


Telehealth in Informal Caregivers of Stroke Survivors: A Systematic Review

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Eligibility Criteria
2.3. Search Strategy
- -
- Pubmed, article type: “clinical trial”, “controlled clinical trial”, “randomized clinical trial”; language: “English”, “Spanish”.
- -
- Web of Science: “English”, “Spanish”, “clinical trial”.
- -
- Scopus: “English”, “Spanish”, “article”.
- -
- CINALH, Psychology and Behavioral Sciences Collection and APA PsycInfo: “English”.
2.4. Selection Process and Data Collection
2.5. Data Extraction
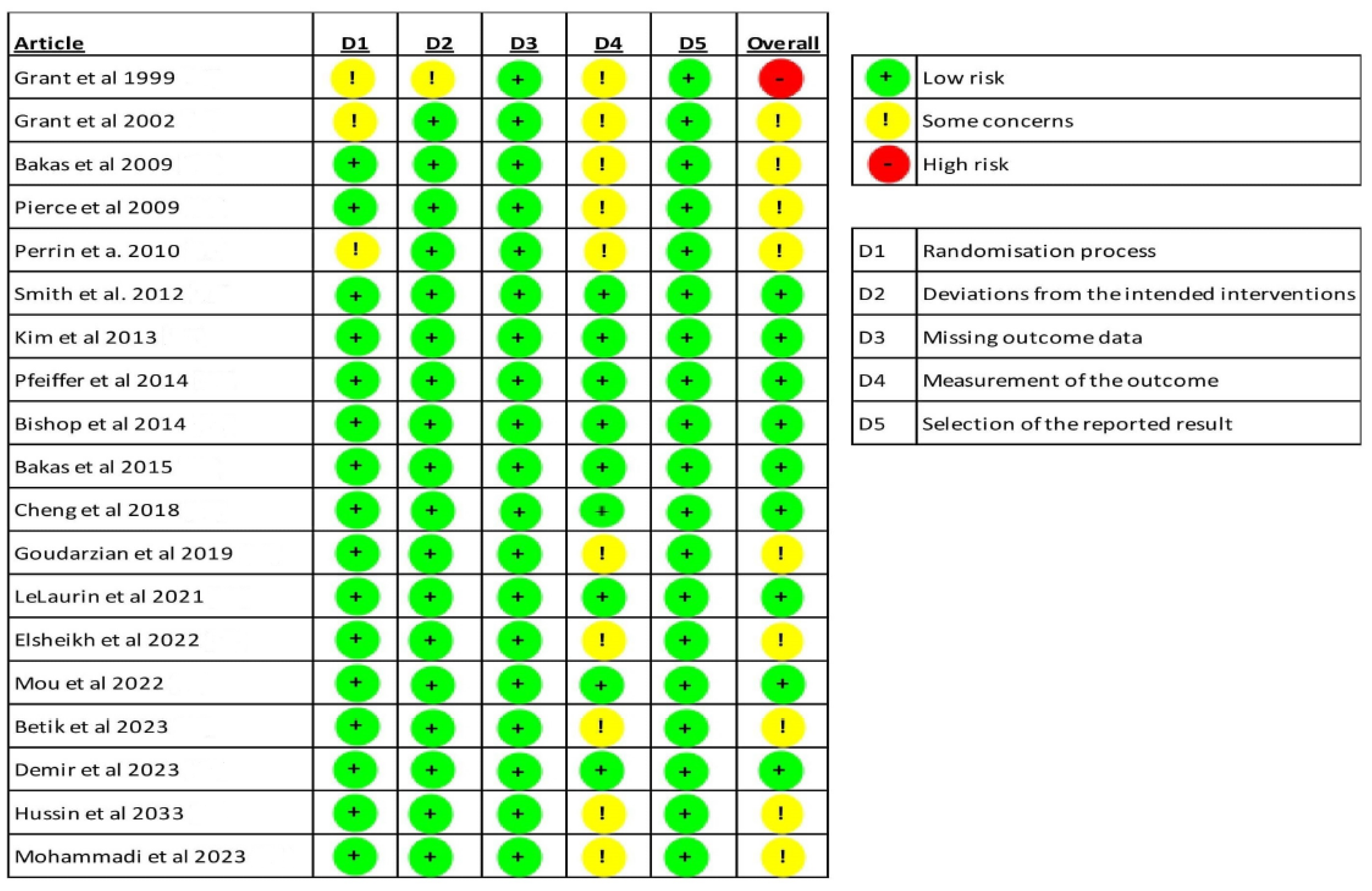
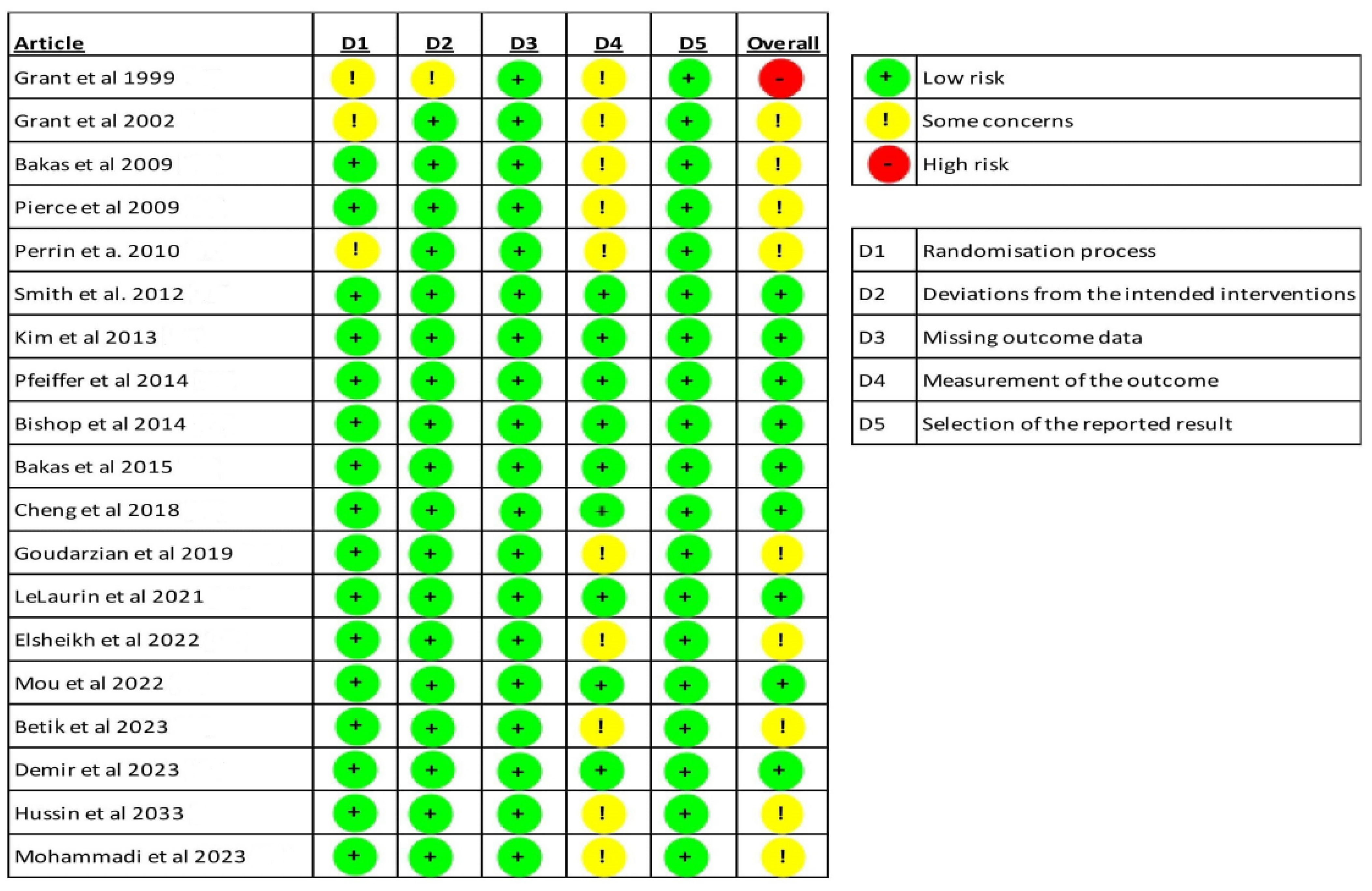
2.6. Risk of Bias
- (1)
- Bias arising from the randomisation process.
