
Fasting Plasma Ketone Bodies Are Associated with NT-proBNP: A Potential Mechanism to Provide Fuel for the Failing Heart

 ,
,  , , and
, , and
Abstract

1. Introduction
2. Patients and Methods
2.1. Study Population and Definitions
2.2. Laboratory Methods
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Murphy, S.P.; Ibrahim, N.E.; Januzzi, J.L. Heart Failure with Reduced Ejection Fraction: A Review. JAMA J. Am. Med. Assoc. 2020, 324, 488–504. [Google Scholar] [CrossRef] [PubMed]
- Emmons-Bell, S.; Johnson, C.; Roth, G. Prevalence, Incidence and Survival of Heart Failure: A Systematic Review. Heart 2022, 108, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Laffel, L. Ketone Bodies: A Review of Physiology, Pathophysiology and Application of Monitoring to Diabetes. Diabetes Metab. Res. Rev. 1999, 15, 412–426. [Google Scholar] [CrossRef]
- Watanabe, M.; Tozzi, R.; Risi, R.; Tuccinardi, D.; Mariani, S.; Basciani, S.; Spera, G.; Lubrano, C.; Gnessi, L. Beneficial Effects of the Ketogenic Diet on Nonalcoholic Fatty Liver Disease: A Comprehensive Review of the Literature. Obes. Rev. 2020, 21, e13024. [Google Scholar] [CrossRef] [PubMed]
- Lommi, J.; Kupari, M.; Koskinen, P.; Näveri, H.; Leinonen, H.; Pulkki, K.; Härkönnen, M. Blood Ketone Bodies in Congestive Heart Failure. JACC 1996, 28, 665–672. [Google Scholar] [CrossRef]
- Selvaraj, S.; Kelly, D.P.; Margulies, B.K. Implications of Altered Ketone Metabolism and Therapeutic Ketosis in Heart Failure Senthil. Circulation 2020, 141, 1800–1812. [Google Scholar] [CrossRef]
- Marcondes-Braga, F.G.; Gutz, I.G.R.; Batista, G.L.; Saldiva, P.H.N.; Ayub-Ferreira, S.M.; Issa, V.S.; Mangini, S.; Bocchi, E.A.; Bacal, F. Exhaled Acetone as a New Biomarker of Heart Failure Severity. Chest 2012, 142, 457–466. [Google Scholar] [CrossRef]
- Flores-Guerrero, J.L.; Westenbrink, B.D.; Connelly, M.A.; Otvos, J.D.; Groothof, D.; Shalaurova, I.; Garcia, E.; Navis, G.; de Boer, R.A.; Bakker, S.J.L.; et al. Association of Beta-Hydroxybutyrate with Development of Heart Failure: Sex Differences in a Dutch Population Cohort. Eur. J. Clin. Investig. 2021, 51, e13468. [Google Scholar] [CrossRef]
- Stanley, W.C.; Recchia, F.A.; Lopaschuk, G.D. Myocardial Substrate Metabolism in the Normal and Failing Heart. Physiol. Rev. 2005, 85, 1093–1129. [Google Scholar] [CrossRef]
