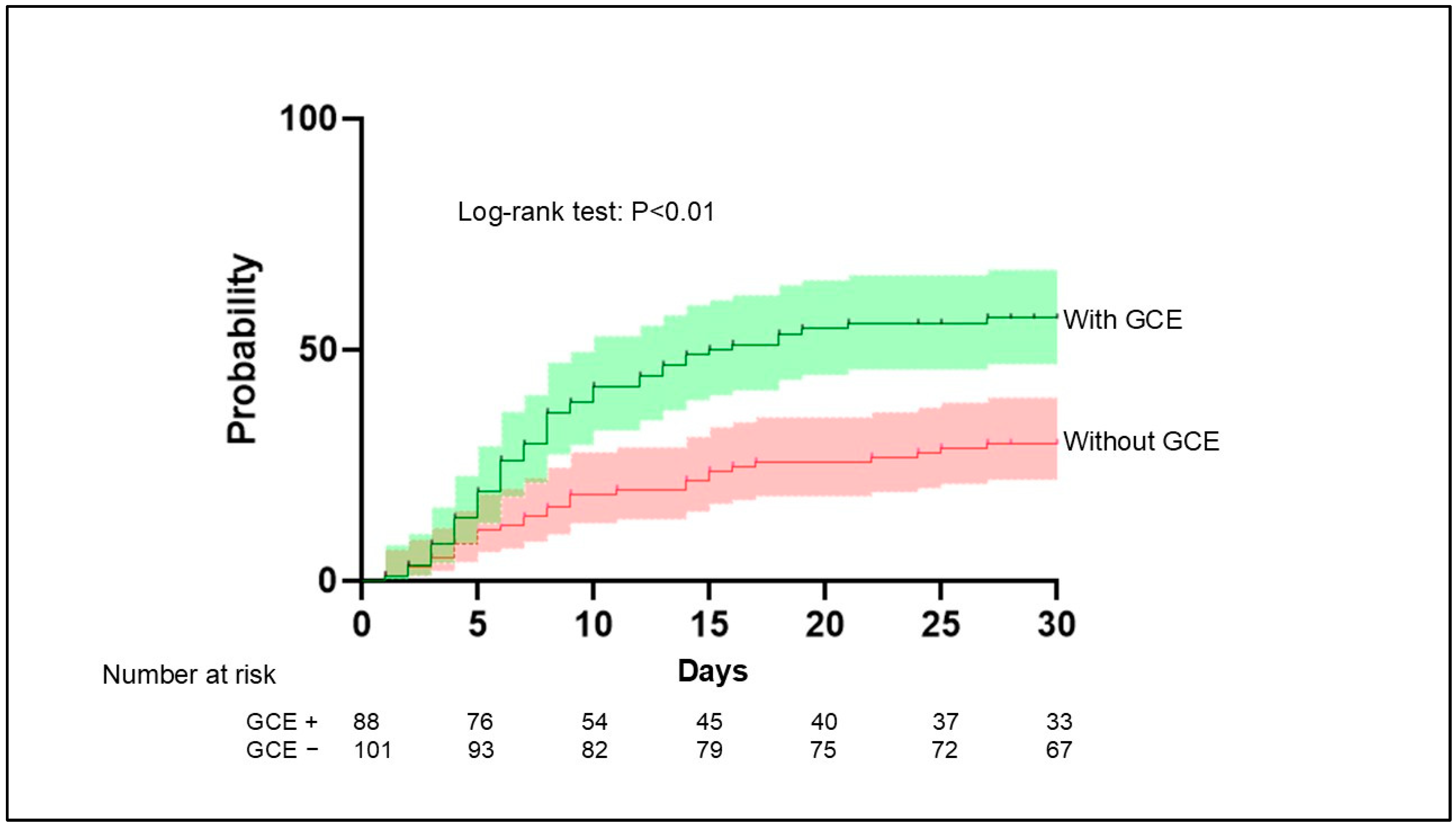
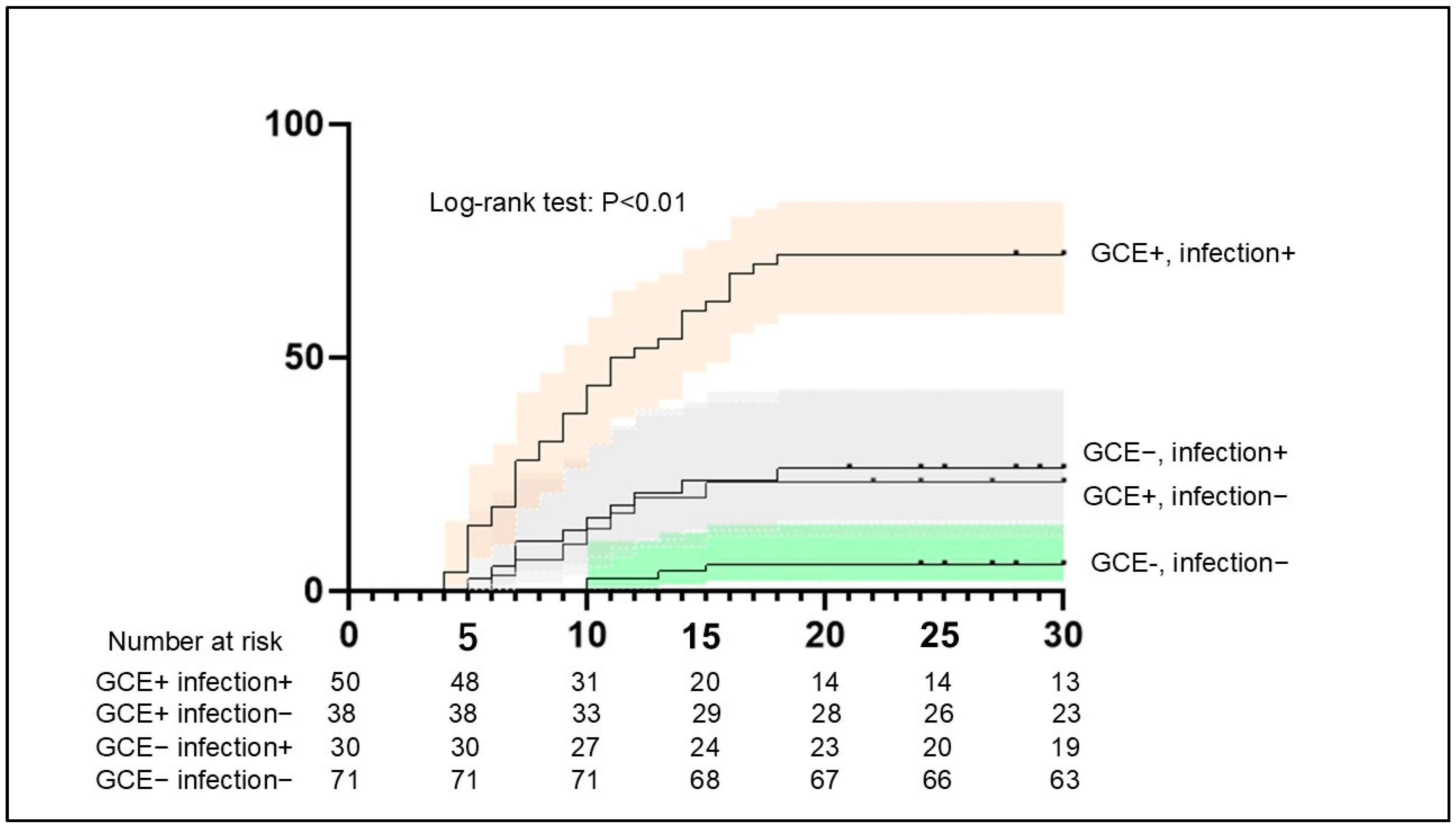
3.4. DCI Occurrence in Patients with Both GCE and Infection
3.5. Clinical Outcomes and Hospital Stay in Patients with GCE and Infection
4. Discussion
4.1. Relationship of EBI with Developing Infection
4.2. Infection Following GCE Is Associated with DCI
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Toyoda, K.; Yoshimura, S.; Nakai, M.; Koga, M.; Sasahara, Y.; Sonoda, K.; Kamiyama, K.; Yazawa, Y.; Kawada, S.; Sasaki, M.; et al. Twenty-Year Change in Severity and Outcome of Ischemic and Hemorrhagic Strokes. JAMA Neurol. 2022, 79, 61–69. [Google Scholar] [CrossRef]
- Rass, V.; Helbok, R. Early Brain Injury After Poor-Grade Subarachnoid Hemorrhage. Curr. Neurol. Neurosci. Rep. 2019, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.; Park, S. Spontaneous subarachnoid haemorrhage. Lancet 2022, 400, 846–862. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Wu, Y.; Hu, Z.; Wang, S.; Zhou, S.; Zhou, C.; Gao, X.; Huang, Y. The mechanism of ferroptosis in early brain injury after subarachnoid hemorrhage. Front. Immunol. 2023, 14, 1191826. [Google Scholar] [CrossRef]
- Thilak, S.; Brown, P.; Whitehouse, T.; Gautam, N.; Lawrence, E.; Ahmed, Z.; Veenith, T. Diagnosis and management of subarachnoid haemorrhage. Nat. Commun. 2024, 15, 1850. [Google Scholar] [CrossRef]
- Grote, E.; Hassler, W. The critical first minutes after subarachnoid hemorrhage. Neurosurgery 1988, 22, 654–661. [Google Scholar] [CrossRef]
- Chaudhry, S.R.; Kahlert, U.D.; Kinfe, T.M.; Lamprecht, A.; Niemela, M.; Hanggi, D.; Muhammad, S. Elevated Systemic IL-10 Levels Indicate Immunodepression Leading to Nosocomial Infections after Aneurysmal Subarachnoid Hemorrhage (SAH) in Patients. Int. J. Mol. Sci. 2020, 21, 1569. [Google Scholar] [CrossRef]
- Mitchelle, A.; Gorolay, V.V.; Aitken, M.; Hanneman, K.; Huo, Y.R.; Manning, N.; Tan, I.; Chan, M.V. CTP for the Screening of Vasospasm and Delayed Cerebral Ischemia in Aneurysmal SAH: A Systematic Review and Meta-analysis. Am. J. Neuroradiol. 2024, 45, 871–878. [Google Scholar] [CrossRef]