- (2)
- Bias due to deviations from the intended interventions.
- (3)
- Bias due to missing outcome data.
- (4)
- Bias in the outcome measurement of the outcome.
- (5)
- Bias in the selection of the reported outcome.
2.7. Quality Assessment
2.8. Data Synthesis
3. Results
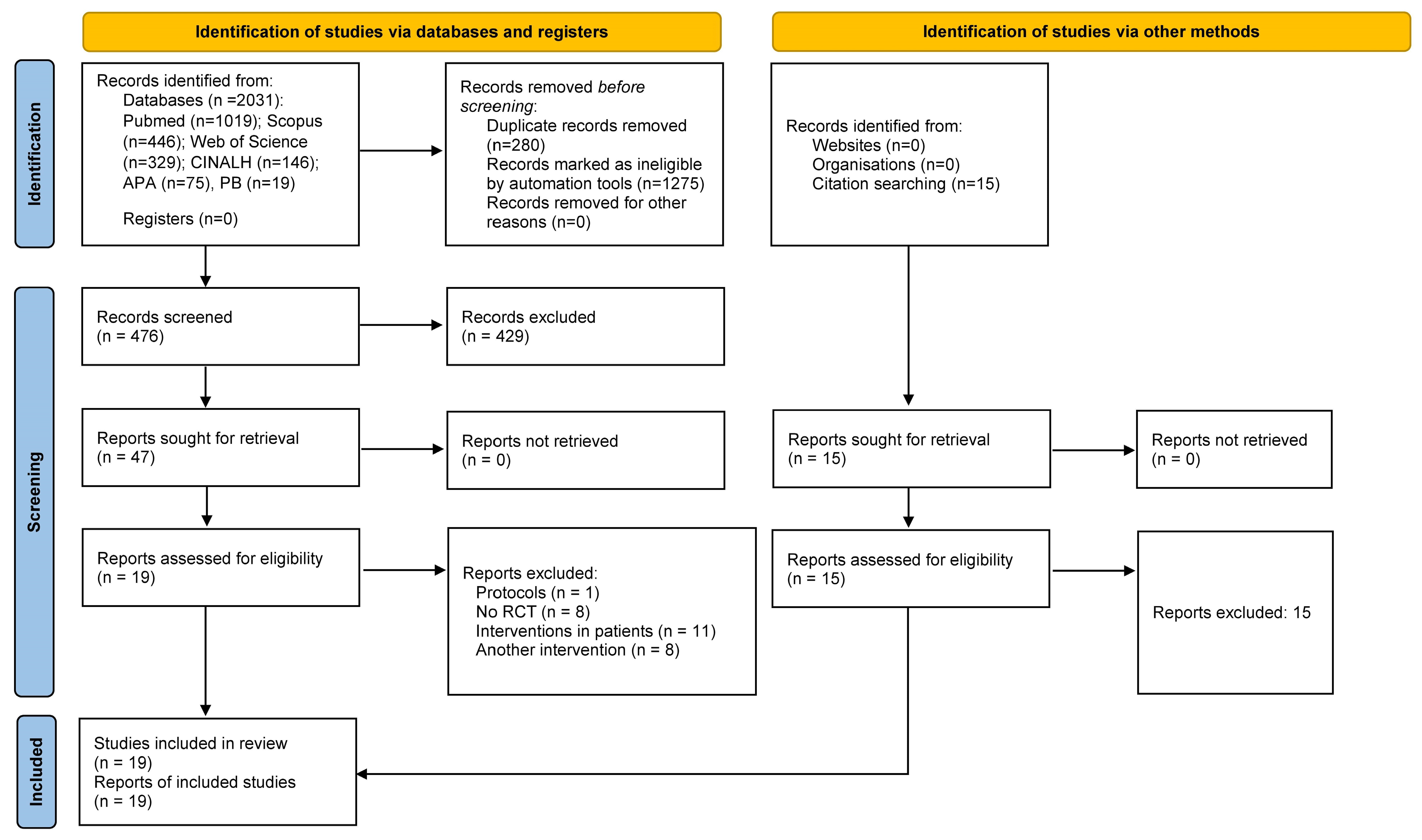
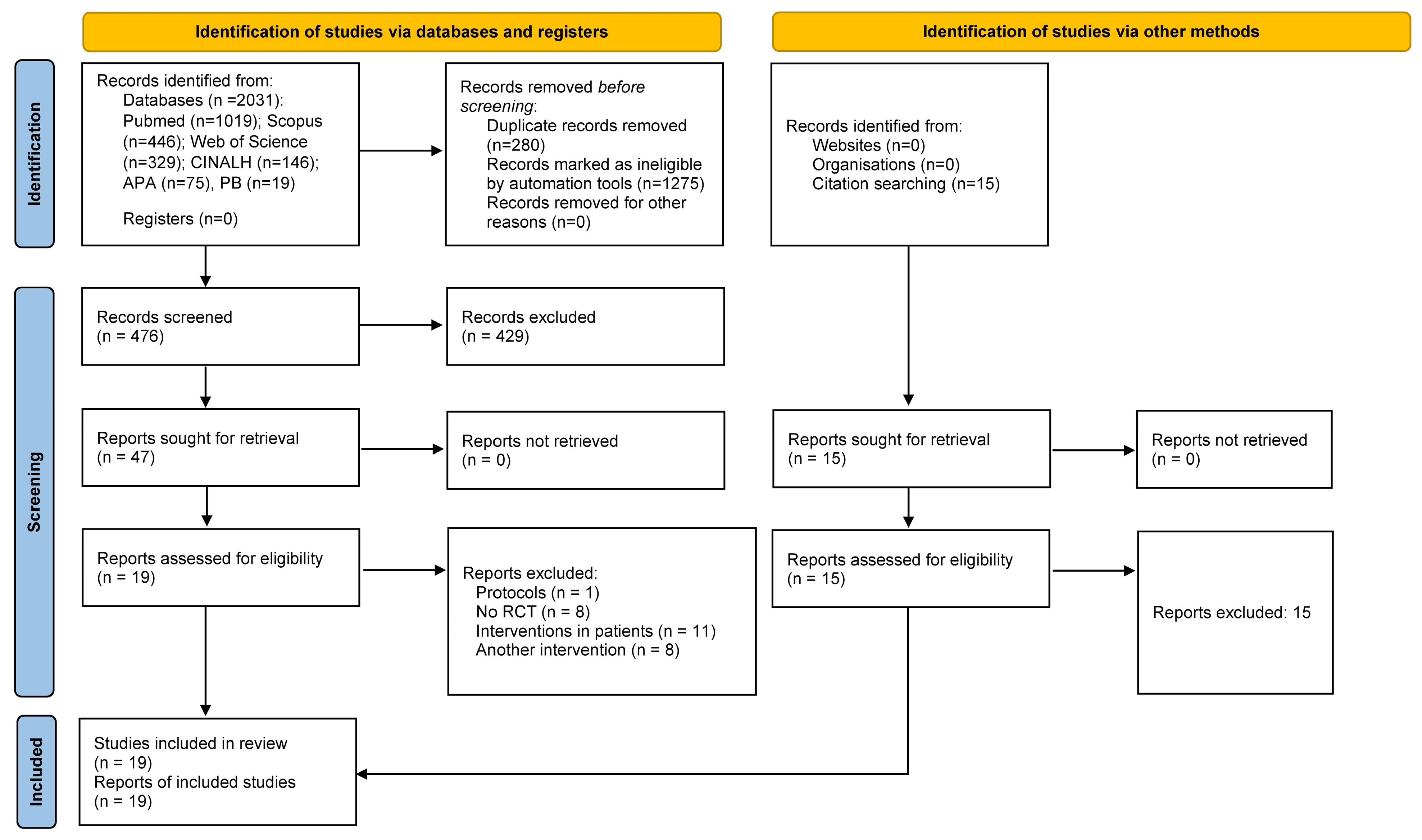
3.1. Study Selection
3.2. Sample Size and Participant Characteristics (Age and Number of Women per Study) of the Articles Reviewed
3.3. Interventions
3.4. Outcomes
3.5. Results
3.6. Risk of Bias
3.7. Quality Assessment
4. Discussion
4.1. Population
4.2. Interventions
4.3. Outcomes
4.4. Results
4.5. Risk of Bias
4.6. Quality Assessment
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
| Paper | Randomisation Present | Appropriated Randomisation Utilised | Blinded Present | Appropriated Blinded Utilised | Description of Withdrawals and Dropouts | Total |
|---|---|---|---|---|---|---|
| Grant et al., 1999 [43] | 0 | 0 | 0 | 0 | 0 | 0 |
| Grant et al., 2002 [44] | 1 | 0 | 0 | 0 | 1 | 2 |
| Bakas et al., 2009 [45] | 1 | 1 | 0 | 0 | 1 | 3 |
| Pierce et al., 2009 [46] | 1 | 1 | 0 | 0 | 1 | 3 |
| Perrin et al., 2010 [47] | 1 | 1 | 0 | 0 | 1 | 3 |
| Smith et al., 2012 [48] | 1 | 1 | 0 | 0 | 1 | 3 |
| Kim et al., 2013 [49] | 1 | 1 | 0 | 0 | 1 | 3 |
| Pfeiffer et al., 2014 [50] | 1 | 1 | 0 | 0 | 1 | 3 |
| Bishop et al., 2014 [51] | 1 | 1 | 0 | 0 | 1 | 3 |
| Bakas et al., 2015 [52] | 1 | 1 | 0 | 0 | 1 | 3 |
| Cheng et al., 2015 [53] | 1 | 1 | 0 | 0 | 1 | 3 |
| Goudarzian et al., 2019 [54] | 1 | 1 | 0 | 0 | 0 | 2 |
| LeLaurin et al., 2021 [55] | 1 | 1 | 0 | 0 | 1 | 3 |
| Elsheikh et al., 2022 [56] | 1 | 1 | 0 | 0 | 1 | 3 |
| Mou et al., 2022 [57] | 1 | 1 | 0 | 0 | 1 | 3 |
| Betik et al., 2023 [58] | 1 | 1 | 0 | 0 | 1 | 3 |
| Demir et al., 2023 [59] | 1 | 1 | 0 | 0 | 1 | 3 |
| Hussin et al., 2023 [60] | ||||||
| Mohammadi et al., 2023 [61] | 1 | 1 | 0 | 0 | 1 | 3 |
References
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Maresova, P.; Javanmardi, E.; Barakovic, S.; Barakovic Husic, J.; Tomsone, S.; Krejcar, O.; Kuca, K. Consequences of chronic diseases and other limitations associated with old age—A scoping review. BMC Public Health 2019, 19, 1431. [Google Scholar] [CrossRef]
- Pache, B.; Vollenweider, P.; Waeber, G.; Marques-Vidal, P. Prevalence of measured and reported multimorbidity in a representative sample of the Swiss population. BMC Public Health 2014, 15, 65. [Google Scholar]
- Chi, N.C.; Demiris, G. A systematic review of telehealth tools and interventions to support family caregivers. J. Telemed. Telecare 2015, 21, 37–44. [Google Scholar] [CrossRef]
- Kent, E.E.; Rowland, J.H.; Northouse, L.; Litzelman, K.; Chou, W.Y.; Shelburne, N.; Timura, C.; O’Mara, A.; Huss, K. Caring for caregivers and patients: Research and clinical priorities for informal cancer caregiving. Cancer 2016, 122, 1987–1995. [Google Scholar] [CrossRef]
- Zapata-Sampedro, M.A.; Matute-Caballero, M.N.; Gómez-Reina, M.V. Plan de cuidados enfermeros al cuidador informal: Caso clínico. Enferm. Clin. 2007, 17, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Pristavec, T.; Luth, E.A. Informal Caregiver Burden, Benefits, and Older Adult Mortality: A Survival Analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 2193–2206. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Chiu, J.; Bursnall, S.; Cannon, T. Relations between social support, appraisal and coping and both positive and negative outcomes in young carers. J. Health Psychol. 2007, 12, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Winter, K.H.; Bouldin, E.D.; Andresen, E.M. Lack of choice in caregiving decision and caregiver risk of stress, North Carolina, 2005. Prev. Chronic Dis. 2010, 7, A41. [Google Scholar]
- Ornstein, K.; Gaugler, J.E. The problem with “problem behaviors”: A systematic review of the association between individual patient behavioral and psychological symptoms and caregiver depression and burden within the dementia patient-caregiver dyad. Int. Psychogeriatr. 2012, 24, 1536–1552. [Google Scholar] [CrossRef]
- Christian, L.M.; Wilson, S.J.; Madison, A.A.; Prakash, R.S.; Burd, C.E.; Rosko, A.E.; Kiecolt-Glaser, J.K. Understanding the health effects of caregiving stress: New directions in molecular aging. Ageing Res. Rev. 2023, 92, 102096. [Google Scholar] [CrossRef]
- Graven, L.J.; Boel-Studt, S.; Buck, H.G.; Abbott, L.; Grant, J.S. Heart Failure Caregiver Self-Care: A Latent Class Analysis. Clin. Nurs. Res. 2021, 30, 625–635. [Google Scholar] [CrossRef]
- Riffin, C.; Van Ness, P.H.; Wolff, J.L.; Fried, T. Multifactorial Examination of Caregiver Burden in a National Sample of Family and Unpaid Caregivers. J. Am. Geriatr. Soc. 2019, 67, 277–283. [Google Scholar] [CrossRef]
- Cheng, S.T. Dementia Caregiver Burden: A Research Update and Critical Analysis. Curr. Psychiatry Rep. 2017, 19, 64. [Google Scholar] [CrossRef] [PubMed]
