
Oral Bisphosphonates for Colorectal Cancer Prevention: A Meta-Analytic Reappraisal Beyond Bone Health
 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
- (1)
- Randomized controlled trials, prospective or retrospective cohort studies, nested case–control studies, or population-based case–control studies;
- (2)
- The primary outcome was the incidence of colorectal, colon, or rectal cancer;
- (3)
- The study reported relative risks (RRs), odds ratios (ORs), or hazard ratios (HRs), along with 95% confidence intervals or enough data to calculate them;
- (4)
- Bisphosphonate exposure was defined as having at least one documented prescription or dispensation prescription of BPs, or reporting of BPs in a pharmacy record or an interview in at least the last two weeks.
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
2.6. Ethics Statement
3. Results
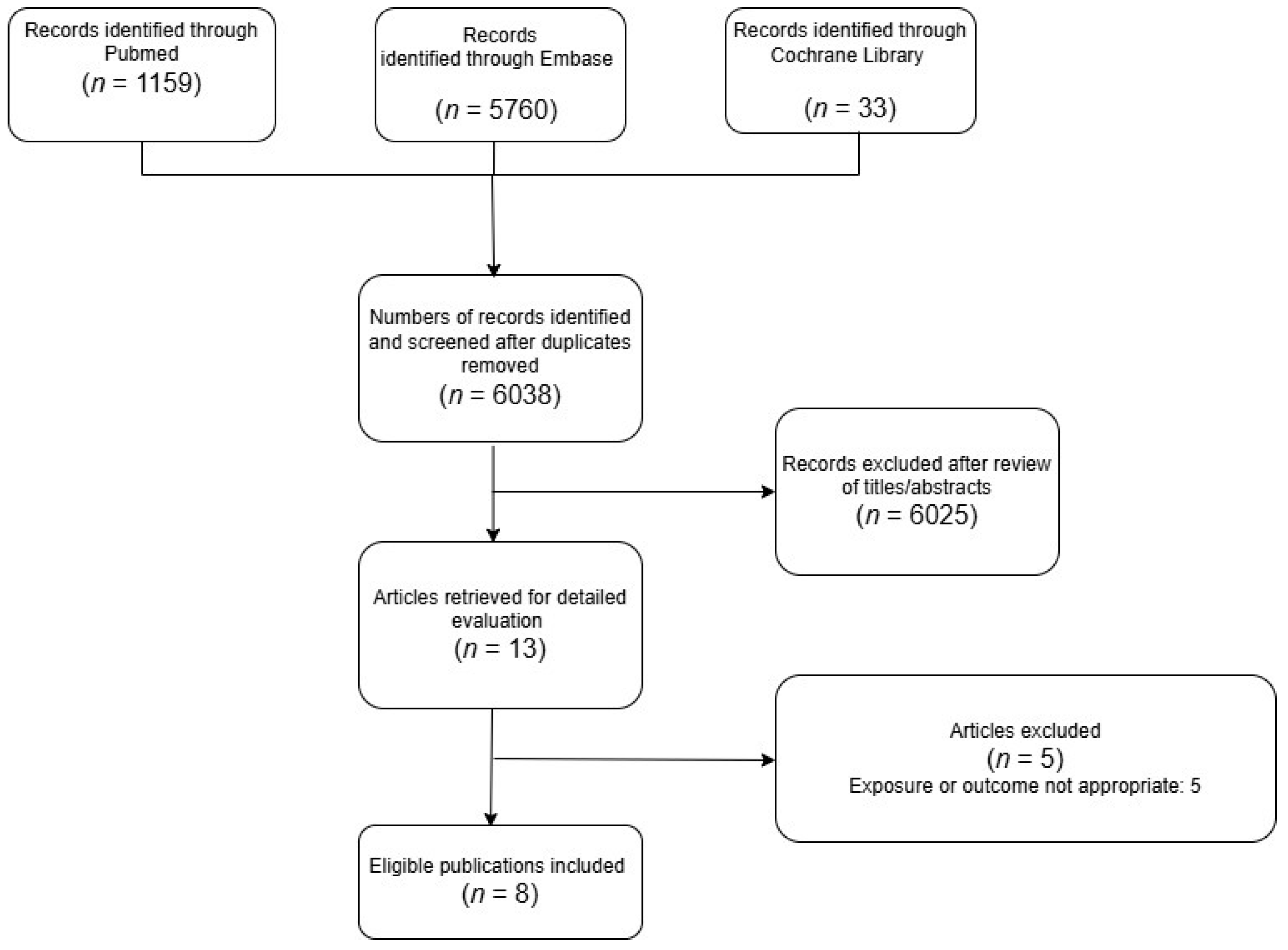
3.1. Literature Search
3.2. Study Characteristics
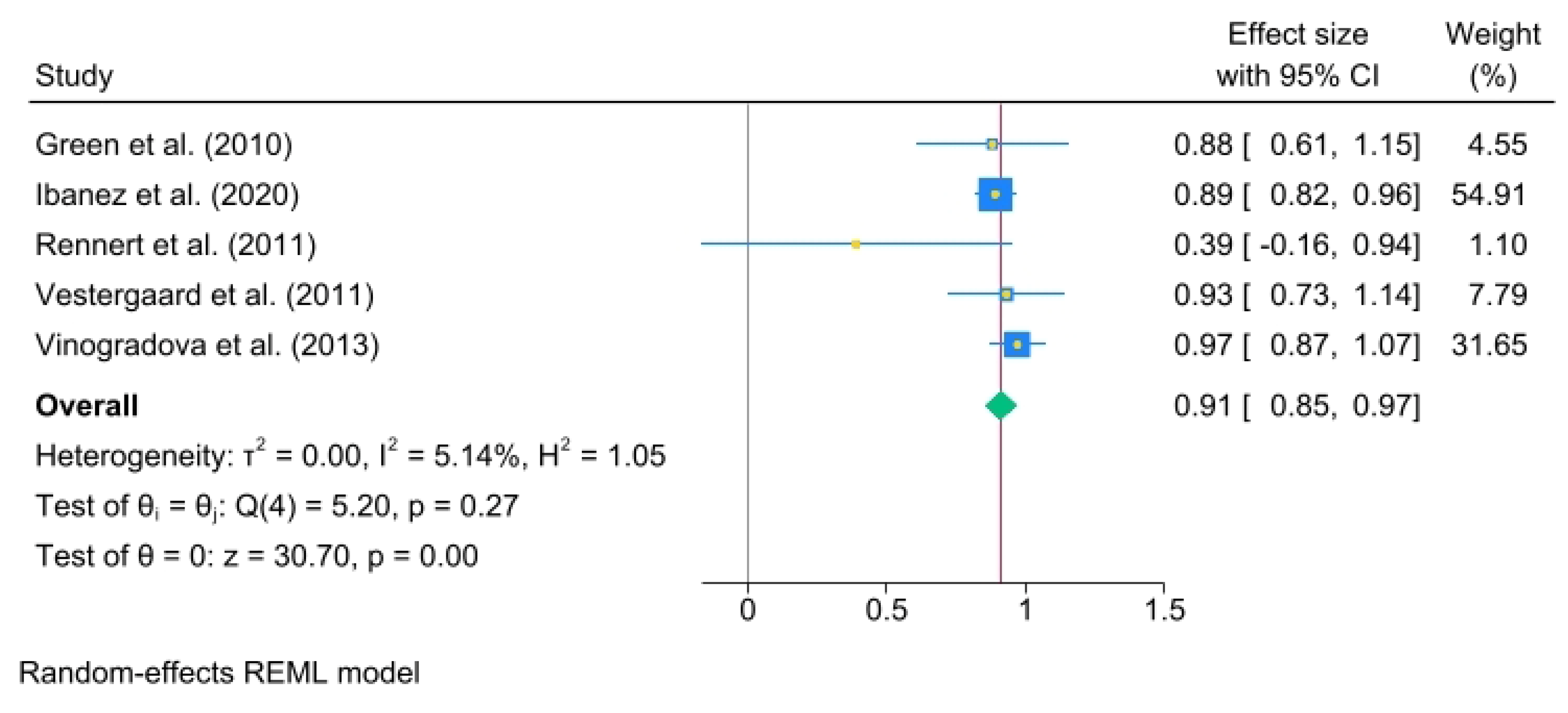
3.3. Duration of Exposure Analysis
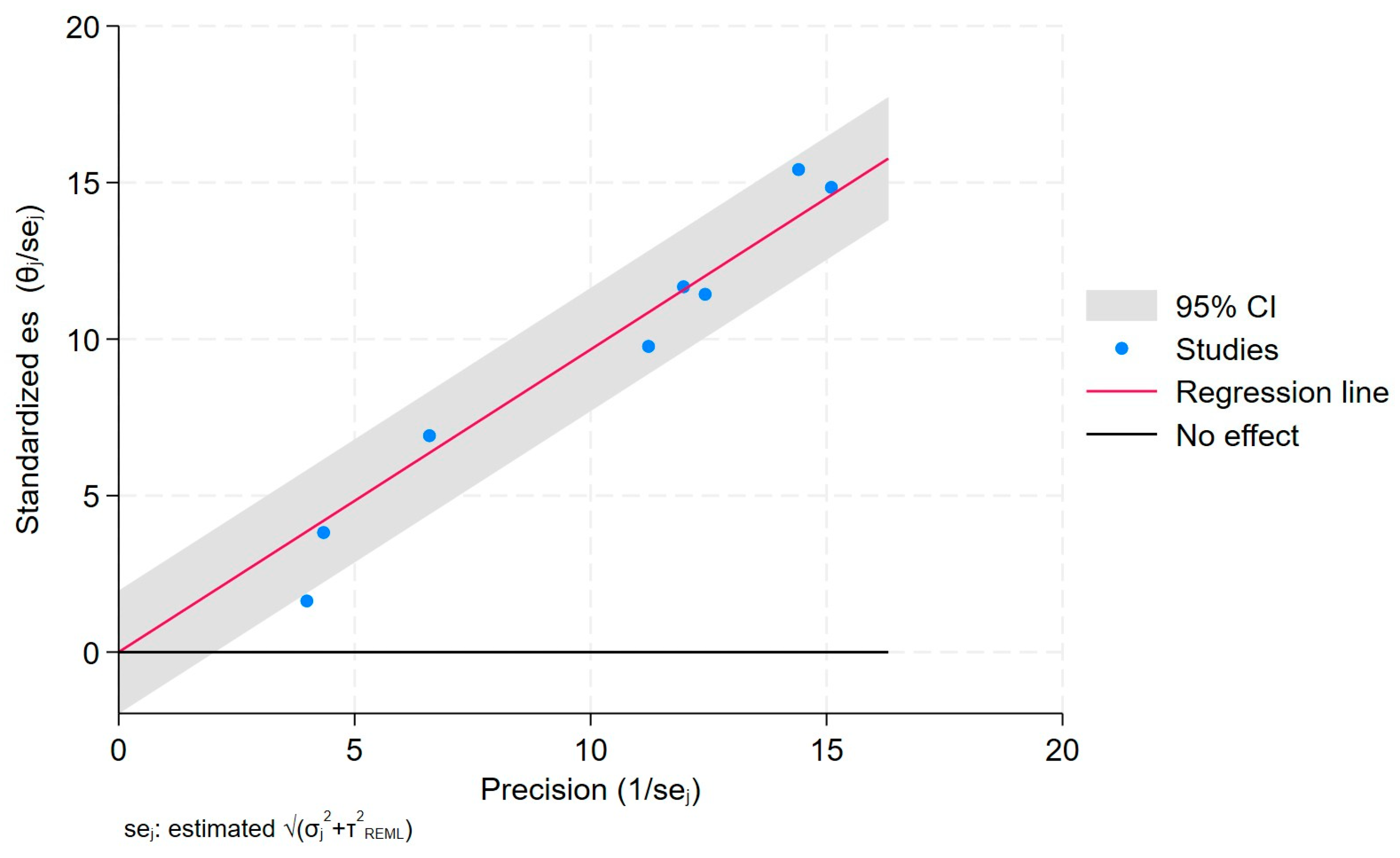
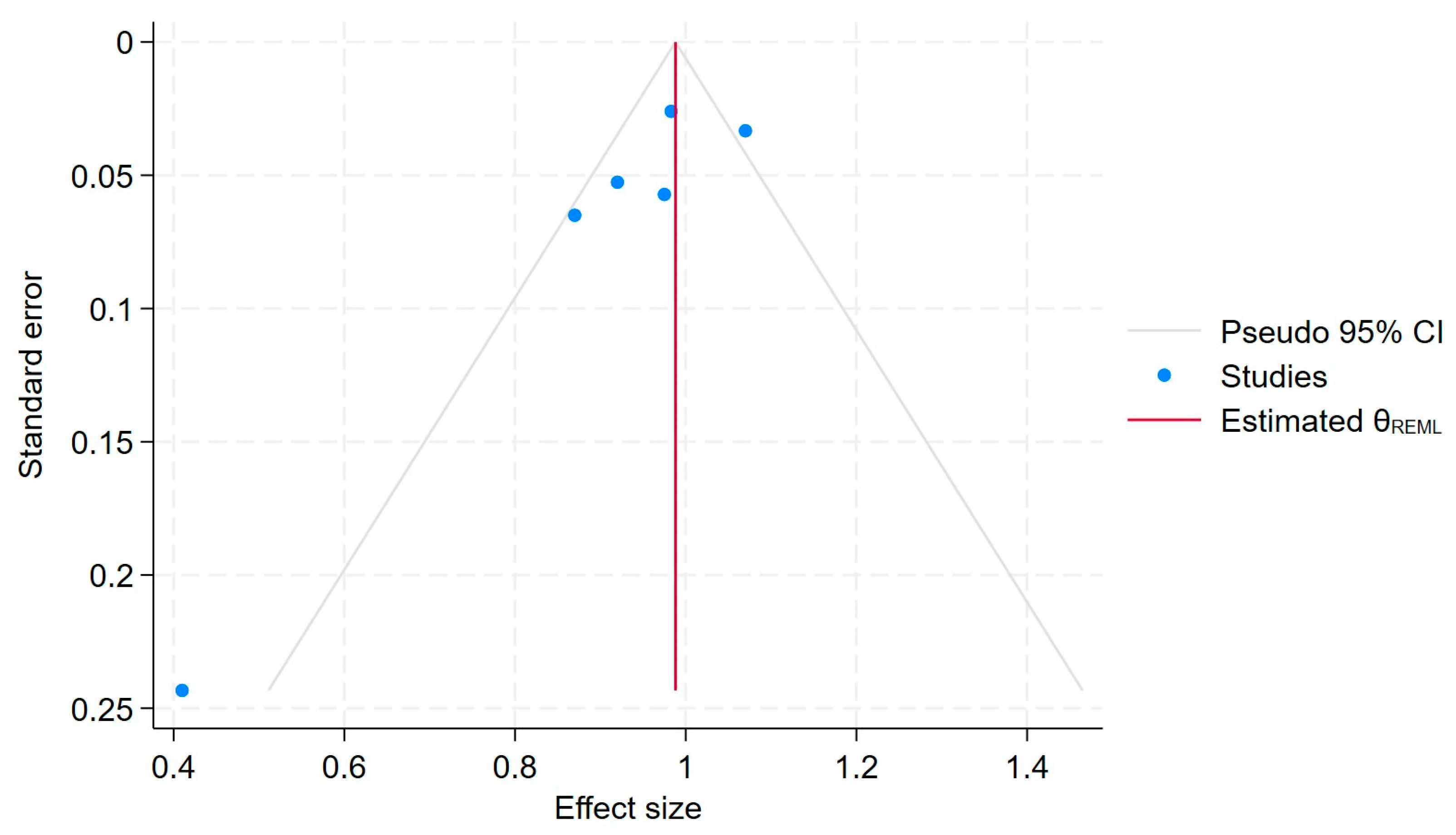
3.4. Heterogeneity and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BP | Bisphosphonate |
| CRC | Colorectal cancer |
| FDA | Food and Drug Administration |
References
- Newcomb, P.A.; Trentham-Dietz, A.; Hampton, J.M. Bisphosphonates for osteoporosis treatment are associated with reduced breast cancer risk. Br. J. Cancer 2010, 102, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, P. Occurrence of gastrointestinal