
Enhancing Communication in Minimally Verbal Autistic Children: A Study on NAO-Assisted Therapy

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
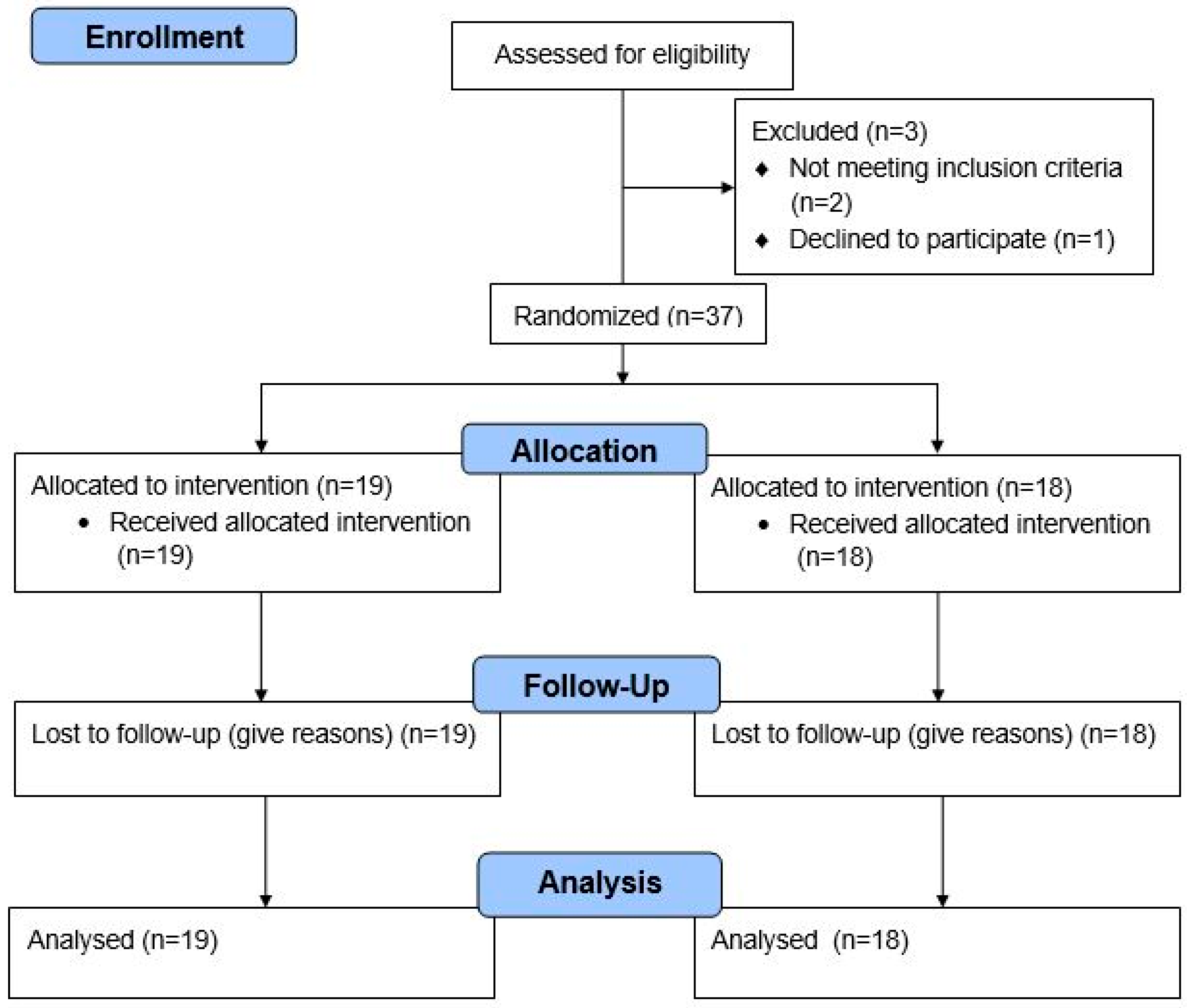
2.1. Study Design
2.2. Inclusion Criteria
2.3. Measures
- −
- Construction spontaneous production (Cons. Spont): The number of words spontaneously produced by the child during the session.