- Joling, K.J.; van Marwijk, H.W.; Veldhuijzen, A.E.; van der Horst, H.E.; Scheltens, P.; Smit, F.; van Hout, H.P. The two-year incidence of depression and anxiety disorders in spousal caregivers of persons with dementia: Who is at the greatest risk? Am. J. Geriatr. Psychiatry 2015, 23, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Regenhardt, R.W.; Das, A.S.; Lo, E.H.; Caplan, L.R. Advances in Understanding the Pathophysiology of Lacunar Stroke: A Review. JAMA Neurol. 2018, 75, 273–1281. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the global burden of disease study 2010. Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Mackay, J.; Mensah, G. The Atlas of Heart Disease and Stroke; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for adult stroke rehabilitation and recovery. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Larson, J.; Franzén-Dahlin, A.; Billing, E.; Arbin, M.; Murray, V.; Wredling, R. The impact of a nurse-led support and education programme for spouses of stroke patients: A randomized controlled trial. J. Clin. Nurs. 2005, 14, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, H.; Atkinson, C.; Bond, S.; Suddes, M.; Dobson, R.; Curless, R. Randomized controlled trial of a comprehensive stroke education program for patients and caregivers. Stroke 1999, 30, 2585–2591. [Google Scholar] [CrossRef] [PubMed]
- Hickenbottom, S.L.; Fendraick, J.M.; Kutcher, J.S.; Kabeto, M.U.; Katz, S.J.; Langa, K.M. A national study of the quantity and cost of informal caregiving for the elderly with a stroke. Neurology 2002, 58, 1754–1759. [Google Scholar] [CrossRef]
- Visser-Meily, A.; Post, M.; van de Port, I.; Maas, C.; Forstberg-Warleby, G.; Lindeman, E. Psychosocial functioning of spouses with patients with stroke from initial rehabilitation to 3 years post-stroke: Course and relations with coping strategies. Stroke 2009, 40, 1399–1404. [Google Scholar] [CrossRef]
- Boonsin, S.; Deenan, A.; Wacharasin, C. Factors Influencing the Burden of Family Caregiving for Survivors of Stroke. Pac. Rim Int. J. Nurs. Res. 2021, 25, 102–113. [Google Scholar]
- Pindus, D.M.; Mullis, R.; Lim, L.; Wellwood, I.; Rundell, A.V.; Azah Abd Aziz, N.; Mant, J. Stroke Survivors’ and Informal Caregivers’ Experiences of Primary Care and Community Healthcare Services—A Systematic Review and Meta-Ethnography. PLoS ONE 2018, 13, e0192533. [Google Scholar]
- Martinsen, R.; Kirkevold, M.; Sveen, U. Young and midlife stroke survivors’ experiences with the health services and long-term follow-up needs. J. Neurosci. Nurs. 2015, 47, 27–35. [Google Scholar] [CrossRef]
- Bashshur, R.L.; Shannon, G.; Krupinski, E.A.; Grigsby, J. Sustaining and realizing the promise of telemedicine. Telemed. e-Health 2013, 19, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Aldehaim, A.Y.; Alotaibi, F.F.; Uphold, C.R.; Dang, S. The impact of technology-based interventions on informal caregivers of stroke survivors: A systematic review. Telemed. J. e-Health 2016, 22, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Glueckauf, R.L.; Davis, W.S.; Willis, F.; Sharma, D.; Gustafson, D.J.; Hayes, J.; Stutzman, M.; Proctor, J.; Kazmer, M.M.; Murray, L.; et al. Telephone-based, cognitive-behavioral therapy for African American dementia caregivers with depression: Initial findings. Rehabil. Psychol. 2012, 57, 124–139. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Alcalá, C.I.; Pliego-Pastrana, P.; Rosales-Lagarde, A.; Lopez-Noguerola, J.S.; Molina-Trinidad, E.M. Information and Communication Technologies in the Care of the Elderly: Systematic Review of Applications Aimed at Patients With Dementia and Caregivers. JMIR Rehabil. Assist. Technol. 2016, 3, e6. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Jin, W.; Zhang, X.X.; Xu, W.; Liu, X.N.; Ren, C.C. Telerehabilitation Approaches for Stroke Patients: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Stroke Cerebrovasc. Dis. 2015, 24, 2660–2668. [Google Scholar] [CrossRef] [PubMed]
- Tchero, H.; Tabue Teguo, M.; Lannuzel, A.; Rusch, E. Telerehabilitation for Stroke Survivors: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2018, 20, e10867. [Google Scholar] [CrossRef] [PubMed]
- Johansson, T.; Wild, C. Telerehabilitation in stroke care—A systematic review. J. Telemed. Telecare 2011, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.-J.; Song, Y.-Y.; Wang, C.; Jiang, Y.; Cui, W.-Y.; Liu, W.-J.; Liu, Y. Telerehabilitation for Family Caregivers of Stroke Survivors: A Systematic Review and Meta-Analysis. J. Nurs. Manag. 2023, 2023, 3450312. [Google Scholar] [CrossRef]
- Denham AM, J.; Wynne, O.; Baker, A.L.; Spratt, N.J.; Bonevski, B. The unmet needs of carers of stroke survivors: An evaluation of Google search results. Health Inform. J. 2020, 26, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Firmawati, E.; Setyopanoto, I.; Pangastuti, H.S. Mobile Health Application to Support Family Recurrent Stroke Prevention: Scoping Review. Open Access Maced. J. Med. Sci. 2021, 9, 142–151. [Google Scholar] [CrossRef]
- Lobo, E.H.; Frølich, A.; Kensing, F.; Rasmussen, L.J.; Livingston, P.M.; Grundy, J.; Abdelrazek, M. mHealth applications to support caregiver needs and engagement during stroke recovery: A content review. Res. Nurs. Health 2021, 44, 213–225. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D. Evaluations of the uptake and impact of the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and extensions: A scoping review. Syst. Rev. 2017, 6, 263. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef]
