

Perioperative Outcomes of Non-Intubated Versus Intubated Anesthesia in Video-Assisted Thoracoscopic Surgery for Early-Stage Non-Small Cell Lung Cancer: A Propensity Score-Matched Analysis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants and Data Sources
2.3. Anesthetic Technique
2.4. Surgical Procedure
2.5. Variables
2.6. Statistical Methods
3. Results
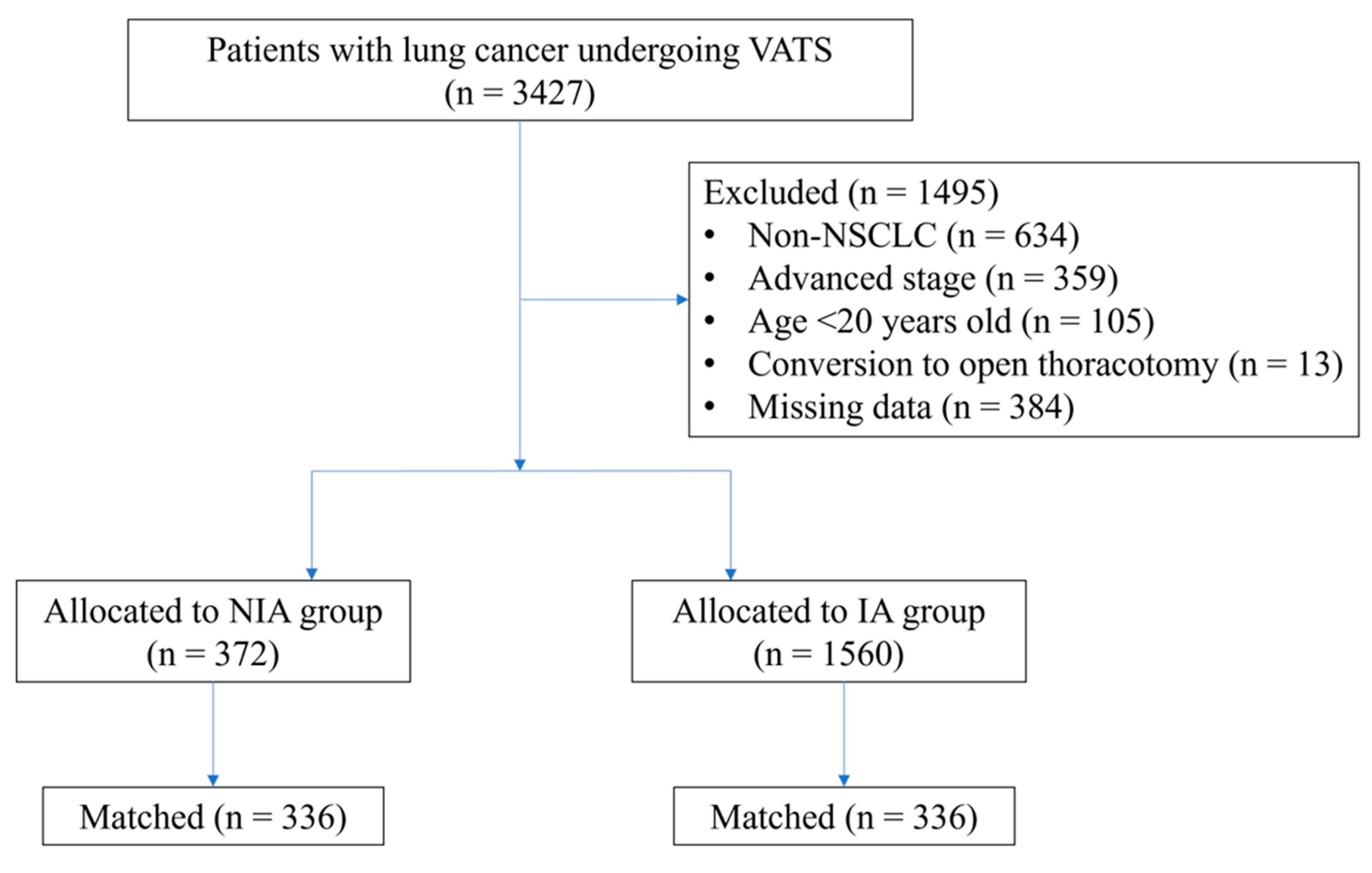
3.1. Patient and Treatment Characteristics
3.2. Perioperative Outcomes
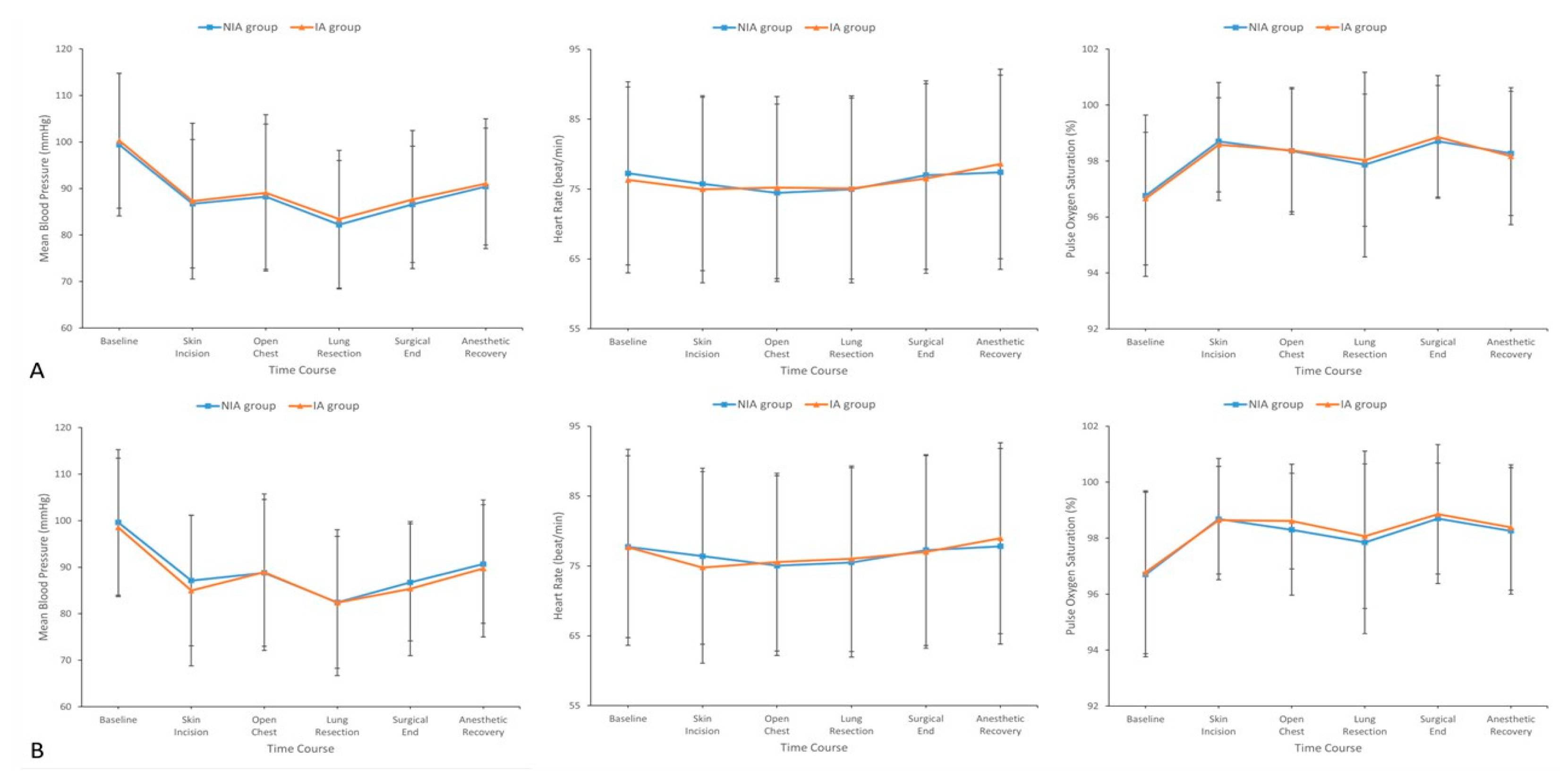
3.3. Intraoperative Hemodynamic Stability
3.4. Subgroup Analyses of Perioperative Complications
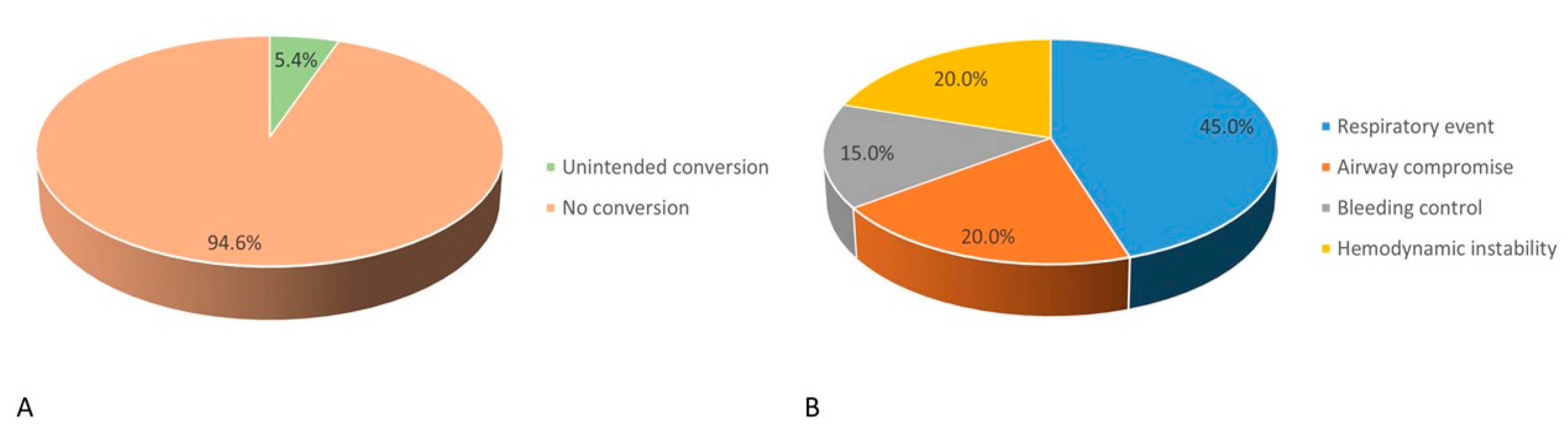
3.5. Incidence and Causes of Conversion to IA
3.6. Risk Factors for Conversion to IA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nasim, F.; Sabath, B.F.; Eapen, G.A. Lung Cancer. Med. Clin. N. Am. 2019, 103, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef] [PubMed]
- Whitson, B.A.; Groth, S.S.; Duval, S.J.; Swanson, S.J.; Maddaus, M.A. Surgery for early-stage non-small cell lung cancer: A systematic review of the videoassisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann. Thorac. Surg. 2008, 86, 2008–2018. [Google Scholar] [CrossRef]
- Zhu, M.; Fu, X.N.; Chen, X. Lobectomy by video-assisted thoracoscopic surgery (VATS) for early stage of non-small cell lung cancer. Front. Med. 2011, 5, 53–60. [Google Scholar] [CrossRef]
- Bernasconi, F.; Piccioni, F. One-lung ventilation for thoracic surgery: Current perspectives. Tumori 2017, 103, 495–503. [Google Scholar] [CrossRef]
- Janik, M.; Juhos, P.; Lučenič, M.; Tarabova, K. Non-intubated Thoracoscopic Surgery-Pros and Cons. Front. Surg. 2021, 8, 801718. [Google Scholar] [CrossRef]
- Koh, L.Y.; Hwang, N.C. Anesthesia for Nonintubated Video-Assisted Thoracoscopic Surgery. J. Cardiothorac. Vasc. Anesth. 2023, 37, 1275–1283. [Google Scholar] [CrossRef]
- Irons, J.F.; Miles, L.F.; Joshi, K.R.; Klein, A.A.; Scarci, M.; Solli, P.; Martinez, G. Intubated Versus Nonintubated General Anesthesia for Video-Assisted Thoracoscopic Surgery-A Case-Control Study. J. Cardiothorac. Vasc. Anesth. 2017, 31, 411–417. [Google Scholar] [CrossRef]
- Shi, Y.; Yu, H.; Huang, L.; Wang, S.; Chi, D.; Chen, C.; Liu, B. Postoperative pulmonary complications and hospital stay after lung resection surgery: A meta-analysis comparing nonintubated and intubated anesthesia. Medicine 2018, 97, e10596. [Google Scholar] [CrossRef]
