
Long-Term Antithrombotic Therapy in Patients with Atrial Fibrillation and Percutaneous Coronary Intervention

 ,
,  , ,
, ,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Antithrombotic Therapy in AF-PCI Patients
3. Observational and Randomized Studies of Long-Term Antithrombotic Regimens in AF-PCI
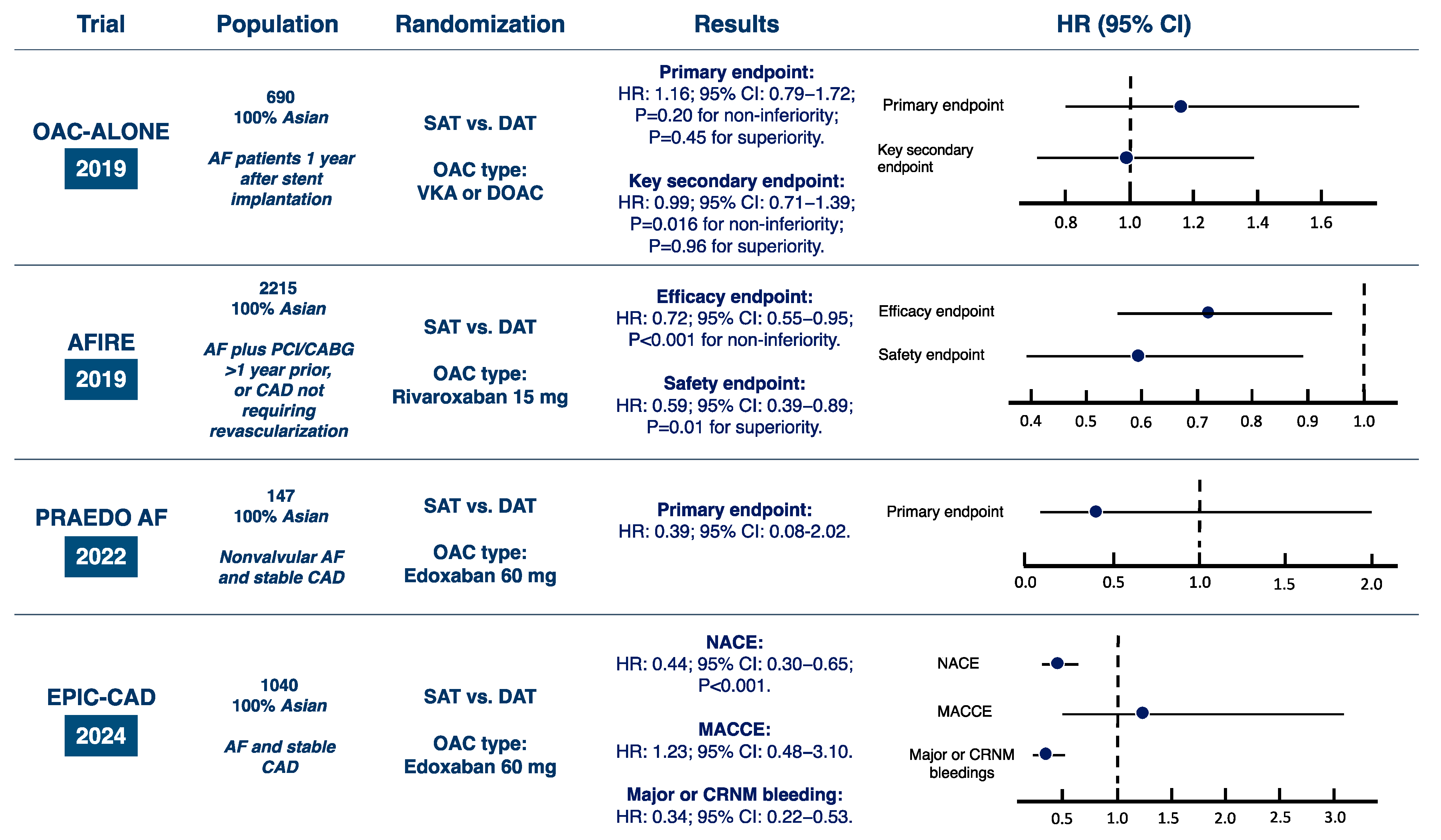
3.1. OAC-ALONE Trial
3.2. AFIRE Trial
3.3. PRAEDO AF Trial
3.4. MASTER DAPT Trial Sub-Analysis
3.5. EPCIC-CAD Trial
3.6. Observational Studies
4. Synthesis of the Available Evidence from Meta-Analyses
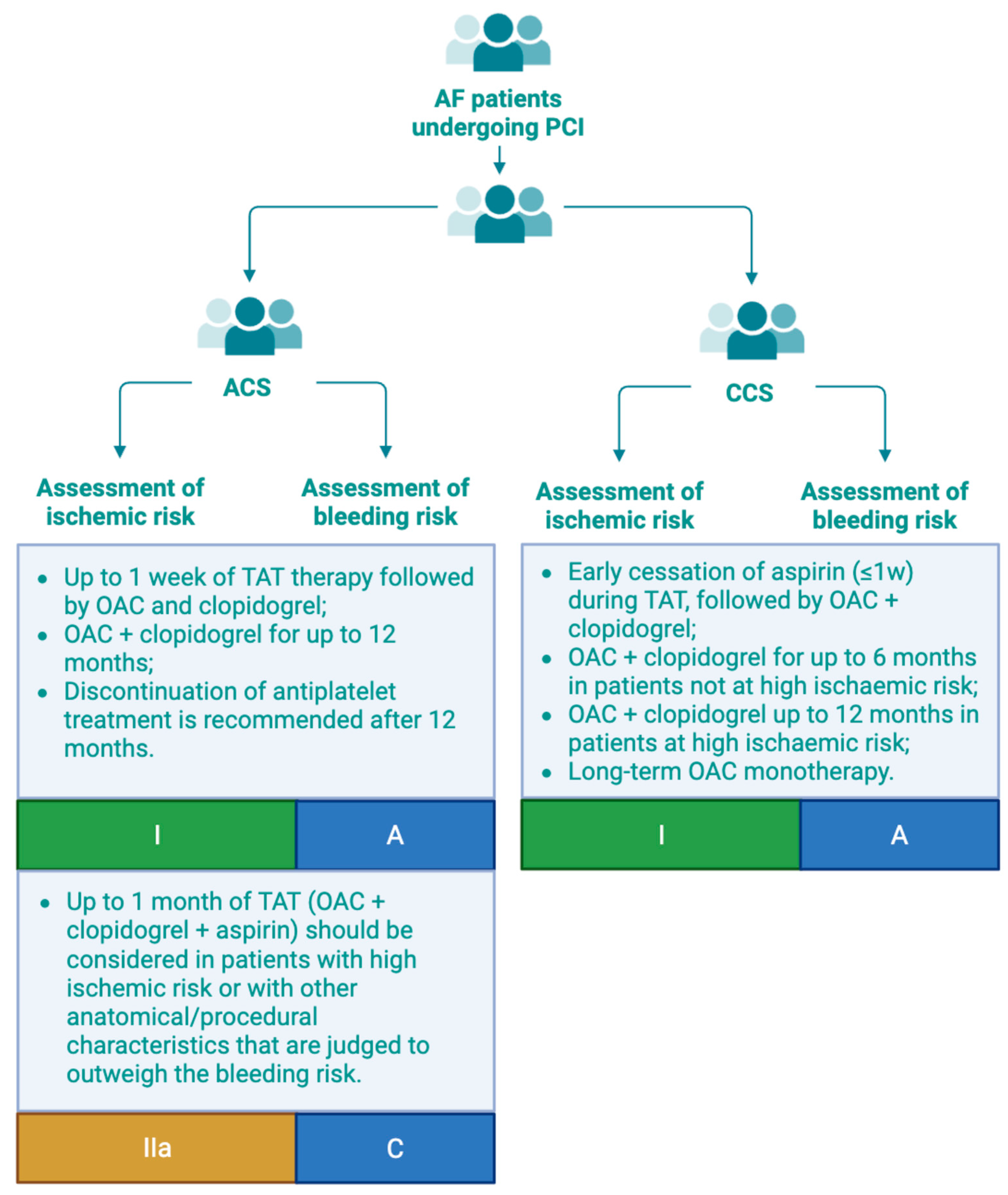
5. Practical Recommendations by Current Guidelines
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sagris, M.; Vardas, E.P.; Theofilis, P.; Antonopoulos, A.S.; Oikonomou, E.; Tousoulis, D. Atrial fibrillation: Pathogenesis, predisposing factors, and genetics. Int. J. Mol. Sci. 2022, 23, 6. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, I.C.; Rienstra, M.; Bunting, K.V.; Casado-Arroyo, R.; Caso, V.; Crijns, H.J.G.M.; De Potter, T.J.R.; Dwight, J.; Guasti, L.; Hanke, T.; et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2024, 45, 3314–3414. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Huber, K.; Mehran, R.; Lip, G.Y.; Faxon, D.P.; Granger, C.B.; Vranckx, P.; Lopes, R.D.; Montalescot, G.; Cannon, C.P.; et al. Management of Antithrombotic Therapy in Atrial Fibrillation Patients Undergoing PCI: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 83–99. [Google Scholar] [CrossRef]
- Calabrò, P.; Niccoli, G.; Gragnano, F.; Grove, E.L.; Vergallo, R.; Mikhailidis, D.P.; Patti, G.; Spaccarotella, C.; Katsiki, N.; Masiero, G.; et al. Are we ready for a gender-specific approach in interventional cardiology? Int. J. Cardiol. 2019, 286, 226–233. [Google Scholar] [CrossRef]
- Gragnano, F.; Capolongo, A.; Micari, A.; Costa, F.; Garcia-Ruiz, V.; De Sio, V.; Terracciano, F.; Cesaro, A.; Moscarella, E.; Coletta, S.; et al. Clinical Medicine Antithrombotic Therapy Optimization in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention. J. Clin. Med. 2023, 13, 98. [Google Scholar] [CrossRef]