- Oremus, M.; Wolfson, C.; Perrault, A.; Demers, L.; Momoli, F.; Moride, Y. Interrater reliability of the modified Jadad quality scale for systematic reviews of Alzheimer’s disease drug trials. Dement. Geriatr. Cogn. Disord. 2001, 12, 232–236. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Clark, H.; Wells, G.A.; Huët, C.; McAlister, F.A.; Salmi, L.R.; Fergusson, D.; Laupacis, A. Assessing the quality of randomized trials: Reliability of the Jadad scale. Control. Clin. Trials 1999, 20, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.S. Social problem-solving partnerships with family caregivers. Rehabil. Nurs. 1999, 24, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.S.; Elliott, T.R.; Weaver, M.; Bartolucci, A.A.; Giger, J.N. Telephone intervention with family caregivers of stroke survivors after rehabilitation. Stroke 2002, 33, 2060–2065. [Google Scholar] [CrossRef]
- Bakas, T.; Farran, C.J.; Austin, J.K.; Given, B.A.; Johnson, E.A.; Williams, L.S. Stroke caregiver outcomes from the Telephone Assessment and Skill-Building Kit (TASK). Top. Stroke Rehabil. 2009, 16, 105–121. [Google Scholar] [CrossRef]
- Pierce, L.L.; Steiner, V.L.; Khuder, S.A.; Govoni, A.L.; Horn, L.J. The effect of a Web-based stroke intervention on carers’ well-being and survivors’ use of healthcare services. Disabil. Rehabil. 2009, 31, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Perrin, P.B.; Johnston, A.; Vogel, B.; Heesacker, M.; Vega-Trujillo, M.; Anderson, J.; Rittman, M. A culturally sensitive Transition Assistance Program for stroke caregivers: Examining caregiver mental health and stroke rehabilitation. J. Rehabil. Res. Dev. 2010, 47, 605–617. [Google Scholar] [CrossRef]
- Smith, G.C.; Egbert, N.; Dellman-Jenkins, M.; Nanna, K.; Palmieri, P.A. Reducing depression in stroke survivors and their informal caregivers: A randomized clinical trial of a Web-based intervention. Rehabil. Psychol. 2012, 57, 196–206. [Google Scholar] [CrossRef]
- Kim, J.I.; Lee, S.; Kim, J.H. Effects of a web-based stroke education program on recurrence prevention behaviors among stroke patients: A pilot study. Health Educ. Res. 2013, 28, 488–501. [Google Scholar] [CrossRef]
- Pfeiffer, K.; Beische, D.; Hautzinger, M.; Berry, J.W.; Wengert, J.; Hoffrichter, R.; Becker, C.; van Schayck, R.; Elliott, T.R. Telephone-based problem-solving intervention for family caregivers of stroke survivors: A randomized controlled trial. J. Consult. Clin. Psychol. 2014, 82, 628–643. [Google Scholar] [CrossRef]
- Bishop, D.; Miller, I.; Weiner, D.; Guilmette, T.; Mukand, J.; Feldmann, E.; Keitner, G.; Springate, B. Family Intervention: Telephone Tracking (FITT): A pilot stroke outcome study. Top. Stroke Rehabil. 2014, 21 (Suppl. S1), S63–S74. [Google Scholar] [CrossRef]
- Bakas, T.; Austin, J.K.; Habermann, B.; Jessup, N.M.; McLennon, S.M.; Mitchell, P.H.; Morrison, G.; Yang, Z.; Stump, T.E.; Weaver, M.T. Telephone Assessment and Skill-Building Kit for Stroke Caregivers: A Randomized Controlled Clinical Trial. Stroke 2015, 46, 3478–3487. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Chair, S.Y.; Chau, J.P.C. Effectiveness of a strength-oriented psychoeducation on caregiving competence, problem-solving abilities, psychosocial outcomes and physical health among family caregiver of stroke survivors: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 87, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Goudarzian, M.; Fallahi-Khoshknab, M.; Dalvandi, A.; Delbari, A.; Biglarian, A. Effect of Telenursing on Levels of Depression and Anxiety in Caregivers of Patients with Stroke: A Randomized Clinical Trial. Iran. J. Nurs. Midwifery Res. 2018, 23, 248–252. [Google Scholar] [PubMed]
- LeLaurin, J.H.; Freytes, I.M.; Findley ke Schmitzberger, M.K.; Eliazar-Macke, N.D.; Orozco, T.; Uphold, C.R. Feasibility and acceptability of a telephone and web-bases stroke caregiver intervention: A pilot randomized controlled trial of the RESCUE intervention. Clin. Rehabil. 2021, 35, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, M.A.; Moriyama, M.; Rahman, M.M.; Kako, M.; El-Monshed, A.H.; Zoromba, M.; Zehry, H.; Khalil, M.H.; El-Gilany, A.H.; Amr, M. Effect of a tailored multidimensional intervention on the care burden among family caregivers of stroke survivors: A randomised controlled trial. BMJ Open 2022, 12, e049741. [Google Scholar] [CrossRef] [PubMed]
- Mou, H.; Lam, S.K.K.; Chien, W.T. Effects of a family-focused dyadic psychoeducational intervention for stroke survivors and their family caregivers: A pilot study. BMC Nurs. 2022, 21, 364. [Google Scholar] [CrossRef]
- Bitek, D.E.; Erol, O. The effect of discharge training and telephone counseling service on patients’ functional status and caregiver burden after stroke: A randomized controlled trial. Neurol. Asia 2023, 28, 583–592. [Google Scholar] [CrossRef]
- Demir Avci, Y.; Gözüm, S. Effects of Transitional Care Model-Based Interventions for Stroke Patients and Caregivers on Caregivers’ Competence and Patient Outcomes: Randomized Controlled Trial. Comput. Inform. Nurs. 2023, 41, 805–814. [Google Scholar] [CrossRef]