- Lin, W.L.; Cherng, C.H. Predicting Optimal Insertion Depth of a Left-sided Double-Lumen Endobronchial Tube. J. Cardiothorac. Vasc. Anesth. 2016, 30, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.C.; Huang, T.W.; Tseng, W.C.; Lin, W.L.; Chang, H.; Wu, Z.F. Sevoflurane is an effective adjuvant to propofol-based total intravenous anesthesia for attenuating cough reflex in nonintubated video-assisted thoracoscopic surgery. Medicine 2018, 97, e12927. [Google Scholar] [CrossRef]
- Lohser, J.; Slinger, P. Lung Injury After One-Lung Ventilation: A Review of the Pathophysiologic Mechanisms Affecting the Ventilated and the Collapsed Lung. Anesth. Analg. 2015, 121, 302–318. [Google Scholar] [CrossRef] [PubMed]
- Birim, O.; Maat, A.P.; Kappetein, A.P.; van Meerbeeck, J.P.; Damhuis, R.A.; Bogers, A.J. Validation of the Charlson comorbidity index in patients with operated primary non-small cell lung cancer. Eur. J. Cardiothorac. Surg. 2003, 23, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Fleisher, L.A.; Fleischmann, K.E.; Auerbach, A.D.; Barnason, S.A.; Beckman, J.A.; Bozkurt, B.; Davila-Roman, V.G.; Gerhard-Herman, M.D.; Holly, T.A.; Kane, G.C.; et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J. Am. Coll. Cardiol. 2014, 64, e77–e137. [Google Scholar] [CrossRef]
- Austin, P.C.; Jembere, N.; Chiu, M. Propensity score matching and complex surveys. Stat. Methods Med. Res. 2018, 27, 1240–1257. [Google Scholar] [CrossRef]
- Yu, J.; Tantraworasin, A.; Laohathai, S. Non-intubated versus intubated videoassisted thoracoscopic lobectomy for lung cancer patients. Asian J. Surg. 2024, 47, 402–406. [Google Scholar] [CrossRef]
- Liu, J.; Cui, F.; Pompeo, E.; Gonzalez-Rivas, D.; Chen, H.; Yin, W.; Shao, W.; Li, S.; Pan, H.; Shen, J.; et al. The impact of non-intubated versus intubated anaesthesia on early outcomes of video-assisted thoracoscopic anatomical resection in non-small-cell lung cancer: A propensity score matching analysis. Eur. J. Cardiothorac. Surg. 2016, 50, 920–925. [Google Scholar] [CrossRef]
- Zhang, K.; Chen, H.G.; Wu, W.B.; Li, X.J.; Wu, Y.H.; Xu, J.N.; Jia, Y.B.; Zhang, J. Nonintubated video-assisted thoracoscopic surgery vs. intubated video-assisted thoracoscopic surgery for thoracic disease: A systematic review and metaanalysis of 1,684 cases. J. Thorac. Dis. 2019, 11, 3556–3568. [Google Scholar] [CrossRef]
- Cui, F.; Liu, J.; Li, S.; Yin, W.; Xin, X.; Shao, W.; He, J. Tubeless video-assisted thoracoscopic surgery (VATS) under non-intubated, intravenous anesthesia with spontaneous ventilation and no placement of chest tube postoperatively. J. Thorac. Dis. 2016, 8, 2226–2232. [Google Scholar] [CrossRef]