- −
- Comprehension of words (CW): The ability of the child to understand and respond to spoken words.
- −
- Comprehension of sentences (CS): The ability of the child to comprehend and respond to spoken sentences.
- −
- Comprehension total (Comp. total): The cumulative score derived from CW and CS, representing overall language comprehension.
- −
- Nominating body parts (NB) and objects (NO): The child’s ability to name common objects and body parts.
- −
- Naming total: A combined measure of NB and NO, reflecting the child’s ability to label objects and body parts.
- −
- Phonological and morphosyntactic accuracy (AP and AM): The accuracy with which the child produces sounds and follows grammatical structures in their speech.
- −
- Sentence construction (SC): The ability of the child to construct grammatically correct sentences.
- −
- Consistent period (Cons. Period): The duration of time during which the child consistently produces verbal responses.
- −
- Mean length of the utterance (Cons. MLU): The average length of verbal expressions in morphemes, calculated to assess syntactic complexity.
2.4. Intervention
2.5. Statistics
3. Results
3.1. Participant Recruitment and Completion
3.2. Feasibility and Safety
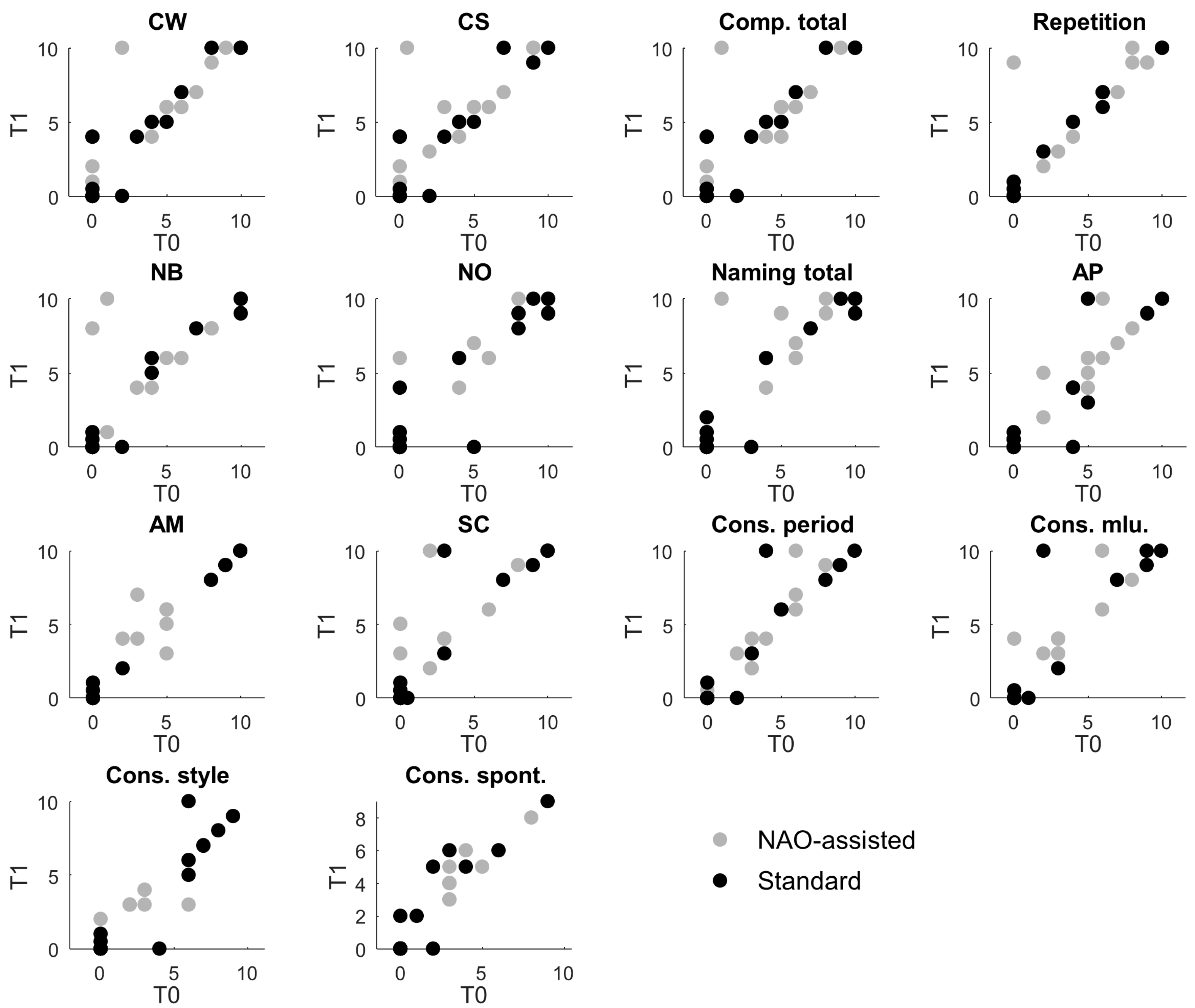
3.3. The NAO-Assisted Rehabilitation Showed Better Outcomes
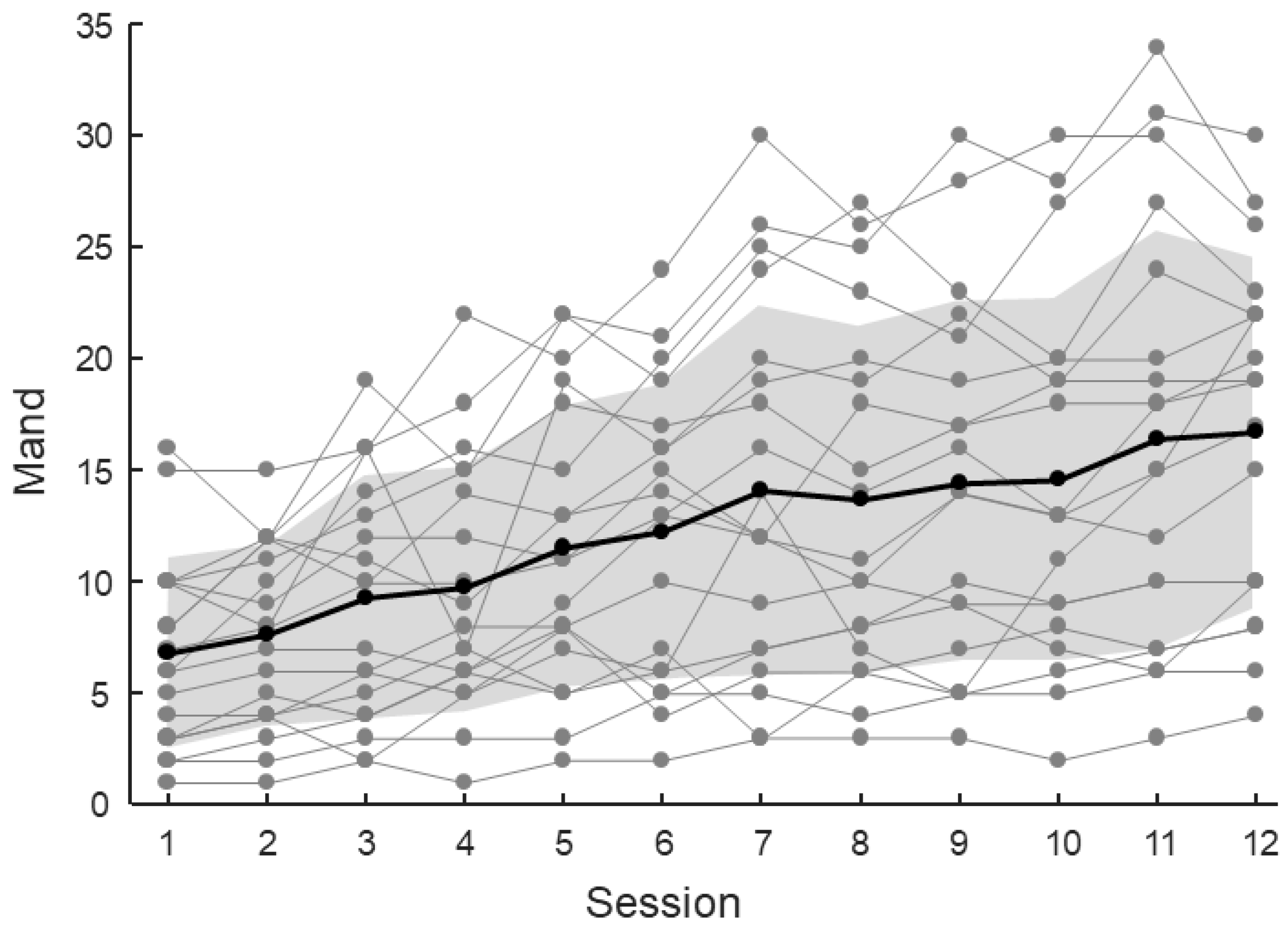
3.4. The Mand Increased Across Sessions
3.5. Influence of Verbal Communication Aspects on the Mand
4. Discussion
4.1. Relevance to Previous Research
4.2. Contributions of the Present Study
4.3. Implications for Practice and Integration
4.4. Future Directions
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASD | Autism spectrum disorder |
| MV | Minimally verbal |
| ABA | Applied behavior analysis |
| AAC | Augmentative and alternative communication |
| VR | Virtual reality |
| ADOS | Autism Diagnostic Observation and Schedule |
| VABS | Vineland Adaptive Behavior Scales |
| TVL | Language Development Level Test |
| Cons. Spont | Construction spontaneous production |
| CW | Comprehension of words |
| CS | Comprehension of sentences |
| Comp. total | Comprehension total |
| NB | Nominating body parts |
| NO | Nominating objects |
| AP | Phonological accuracy |
| AM | Morphosyntactis accuracy |
| SC | Sentence construction |
| Cons. Period | Consistent period |
| Cons. MLU | Mean length of utterance |
| IOA | Inter-observer agreement |