- Horton, J.L.; Davidson, M.T.; Kurishima, C.; Vega, R.B.; Powers, J.C.; Matsuura, T.R.; Petucci, C.; Lewandowski, E.D.; Crawford, P.A.; Muoio, D.M.; et al. The Failing Heart Utilizes 3-Hydroxybutyrate as a Metabolic Stress Defense. JCI Insight 2019, 4, e124079. [Google Scholar] [CrossRef]
- Murashige, D.; Jang, C.; Neinast, M.; Edwards, J.J.; Cowan, A.; Hyman, M.C.; Rabinowitz, J.D.; Frankel, D.S.; Arany, Z. Comprehensive Quantification of Fuel Use by the Failing and Nonfailing Human Heart. Science 1979 2020, 370, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Yurista, S.R.; Nguyen, C.T.; Rosenzweig, A.; de Boer, R.A.; Westenbrink, B.D. Ketone Bodies for the Failing Heart: Fuels That Can Fix the Engine? Trends Endocrinol. Metab. 2021, 32, 814–826. [Google Scholar] [CrossRef] [PubMed]
- Oremus, M.; McKelvie, R.; Don-Wauchope, A.; Santaguida, P.L.; Ali, U.; Balion, C.; Hill, S.; Booth, R.; Brown, J.A.; Bustamam, A.; et al. A Systematic Review of BNP and NT-ProBNP in the Management of Heart Failure: Overview and Methods. Heart Fail. Rev. 2014, 19, 413–419. [Google Scholar] [CrossRef]
- Mueller, C.; McDonald, K.; de Boer, R.A.; Maisel, A.; Cleland, J.G.F.; Kozhuharov, N.; Coats, A.J.S.; Metra, M.; Mebazaa, A.; Ruschitzka, F.; et al. Heart Failure Association of the European Society of Cardiology Practical Guidance on the Use of Natriuretic Peptide Concentrations. Eur. J. Heart Fail. 2019, 21, 715–731. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, W.; Rühs, H.; Burghaus, R.; Diedrich, C.; Duwal, S.; Eissing, T.; Garmann, D.; Meyer, M.; Ploeger, B.; Lippert, J. NT-ProBNP Qualifies as a Surrogate for Clinical End Points in Heart Failure. Clin. Pharmacol. Ther. 2021, 110, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Lafontan, M.; Moro, C.; Sengenes, C.; Galitzky, J.; Crampes, F.; Berlan, M. An Unsuspected Metabolic Role for Atrial Natriuretic Peptides: The Control of Lipolysis, Lipid Mobilization, and Systemic Nonesterified Fatty Acids Levels in Humans. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2032–2042. [Google Scholar] [CrossRef] [PubMed]
- Beleigoli, A.M.R.; Diniz, M.F.H.S.; Ribeiro, A.L.P. Natriuretic Peptides: Linking Heart and Adipose Tissue in Obesity and Related Conditions—A Systematic Review. Obes. Rev. 2009, 10, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Frühbeck, G.; Méndez-Giménez, L.; Fernández-Formoso, J.A.; Fernández, S.; Rodríguez, A. Regulation of Adipocyte Lipolysis. Nutr. Res. Rev. 2014, 27, 63–93. [Google Scholar] [CrossRef]