- De Sio, V.; Gragnano, F.; Capolongo, A.; Terracciano, F.; Maddaluna, P.; Guarnaccia, N.; Verde, G.; Cesaro, A.; Moscarella, E.; Costa, F.; et al. Antithrombotic therapy in patients with atrial high-rate episodes (AHREs): Current evidence and open questions. Int. J. Cardiol. 2025, 422, 132921. [Google Scholar] [CrossRef] [PubMed]
- De Caterina, R.; Agewall, S.; Andreotti, F.; Angiolillo, D.J.; Bhatt, D.L.; A Byrne, R.; Collet, J.-P.; Eikelboom, J.; Fanaroff, A.C.; Gibson, C.M.; et al. Great Debate: Triple antithrombotic therapy in patients with atrial fibrillation undergoing coronary stenting should be limited to 1 week. Eur. Heart J. 2022, 43, 3512–3527. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef]
- Gragnano, F.; van Klaveren, D.; Heg, D.; Räber, L.; Krucoff, M.W.; Raposeiras-Roubín, S.; Berg, J.M.T.; Leonardi, S.; Kimura, T.; Corpataux, N.; et al. Derivation and Validation of the PRECISE-HBR Score to Predict Bleeding After Percutaneous Coronary Intervention. Circulation 2024, 151, 343–355. [Google Scholar] [CrossRef]
- Gargiulo, G.; Goette, A.; Tijssen, J.; Eckardt, L.; Lewalter, T.; Vranckx, P.; Valgimigli, M. Safety and efficacy outcomes of double vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials. Eur. Heart J. 2019, 40, 3757–3767. [Google Scholar] [CrossRef]
- Galli, M.; Gragnano, F.; Berteotti, M.; Marcucci, R.; Gargiulo, G.; Calabrò, P.; Terracciano, F.; Andreotti, F.; Patti, G.; De Caterina, R.; et al. Antithrombotic Therapy in High Bleeding Risk, Part I: Percutaneous Cardiac Interventions. JACC Cardiovasc. Interv. 2024, 17, 2197–2215. [Google Scholar] [CrossRef] [PubMed]
- Abraham, N.S.; Hartman, C.; Richardson, P.; Castillo, D.; Street, R.L.; Naik, A.D. Risk of Lower and upper gastrointestinal bleeding, transfusions, and hospitalizations with complex antithrombotic therapy in elderly patients. Circulation 2013, 128, 1869–1877. [Google Scholar] [CrossRef] [PubMed]
- Gragnano, F.; Calabro, P.; Valgimigli, M. Is triple antithrombotic therapy, or rather its duration and composition, the true culprit for the excess of bleeding events observed in patients with atrial fibrillation undergoing coronary intervention? Eur. Heart J. 2019, 40, 216–217. [Google Scholar] [CrossRef]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 83, 109–279. [Google Scholar] [CrossRef]