cancer in users of bisphosphonates and other antiresorptive drugs against osteoporosis. Calcif. Tissue Int. 2011, 89, 434–441. [Google Scholar] [CrossRef]
- Watts, N.B.; Bilezikian, J.P.; Camacho, P.M.; Greenspan, S.L.; Harris, S.T.; Hodgson, S.F.; Kleerekoper, M.; Luckey, M.M.; McClung, M.R.; Pollack, R.P.; et al. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the diagnosis and treatment of postmenopausal osteoporosis: Executive summary of recommendations. Endocr. Pract. 2010, 16, 1016–1019. [Google Scholar] [CrossRef] [PubMed]
- Composton, J.; Cooper, A.; Cooper, C.; Francis, R.; Kanis, J.A.; Marsh, D.; McCloskey, E.V.; Reid, D.M.; Selby, P.; Wilkins, M.; et al. Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK. Maturitas 2009, 62, 105–108. [Google Scholar] [CrossRef]
- Heras, P.; Karagiannis, S.; Kritikos, K.; Hatzopoulos, A.; Mitsibounas, D. Ibandronate is effective in preventing skeletal events in patients with bone metastases from colorectal cancer. Eur. J. Cancer Care 2007, 16, 539–542. [Google Scholar] [CrossRef]
- Passarelli, M.N.; Newcomb, P.A.; LaCroix, A.Z.; Lane, D.S.; Ho, G.Y.F.; Chlebowski, R.T. Oral bisphosphonate use and colorectal cancer incidence in the Women’s Health Initiative. J. Bone Miner. Res. 2013, 28, 2043–2048. [Google Scholar] [CrossRef]
- Grant, M.; Mlineritsch, B.; Schippinger, W.; Luschin-Ebengreuth, G.; Pöstlberger, S.; Menzel, C.; Jakesz, R.; Seifert, M.; Hubalek, M.; Bjelic-Radisic, V.; et al. Endocrine therapy plus zoledronic acid in premenopausal breast cancer. N. Engl. J. Med. 2009, 360, 679–691. [Google Scholar]
- Sewing, L.; Steinberg, F.; Schmidt, H.; Göke, R. The bisphosphonate zoledronic acid inhibits the growth of HCT-116 colon carcinoma cells and induces tumor cell apoptosis. Apoptosis 2008, 13, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Luckman, S.P.; Hughes, D.E.; Coxon, F.P.; Graham, R.; Russell, G.; Rogers, M.J. Nitrogen-containing bisphosphonates inhibit the mevalonate pathway and prevent post-translational prenylation of GTP-binding proteins, including Ras. J. Bone Miner. Res. 1998, 13, 581–589. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0; Available online: http://www.handbook.Cochrane.Org (accessed on 17 April 2025).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 17 April 2025).