- Sengenès, C.; Berlan, M.; Glisezinski, I.; Lafontan, M.; Galitzky, J. Natriuretic Peptides: A New Lipolytic Pathway in Human Adipocytes. FASEB J. 2000, 14, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Galitzky, J.; Sengenès, C.; Thalamas, C.; Marques, M.A.; Senard, J.M.; Lafontan, M.; Berlan, M. The Lipid-Mobilizing Effect of Atrial Natriuretic Peptide Is Unrelated to Sympathetic Nervous System Activation or Obesity in Young Men. J. Lipid Res. 2001, 42, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Voorrips, S.N.; Boorsma, E.M.; Beusekamp, J.C.; De-Boer, R.A.; Connelly, M.A.; Dullaart, R.P.F.; Van-Der-Meer, P.; Van-Veldhuisen, D.J.; Voors, A.A.; Damman, K.; et al. Longitudinal Changes in Circulating Ketone Body Levels in Patients with Acute Heart Failure: A Post Hoc Analysis of the EMPA-Response-AHF Trial. J. Card. Fail. 2023, 29, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, Y.; Nagoshi, T.; Inoue, Y.; Tanaka, Y.; Takahashi, H.; Oi, Y.; Kimura, H.; Minai, K.; Yoshimura, M. Close Linkage between Blood Total Ketone Body Levels and B-Type Natriuretic Peptide Levels in Patients with Cardiovascular Disorders. Sci. Rep. 2021, 11, 6498. [Google Scholar] [CrossRef] [PubMed]
- Hillege, H.L.; Janssen, W.M.T.; Bak, A.A.A.; Diercks, G.F.H.; Grobbee, D.E.; Crijns, H.J.G.M.; Van Gilst, W.H.; De Zeeuw, D.; De Jong, P.E. Microalbuminuria Is Common, also in a Nondiabetic, Nonhypertensive Population, and an Independent Indicator of Cardiovascular Risk Factors and Cardiovascular Morbidity. J. Intern. Med. 2001, 249, 519–526. [Google Scholar] [CrossRef]
- Brouwers, F.P.; Van Gilst, W.H.; Damman, K.; Van Den Berg, M.P.; Gansevoort, R.T.; Bakker, S.J.L.; Hillege, H.L.; Van Veldhuisen, D.J.; Van Der Harst, P.; De Boer, R.A. Clinical Risk Stratification Optimizes Value of Biomarkers to Predict New-Onset Heart Failure in a Community-Based Cohort. Circ. Heart Fail. 2014, 7, 723–731. [Google Scholar] [CrossRef]
- Paulus, W.J.; Tschöpe, C.; Sanderson, J.E.; Rusconi, C.; Flachskampf, F.A.; Rademakers, F.E.; Marino, P.; Smiseth, O.; Keilenaer, G.; Leite-Moreira, A.F.; et al. How to Diagnose Diastolic Heart Failure—A Consensus Statement. Eur. Heart J. 2007, 28, 2421–2423. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating Glomerular Filtration Rate from Serum Creatinine and Cystatin C. New Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef]