References
- Brignell, A.; Williams, K.; Docking, K.; Munro, N. Communication interventions for autism spectrum disorder in minimally verbal children. Cochrane Database Syst. Rev. 2018, 11, CD012324. [Google Scholar] [CrossRef] [PubMed]
- Rose, V.; Trembath, D.; Keen, D.; Paynter, J. The proportion of minimally verbal children with autism spectrum disorder in a community-based early intervention programme. J. Intellect. Disabil. Res. 2016, 60, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl. Pediatr. 2020, 9 (Suppl. S1), S55–S65. [Google Scholar] [CrossRef] [PubMed]
- Koegel, L.K.; Bryan, K.M.; Su, P.L.; Vaidya, M.; Camarata, S. Definitions of Nonverbal and Minimally Verbal in Research for Autism: A Systematic Review of the Literature. J. Autism Dev. Disord. 2020, 50, 2957–2972. [Google Scholar] [CrossRef]
- Pizzano, M.; Shire, S.; Shih, W.; Levato, L.; Landa, R.; Lord, C.; Smith, T.; Kasari, C. Profiles of minimally verbal autistic children: Illuminating the neglected end of the spectrum. Autism Res. 2024, 17, 1218–1229. [Google Scholar] [CrossRef]
- Cucinotta, F.; Ricciardello, A.; Turriziani, L.; Calabrese, G.; Briguglio, M.; Boncoddo, M.; Bellomo, F.; Tomaiuolo, P.; Martines, S.; Bruschetta, M.; et al. FARP-1 deletion is associated with lack of response to autism treatment by early start denver model in a multiplex family. Mol. Genet. Genom. Med. 2020, 8, e1373. [Google Scholar] [CrossRef]
- Cucinotta, F.; Ricciardello, A.; Turriziani, L.; Mancini, A.; Keller, R.; Sacco, R.; Persico, A.M. Efficacy and Safety of Q10 Ubiquinol With Vitamins B and E in Neurodevelopmental Disorders: A Retrospective Chart Review. Front. Psychiatry 2022, 13, 829516. [Google Scholar] [CrossRef]
- Thiemann-Bourque, K.; Brady, N.; McGuff, S.; Stump, K.; Naylor, A. Picture Exchange Communication System and Pals: A Peer-Mediated Augmentative and Alternative Communication Intervention for Minimally Verbal Preschoolers With Autism. J. Speech Lang. Hear. Res. 2016, 59, 1133–1145. [Google Scholar] [CrossRef]
- Tager-Flusberg, H.; Plesa Skwerer, D.; Joseph, R.M.; Brukilacchio, B.; Decker, J.; Eggleston, B.; Meyer, S.; Yoder, A. Conducting research with minimally verbal participants with autism spectrum disorder. Autism 2017, 21, 852–861. [Google Scholar] [CrossRef]