- Sørensen, R.; Hansen, M.L.; Abildstrom, S.Z.; Hvelplund, A.; Andersson, C.; Jørgensen, C.; Madsen, J.K.; Hansen, P.R.; Køber, L.; Torp-Pedersen, C.; et al. Risk of bleeding in patients with acute myocardial infarction treated with different combinations of aspirin, clopidogrel, and vitamin K antagonists in Denmark: A retrospective analysis of nationwide registry data. Lancet 2009, 374, 1967–1974. [Google Scholar] [CrossRef]
- Chiarito, M.; Cao, D.; Cannata, F.; Godino, C.; Lodigiani, C.; Ferrante, G.; Lopes, R.D.; Alexander, J.H.; Reimers, B.; Condorelli, G.; et al. Direct Oral Anticoagulants in Addition to Antiplatelet Therapy for Secondary Prevention After Acute Coronary Syndromes: A Systematic Review and Meta-analysis. JAMA Cardiol. 2018, 3, 234–241. [Google Scholar] [CrossRef]
- Bassand, J.-P.; Apenteng, P.N.; Atar, D.; Camm, A.J.; Cools, F.; Corbalan, R.; A Fitzmaurice, D.; Fox, K.A.; Goto, S.; Haas, S.; et al. GARFIELD-AF: A worldwide prospective registry of patients with atrial fibrillation at risk of stroke. Future Cardiol. 2021, 17, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Ancedy, Y.; Lecoq, C.; Etienne, C.S.; Ivanes, F.; Angoulvant, D.; Babuty, D.; Lip, G.Y.; Fauchier, L. Antithrombotic management in patients with atrial fibrillation undergoing coronary stent implantation: What is the impact of guideline adherence? Int. J. Cardiol. 2016, 203, 987–994. [Google Scholar] [CrossRef]
- Alexander, J.H.; Wojdyla, D.; Vora, A.N.; Thomas, L.; Granger, C.B.; Goodman, S.G.; Aronson, R.; Windecker, S.; Mehran, R.; Lopes, R.D. Risk/Benefit Tradeoff of Antithrombotic Therapy in Patients With Atrial Fibrillation Early and Late After an Acute Coronary Syndrome or Percutaneous Coronary Intervention: Insights From AUGUSTUS. Circulation 2020, 141, 1618–1627. [Google Scholar] [CrossRef]
- Fanaroff, A.C.; Li, S.; Marquis-Gravel, G.; Giri, J.; Lopes, R.D.; Piccini, J.P.; Wang, T.Y. Atrial Fibrillation and Coronary Artery Disease: A Long-Term Perspective on the Need for Combined Antithrombotic Therapy. Circ. Cardiovasc. Interv. 2021, 14, E011232. [Google Scholar] [CrossRef]