- Hussin, R.; Aziz, A.F.A.; Ali, M.F.; Monoto, E.M.M.; Arvinder-Singh, H.S.; Alabed, A.A.A.; Zaidi, W.A.W.; Ibrahim, N.M.; FRCPE. Stroke Riskometer Application (SRA™) influence on lifestyle changes of home bound familial Malaysian stroke caregivers: A randomised controlled trial in a primary care based longer term stroke care facility. BMC Prim. Care 2023, 24, 181. [Google Scholar] [CrossRef]
- Mohammadi, F.; Ardalan, H.B.; Dehghankar, L.; Motalebi, S.A. Effect of Telenursing on the Quality of Life of Caregivers of Older Patients with Stroke. Rev. Recent Clin. Trials 2023, 18, 275–281. [Google Scholar] [CrossRef]
- Perry, L.; Middleton, S. An investigation of family carers’ needs following stroke survivors’ discharge from acute hospital care in Australia. Disabil. Rehabil. 2011, 33, 1890–1900. [Google Scholar] [CrossRef]
- Piran, P.; Thomas, J.; Kunnakkat, S.; Pandey, A.; Gilles, N.; Weingast, S.; Burton, D.; Balucani, C.; Levine, S.R. Mobile Applications for Stroke (MAPPS) Investigators. Medical Mobile Applications for Stroke Survivors and Caregivers. J. Stroke Cerebrovasc. Dis. 2019, 28, 104318. [Google Scholar] [CrossRef]
- Dunne, S.; Close, H.; Richards, N.; Ellison, A.; Lane, A.R. Maximizing Telerehabilitation for Patients with Visual Loss after Stroke: Interview and Focus Group Study with Stroke Survivors, Carers, and Occupational Therapists. J. Med. Internet Res. 2020, 22, e19604. [Google Scholar] [CrossRef]
- Brouns, B.; Meesters, J.J.L.; Wentink, M.M.; de Kloet, A.J.; Arwert, H.J.; Vliet Vlieland, T.P.M.; Boyce, L.W.; van Bodegom-Vos, L. Why the uptake of eRehabilitation programs in stroke care is so difficult-a focus group study in the Netherlands. Implement. Sci. 2018, 13, 133. [Google Scholar] [CrossRef]
- Busetto, L.; Sert, M.; Herzog, F.; Hoffmann, J.; Stang, C.; Amiri, H.; Seker, F.; Purrucker, J.; Mundiyanapurath, S.; Ringleb, P.A.; et al. “But it’s a nice compromise”—Qualitative multi-centre study of barriers and facilitators to acute telestroke cooperation in a regional stroke network. Eur. J. Neurol. 2022, 29, 208–216. [Google Scholar] [CrossRef]
- Lutz, B.J.; Chumbler, N.R.; Lyles, T.; Hoffman, N.; Kobb, R. Testing a home-telehealth programme for US veterans recovering from stroke and their family caregivers. Disabil. Rehabil. 2009, 31, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.M.; Stone, S.D.; Huijbregts, M.P. Remote participants’ experiences with a group-based stroke self-management program using videoconference technology. Rural Remote Health 2012, 12, 1947. [Google Scholar] [CrossRef] [PubMed]
- Al-Khathaami, A.M.; Alshahrani, S.M.; Kojan, S.M.; Al-Jumah, M.A.; Alamry, A.A.; El-Metwally, A.A. Cultural acceptance of robotic telestroke medicine among patients and healthcare providers in Saudi Arabia. Results of a pilot study. Neurosciences 2015, 20, 27–30. [Google Scholar] [PubMed]
- Gong, E.; Gu, W.; Luo, E.; Tan, L.; Donovan, J.; Sun, C.; Yang, Y.; Zang, L.; Bao, P.; Yan, L.L. Development and Local Contextualization of Mobile Health Messages for Enhancing Disease Management Among Community-Dwelling Stroke Patients in Rural China: Multimethod Study. JMIR Mhealth Uhealth 2019, 7, e15758. [Google Scholar] [CrossRef]
- Bakas, T.; Farran, C.J.; Austin, J.K.; Given, B.A.; Johnson, E.A.; Williams, L.S. Content validity and satisfaction with a stroke caregiver intervention program. J. Nurs. Sch. 2009, 41, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Nichols, M.; Singh, A.; Sarfo, F.S.; Treiber, F.; Tagge, R.; Jenkins, C.; Ovbiagele, B. Post-intervention qualitative assessment of mobile health technology to manage hypertension among Ghanaian stroke survivors. J. Neurol. Sci. 2019, 406, 116462. [Google Scholar] [CrossRef]
- Gibson, J.; Lightbody, E.; McLoughlin, A.; McAdam, J.; Gibson, A.; Day, E.; Fitzgerald, J.; May, C.; Price, C.; Emsley, H.; et al. ‘It was like he was in the room with us’: Patients’ and carers’ perspectives of telemedicine in acute stroke. Health Expect. 2016, 19, 98–111. [Google Scholar] [CrossRef]
- Wentink, M.; van Bodegom-Vos, L.; Brouns, B.; Arwert, H.; Houdijk, S.; Kewalbansing, P.; Boyce, L.; Vliet Vlieland, T.; de Kloet, A.; Meesters, J. How to improve eRehabilitation programs in stroke care? A focus group study to identify requirements of end-users. BMC Med. Inform. Decis. Mak. 2019, 19, 145. [Google Scholar] [CrossRef]
- Arnrich, B.; Mayora, O.; Bardram, J.; Tröster, G. Pervasive healthcare: Paving the way for a pervasive, user-centered and preventive healthcare model. Methods Inf. Med. 2010, 49, 67–73. [Google Scholar] [PubMed]
- Bakas, T.; McCarthy, M.J.; Israel, J.; Brehm, B.J.; Dunning, K.; Rota, M.; Turner, M.; Miller, E.L. Adapting the telephone assessment and skill-building kit to the telehealth technology preferences of stroke family caregivers. Res. Nurs. Health 2021, 44, 81–91. [Google Scholar] [CrossRef]
- Bernocchi, P.; Vanoglio, F.; Baratti, D.; Morini, R.; Rocchi, S.; Luisa, A.; Scalvini, S. Home-based telesurveillance and rehabilitation after stroke: A real-life study. Top. Stroke Rehabil. 2016, 23, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Bakas, T.; Jessup, N.M.; McLennon, S.M.; Habermann, B.; Weaver, M.T.; Morrison, G. Tracking patterns of needs during a telephone follow-up programme for family caregivers of persons with stroke. Disabil. Rehabil. 2016, 38, 1780–1790. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, S.W.H. Telemedicine Cost-Effectiveness for Diabetes Management: A Systematic Review. Diabetes Technol. Ther. 2018, 20, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.S.; Pittman, C.A.; Price, C.L.; Nieman, C.L.; Oh, E.S. Telemedicine and Dementia Care: A Systematic Review of Barriers and Facilitators. J. Am. Med. Dir. Assoc. 2021, 22, 1396–1402. [Google Scholar] [CrossRef] [PubMed]