- Crowe, B.; Machalicek, W.; Wei, Q.; Drew, C.; Ganz, J. Augmentative and Alternative Communication for Children with Intellectual and Developmental Disability: A Mega-Review of the Literature. J. Dev. Phys. Disabil. 2022, 34, 1–42. [Google Scholar] [CrossRef]
- Korneder, J.; Louie, W.G.; Pawluk, C.M.; Abbas, I.; Brys, M.; Rooney, F. Robot-mediated interventions for teaching children with ASD: A new intraverbal skill. Assist. Technol. Off. J. RESNA 2022, 34, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.; Mophosho, M.; Moonsamy, S. Communication strategies used by adolescents with autism spectrum disorder and health professionals during treatment. Afr. J. Disabil. 2022, 11, 811. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, P.; Tonacci, A.; Tartarisco, G.; Billeci, L.; Ruta, L.; Gangemi, S.; Pioggia, G. Autism and social robotics: A systematic review. Autism Res. Off. J. Int. Soc. Autism Res. 2016, 9, 165–183. [Google Scholar] [CrossRef]
- Robins, B.; Dautenhahn, K.; Boekhorst, R.T.; Billard, A. Robotic assistants in therapy and education of children with autism: Can a small humanoid robot help encourage social interaction skills? Univers. Access Inf. Soc. 2005, 4, 105–120. [Google Scholar] [CrossRef]
- Cappadona, I.; Ielo, A.; La Fauci, M.; Tresoldi, M.; Settimo, C.; De Cola, M.C.; Muratore, R.; De Domenico, C.; Di Cara, M.; Corallo, F.; et al. Feasibility and Effectiveness of Speech Intervention Implemented with a Virtual Reality System in Children with Developmental Language Disorders: A Pilot Randomized Control Trial. Children 2023, 10, 1336. [Google Scholar] [CrossRef]
- Geminiani, A.; Santos, L.; Casellato, C.; Farabbi, A.; Farella, N.; Santos-Victor, J.; Olivieri, I.; Pedrocchi, A. Design and validation of two embodied mirroring setups for interactive games with autistic children using the NAO humanoid robot. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1641–1644. [Google Scholar] [CrossRef]
- Javed, H.; Park, C.H. Promoting Social Engagement With a Multi-Role Dancing Robot for In-Home Autism Care. Front. Robot. AI 2022, 9, 880691. [Google Scholar] [CrossRef]
- So, W.C.; Wong, M.K.; Lam, C.K.; Lam, W.Y.; Chui, A.T.; Lee, T.L.; Ng, H.M.; Chan, C.H.; Fok, D.C. Using a social robot to teach gestural recognition and production in children with autism spectrum disorders. Disabil. Rehabil. Assist. Technol. 2018, 13, 527–539. [Google Scholar] [CrossRef]
- Rakhymbayeva, N.; Amirova, A.; Sandygulova, A. A Long-Term Engagement with a Social Robot for Autism Therapy. Front. Robot. AI 2021, 16, 669972. [Google Scholar] [CrossRef]