- Liu, J.; Liang, H.; Cui, F.; Liu, H.; Zhu, C.; Liang, W.; He, J. Spontaneous versus mechanical ventilation during video-assisted thoracoscopic surgery for spontaneous pneumothorax: A randomized trial. J. Thorac. Cardiovasc. Surg. 2022, 163, 1702–1714.e7. [Google Scholar] [CrossRef]
- Dunkman, W.J.; Manning, M.W. Enhanced Recovery After Surgery and Multimodal Strategies for Analgesia. Surg. Clin. N. Am. 2018, 98, 1171–1184. [Google Scholar] [CrossRef]
- Zhang, X.X.; Song, C.T.; Gao, Z.; Zhou, B.; Wang, H.B.; Gong, Q.; Li, B.; Guo, Q.; Li, H.F. A comparison of non-intubated video-assisted thoracic surgery with spontaneous ventilation and intubated video-assisted thoracic surgery: A meta-analysis based on 14 randomized controlled trials. J. Thorac. Dis. 2021, 13, 1624–1640. [Google Scholar] [CrossRef]
- Chiang, X.H.; Lin, M.W. Converting to Intubation During Non-intubated Thoracic Surgery: Incidence, Indication, Technique, and Prevention. Front. Surg. 2021, 8, 769850. [Google Scholar] [CrossRef]
- Moon, Y.; AlGhamdi, Z.M.; Jeon, J.; Hwang, W.; Kim, Y.; Sung, S.W. Non-intubated thoracoscopic surgery: Initial experience at a single center. J. Thorac. Dis. 2018, 10, 3490–3498. [Google Scholar] [CrossRef]
- Anile, M.; Vannucci, J.; Ferrante, F.; Bruno, K.; De Paolo, D.; Bassi, M.; Pugliese, F.; Venuta, F.; NIVATS Interest Group. Non-Intubated Thoracic Surgery: Standpoints and Perspectives. Front. Surg. 2022, 9, 937633. [Google Scholar] [CrossRef]
- Huang, K.; Zhang, Z.; Hu, T.; Qiao, L. Advances in the use of non-intubated spontaneous-ventilation video-assisted thoracoscopic surgery. Front. Surg. 2025, 12, 1584017. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Overall Patients | Matched Patients | ||||||
|---|---|---|---|---|---|---|---|---|
| NIA Group (n = 372) | IA Group (n = 1560) | p Value | NIA Group (n = 336) | IA Group (n = 336) | p Value | SMD | ||
| Time since the earliest included patient (yrs), mean (SD) | 5.03 (2.25) | 4.40 (2.37) | <0.001 | 4.93 (2.30) | 3.32 (2.55) | <0.001 | 0.663 | |
| Calendar period, n (%) | <0.001 | <0.001 | 0.331 | |||||
| 2015–2016 | 49 (13.2) | 311 (20.0) | 49 (14.6) | 130 (38.7) | ||||
| 2017–2018 | 65 (17.5) | 400 (25.6) | 60 (17.9) | 85 (25.3) | ||||
| 2019–2020 | 85 (22.8) | 323 (20.7) | 78 (23.2) | 45 (13.4) | ||||
| 2021–2022 | 173 (46.5) | 526 (33.7) | 149 (44.3) | 76 (22.6) | ||||
| Sex (male), n (%) | 126 (33.9) | 635 (40.7) | 0.015 | 118 (35.1) | 106 (31.5) | 0.326 | 0.076 | |
| Age (yrs old), mean (SD) | 57.92 (11.05) | 60.72 (10.81) | <0.001 | 58.25 (11.14) | 58.25 (12.04) | 0.997 | 0.000 | |
| BMI (kg/m2), mean (SD) | 22.62 (2.99) | 24.04 (3.96) | <0.001 | 22.77 (3.02) | 22.44 (3.03) | 0.156 | 0.109 | |