- Garcia, E.; Shalaurova, I.; Matyus, S.P.; Oskardmay, D.N.; Otvos, J.D.; Dullaart, R.P.F.; Connelly, M.A. Ketone Bodies Are Mildly Elevated in Subjects with Type 2 Diabetes Mellitus and Are Inversely Associated with Insulin Resistance as Measured by the Lipoprotein Insulin Resistance Index. J. Clin. Med. 2020, 9, 321. [Google Scholar] [CrossRef]
- Pandey, A.; Vaduganathan, M.; Patel, K.V.; Ayers, C.; Ballantyne, C.M.; Kosiborod, M.N.; Carnethon, M.; DeFilippi, C.; McGuire, D.K.; Khan, S.S.; et al. Biomarker-Based Risk Prediction of Incident Heart Failure in Pre-Diabetes and Diabetes. JACC Heart Fail. 2021, 9, 215–223. [Google Scholar] [CrossRef]
- Després, J.P.; Moorjani, S.; Tremblay, A.; Ferland, M.; Lupien, P.J.; Nadeau, A.; Bouchard, C. Relation of High Plasma Triglyceride Levels Associated with Obesity and Regional Adipose Tissue Distribution to Plasma Lipoprotein-Lipid Composition in Premenopausal Women. Clin. Investig. Med. 1989, 12, 374–380. [Google Scholar]
- Rydén, M.; Bäckdahl, J.; Petrus, P.; Thorell, A.; Gao, H.; Coue, M.; Langin, D.; Moro, C.; Arner, P. Impaired Atrial Natriuretic Peptide-Mediated Lipolysis in Obesity. Int. J. Obes. 2016, 40, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Post, A.; Garcia, E.; van den Berg, E.H.; Flores-Guerrero, J.L.; Gruppen, E.G.; Groothof, D.; Westenbrink, B.D.; Connelly, M.A.; Bakker, S.J.L.; Dullaart, R.P.F. Nonalcoholic Fatty Liver Disease, Circulating Ketone Bodies and All-Cause Mortality in a General Population-Based Cohort. Eur. J. Clin. Investig. 2021, 51, e13627. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Yang, R.; Kuang, M.; Yu, M.; Zhong, M.; Zou, Y. Triglyceride Glucose-Body Mass Index in Identifying High-Risk Groups of Pre-Diabetes. Lipids Health Dis. 2021, 20, 161. [Google Scholar] [CrossRef] [PubMed]
- Lopaschuk, G.D.; Karwi, Q.G.; Tian, R.; Wende, A.R.; Abel, E.D. Cardiac Energy Metabolism in Heart Failure. Circ. Res. 2021, 128, 1487–1513. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Zhang, C.; Shang, F.F.; Luo, M.; You, Y.; Zhai, Q.; Xia, Y.; Luo, S. Ketogenic Diet Ameliorates Cardiac Dysfunction via Balancing Mitochondrial Dynamics and Inhibiting Apoptosis in Type 2 Diabetic Mice. Aging Dis. 2020, 11, 229–240. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Polidori, D.; Iijima, H.; Goda, M.; Maruyama, N.; Inagaki, N.; Crawford, P.A. Intra- and Inter-Subject Variability for Increases in Serum Ketone Bodies in Patients with Type 2 Diabetes Treated with the Sodium Glucose Co-Transporter 2 Inhibitor Canagliflozin. Diabetes Obes. Metab. 2018, 20, 1321–1326. [Google Scholar] [CrossRef]