- Puglisi, A.; Caprì, T.; Pignolo, L.; Gismondo, S.; Chilà, P.; Minutoli, R.; Marino, F.; Failla, C.; Arnao, A.A.; Tartarisco, G.; et al. Social Humanoid Robots for Children with Autism Spectrum Disorders: A Review of Modalities, Indications, and Pitfalls. Children 2022, 9, 953. [Google Scholar] [CrossRef]
- Bharatharaj, J.; Huang, L.; Al-Jumaily, A.; Mohan, R.E.; Krägeloh, C. Sociopsychological and physiological effects of a robot-assisted therapy for children with autism. Int. J. Adv. Robot. Syst. 2017, 14, 1729881417736895. [Google Scholar] [CrossRef]
- Filippini, C.; Perpetuini, D.; Cardone, D.; Merla, A. Improving Human-Robot Interaction by Enhancing NAO Robot Awareness of Human Facial Expression. Sensors 2021, 21, 6438. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Santini, S.J.; Di Genova, D.; Maggi, G.; Verrotti, A.; Farello, G.; Romualdi, R.; Alisi, A.; Tozzi, A.E.; Balsano, C. Using the Social Robot NAO for Emotional Support to Children at a Pediatric Emergency Department: Randomized Clinical Trial. J. Med. Internet Res. 2022, 24, e29656. [Google Scholar] [CrossRef] [PubMed]
- Holeva, V.; Nikopoulou, V.A.; Lytridis, C.; Bazinas, C.; Kechayas, P.; Sidiropoulos, G.; Papadopoulou, M.; Kerasidou, M.D.; Karatsioras, C.; Geronikola, N.; et al. Effectiveness of a Robot-Assisted Psychological Intervention for Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2024, 5, 577–593. [Google Scholar] [CrossRef]
- Salimi, Z.; Jenabi, E.; Bashirian, S. Are social robots ready yet to be used in care and therapy of autism spectrum disorder: A systematic review of randomized controlled trials. Neurosci. Biobehav. Rev. 2021, 129, 1–16. [Google Scholar] [CrossRef]
- Yun, S.S.; Choi, J.; Park, S.K.; Bong, G.Y.; Yoo, H. Social skills training for children with autism spectrum disorder using a robotic behavioral intervention system. Autism Res. 2017, 10, 1306–1323. [Google Scholar] [CrossRef]
- Zhao, M.; Zhao, Q.; Liu, Q.; Li, N.; Peng, H.; Hu, B. A humanoid robot used as an assistive intervention tool for children with autism spectrum disorder: A preliminary research. In Proceedings of the Brain and Health Informatics: International Conference, BHI 2013, Maebashi, Japan, 29–31 October 2013; Springer International Publishing: Berlin/Heidelberg, Germany, 2013; pp. 336–347. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A.; PAFS consensus group. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef]