- Umekawa, M.; Yoshikawa, G. Impact of ventriculo-cisternal irrigation on prevention of delayed cerebral infarction in aneurysmal subarachnoid hemorrhage: A single-center retrospective study and literature review. Neurosurg. Rev. 2023, 47, 6. [Google Scholar] [CrossRef]
- Frontera, J.A.; Claassen, J.; Schmidt, J.M.; Wartenberg, K.E.; Temes, R.; Connolly, E.S.; MacDonald, R.L., Jr.; Mayer, S.A. Prediction of symptomatic vasospasm after subarachnoid hemorrhage: The modified fisher scale. Neurosurgery 2006, 59, 21–27. [Google Scholar]
- Cao, W.; Song, Y.; Bai, X.; Yang, B.; Li, L.; Wang, X.; Wang, Y.; Chang, W.; Chen, Y.; Wang, Y.; et al. Systemic-inflammatory indices and clinical outcomes in patients with anterior circulation acute ischemic stroke undergoing successful endovascular thrombectomy. Heliyon 2024, 10, e31122. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Wang, Z.; Song, J.; Ji, Y. Correlation analysis of inflammatory markers with the short-term prognosis of acute ischaemic stroke. Sci. Rep. 2024, 14, 17772. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Savarraj, J.P.; Pervez, M.; Jones, W.; Park, J.; Jeon, S.B.; Kwon, S.U.; Chang, T.R.; Lee, K.; Kim, D.H.; et al. The Subarachnoid Hemorrhage Early Brain Edema Score Predicts Delayed Cerebral Ischemia and Clinical Outcomes. Neurosurgery 2018, 83, 137–145. [Google Scholar] [CrossRef]
- Vergouwen, M.D.; Vermeulen, M.; van Gijn, J.; Rinkel, G.J.; Wijdicks, E.F.; Muizelaar, J.P.; Mendelow, A.D.; Juvela, S.; Yonas, H.; Terbrugge, K.G.; et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: Proposal of a multidisciplinary research group. Stroke 2010, 41, 2391–2395. [Google Scholar] [CrossRef]
- Kilgore, C.B.; Ran, K.R.; Kalluri, A.L.; Nair, S.K.; Kim, J.E.; Caplan, J.M.; Jackson, C.M.; Gonzalez, L.F.; Huang, J.; Tamargo, R.J.; et al. Perioperative Infection After Aneurysmal Subarachnoid Hemorrhage: Risk Factors, Causative Pathogens, and Long-Term Outcomes. Neurosurgery 2024, 94, 325–333. [Google Scholar] [CrossRef]