- Ariza-Vega, P.; Prieto-Moreno, R.; Mora-Traverso, M.; Molina-García, P.; Ashe, M.C.; Martín-Matillas, M. Co-creation of mHealth intervention for older adults with hip fracture and family caregivers: A qualitative study. Disabil. Rehabil. Assist. Technol. 2022, 1–10. [Google Scholar] [CrossRef]
| Article | n | Age | Women |
|---|---|---|---|
| Grant et al., 1999 [43] | 30 IG: 10 CG: 10 PAG: 10 | 56 years | 21 |
| Grant et al., 2002 [44] | 74 | 56 ± 12 years | 67 |
| Bakas et al., 2009 [45] | 40 IG: 21 CG: 19 | IG: 56.43 ± 9.61 CG: 57.84 ± 11.8 | IG: 13 CG: 16 |
| Pierce et al., 2009 [46] | 103 IG: 51 CG: 52 | IG: 54 ± 12.2 CG: 55 ± 13.1 | IG: 25 CG: 30 |
| Perrin et al., 2010 [47] | 61 | 58.5 ± 12.0 | 56 |
| Smith et al., 2012 [48] | 32 IG: 19 CG: 19 | IG: 55.3 ± 6.9 CG: 54.9 ± 12.9 | NI |
| Kim et al., 2013 [49] | 36 IG: 18 CG: 18 | IG: 49.8 ± 14.8 CG: 57.3 ± 11.5 | NI |
| Pfeiffer et al., 2014 [50] | 122 IG: 60 CG: 62 | IG: 66.7 ± 9.9 CG: 65.6 ± 10.1 | IG: 46 CG: 49 |
| Bishop et al., 2014 [51] | 49 IG: 23 CG: 26 | 56.8 ± 16. | 32 |
| Bakas et al., 2015 [52] | 254 IG: 123 CG: 131 | IG: 54.0 ± 12.5 CG: 4.7 ± 11.4 | IG: 96 CG: 103 |
| Cheng et al., 2018 [53] | 128 IG: 64 CG: 64 | IG: 49.08 ± 12.09 CG: 49.11 ± 12.90 | IG: 50 CG: 46 |
| Goudarzian et al., 2019 [54] | 152 IG: 76 CG: 76 | IG: 49.04 ± 14.96 CG: 49.48 (15.05) | 90 |
| LeLaurin et al., 2021 [55] | 53 IG 4 weeks: 13 IG 8 weeks: 13 CG: 13 AG: 14 | 60.3 ± 10.1 | 49 |
| Elsheikh et al., 2022 [56] | 110 IG: 55 CG: 55 | IG: 35 (25–55) CG: 35 (25–57) | IG: 42 CG: 40 |
| Mou et al., 2022 [57] | 40 IG: 20 CG: 20 | IG: 45.61 ± 12.14 CG: 48.10 ± 12.20 | IG: 9 CG: 10 |
| Demir et al., 2023 [58] | 63 IG: 33 CG: 30 | IG: 35.48 ± 10.77 CG: 36.07 ± 10.88 | IG: 27 CG: 27 |
| Bitek et al., 2023 [59] | 80 IG: 40 CG: 40 | IG: 54.61 ± 11.73 CG: 51.60 ± 14.18 | IG: 70.6% CG: 71.4% |
| Hussin et al., 2023 [60] | 75 IG: 38 CG: 37 | IG: 46.1 ± 11.3 CG: 45.6 ± 12.8 | IG: 25 CG: 24 |
| Mohammadi et al., 2023 [61] | 84 IG: 42 CG: 42 | IG: 46.16 ± 11.32 CG: 46.1 ± 10.5 | IG: 27 CG: 25 |
| Article | Interventions | Outcomes | Measurement Times |
|---|---|---|---|
| Grant et al., 1999 [43] | IG: telephone contact CG: control PAG: home visit 12 weeks | General health (SF-36) Problem-solving skills (PSI) Satisfaction (CSQ) Depression (CES-D) Caregiver preparedness (PCS) Caregiving burden (CBS) | Week 0 Week 2 Week 5 Week 13 |
| Grant et al., 2002 [44] | IG: social problem-solving telephone partnerships CG: usual discharge planning services SG: sham telephone intervention 12 weeks | General health (SF-36) Problem-solving skills (PSI) Satisfaction (CSQ) Depression (CES-D) Caregiver preparedness (PCS) Caregiving burden (CBS) | Week 0 Week 2 Week 5 Week 13 |
| Bakas et al., 2009 [45] | IG: TASK (phone intervention) CG: attention control group (including phone calls) 8 weeks | Caregiver optimism (LOT-R) Perceived difficulty with tasks (OCBS) Threat appraisal (ACS) Depression (PHQ-9) Caregiver life changes (BCOS) General health (SF-36) | Week 0 Week 4 Week 8 Week 12 |
| Pierce et al., 2009 [46] | IG: web-based intervention CG: usual care 12 months | Depression (CES-D) Satisfaction (SWLS) | Week 0 Month 3 Month 6 Month 9 Month 12 |
| Perrin et a. 2010 [47] | IG: transition assistance program, including 4 videophones CG: standard care 6 weeks | Caregiver burden (CSI) Depression (CES-D) Caregiver satisfaction (VACCHTPSS) | Week 0 Week 4 Week 12 |
| Smith et al., 2012 [48] | IG: web-based intervention (online information, educational videos, chat sessions, e-mail) CG: relevant online information 11 weeks | Depression (CES-D and PHQ-9) Mastery (Mastery Scale) Self esteem (SES) Social support (MOS social support survey) Treatment credibility, reported effort, and perceived benefit | Week 0 Week 11 Week 15 |
| Kim et al., 2013 [49] | IG: web-based intervention CG: usual care 9 weeks | Caregiver mastery (CGMS) | Week 0 Month 3 |
| Pfeiffer et al., 2014 [50] | IG: telephone-based problem-solving intervention CG: information letters 3 months | Depression (CES-D) Caregiving competence (SCQ) | Week 0 Month 3 Month 12 |
| Bishop et al., 2014 [51] | FIIT: family intervention telephone tracking CG: standard medical follow-up 6 months | Functional independence (FAI) Depression (GDS) Family functioning (FAD) | Week 0 Month 3 Month 6 |
| Bakas et al., 2015 [52] | IG: TASK II (phone intervention) CG: information, support, and referral (phone) 12 weeks | Depression (PHQ-9) Caregiver life changes (BCOS) Unhealthy days | Week 0 Week 8 Week 12 Week 24 Week 52 |
| Cheng et al., 2018 [53] | IG: strength-oriented psychoeducational programme (six 30 min phone sessions) CG: usual care 26 weeks | Caregiving competence (CGS) Caregiver burden (CSI) Problem-solving skills (PSI) Depression (CES-D) General health (SF-12) Social support (SSQ) | Week 0 Week 26 Week 32 Week 40 |