- American Psychiatric Association, DSM Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S.L. Autism Diagnostic Observation Schedule (ADOS-2) Modules 1–4; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. Vineland Adaptive Behaviour Scale, 2nd ed.; Pearson Assessments Press: Minneapolis, MN, USA, 2005. [Google Scholar]
- Cornoldi, C.; Giofrè, D.; Belacchi, C. Leiter-3 Leiter International Performance Scale Third Edition Standardizzazione Italiana [Italian Standardization]; Giunti, O.S., Ed.; Raffaello Cortina Editore: Milan, Italiy, 2016. [Google Scholar]
- Cianchetti, C.; Fancello, G.S. Test TVL. Test di Valutazione del Linguaggio. Livello Prescolare; Edizioni Erickson: Trento, Italy, 1997; Volume 16. [Google Scholar]
- Tager-Flusberg, H.; Kasari, C. Minimally verbal school-aged children with autism spectrum disorder: The neglected end of the spectrum. Autism Res. 2013, 6, 468–478. [Google Scholar] [CrossRef]
- Bal, V.H.; Katz, T.; Bishop, S.L.; Krasileva, K. Understanding definitions of minimally verbal across instruments: Evidence for subgroups within minimally verbal children and adolescents with autism spectrum disorder. J. Child Psychol. Psychiatry 2016, 57, 1424–1433. [Google Scholar] [CrossRef]
- Scassellati, B.; Admoni, H.; Matarić, M. Robots for use in autism research. Annu. Rev. Biomed. Eng. 2012, 14, 275–294. [Google Scholar] [CrossRef]
- Diehl, J.J.; Schmitt, L.M.; Villano, M.; Crowell, C.R. The Clinical Use of Robots for Individuals with Autism Spectrum Disorders: A Critical Review. Res. Autism Spectr. Disord. 2012, 6, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Anzalone, S.M.; Tilmont, E.; Boucenna, S.; Xavier, J.; Jouen, A.L.; Bodeau, N.; Maharatna, K.; Chetouani, M.; Cohen, D.; MICHELANGELO Study Group. How children with autism spectrum disorder behave and explore the 4-dimensional (spatial 3D+ time) environment during a joint attention induction task with a robot. Res. Autism Spectr. Disord. 2014, 8, 814–826. [Google Scholar] [CrossRef]
- Bekele, E.; Crittendon, J.A.; Swanson, A.; Sarkar, N.; Warren, Z.E. Pilot clinical application of an adaptive robotic system for young children with autism. Autism 2013, 18, 598–608. [Google Scholar] [CrossRef] [PubMed]