| Cigarette smoking, n (%) | 58 (15.6) | 374 (24.0) | <0.001 | 58 (17.3) | 52 (15.5) | 0.532 | 0.049 | |
| Alcohol consumption, n (%) | 12 (3.2) | 75 (4.8) | 0.186 | 11 (3.3) | 10 (3.0) | 0.825 | 0.017 | |
| Charlson comorbidity index, mean (SD) | 3.87 (1.34) | 4.28 (1.49) | <0.001 | 3.92 (1.35) | 3.98 (1.39) | 0.593 | 0.044 | |
| FEV1 (% predicted), mean (SD) | 92.05 (16.92) | 90.39 (17.96) | 0.105 | 91.66 (17.16) | 90.67 (18.04) | 0.463 | 0.056 | |
| DLCO (% predicted), mean (SD) | 95.67 (17.71) | 96.02 (18.20) | 0.739 | 94.92 (17.26) | 95.95 (19.18) | 0.463 | 0.056 | |
| ASA class, n (%) | <0.001 | 0.472 | 0.047 | |||||
| I | 15 (4.0) | 37 (2.4) | 12 (3.6) | 16 (4.8) | ||||
| II | 289 (77.7) | 1089 (69.8) | 261 (77.6) | 248 (73.8) | ||||
| III | 68 (18.3) | 434 (27.8) | 63 (18.8) | 72 (21.4) | ||||
| Functional status (≥4 METs), n (%) | 301 (80.9) | 1106 (70.9) | <0.001 | 270 (80.4) | 262 (78.0) | 0.447 | 0.059 | |
| Mallampati score, n (%) | 0.001 | 0.228 | 0.066 | |||||
| I | 4 (1.1) | 5 (0.3) | 3 (0.9) | 3 (0.9) | ||||
| II | 356 (95.7) | 1427 (91.5) | 321 (95.5) | 328 (97.6) | ||||
| III | 12 (3.2) | 128 (8.2) | 12 (3.6) | 5 (1.5) | ||||
| Histological subtype, n (%) | 0.326 | 0.590 | 0.040 | |||||
| Adenocarcinoma | 270 (72.6) | 1182 (75.8) | 242 (72.0) | 238 (70.8) | ||||
| SCC | 101 (27.1) | 370 (23.7) | 93 (27.7) | 95 (28.3) | ||||
| Large cell carcinoma | 1 (0.3) | 8 (0.5) | 1 (0.3) | 3 (0.9) | ||||
| Lesion site, n (%) | 0.950 | 0.810 | 0.049 | |||||
| RUL | 112 (30.1) | 495 (31.7) | 100 (29.8) | 107 (31.9) | ||||
| RML | 32 (8.6) | 132 (8.5) | 29 (8.6) | 32 (9.5) | ||||
| RLL | 80 (21.5) | 321 (20.6) | 73 (21.7) | 74 (22.0) | ||||
| LUL | 86 (23.1) | 353 (22.6) | 79 (23.5) | 66 (19.6) | ||||
| LLL | 62 (16.7) | 256 (16.4) | 55 (16.4) | 57 (17.0) | ||||
| Lingula | 0 (0.0) | 3 (0.2) | 0 (0.0) | 0 (0.0) | ||||
| TNM stage, n (%) | <0.001 | 0.177 | 0.072 | |||||
| 0 (CIS) | 45 (12.1) | 64 (4.1) | 39 (11.6) | 25 (7.4) | ||||
| I | 239 (64.2) | 1075 (68.9) | 210 (62.5) | 223 (66.4) | ||||
| II | 88 (23.7) | 421 (27.0) | 87 (25.9) | 88 (26.2) | ||||
| Differentiation grade, n (%) | 0.005 | 0.851 | 0.022 | |||||
| I | 94 (25.3) | 282 (18.1) | 84 (25.0) | 83 (24.7) | ||||
| II | 201 (54.0) | 891 (57.1) | 182 (54.2) | 177 (52.7) | ||||
| III | 77 (20.7) | 387 (24.8) | 70 (20.8) | 76 (22.6) | ||||
| Surgeon experience (yrs), n (%) | <0.001 | <0.001 | 0.234 | |||||
| <10 | 13 (3.5) | 241 (15.4) | 13 (3.9) | 34 (10.1) | ||||
| 10–20 | 345 (92.7) | 1185 (76.0) | 311 (92.5) | 254 (75.6) | ||||
| >20 | 14 (3.8) | 134 (8.6) | 12 (3.6) | 48 (14.3) | ||||