- Wang, T.; Hao, J.; Zhou, J.; Chen, G.; Shen, H.; Sun, Q. Development and validation of a machine-learning model for predicting postoperative pneumonia in aneurysmal subarachnoid hemorrhage. Neurosurg. Rev. 2024, 47, 668. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, Y.; Zhao, J.; Deng, L. Neutrophil-lymphocyte ratio on first and third postoperative days: Associated with severe pneumonia in aneurysmal subarachnoid hemorrhage patients undergoing surgeries. Neurosurg. Rev. 2024, 47, 70. [Google Scholar] [CrossRef]
- Ivanidze, J.; Ferraro, R.A.; Giambrone, A.E.; Segal, A.Z.; Gupta, A.; Sanelli, P.C. Blood-Brain Barrier Permeability in Aneurysmal Subarachnoid Hemorrhage: Correlation With Clinical Outcomes. Am. J. Roentgenol. 2018, 211, 891–895. [Google Scholar] [CrossRef]
- Suzuki, H.; Fujimoto, M.; Kawakita, F.; Liu, L.; Nakatsuka, Y.; Nakano, F.; Nishikawa, H.; Okada, T.; Kanamaru, H.; Imanaka-Yoshida, K.; et al. Tenascin-C in brain injuries and edema after subarachnoid hemorrhage: Findings from basic and clinical studies. J. Neurosci. Res. 2020, 98, 42–56. [Google Scholar] [CrossRef]
- Cahill, J.; Calvert, J.W.; Zhang, J.H. Mechanisms of early brain injury after subarachnoid hemorrhage. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow and Metab. 2006, 26, 1341–1353. [Google Scholar] [CrossRef]
- Elenkov, I.J.; Wilder, R.L.; Chrousos, G.P.; Vizi, E.S. The sympathetic nerve--an integrative interface between two supersystems: The brain and the immune system. Pharmacol. Rev. 2000, 52, 595–638. [Google Scholar] [CrossRef] [PubMed]
- Soto-Tinoco, E.; Guerrero-Vargas, N.N.; Buijs, R.M. Interaction between the hypothalamus and the immune system. Exp. Physiol. 2016, 101, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Savarraj, J.; Parsha, K.; Hergenroeder, G.; Ahn, S.; Chang, T.R.; Kim, D.H.; Choi, H.A. Early Brain Injury Associated with Systemic Inflammation After Subarachnoid Hemorrhage. Neurocrit. Care 2018, 28, 203–211. [Google Scholar] [CrossRef]
- Jiang, C.; Kong, W.; Wang, Y.; Ziai, W.; Yang, Q.; Zuo, F.; Li, F.; Wang, Y.; Xu, H.; Li, Q.; et al. Changes in the cellular immune system and circulating inflammatory markers of stroke patients. Oncotarget 2017, 8, 3553–3567. [Google Scholar] [CrossRef]
- Klehmet, J.; Harms, H.; Richter, M.; Prass, K.; Volk, H.D.; Dirnagl, U.; Meisel, A.; Meisel, C. Stroke-induced immunodepression and post-stroke infections: Lessons from the preventive antibacterial therapy in stroke trial. Neuroscience 2009, 158, 1184–1193. [Google Scholar] [CrossRef]