- Shamsuddin, S.; Yussof, H.; Mohamed, S.; Hanapiah, F.A.; Ismail, L.I. Stereotyped behavior of autistic children with lower IQ level in HRI with a humanoid robot. In Proceedings of the 2013 IEEE Workshop on Advanced Robotics and its Social Impacts, Tokyo, Japan, 7–9 November 2013; pp. 175–180. [Google Scholar]
- Warren, Z.E.; Zheng, Z.; Swanson, A.R.; Bekele, E.; Zhang, L.; Crittendon, J.A.; Sarkar, N. Can robotic interaction improve joint attention skills? J. Autism Dev. Disord. 2013, 45, 3726–3734. [Google Scholar] [CrossRef]
- Schlink, A.; Kasari, C. Characterizing social communication among minimally verbal children with autism: An application of item response theory. Autism Res. 2024, 17, 1830–1843. [Google Scholar] [CrossRef]
- Scassellati, B.; Boccanfuso, L.; Huang, C.M.; Mademtzi, M.; Qin, M.; Salomons, N.; Ventola, P.; Shic, F. Improving social skills in children with ASD using a long-term, in-home social robot. Sci. Robot. 2018, 3, eaat7544. [Google Scholar] [CrossRef]
- Wetherby, A.M.; Watt, N.; Morgan, L.; Shumway, S. Social communication profiles of children with autism spectrum disorders late in the second year of life. J. Autism Dev. Disord. 2007, 37, 960–975. [Google Scholar] [CrossRef]
- Kasari, C.; Brady, N.; Lord, C.; Tager-Flusberg, H. Assessing the minimally verbal school-aged child with autism spectrum disorder. Autism Res. 2013, 6, 479–493. [Google Scholar] [CrossRef]
- Srinivasan, S.M.; Eigsti, I.M.; Gifford, T.; Bhat, A.N. The effects of embodied rhythm and robotic interventions on the spontaneous and responsive verbal communication skills of children with Autism Spectrum Disorder (ASD): A further outcome of a pilot randomized controlled trial. Res. Autism Spectr. Disord. 2016, 27, 73–87. [Google Scholar] [CrossRef]
- Charman, T.; Drew, A.; Baird, C.; Baird, G. Measuring early language development in preschool children with autism spectrum disorder using the MacArthur Communicative Development Inventory (Infant Form). J. Child Lang. 2003, 30, 213–236. [Google Scholar] [CrossRef]
- Ray-Subramanian, C.E.; Ellis Weismer, S. Receptive and expressive language as predictors of restricted and repetitive behaviors in young children with autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 2113–2120. [Google Scholar] [CrossRef] [PubMed]
- Conti-Ramsden, G.; St Clair, M.C.; Pickles, A.; Durkin, K. Developmental trajectories of verbal and nonverbal skills in individuals with a history of specific language impairment: From childhood to adolescence. J. Speech Lang. Hear. Res. 2012, 55, 1716–1735. [Google Scholar] [CrossRef] [PubMed]