| Procedural type, n (%) | <0.001 | 0.507 | 0.045 | |||||
| Wedge resection | 339 (91.1) | 768 (49.2) | 303 (90.2) | 308 (91.7) | ||||
| Segmentectomy | 21 (5.7) | 334 (21.4) | 21 (6.2) | 21 (6.2) | ||||
| Lobectomy | 12 (3.2) | 458 (29.4) | 12 (3.6) | 7 (2.1) | ||||
| Anesthesiologist experience (yrs), n (%) | 0.568 | 0.647 | 0.036 | |||||
| <10 | 46 (12.4) | 226 (14.5) | 42 (12.5) | 43 (12.8) | ||||
| 10–20 | 276 (74.2) | 1133 (72.6) | 252 (75.0) | 243 (72.3) | ||||
| >20 | 50 (13.4) | 201 (12.9) | 42 (12.5) | 50 (14.9) | ||||
| Anesthesia technique, n (%) | <0.001 | <0.001 | 0.160 | |||||
| TIVA | 55 (14.8) | 626 (40.1) | 54 (16.1) | 61 (18.2) | ||||
| INHA | 50 (13.4) | 39 (2.5) | 49 (14.6) | 17 (5.0) | ||||
| Mixed anesthesia | 267 (71.8) | 895 (57.4) | 233 (69.3) | 258 (76.8) | ||||
| Variables | Overall Patients | Matched Patients | ||||||
|---|---|---|---|---|---|---|---|---|
| NIA Group (n = 372) | IA Group (n = 1560) | p Value | NIA Group (n = 336) | IA Group (n = 336) | p Value | SMD | ||
| Intraoperative variables | ||||||||
| Operation time (mins), mean (SD) | 74.46 (24.63) | 103.60 (85.03) | <0.001 | 74.88 (25.04) | 79.58 (62.28) | 0.200 | NA | |
| Anesthesia time (mins), mean (SD) | 102.03 (28.33) | 143.91 (91.74) | <0.001 | 102.38 (28.96) | 116.90 (67.96) | <0.001 | NA | |
| Induction time (mins), mean (SD) | 20.50 (8.66) | 30.05 (13.43) | <0.001 | 20.35 (8.66) | 27.55 (12.50) | <0.001 | NA | |
| Emergence time (mins), mean (SD) | 7.08 (4.85) | 10.25 (6.40) | <0.001 | 7.15 (4.74) | 9.77 (5.46) | <0.001 | NA | |
| Intraoperative fentanyl consumption (mcg), mean (SD) | 108.70 (38.59) | 146.29 (59.97) | <0.001 | 108.66 (39.11) | 130.45 (52.11) | <0.001 | NA | |
| Intraoperative epidural analgesia, n (%) | 1 (0.3) | 25 (1.6) | 0.045 | 1 (0.3) | 6 (1.8) | 0.057 | NA | |
| Intraoperative NSAID administration, n (%) | 86 (23.1) | 309 (19.8) | 0.155 | 73 (21.7) | 66 (19.6) | 0.505 | NA | |
| Intraoperative fluid intake (mL), mean (SD) | 317.50 (192.21) | 656.76 (617.77) | <0.001 | 319.52 (196.31) | 539.02 (411.37) | <0.001 | NA | |
| Intraoperative blood loss (mL), mean (SD) | 26.59 (72.34) | 59.61 (203.22) | <0.001 | 27.29 (76.09) | 40.39 (102.95) | 0.061 | NA | |
| Intraoperative transfusion, n (%) | 3 (0.8) | 41 (2.6) | 0.034 | 3 (0.9) | 8 (2.4) | 0.128 | NA | |
| Intraoperative adverse events, n (%) | ||||||||
| Patient movement | 61 (16.4) | 0 (0.0) | <0.001 | 56 (16.7) | 0 (0.0) | <0.001 | NA | |
| Pulmonary episodes | 17 (4.6) | 42 (2.7) | 0.059 | 16 (4.8) | 10 (3.0) | 0.230 | NA | |