- Lamberts, M.; Gislason, G.H.; Lip, G.Y.; Lassen, J.F.; Olesen, J.B.; Mikkelsen, A.P.; Sørensen, R.; Køber, L.; Torp-Pedersen, C.; Hansen, M.L. Antiplatelet therapy for stable coronary artery disease in atrial fibrillation patients taking an oral anticoagulant: A nationwide cohort study. Circulation 2014, 129, 1577–1585. [Google Scholar] [CrossRef]
- Jensen, T.; Thrane, P.G.; Olesen, K.K.W.; Würtz, M.; Mortensen, M.B.; Gyldenkerne, C.; Thim, T.; Nørgaard, B.L.; Jensen, J.M.; Kristensen, S.D.; et al. Antithrombotic treatment beyond 1 year after percutaneous coronary intervention in patients with atrial fibrillation. Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Matsumura-Nakano, Y.; Shizuta, S.; Komasa, A.; Morimoto, T.; Masuda, H.; Shiomi, H.; Goto, K.; Nakai, K.; Ogawa, H.; Kobori, A.; et al. Open-Label Randomized Trial Comparing Oral Anticoagulation With and Without Single Antiplatelet Therapy in Patients With Atrial Fibrillation and Stable Coronary Artery Disease Beyond 1 Year After Coronary Stent Implantation. Circulation 2019, 139, 604–616. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, S.; Kaikita, K.; Akao, M.; Ako, J.; Matoba, T.; Nakamura, M.; Miyauchi, K.; Hagiwara, N.; Kimura, K.; Hirayama, A.; et al. Antithrombotic Therapy for Atrial Fibrillation with Stable Coronary Disease. N. Engl. J. Med. 2019, 381, 1103–1113. [Google Scholar] [CrossRef]
- Noda, T.; Nochioka, K.; Kaikita, K.; Akao, M.; Ako, J.; Matoba, T.; Nakamura, M.; Miyauchi, K.; Hagiwara, N.; Kimura, K.; et al. Antithrombotic monotherapy for stable coronary artery disease and atrial fibrillation patients with and without prior coronary artery revascularization: Insights from the AFIRE trial. Eur. Heart J. 2023, 44 (Suppl. S1), ehac779-052. [Google Scholar] [CrossRef]
- Fukamachi, D.; Okumura, Y.; Matsumoto, N.; Tachibana, E.; Oiwa, K.; Ichikawa, M.; Haruta, H.; Nomoto, K.; Arima, K.; Hirayama, A. Edoxaban Monotherapy in Nonvalvular Atrial Fibrillation Patients with Coronary Artery Disease. J. Interv. Cardiol. 2022, 2022, 5905022. [Google Scholar] [CrossRef]