- Mengel, A.; Ulm, L.; Hotter, B.; Harms, H.; Piper, S.K.; Grittner, U.; Montaner, J.; Meisel, C.; Meisel, A.; Hoffmann, S. Biomarkers of immune capacity, infection and inflammation are associated with poor outcome and mortality after stroke—the PREDICT study. BMC Neurol. 2019, 19, 148. [Google Scholar] [CrossRef]
- Sarrafzadeh, A.; Schlenk, F.; Meisel, A.; Dreier, J.; Vajkoczy, P.; Meisel, C. Immunodepression after aneurysmal subarachnoid hemorrhage. Stroke 2011, 42, 53–58. [Google Scholar] [CrossRef]
- Zhong, W.; Zhang, Z.; Zhao, P.; Shen, J.; Li, X.; Wang, D.; Li, G.; Su, W. The Impact of Initial Systemic Inflammatory Response After Aneurysmal Subarachnoid Hemorrhage. Turk. Neurosurg. 2017, 27, 346–352. [Google Scholar]
- Croci, D.M.; Sivanrupan, S.; Wanderer, S.; Agnoletto, G.J.; Chiappini, A.; Gruter, B.E.; Andereggen, L.; Mariani, L.; Taussky, P.; Marbacher, S. Preclinical and clinical role of interleukin-6 in the development of delayed cerebral vasospasm and neuronal cell death after subarachnoid hemorrhage: Towards a potential target therapy? Neurosurg. Rev. 2022, 45, 395–403. [Google Scholar] [CrossRef]
- Li, X.; Zeng, L.; Lu, X.; Chen, K.; Yu, M.; Wang, B.; Zhao, M. Early Brain Injury and Neuroprotective Treatment after Aneurysmal Subarachnoid Hemorrhage: A Literature Review. Brain Sci. 2023, 13, 1083. [Google Scholar] [CrossRef]
- Bogossian, E.G.; Attanasio, L.; Creteur, J.; Grimaldi, D.; Schuind, S.; Taccone, F.S. The Impact of Extracerebral Infection After Subarachnoid Hemorrhage: A Single-Center Cohort Study. World Neurosurg. 2020, 144, e883–e897. [Google Scholar] [CrossRef] [PubMed]
- Douds, G.L.; Tadzong, B.; Agarwal, A.D.; Krishnamurthy, S.; Lehman, E.B.; Cockroft, K.M. Influence of Fever and hospital-acquired infection on the incidence of delayed neurological deficit and poor outcome after aneurysmal subarachnoid hemorrhage. Neurol. Res. Int. 2012, 2012, 479865. [Google Scholar] [CrossRef] [PubMed]