| Cardiovascular episodes | 9 (2.4) | 26 (1.7) | 0.328 | 9 (2.7) | 5 (1.5) | 0.280 | NA | |
| Postoperative variables | ||||||||
| Grade of surgical complications, n (%) | 0.472 | 0.060 | NA | |||||
| 0 | 121 (32.5) | 459 (29.4) | 110 (32.7) | 108 (32.1) | ||||
| I | 247 (66.4) | 1062 (68.1) | 223 (66.4) | 219 (65.2) | ||||
| II | 3 (0.8) | 19 (1.2) | 3 (0.9) | 1 (0.3) | ||||
| III | 0 (0.0) | 1 (0.1) | 0 (0.0) | 0 (0.0) | ||||
| IV | 1 (0.3) | 12 (0.8) | 0 (0.0) | 4 (1.2) | ||||
| V | 0 (0.0) | 7 (0.4) | 0 (0.0) | 4 (1.2) | ||||
| Postoperative fentanyl consumption (mcg), mean (SD) | 337.79 (274.63) | 425.31 (309.74) | <0.001 | 336.68 (275.55) | 387.51 (276.08) | 0.017 | NA | |
| Postoperative adverse events, n (%) | ||||||||
| POST | 12 (3.2) | 66 (4.2) | 0.376 | 11 (3.3) | 18 (5.4) | 0.184 | NA | |
| PONV | 4 (1.1) | 30 (1.9) | 0.264 | 3 (0.9) | 7 (2.1) | 0.203 | NA | |
| Pulmonary episodes | 6 (1.6) | 81 (5.2) | 0.003 | 5 (1.5) | 16 (4.8) | 0.015 | NA | |
| Cardiovascular episodes | 2 (0.5) | 31 (2.0) | 0.053 | 1 (0.3) | 10 (3.0) | 0.006 | NA | |
| Postoperative mechanical ventilation, n (%) | 2 (0.5) | 88 (5.6) | <0.001 | 1 (0.3) | 13 (3.9) | 0.001 | NA | |
| Postoperative ICU admission, n (%) | 4 (1.1) | 90 (5.8) | <0.001 | 3 (0.9) | 13 (3.9) | 0.011 | NA | |
| Length of postoperative hospital stay (days), mean (SD) | 4.13 (2.61) | 5.90 (8.77) | <0.001 | 4.10 (2.65) | 5.68 (10.88) | 0.010 | NA | |
| Length of total hospital stay (days), mean (SD) | 7.06 (3.89) | 10.04 (10.33) | <0.001 | 7.02 (3.82) | 9.30 (11.48) | 0.001 | NA | |
| Patient satisfaction, n (%) | 0.002 | 0.005 | NA | |||||
| Very satisfactory | 256 (68.8) | 946 (60.6) | 230 (68.5) | 209 (62.2) | ||||
| Satisfactory | 116 (31.2) | 591 (37.9) | 106 (31.5) | 118 (35.1) | ||||
| Neutral | 0 (0.0) | 23 (1.5) | 0 (0.0) | 9 (2.7) | ||||
| Surgeon satisfaction, n (%) | 0.103 | 0.404 | NA | |||||
| Very satisfactory | 268 (72.0) | 1072 (68.7) | 243 (72.3) | 241 (71.7) | ||||
| Satisfactory | 102 (27.4) | 457 (29.3) | 92 (27.4) | 91 (27.1) | ||||
| Neutral | 2 (0.5) | 31 (2.0) | 1 (0.3) | 4 (1.2) | ||||
| Surgery cost (USD), mean (SD) | 1929.42 (579.95) | 2383.70 (842.89) | <0.001 | 1938.56 (584.7) | 2003.61 (715.51) | 0.197 | NA | |
| Anesthesia cost (USD), mean (SD) | 244.21 (95.51) | 320.83 (167.60) | <0.001 | 245.98 (98.81) | 283.21 (126.17) | <0.001 | NA | |
| Total cost (USD), mean (SD) | 7107.48 (2386.64) | 9929.54 (8212.35) | <0.001 | 7097.54 (2401.09) | 8957.03 (9401.49) | <0.001 | NA | |
| Stratified Variable | Ventilation Strategy | Crude OR (95% CI) | p Value | p Value (Interaction) | PS-Matched OR (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Calendar | 0.102 | |||||