- Okamoto, A.; Yokokawa, H.; Sanada, H.; Naito, T. Changes in Levels of Biomarkers Associated with Adipocyte Function and Insulin and Glucagon Kinetics During Treatment with Dapagliflozin Among Obese Type 2 Diabetes Mellitus Patients. Drugs R&D 2016, 16, 255–261. [Google Scholar] [CrossRef]
- Ferrannini, E.; Baldi, S.; Frascerra, S.; Astiarraga, B.; Heise, T.; Bizzotto, R.; Mari, A.; Pieber, T.R.; Muscelli, E. Shift to Fatty Substrate Utilization in Response to Sodium-Glucose Cotransporter 2 Inhibition in Subjects without Diabetes and Patients with Type 2 Diabetes. Diabetes 2016, 65, 1190–1196. [Google Scholar] [CrossRef]
- Selvaraj, S.; Fu, Z.; Jones, P.; Kwee, L.C.; Windsor, S.L.; Ilkayeva, O.; Newgard, C.B.; Margulies, K.B.; Husain, M.; Inzucchi, S.E.; et al. Metabolomic Profiling of the Effects of Dapagliflozin in Heart Failure with Reduced Ejection Fraction: DEFINE-HF. Circulation 2022, 146, 808–818. [Google Scholar] [CrossRef]
- Yang, X.; Liu, Q.; Li, Y.; Ding, Y.; Zhao, Y.; Tang, Q.; Wu, T.; Chen, L.; Pu, S.; Cheng, S.; et al. Inhibition of the Sodium–Glucose Co-Transporter SGLT2 by Canagliflozin Ameliorates Diet-Induced Obesity by Increasing Intra-Adipose Sympathetic Innervation. Br. J. Pharmacol. 2021, 178, 1756–1771. [Google Scholar] [CrossRef]
- Moro, C.; Lafontan, M. Natriuretic Peptides and CGMP Signaling Control of Energy Homeostasis. Am. J. Physiol. Heart Circ. Physiol. 2013, 304, 358–368. [Google Scholar] [CrossRef]
- Loomba, R.; Sanyal, A.J. The Global NAFLD Epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef]
- Vos, M.; Faasse, S.; Braun, H. The Role of NAFLD in Cardiometabolic Disease: An Update. F1000Research 2018, 7, 170. [Google Scholar] [CrossRef]
- Bozkurt, B.; Aguilar, D.; Deswal, A.; Dunbar, S.B.; Francis, G.S.; Horwich, T.; Jessup, M.; Kosiborod, M.; Pritchett, A.M.; Ramasubbu, K.; et al. Contributory Risk and Management of Comorbidities of Hypertension, Obesity, Diabetes Mellitus, Hyperlipidemia, and Metabolic Syndrome in Chronic Heart Failure: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e535–e578. [Google Scholar] [CrossRef]
- Szili-Torok, T.; de Borst, M.H.; Garcia, E.; Gansevoort, R.T.; Dullaart, R.P.F.; Connelly, M.A.; Bakker, S.J.L.; Tietge, U.J.F. Fasting Ketone Bodies and Incident Type 2 Diabetes in the General Population. Diabetes 2023, 72, 1187–1192. [Google Scholar] [CrossRef]