- Frontera, J.A.; Fernandez, A.; Schmidt, J.M.; Claassen, J.; Wartenberg, K.E.; Badjatia, N.; Parra, A.; Connolly, E.S.; Mayer, S.A. Impact of nosocomial infectious complications after subarachnoid hemorrhage. Neurosurgery 2008, 62, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Laban, K.G.; Rinkel, G.J.; Vergouwen, M.D. Nosocomial infections after aneurysmal subarachnoid hemorrhage: Time course and causative pathogens. Int. J. Stroke 2015, 10, 763–766. [Google Scholar] [CrossRef]
- Chefer, V.I.; Thompson, A.C.; Zapata, A.; Shippenberg, T.S. Overview of brain microdialysis. Curr. Protoc. Neurosci. 2009, 47, 7-1. [Google Scholar] [CrossRef]
- Messina, R.; de Gennaro, L.; De Robertis, M.; Pop, R.; Chibbaro, S.; Severac, F.; Blagia, M.; Balducci, M.T.; Bozzi, M.T.; Signorelli, F. Cerebrospinal Fluid Lactate and Glucose Levels as Predictors of Symptomatic Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2023, 170, e596–e602. [Google Scholar] [CrossRef]
- Rosenthal, E.S.; Biswal, S.; Zafar, S.F.; O’Connor, K.L.; Bechek, S.; Shenoy, A.V.; Boyle, E.J.; Shafi, M.M.; Gilmore, E.J.; Foreman, B.P.; et al. Continuous electroencephalography predicts delayed cerebral ischemia after subarachnoid hemorrhage: A prospective study of diagnostic accuracy. Ann. Neurol. 2018, 83, 958–969. [Google Scholar] [CrossRef]
- Yang, X.; Peng, J.; Pang, J.; Wan, W.; Zhong, C.; Peng, T.; Bao, K.; Jiang, Y. The Association Between Serum Macrophage Migration Inhibitory Factor and Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage. Neurotox. Res. 2020, 37, 397–405. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SAH Patients | |
|---|---|
| Number | 189 |
| Demographic | |
| Age | 68.8 ± 11.9 |
| Sex (female) | 134 (70.9%) |
| Hypertension | 59 (31.2%) |
| Diabetic mellitus | 35 (18.5%) |
| Dyslipidemia | 40 (21.2%) |
| Patients condition | |
| WFNS grade | |
| 1 | 64 (33.9%) |
| 2 | 38 (20.1%) |
| 3 | 8 (4.2%) |
| 4 | 40 (21.2%) |
| 5 | 39 (20.6%) |
| Radiological finding | |
| GCE | 88 (46.6%) |
| Aneurism location | |
| Acom | 59 (31.2%) |
| ICA | 49 (25.9%) |
| MCA | 42 (22.2%) |
| Distal ACA | 12 (6.3%) |
| Posterior circulation | 27 (14.4%) |
| IVH | 33 (17.5%) |
| ICH | 39 (20.6%) |
| Hydrocephalus | 90 (47.6%) |
| modified Fisher grade | |
| Grade0 | 9 (4.8%) |
| Grade1 | 11 (5.8%) |
| Grade2 | 6 (3.2%) |
| Grade3 | 29 (15.3%) |