- Valgimigli, M.; Frigoli, E.; Vranckx, P.; Ozaki, Y.; Morice, M.-C.; Chevalier, B.; Onuma, Y.; Windecker, S.; Delorme, L.; Kala, P.; et al. Impact of Medication Nonadherence in a Clinical Trial of Dual Antiplatelet Therapy. J. Am. Coll. Cardiol. 2022, 80, 766–778. [Google Scholar] [CrossRef]
- Cho, M.S.; Kang, D.-Y.; Ahn, J.-M.; Yun, S.-C.; Oh, Y.-S.; Lee, C.H.; Choi, E.-K.; Lee, J.H.; Kwon, C.H.; Park, G.-M.; et al. Edoxaban Antithrombotic Therapy for Atrial Fibrillation and Stable Coronary Artery Disease. N. Engl. J. Med. 2024, 391, 2075–2086. [Google Scholar] [CrossRef] [PubMed]
- Smits, P.C.; Frigoli, E.; Tijssen, J.; Jüni, P.; Vranckx, P.; Ozaki, Y.; Morice, M.-C.; Chevalier, B.; Onuma, Y.; Windecker, S.; et al. Abbreviated Antiplatelet Therapy in Patients at High Bleeding Risk With or Without Oral Anticoagulant Therapy After Coronary Stenting: An Open-Label, Randomized, Controlled Trial. Circulation 2021, 144, 1196–1211. [Google Scholar] [CrossRef]
- Valgimigli, M.; Frigoli, E.; Heg, D.; Tijssen, J.; Jüni, P.; Vranckx, P.; Ozaki, Y.; Morice, M.-C.; Chevalier, B.; Onuma, Y.; et al. Dual Antiplatelet Therapy after PCI in Patients at High Bleeding Risk. N. Engl. J. Med. 2021, 385, 1643–1655. [Google Scholar] [CrossRef]
- Montalto, C.; Costa, F.; Leonardi, S.; Micari, A.; A Oreglia, J.; Vranckx, P.; Capodanno, D.; Berg, J.T.; Lopes, R.D.; Valgimigli, M. Dual antiplatelet therapy duration after percutaneous coronary intervention in patients with indication to oral anticoagulant therapy. A systematic review and meta-analysis of randomized controlled trials. Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Ahsan, A.; Shafiq, A.; Ahmed, R.; Alam, M.; Sabouret, P.; Rana, J.S.; Fonarow, G.C. Meta-Analysis Comparing Oral Anticoagulant Monotherapy Versus Dual Antithrombotic Therapy in Patients With Atrial Fibrillation and Stable Coronary Artery Disease. Clin. Cardiol. 2024, 47, e70026. [Google Scholar] [CrossRef] [PubMed]