| period | ||||||
| 2015–2018 | IA | 1.00 | 1.00 | |||
| NIA | 1.17 | 0.637 | 1.21 | 0.627 | ||
| (0.61–2.24) | (0.57–2.57) | |||||
| 2019–2022 | IA | 1.00 | 1.00 | |||
| NIA | 0.56 | 0.052 | 0.67 | 0.367 | ||
| (0.31–1.01) | (0.29–1.59) | |||||
| Surgeon | 0.123 | |||||
| experience | ||||||
| <10 years | IA | cannot converge | cannot converge | |||
| NIA | ||||||
| ≥10 years | IA | 1.00 | 1.00 | |||
| NIA | 0.80 | 0.328 | 0.79 | 0.408 | ||
| (0.52–1.25) | (0.45–1.38) | |||||
| Procedural | 0.536 | |||||
| type | ||||||
| Wedge resection | IA | 1.00 | 1.00 | |||
| NIA | 0.68 | 0.124 | 0.81 | 0.494 | ||
| (0.42–1.11) | (0.45–1.47) | |||||
| Other procedures | IA | 1.00 | 1.00 | |||
| NIA | 1.03 | 0.960 | 0.83 | 0.832 | ||
| (0.31–3.47) | (0.15–4.50) | |||||
| Anesthesia | 0.463 | |||||
| technique | ||||||
| TIVA | IA | 1.00 | 1.00 | |||
| NIA | 0.37 | 0.175 | 0.35 | 0.214 | ||
| (0.09–1.56) | (0.07–1.83) | |||||
| INHA | IA | 1.00 | 1.00 | |||
| NIA | 1.19 | 0.796 | 2.23 | 0.473 | ||
| (0.31–4.56) | (0.25–20.0) | |||||
| Mixed anesthesia | IA | 1.00 | 1.00 | |||
| NIA | 0.72 | 0.218 | 0.80 | 0.513 | ||
| (0.42–1.22) | (0.42–1.55) |
| Variables | Univariable | Multivariable | |||
|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | ||
| Time since the earliest included patient (yrs) | 0.85 (0.70–1.03) | 0.091 | |||
| Sex, female (ref: male) | 2.03 (0.82–5.03) | 0.124 | |||
| Age (yrs old) | 1.02 (0.98–1.07) | 0.354 | |||
| BMI (kg/m2) | 1.10 (0.96–1.26) | 0.168 | |||
| Cigarette smoking (ref: no) | 1.88 (0.66–5.39) | 0.240 | |||
| Alcohol consumption (ref: no) | 1.63 (0.20–13.3) | 0.648 | |||
| Charlson comorbidity index | 1.21 (0.87–1.67) | 0.259 | |||
| FEV1 (% predicted) | 1.00 (0.98–1.03) | 0.755 | |||
| DLCO (% predicted) | 1.02 (1.00–1.05) | 0.061 | |||
| ASA class (ref: I) | |||||
| II | 0.55 (0.07–4.60) | 0.584 | |||
| III | 1.87 (0.22–16.2) | 0.571 | |||
| Mallampati score, III (ref: I + II) | 3.80 (0.77–18.6) | 0.100 | |||
| Histological subtype, SCC (ref: adenocarcinoma) | 1.15 (0.43–3.09) | 0.774 | |||
| Lesion site (ref: RUL) | |||||
| RML | 2.41 (0.73–7.95) | 0.150 | |||
| RLL | 0.16 (0.02–1.34) | 0.092 | |||
| LUL | 0.63 (0.18–2.18) | 0.470 | |||
| LLL | 0.43 (0.09–2.11) | 0.300 | |||
| TNM stage (ref: CIS) | |||||
| I | 0.68 (0.18–2.52) | 0.560 | |||
| II | 1.02 (0.24–4.30) | 0.974 | |||
| Differentiation grade (ref: I) | |||||
| II | 0.33 (0.11–0.98) | 0.046 | 0.37 (0.09–1.45) | 0.153 | |
| III | 0.91 (0.30–2.74) | 0.865 | 1.05 (0.25–4.51) | 0.945 | |