| Grade4 | 134 (70.9%) |
| Treatment | |
| Endovascular | 118 (62.4%) |
| Clipping | 71 (37.6%) |
| mechanical ventilation | 82 (43.3%) |
| Central venous catheter use | 160 (84.7%) |
| Morbidity | |
| Infection | 80 patients with 98 infection |
| pneumonia | 53 |
| UTI | 31 |
| sepsis | 8 |
| Meningitis | 4 |
| Biliary | 2 |
| Delayed cerebral ischemic | 58 (30.7%) |
| Outcime | |
| mRS | |
| Good outcome (mRS 0–3) | 119 (63.0%) |
| Poor outcome (mRS 4–6) | 70 (37.0%) |
| Infection Positive | Infection Negative | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| Number (N = 189) | 80 | 109 | p Value | p Value | Odds (95%CI) |
| Demographic | |||||
| Age | 71.8 ± 10.9 | 66.9 ± 12.8 | 0.02 | 0.03 | 2.5 (1.2–4.9) |
| Sex (female) | 54 | 80 | 0.42 | ||
| Hypertension | 20 | 29 | 0.87 | ||
| Diabetic mellitus | 15 | 20 | 0.98 | ||
| Dyslipidemia | 19 | 21 | 0.48 | ||
| Patients condition | |||||
| WFNS grade (4, 5) | 45 | 34 | 0.005 | 0.01 | 3.9 (1.5–9.5) |
| Radiological finding | |||||
| Anrurysm type | |||||
| Saccular | 75 | 101 | 0.98 | ||
| Fusiform | 5 | 8 | |||
| GCE | 50 | 38 | <0.001 | 0.01 | 3.3 (1.3–8.6) |
| Aneurism location | |||||
| Acom | 28 | 31 | 0.86 | ||
| ICA | 20 | 29 | |||
| MCA | 18 | 24 | |||
| Distal ACA | 4 | 8 | |||
| Posterior circulation | 10 | 17 | |||
| IVH | 15 | 18 | 0.7 | ||
| ICH | 22 | 17 | 0.07 | 0.09 | |
| Hydrocephalus | 40 | 50 | 0.66 | ||
| modified Fisher grade | |||||
| Grade0 | 4 | 5 | 0.98 | ||
| Grade1 | 5 | 6 | |||
| Grade2 | 3 | 3 | |||
| Grade3 | 11 | 18 | |||
| Grade4 | 57 | 77 | |||
| Treatment | |||||
| Aneurysm treatment | |||||
| Endovascular | 55 | 63 | 0.13 | 0.19 | |
| Clipping | 25 | 46 | |||
| Mechanical ventilation use | 45 | 37 | 0.003 | 0.04 | 1.4 (1.1–3.9) |
| Central venous catheter use | 70 | 90 | 0.42 | ||
| DCI Positive | DCI Negative | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| NUMBER (N = 189) | 58 | 131 | p Value | p Value | Odds (95%CI) |
| Demographic | |||||
| Age | 70.8 ± 10.9 | 67.9 ± 12.8 | 0.03 | 0.03 | 2.3 (1.1–4.6) |
| Sex (female) | 40 | 94 | 0.73 | ||
| Hypertension | 15 | 34 | 0.98 | ||
| Diabeticmellitus | 11 | 24 | 0.98 | ||
| Dyslipidemia | 15 | 25 | 0.34 | ||