| Goudarzian et al., 2019 [54] | IG: phone consultation CG: usual care 3 moths | Depression (BDI) Anxiety (BAI) | Week 0 Month 3 |
| LeLaurin et al., 2021 [55] | IG: RESCUE programme: web-based and phone intervention CG: usual care 4–8 weeks | Depression (CES-D) Caregiver burden (ZBISF) | Week 0 Week 5 or 9 Week 21 or 25 |
| Elsheikh et al., 2022 [56] | IG: multiple methods, including 6 phone calls CG: institutional booklet 6 months | Quality of life (WHOQOL-BREF) Care burden (ZBISF) | Week 0 Month 3 Month 6 |
| Mou et al., 2002 [57] | IG: patient–caregiver dyads education (telephone calls) CG: usual care 4 weeks | Caregiver burden (CSI) Family functioning (F-COPES) Caregiving competence (CCS) Anxiety (GAD-7) | Week 0 Week 4 |
| Betik et al., 2023 [58] | IG: discharge training and telephone counselling (4 sessions) CG: routine care 12 weeks | Caregiver burden (ZCBS) | Week 0 Month 3 |
| Demir et al., 2023 [59] | IG: transitional care model (education via web and phone calls) CG: usual care 12 weeks CG: routine care 12 weeks | Caregiving competence (CCS) Caregiver preparedness (PCS) Caregivers’ e-Health Literacy (eHLS) Caregiver burden (MBIGF) | Week 0 Week 12 |
| Hussin et al., 2023 [60] | IG: stroke riskometer application CG: usual care 12 weeks | Lifestyle changes (LS7) Caregiver’s stroke risk | Week 0 Week 12 |
| Mohammadi et al., 2023 [61] | IG: phone and social media CG: usual care 12 weeks | General health (SF-36) | Week 0 Week 12 |
| Article | Outcomes | Results |
|---|---|---|
| Grant et al., 1999 [43] | CES-D week 2 = ß = 1.63 (p < 0.01) CES-D week 5 = ß = 0.91 (p = 0.05) PSI week 2 = ß = −2.26 (p < 0.01) PSI week 5 = ß = −2.14 (p < 0.05) PCS week 1 = ß = 1.36 (p < 0.01) PCS week 5 = ß = 0.73 (p < 0.05) | The IG scored statistically significantly better on depression, problem-solving skills, and caregiving preparedness during the intervention (weeks 2 and 5) compared to the other two groups. It also improved, although without significant results, after the intervention (weeks 13). |
| Grant et al., 2002 [44] | PCS = IG = 19.12 ± 1.61 (p < 0.01); CG = 0.01 ± 1.65 (p > 0.05); SG = 0.78 ± 1.63 (p > 0.05) CES-D = IG = 14.68 ± 1.61 (p < 0.01); CG = 0.08 ± 1.65 (p > 0.05); SG = 3.56 ± 1.63 (p > 0.05) PSI = IG = −7.2 ± 1.59 (p < 0.05); GC = 1.91 ± 1.65 (p > 0.05); SG = 0. ± 1.62 (p > 0.05) | The IG showed better problem-solving skills, greater caregiver preparedness, and less depression compared to SG and CG (p < 0.05). No differences were found in the caregiving burden. |
| Bakas et al., 2009 [45] | LOT-R week 4 = 18.34 ± 0.92 vs. 14.78 ± 0.97 (p < 0.05) LOT-R week 8 = 18.14 ± 0.84 vs. 14.85 ± 0.89 (p < 0.05) LOT-R week 12 = 17.61 ± 1 vs. 13.59 ± 1.06 (p < 0.05) OCBS week 4 = 22.87 ± 1.38 vs. 27.94 ± 1.47 (p < 0.05) OCBS week 8 = 22.61 ± 1.39 vs. 26.07 ± 1.48 (p > 0.05) OCBS week 12 = 22.34 ± 1.41 vs. 24.63 ± 1.49 (p > 0.05) ACS week 4 = 31.55 ± 1.83 vs. 34.5 ± 1.94 (p > 0.05) ACS week 8 = 28.38 ± 1.86 vs. 35.48 ± 1.98 (p < 0.05) ACS week 12 = 30.64 ± 2.84 vs. 38.92 ± 1.87 (p < 0.05) | The IG showed significant increases in optimism (weeks 4, 8, 12), improvement in task difficulty (week 4), and threat appraisal (weeks 8 and 12) compared to the CG. |
| Pierce et al., 2009 [46] | CES-D = 12.3 ± 9.8 vs. 9 ± 9.1 (p > 0.05) SWLS = 21.7± 6.7 vs. 24.6± 6 (p > 0.05) | No statistical difference between groups was found in depression and satisfaction. |
| Perrin et al., 2010 [47] | CSI 1–3 months a = −1.64 ± 3.31 vs. 2 ± 6.26 (p < 0.05) CES-D = −1.81 b (p > 0.05) | The IG shows significantly lower caregiver strain at 3 months. The IG showed also less depression than the CG, but without statistical significance. |
| Smith et al., 2012 [48] | CES-D week 11 = 13.9 ± 2 vs. 19.7 ± 1.8 (p < 0.05) CES-D week 15 = 13.4 ± 1.6 vs. 24.1 ± 0.5 (p < 0.05) | The IG showed significantly lower depression than the CG in weeks 11 and 15. No significant differences were found for other variables. |
| Kim et al., 2013 [49] | CGMS = (19.7 ± 2.8 vs. 22.8 ± 2.5) (p < 0.05) | The IG improved significantly in mastery. |
| Pfeiffer et al., 2014 [50] | CES-D months 3 = 17.3 ± 7.55 vs. 20.4 ± 9.44 (p < 0.05) CES-D months 12 = 2.4 ± 7.52 vs. 18.2 ± 10.87 (p < 0.05) | The IG showed significantly lower levels of depressive symptoms after both 3 and 12 months. No significant differences were found for other variables. |
| Bishop et al., 2014 [51] | FAD months 3 = 2.4 ± 4.6 vs. −2.5 ± 3.5 (p < 0.05) FAD month 6 = 2.7 ± 6.4 vs. −2.8 ± 4 (p < 0.05) FAI month 3 = −0.65 ± 5.4 vs. 2.13 ± 3.72 (p < 0.05) FAI month 6 = −0.84 ± 4.5 vs. 1.74 ± 3.8 (p < 0.05) | The IG showed an improvement in both independence functioning in months 3 and 6 and family functioning in months 3 and 6. |
| Bakas et al., 2015 [52] | PHQ-9 weeks 1–8 = −3.6 ± 0.8 vs. −0.9 ± 0.7 (p < 0.05) PHQ.9 weeks 1–12= −3.9 ± 0.8 vs. −2 ± 0.7 (p < 0.05) PHQ-9 weeks 1–24 = −3.6 ± 0.7 vs. −1.6 ± 0.6 (p < 0.05) PHQ-9 weeks 1–52 = −4 ± 0.8 vs. −1.1 ± 0.7 (p < 0.05) BCOS weeks 1–8 = 2.9 ± 1.3 vs. 1.2 ± 1.2 (p < 0.05) Unhealthy days weeks 1–8 = −1.1 ± 0.9 vs. 1.8 ± 0.9 (p < 0.05) | There was a statistically significant reduction in depression in weeks 8, 12, 24, and 52; an improvement in life changes in week 8 and a reduction in unhealthy days in week 8 in the IG. |