- Rashedi, S.; Keykhaei, M.; Sato, A.; Steg, P.G.; Piazza, G.; Eikelboom, J.W.; Lopes, R.D.; Bonaca, M.P.; Yasuda, S.; Ogawa, H.; et al. Anticoagulation and Antiplatelet Therapy for Atrial Fibrillation and Stable Coronary Disease: Meta-Analysis of Randomized Trials. J. Am. Coll. Cardiol. 2025, 85, 1189–1203. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Hong, S.-J.; Gragnano, F.; Chalkou, K.; Franzone, A.; da Costa, B.R.; Baber, U.; Kim, B.-K.; Jang, Y.; Chen, S.-L.; et al. De-escalation to ticagrelor monotherapy versus 12 months of dual antiplatelet therapy in patients with and without acute coronary syndromes: A systematic review and individual patient-level meta-analysis of randomised trials. Lancet 2024, 404, 937–948. [Google Scholar] [CrossRef]
- Cesaro, A.; Taglialatela, V.; Gragnano, F.; Moscarella, E.; Fimiani, F.B.; Conte, M.; Barletta, V.; Monda, E.; Limongelli, G.; Severino, S.; et al. Low-Dose Ticagrelor in Patients With High Ischemic Risk and Previous Myocardial Infarction: A Multicenter Prospective Real-World Observational Study. J. Cardiovasc. Pharmacol. 2020, 76, 173–180. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study | Year | Sample Size | Design | CHA2DS2-VASc Score (Median) | HAS-BLED Score (Median) | Monotherapy Regimen | Dual Therapy Regimen | Endpoints | Follow-Up (Median) |
|---|---|---|---|---|---|---|---|---|---|
| OAC-ALONE [23] | 2019 | 696 | RCT | 4.6 | 2 | Warfarin (75.2%) or DOACs (24.8%) | Warfarin or DOACs plus aspirin or clopidogrel | Primary endpoint: death, MI, stroke, or SE. Key secondary endpoint: primary endpoint or major bleeding (ISTH criteria). | 30 mo. |
| AFIRE [24,25] | 2019 | 2236 | RCT | 4 | 2 | Rivaroxaban 15 mg once daily | Rivaroxaban 15 mg once daily plus aspirin or a P2Y12 inhibitor | Efficacy endpoint: stroke, systemic embolism, MI, unstable angina requiring revascularization, or death. Safety endpoint: major bleeding (ISTH criteria). | 24.1 mo. |
| PRAEDO AF [26] | 2022 | 147 | RCT | 4 | 3 | Edoxaban 60 mg once daily | Edoxaban 60 mg once daily plus clopidogrel | Primary endpoint: major bleeding or clinically significant bleeding (ISTH criteria). | 20.8 mo. |
| EPIC-CAD [28] | 2024 | 1040 | RCT | 4 | 2.2 | Edoxaban 60 mg once daily | Edoxaban 60 mg once daily plus aspirin or a P2Y12 inhibitor | NACE: death, MI, stroke, systemic embolism, unplanned urgent revascularization, major or CRNM bleeding (ISTH criteria). MACCE: death, MI, stroke, or SE. Major or CRNM bleeding. | 12 mo. |