- Kasari, C.; Kaiser, A.; Goods, K.; Nietfeld, J.; Mathy, P.; Landa, R.; Murphy, S.; Almirall, D. Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, G. Autism Early Intervention—Progress, Steps Backward, and the Reconciliation of Conflicting Narratives. Curr. Psychiatry Rep. 2024, 26, 753–760. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Group | Control Group | Total | |
|---|---|---|---|
| Final Sample (n) | 19 | 18 | 37 |
| Females (n, %) | 3 (15.8%) | 3 (16.7%) | 6 (16.2%) |
| Males (n, %) | 16 (84.2%) | 15 (83.3%) | 31 (83.8%) |
| Age (years, mean ± SD) | 8.1 ± 2.5 | 7.3 ± 1.7 | 7.7 ± 2.2 |
| Leiter | 73.3 ± 14.8 | 74.6 ± 14.9 | 73.9 ± 14.6 |
| VABS | 67.5 ± 20.3 | 71.0 ± 14.2 | 69.2 ± 17.5 |
| Ados total scors | 13.4 ± 5.3 | 14.6 ± 5.5 | 14.0 ± 5.4 |
| Comparison score | 6.5 ± 1.6 | 6.8 ± 1.9 | 6.6 ± 1.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Cara, M.; La Fauci, M.; Tresoldi, M.; Caputo, M.R.; Borzelli, D.; Maggio, R.; Campestre, C.; Barbera, A.; Piccolo, A.; De Domenico, C.; et al. Enhancing Communication in Minimally Verbal Autistic Children: A Study on NAO-Assisted Therapy. J. Clin. Med. 2025, 14, 3735. https://doi.org/10.3390/jcm14113735
Di Cara M, La Fauci M, Tresoldi M, Caputo MR, Borzelli D, Maggio R, Campestre C, Barbera A, Piccolo A, De Domenico C, et al. Enhancing Communication in Minimally Verbal Autistic Children: A Study on NAO-Assisted Therapy. Journal of Clinical Medicine. 2025; 14(11):3735. https://doi.org/10.3390/jcm14113735
Chicago/Turabian StyleDi Cara, Marcella, Margherita La Fauci, Maria Tresoldi, Maria Rita Caputo, Daniele Borzelli, Roberta Maggio, Caterina Campestre, Antonella Barbera, Adriana Piccolo, Carmela De Domenico, and et al. 2025. "Enhancing Communication in Minimally Verbal Autistic Children: A Study on NAO-Assisted Therapy" Journal of Clinical Medicine 14, no. 11: 3735. https://doi.org/10.3390/jcm14113735
APA StyleDi Cara, M., La Fauci, M., Tresoldi, M., Caputo, M. R., Borzelli, D., Maggio, R., Campestre, C., Barbera, A., Piccolo, A., De Domenico, C., Di Blasi, M., Calabrò, R. S., Tripodi, E., Impallomeni, C., & Cucinotta, F. (2025). Enhancing Communication in Minimally Verbal Autistic Children: A Study on NAO-Assisted Therapy. Journal of Clinical Medicine, 14(11), 3735. https://doi.org/10.3390/jcm14113735