| Cheng et al., 2018 [53] | CGS week 26 = 12.02 ± 1.79 vs. 11.16 ± 2.35 CGS week 32 = 12.31 ± 1.46 vs. 10.65 ± 2.07 CGS week 40 = 12.48 ± 1.28 vs. 10.65 ± 2.10 (p < 0.05) PSI week 26 = 94.69 ± 12.56 vs. 103.67 ± 19.08 (p < 0.05) PSI week 32 = 93.96 ± 13.89 vs. 106.70 ± 20.12 (p < 0.05) PSI week 40 = 92.59 ± 10.82 vs. 108.08 ± 18.61 (p < 0.05) SSQ week 26 = 5.15 ± 0.55 vs. 4.90 ± 0.84 (p < 0.05) SSQ week 32 = 5.23 ± 0.51 vs. 4.83 ± 0.88 (p < 0.05) SSQ week 40 = 5.11 ± 0.49 vs. 4.81 ± 0.80 (p < 0.05) | The IG improved, compared to CG, throughout the study in caregiving competence problem-solving coping abilities (T0–T1: −5.93 (−11.08, −6.81); T0–T2: −8.74 (−13.81, −3.67); T0–T3: −12.34 (−17.88, −6.81) and social support satisfaction (T0–T1: 0.28 (0.08, 0.47); T0–T1: 0.42 (0.20, 0.64); T0–T3: 0.33 (0.10, 0.55) (p < 0.01). |
| Goudarzian et al., 2019 [54] | BAI = 30.18 ± 5.53 vs. 33.59 ± 6.4 (p < 0.05) BDI = 35.41 ± 9.34 vs. 35.85 ± 7.8 (p > 0.05) | The IG statistically improved in anxiety, but not (p > 0.05) in depression. |
| LeLaurin et al., 2021 [55] | CES-D week 5/9 = 9.4 ± 6.1 vs. 16.4 ± 8.6 vs. 16.2 ± 10.4 vs. 13.7 ± 12.5 CES-D week 21/25 = 12 ± 6.3 vs. 12.9 ± 10.4 vs. 12.7 ± 11.1 vs. 11.6 ± 10.7 ZBISF week 5/9 = 9.4 ± 6.1 vs. 16.4 ± 8.6 vs. 16.2 ± 10.4 vs. 13.7 ± 12.5 ZBISF week 21/25 = 12.6 ± 12.4 vs. 12.9 ± 10.4 vs. 12.7 ± 11.1 vs. 11.6 ± 10.7 | Although the study was not powered for significance testing, no statistically significant findings were found. |
| Elsheikh et al., 2022 [56] | WHOQOL-BREF psychological month 3 = 43.41 ± 19.93 vs. 42.73 ± 18.89 WHOQOL-BREF psychological month 6 = 43.86 ± 19.88 vs. 42.35 ± 19.04 WHOQOL-BREF social month 3 = 71.06 ± 15.45 vs. 70.91 ± 14.77 WHOQOL-BREF social month 6 = 72.12 ± 15.57 vs. 69.85 ± 16.08 ZBISF month 3 = 34.38 ± 7.09 vs. 32.53 ± 7.96 (p > 0.05) ZBISF month 6 = 34.60 ± 7.07 vs. 33.24 ± 7.83 (p > 0.05) | Although the effects of group and time interaction on both the psychological and social relationship domains were significant (p < 0.05), no significant differences within groups or between groups for all domains of QoL were found. No differences were found between groups in care burden. |
| Mou et al., 2022 [57] | CBI = 32.45 ± 15.86 vs. 44.4 ± 16.5 (p < 0.05) CCS = 11.75 ± 2.51 vs. 11.4 ± 1.35 (p < 0.05) F-COPES = 98.75 ± 7.65 vs. 93.4 ± 8.52 (p > 0.05) GAD-7 = 3.45 ± 3.39 vs. 4.65 ± 4.07 (p > 0.05) | The caregiver burden was significantly reduced in the IG compared to the CG. The IG also improved caregivers’ competence. |
| Bitek et al., 2023 [58] | ZCBS = 32.14 ± 15.4 vs. 34.27 ± 14.2 (p < 0.05) | The caregiver´s burden was significantly lower in the IG compared to the CG after the intervention. |
| Demir et al., 2023 [59] | CCS = 13.48 ± 2.31 vs. 11.37 ± 2.48 (p < 0.001) PCS = 28.48 ± 4.74 vs. 20.93 ± 7.10 (p < 0.001) eHLS = 34.42 ± 4.74 vs. 26.93 ± 8.53 (p < 0.001) MBIGF emotional exhaustion = 7.24 ± 3.27 vs. 8.90 ± 3.58 (p < 0.05) MBIGF personal accomplishment = 10.45 ± 4.13 vs. 16.93 ± 5.10 (p < 0.05) MBIGF depersonalization= 6.03 ± 2.38 vs. 6.43 ± 2.70 (p > 0.05) | After the intervention, the IG exhibited significantly better caregiver competence, preparation for care, and e-health literacy than the CG. The IG showed also better results in emotional exhaustion and personal accomplishment. |
| Hussin et al., 2023 [60] | LS7 c = 9.29 (1.59) vs. 8.41 (1.87) (p < 0.05) Stroke risk 5 years c = 2.04 (1.21) vs. 2.57 (1.70) (p > 0.05) Stroke risk 10 years c = 3.53 (2.50) vs. 4.34 (3.28) (p > 0.05) | The IG showed a better improvement in LS7 than CG at 3 months (median difference = (95% CI) = 0.88 (1.68–0.08) (p < 0.05). No differences were found in the risk of stroke (p > 0.05). |
| Mohammadi et al., 2023 [61] | SF-36 psychological subscale = 64.4 ± 14.53 vs. 51.09 ± 14.07 (p < 0.05) SF-36 physical subscale = 80.98 ± 17.06 vs. 77.71 ± 15.21 (p > 0.05) | The IG showed significant differences in the psychological subscale of the SF-36 compared to the CG, but not in the physical domain. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zuil-Escobar, J.C.; Martín-Urrialde, J.A.; Mesa-Jiménez, J.A.; Palomo-Carrión, R.; Martínez-Cepa, C.B. Telehealth in Informal Caregivers of Stroke Survivors: A Systematic Review. J. Clin. Med. 2024, 13, 1810. https://doi.org/10.3390/jcm13061810
Zuil-Escobar JC, Martín-Urrialde JA, Mesa-Jiménez JA, Palomo-Carrión R, Martínez-Cepa CB. Telehealth in Informal Caregivers of Stroke Survivors: A Systematic Review. Journal of Clinical Medicine. 2024; 13(6):1810. https://doi.org/10.3390/jcm13061810
Chicago/Turabian StyleZuil-Escobar, Juan Carlos, Jose Antonio Martín-Urrialde, Juan Andrés Mesa-Jiménez, Rocío Palomo-Carrión, and Carmen Belén Martínez-Cepa. 2024. "Telehealth in Informal Caregivers of Stroke Survivors: A Systematic Review" Journal of Clinical Medicine 13, no. 6: 1810. https://doi.org/10.3390/jcm13061810
APA StyleZuil-Escobar, J. C., Martín-Urrialde, J. A., Mesa-Jiménez, J. A., Palomo-Carrión, R., & Martínez-Cepa, C. B. (2024). Telehealth in Informal Caregivers of Stroke Survivors: A Systematic Review. Journal of Clinical Medicine, 13(6), 1810. https://doi.org/10.3390/jcm13061810