| Meta-Analysis | Year | Sample Size | No. of RCTs Included | RCTs Included | Arms | Endpoints and Results |
|---|---|---|---|---|---|---|
| Montalto et al. [31] | 2023 | 7665 | 5 | WOEST trial; ISAR-TRIPLE trial; AUGUSTUS trial; SAFE-A trial; MASTER DAPT trial. | Abbreviated DAPT regimen vs. extended DAPT strategy (≥3 mo.) |
|
| Ahmed et al. [34] | 2024 | 3945 | 3 | AFIRE; OAC-ALONE; EPIC-CAD. | OAC monotherapy vs. DAT |
|
| Rashedi et al. [35] | 2025 | 4092 | 4 | AFIRE; OAC-ALONE; PRAEDO AF; EPIC-CAD. | OAC monotherapy compared to OAC plus SAPT in patients with AF and stable CAD |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capolongo, A.; De Sio, V.; Gragnano, F.; Galli, M.; Guarnaccia, N.; Maddaluna, P.; Verde, G.; Acerbo, V.; Sabouret, P.; Giacoppo, D.; et al. Long-Term Antithrombotic Therapy in Patients with Atrial Fibrillation and Percutaneous Coronary Intervention. J. Clin. Med. 2025, 14, 3713. https://doi.org/10.3390/jcm14113713
Capolongo A, De Sio V, Gragnano F, Galli M, Guarnaccia N, Maddaluna P, Verde G, Acerbo V, Sabouret P, Giacoppo D, et al. Long-Term Antithrombotic Therapy in Patients with Atrial Fibrillation and Percutaneous Coronary Intervention. Journal of Clinical Medicine. 2025; 14(11):3713. https://doi.org/10.3390/jcm14113713
Chicago/Turabian StyleCapolongo, Antonio, Vincenzo De Sio, Felice Gragnano, Mattia Galli, Natale Guarnaccia, Pasquale Maddaluna, Giuseppe Verde, Vincenzo Acerbo, Pierre Sabouret, Daniele Giacoppo, and et al. 2025. "Long-Term Antithrombotic Therapy in Patients with Atrial Fibrillation and Percutaneous Coronary Intervention" Journal of Clinical Medicine 14, no. 11: 3713. https://doi.org/10.3390/jcm14113713
APA StyleCapolongo, A., De Sio, V., Gragnano, F., Galli, M., Guarnaccia, N., Maddaluna, P., Verde, G., Acerbo, V., Sabouret, P., Giacoppo, D., Conte, M., Coletta, S., Diana, V., Luciani, M., Moscarella, E., Cesaro, A., Pelliccia, F., & Calabrò, P. (2025). Long-Term Antithrombotic Therapy in Patients with Atrial Fibrillation and Percutaneous Coronary Intervention. Journal of Clinical Medicine, 14(11), 3713. https://doi.org/10.3390/jcm14113713