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Corbeil, R.R.; Searle, S.R. Restricted Maximum Likelihood (REML) Estimation of Variance Components in the Mixed Model. Taylor Fr. 1976, 8, 31–38. [Google Scholar] [CrossRef]
- Van Arendok, J.A.; Tier, B.; Bink, C.; Bovenhuis, H. Restricted maximum likelihood analysis of linkage between genetic markers and quantitative trait loci for a granddaughter design. J. Dairy Sci. 1998, 81, 76–84. [Google Scholar] [CrossRef]
- Smith, S.P.; Graser, H.U. Estimating Variance Components in a Class of Mixed Models by Restricted Maximum Likelihood. J. Dairy Sci. 1986, 69, 1156–1165. [Google Scholar] [CrossRef]
- Choi, D.; Choi, S.; Chang, J.; Park, S.M. Exposure to oral bisphosphonates and risk of gastrointestinal cancer. Osteoroporos Int. 2020, 31, 775–782. [Google Scholar] [CrossRef]
- Green, J.; Czanner, G.; Reeves, G.; Watson, J.; Wise, L.; Beral, V. Oral bisphosphonates and risk of cancer of oesophagus, stomach, and colorectum: Case-control analysis within a UK primary care cohort. BMJ 2010, 341, c4444. [Google Scholar] [CrossRef]
- Ibáñez-Sanz, G.; Guinó, E.; Pontes, C.; Morros, R.; de la Peña-Negro, L.C.; Quijada-Manuitt, M.; Moreno, V. Risk of colorectal cancer in users of bisphosphonates: Analysis of population-based electronic health records. Eur. J. Epidemiol. 2020, 35, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Rennert, G.; Pinchev, M.; Rennert, H.S.; Gruber, S.B. Use of bisphosphonates and reduced risk of colorectal cancer. J. Clin. Oncol. 2011, 29, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Vinogradova, Y.; Coupland, C.; Hippisisle-Cox, J. Exposure to bisphosphonates and risk of gastrointestinal cancers: Series of nested case-control studies with QResearch and CPRD data. BMJ 2013, 346, f114. [Google Scholar] [CrossRef]
- Vogtmann, E.; Corley, D.A.; Almers, L.M.; Cardwell, C.R.; Murray, L.J.; Abnet, C.C. Oral bisphosphonates and colorectal cancer. Sci. Rep. 2017, 7, 44177. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.D. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Khalili, H.; Huang, E.S.; Ogino, S.; Fuchs, C.S.; Chan, A.T. A prospective study of bisphosphonate use and risk of colorectal cancer. J. Clin. Oncol. 2012, 30, 3229–3233. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-Analysis of Observational Studies in Epidemiology A Proposal for Reporting Because of Pressure for Timely. Available online: http://www.wesleyan.edu (accessed on 17 April 2025).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design | Mean Age (yrs) | No. Control | No. Cases | Estimation and 95% C.I. | Study Quality | Adjustment for Covariates | Exposition Assessment |
|---|---|---|---|---|---|---|---|---|
| Choi et al. (2020) [17] | Nationwide retrospective cohort study | Control: 67.10 Cases: 68.90 | 402 | 59 | HR: 1.05 (0.80–1.38) OR: 1.05 (0.80–1.38) | 7 | Age, smoking, alcohol consumption, household income, number of received upper GI endoscopies (only of stomach cancer), number of received lower GI endoscopies (only of colorectal cancer), systolic blood pressure, total cholesterol, and fasting serum glucose | Pharmacy record of filling of a prescription |
| Green et al. (2010) [18] | Nested case–control study | Control: 70.10 Cases: 70.10 | 51,467 | 10,365 | OR: 0.87 (0.77–1.00) | 7 | Age, BMI, smoking status (never, past, current, missing), alcohol intake, prescription of NSAIDs as aspirin, prescription of corticosteroids, prescription of acid-suppressant drugs | One or more prescriptions of oral BPs |