| Surgeon experience, ≥10 (ref: <10 yrs) | 0.67 (0.08–5.43) | 0.708 | |||
| Procedural type (ref: wedge resection) | |||||
| Segmentectomy | 0.95 (0.12–7.48) | 0.959 | |||
| Lobectomy | 3.79 (0.77–18.7) | 0.102 | |||
| Anesthesiologist experience, ≥10 (ref: <10 yrs) | 1.29 (0.29–5.73) | 0.742 | |||
| Anesthesia technique (ref: TIVA) | |||||
| INHA | 0.35 (0.04–3.52) | 0.375 | |||
| Mixed anesthesia | 1.10 (0.31–3.93) | 0.878 | |||
| Baseline MBP (mmHg) | 1.01 (0.98–1.04) | 0.498 | |||
| Baseline HR (beat/min) | 1.00 (0.97–1.04) | 0.817 | |||
| Baseline SpO2 (%) | 0.87 (0.78–0.97) | 0.011 | 0.89 (0.80–1.00) | 0.042 | |
| Induction time (mins) | 0.94 (0.88–1.01) | 0.087 | |||
| Intraoperative NSAID administration (ref: no) | 0.35 (0.08–1.56) | 0.170 | |||
| Intraoperative patient movement (ref: no) | 0.55 (0.12–2.44) | 0.433 | |||
| Intraoperative pulmonary episode (ref: no) | 35.2 (11.4–108) | <0.001 | 43.0 (11.6–160) | <0.001 | |
| Intraoperative cardiovascular episode (ref: no) | 29.0 (7.06–119) | <0.001 | 50.0 (9.62–259) | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, H.-H.; Chen, L.-H.; Lai, H.-C.; Wu, Z.-F.; Ko, C.-L.; Lo, K.-L.; Huang, G.-S.; Tseng, W.-C. Perioperative Outcomes of Non-Intubated Versus Intubated Anesthesia in Video-Assisted Thoracoscopic Surgery for Early-Stage Non-Small Cell Lung Cancer: A Propensity Score-Matched Analysis. J. Clin. Med. 2025, 14, 3466. https://doi.org/10.3390/jcm14103466
Huang H-H, Chen L-H, Lai H-C, Wu Z-F, Ko C-L, Lo K-L, Huang G-S, Tseng W-C. Perioperative Outcomes of Non-Intubated Versus Intubated Anesthesia in Video-Assisted Thoracoscopic Surgery for Early-Stage Non-Small Cell Lung Cancer: A Propensity Score-Matched Analysis. Journal of Clinical Medicine. 2025; 14(10):3466. https://doi.org/10.3390/jcm14103466
Chicago/Turabian StyleHuang, Hsiang-Han, Li-Hua Chen, Hou-Chuan Lai, Zhi-Fu Wu, Ching-Lung Ko, Kai-Li Lo, Go-Shine Huang, and Wei-Cheng Tseng. 2025. "Perioperative Outcomes of Non-Intubated Versus Intubated Anesthesia in Video-Assisted Thoracoscopic Surgery for Early-Stage Non-Small Cell Lung Cancer: A Propensity Score-Matched Analysis" Journal of Clinical Medicine 14, no. 10: 3466. https://doi.org/10.3390/jcm14103466
APA StyleHuang, H.-H., Chen, L.-H., Lai, H.-C., Wu, Z.-F., Ko, C.-L., Lo, K.-L., Huang, G.-S., & Tseng, W.-C. (2025). Perioperative Outcomes of Non-Intubated Versus Intubated Anesthesia in Video-Assisted Thoracoscopic Surgery for Early-Stage Non-Small Cell Lung Cancer: A Propensity Score-Matched Analysis. Journal of Clinical Medicine, 14(10), 3466. https://doi.org/10.3390/jcm14103466