| Patients condition | |||||
| WFNS grade (4, 5) | 40 | 39 | <0.001 | <0.001 | 4.5 (1.5–9.2) |
| Radiological finding | |||||
| Anrurysm type | |||||
| Saccular | 54 | 122 | 0.98 | ||
| Fusiform | 4 | 9 | |||
| GCE + infection | 36 | 22 | <0.001 | <0.001 | 4.1 (1.3–8.9) |
| Aneurism location | |||||
| Acom | 20 | 39 | 0.74 | ||
| ICA | 14 | 33 | |||
| MCA | 15 | 27 | |||
| Distal ACA | 2 | 10 | |||
| Posterior circulation | 7 | 20 | |||
| IVH | 13 | 20 | 0.3 | 0.18 | |
| ICH | 14 | 22 | 0.24 | 0.11 | |
| Hydrocephalus | 28 | 62 | 0.95 | ||
| modified Fisher grade | |||||
| Grade0 | 3 | 6 | 0.98 | ||
| Grade1 | 4 | 7 | |||
| Grade2 | 2 | 4 | |||
| Grade3 | 8 | 21 | |||
| Grade4 | 45 | 89 | |||
| Treatment | |||||
| Aneurysm treatment | |||||
| Endovascular | 40 | 78 | 0.33 | ||
| Clipping | 19 | 52 | |||
| Mechanical ventilation use | 30 | 52 | 0.4 | ||
| Central venous catheter use | 50 | 110 | 0.83 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashiwazaki, D.; Maruyama, K.; Hamada, S.; Yamamoto, S.; Hori, E.; Akioka, N.; Noguchi, K.; Kuroda, S. Infection Associated with Global Cerebral Edema and Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage. J. Clin. Med. 2025, 14, 3808. https://doi.org/10.3390/jcm14113808
Kashiwazaki D, Maruyama K, Hamada S, Yamamoto S, Hori E, Akioka N, Noguchi K, Kuroda S. Infection Associated with Global Cerebral Edema and Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage. Journal of Clinical Medicine. 2025; 14(11):3808. https://doi.org/10.3390/jcm14113808
Chicago/Turabian StyleKashiwazaki, Daina, Kunitaka Maruyama, Saori Hamada, Shusuke Yamamoto, Emiko Hori, Naoki Akioka, Kyo Noguchi, and Satoshi Kuroda. 2025. "Infection Associated with Global Cerebral Edema and Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage" Journal of Clinical Medicine 14, no. 11: 3808. https://doi.org/10.3390/jcm14113808
APA StyleKashiwazaki, D., Maruyama, K., Hamada, S., Yamamoto, S., Hori, E., Akioka, N., Noguchi, K., & Kuroda, S. (2025). Infection Associated with Global Cerebral Edema and Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage. Journal of Clinical Medicine, 14(11), 3808. https://doi.org/10.3390/jcm14113808