| Ibanez et al. (2020) [19] | Nested case–control study | Control: 75.70 Cases: 75.50 | 15,289 | 2941 | OR: 0.98 (0.93–1.03) | 7 | BMI, ethnicity, family history of CRC, self-reported sports activity, vegetable intake (≥5 portions per day), aspirin use once a day for at least 3 years, statin use for ≥1 year, use of postmenopausal hormones, calcium | One or more dispensations of oral BPs on prescription records |
| Passarelli et al. (2013) [6] | Nationwide retrospective cohort study | -- | 1805 | 126 | HR: 0.88 (0.72–1.72) OR: 0.88 (0.72–1.72) | 7 | Age, gender, region, year, socioeconomic status, body mass index, smoking, alcohol, comorbidities, nonsteroidal anti-inflammatory drugs, propensity score, bisphosphonates, and vitamin D | Interview to which participants were instructed to bring medication bottles/packaging for drugs taken at least twice per week during previous 2 weeks |
| Rennert et al. (2011) [20] | Nationwide retrospective cohort study | Control: 72.00 Cases: 71.10 | 933 | 933 | OR: 0.41 (0.25–0.67) | 7 | BMI, ethnicity, family history of CRC, self-reported sports activity, vegetable consumption (≥5 portions per day), aspirin use once a day for at least 3 years, statin use ≥ 1 year, use of postmenopausal hormones, calcium | Pharmacy record of filling of a prescription |
| Vestergaard et al. (2011) [2] | Nationwide retrospective cohort study | Control: 70.50 Cases: 70.50 | -- | 409 | OR: 0.97 (0.87–1.09) | 7 | Age, gender, use of inhaled corticosteroids and β-agonist as proxy for smoking, alcoholism, antacid drugs, aspirin, and NSAIDs | Pharmacy record of filling of a prescription |
| Vinogradova et al. (2013) [21] | Nested case–control study | Control: 71.60 Cases: 71.50 | 8576 | 1831 | OR: 1.07 (1.00–1.14) | 7 | BMI, smoking status, alcohol consumption, ethnicity, rheumatoid arthritis, osteoporosis and fractures, use of other osteoporosis drugs, vitamin D, NSAIDs, corticosteroids, acid-lowering drugs, years of data, and family history of colorectal cancer, diabetes, colitis, and Crohn’s disease | One or more dispensations of oral BPs on prescription records |
| Vogtmann et al. (2017) [22] | Nested case–control study | Control: 65.94 Cases: 66.40 | 599,534 | 12,505 | OR: 0.92 (0.83–1.02) | 7 | Gender, age at time of index date (+/−2 years), duration of membership prior to index date (+/−1 year), race, and region of residence. Adjusted model additionally included age, smoking, alcohol use, Charlson comorbidity index, use of NSAIDs, and previous lower GI endoscopy | One or more prescriptions of oral BPs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giusto, E.A.; Donghia, R.; Giorgi, C.; Pinton, P.; Fiorica, F. Oral Bisphosphonates for Colorectal Cancer Prevention: A Meta-Analytic Reappraisal Beyond Bone Health. J. Clin. Med. 2025, 14, 3702. https://doi.org/10.3390/jcm14113702
Giusto EA, Donghia R, Giorgi C, Pinton P, Fiorica F. Oral Bisphosphonates for Colorectal Cancer Prevention: A Meta-Analytic Reappraisal Beyond Bone Health. Journal of Clinical Medicine. 2025; 14(11):3702. https://doi.org/10.3390/jcm14113702
Chicago/Turabian StyleGiusto, Enrico Altiero, Rossella Donghia, Carlotta Giorgi, Paolo Pinton, and Francesco Fiorica. 2025. "Oral Bisphosphonates for Colorectal Cancer Prevention: A Meta-Analytic Reappraisal Beyond Bone Health" Journal of Clinical Medicine 14, no. 11: 3702. https://doi.org/10.3390/jcm14113702
APA StyleGiusto, E. A., Donghia, R., Giorgi, C., Pinton, P., & Fiorica, F. (2025). Oral Bisphosphonates for Colorectal Cancer Prevention: A Meta-Analytic Reappraisal Beyond Bone Health. Journal of Clinical Medicine, 14(11), 3702. https://doi.org/10.3390/jcm14113702