- van der Vaart, A.; Knol, M.G.E.; de Borst, M.H.; Bakker, S.J.L.; Connelly, M.A.; Garcia, E.; Bilo, H.J.G.; van Dijk, P.R.; Dullaart, R.P.F. The Paradoxical Role of Circulating Ketone Bodies in Glycemic Control of Individuals with Type 2 Diabetes: High Risk, High Reward? Biomolecules 2022, 12, 1318. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| All Participants | Participants with HF | Participants without HF | p-Value | |
|---|---|---|---|---|
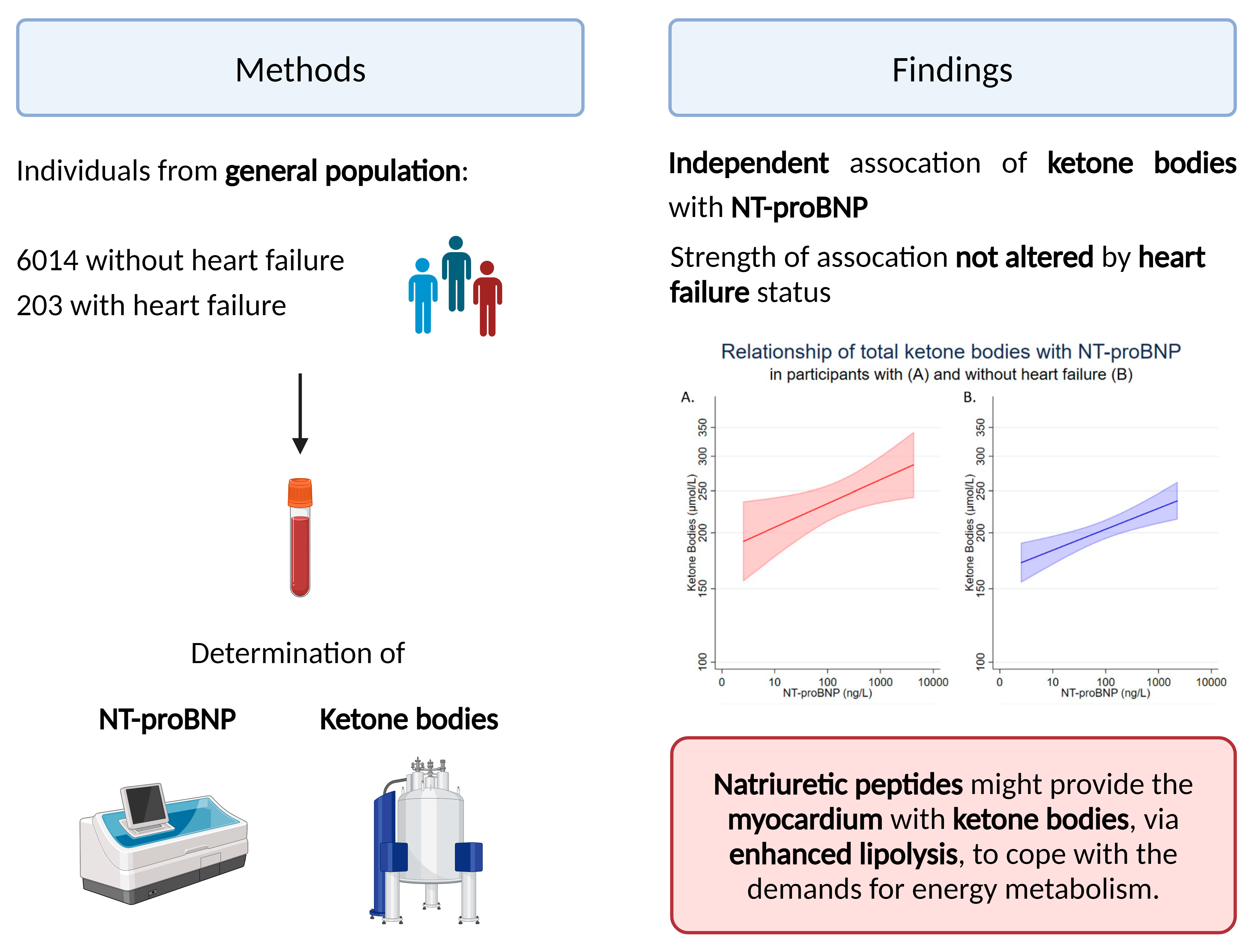
| Number | 6217 | 203 | 6014 | |
| Age, years | 53.6 (12.0) | 65.87 (9.9) | 53.1 (11.9) | <0.001 |
| Females, n (%) | 3149 (50.7%) | 66 (32.5%) | 3083 (51.3%) | <0.001 |
| BMI, kg/m2 | 26.69 (4.35) | 28.79 (4.49) | 26.62 (4.33) | <0.001 |
| Waist circumference, cm | 92.1 (12.8) | 101.4 (13.4) | 91.7 (12.7) | <0.001 |
| Waist–hip ratio | 0.90 (0.09) | 0.96 (0.09) | 0.90 (0.09) | <0.001 |
| SBP, mmHg | 126 (19) | 138 (24) | 126 (18) | <0.001 |
| DBP, mmHg | 73 (9) | 76 (10) | 73 (9) | <0.001 |
| CVD, n (%) | 243 (3.9%) | 49 (24.1%) | 194 (3.2%) | <0.001 |
| Type 2 diabetes, n (%) | 386 (6.2%) | 44 (21.7%) | 342 (5.7%) | <0.001 |
| Hypertension, n (%) | 654 (10.7%) | 65 (32.7%) | 589 (10.0%) | <0.001 |
| Total cholesterol, mmol/L | 5.43 (1.05) | 5.28 (1.06) | 5.43 (1.05) | 0.036 |
| Triglycerides, mmol/L | 1.11 (0.81, 1.61) | 1.28 (1.00, 1.71) | 1.11 (0.80, 1.61) | <0.001 |
| Plasma NT-proBNP, ng/L | 42 (21, 81) | 168 (75, 443) | 41 (21, 77) | <0.001 |
| β-hydroxybutyrate, µmol/L | 122.0 (93.2, 170.1) | 153.9 (111.3, 237.3) | 121.3 (92.8, 168.8) | <0.001 |
| Acetoacetate, µmol/L | 38.4 (25.8, 57.4) | 46.58 (29.2, 74.8) | 38.18 (25.7, 57.0) | <0.001 |
| Acetone, µmol/L | 19.6 (12.7, 29.2) | 24.24 (16.0, 36.3) | 19.5 (12.6, 29.0) | <0.001 |
| Total ketone bodies, µmol/L | 177.8 (139.2, 250.2) | 218.7 (162.5, 338.0) | 176.7 (138.8, 247.4) | <0.001 |
| eGFR, mL/min/1.73 m2 | 92.9 (16.9) | 76.11 (20.0) | 93.43 (16.5) | <0.001 |
| UAE, mg/24h | 8.6 (6.0, 16.1) | 16.4 (8.0, 59.8) | 8.5 (6.0, 15.5) | <0.001 |
| ACEi use, n (%) | 383 (6.5%) | 48 (23.9%) | 335 (5.9%) | <0.001 |
| ARB use, n (%) | 127 (2.1%) | 24 (11.9%) | 103 (1.8%) | <0.001 |
| Betablocker use, n (%) | 594 (10.0%) | 68 (33.8%) | 526 (9.2%) | <0.001 |
| Statin use, n (%) | 474 (8.0%) | 53 (26.4%) | 421 (7.4%) | <0.001 |
| Diuretic use, n (%) | 214 (3.6%) | 30 (14.9%) | 184 (3.2%) | <0.001 |
| HFrEF | HFpEF | p-Value | |
|---|---|---|---|
| Number | 146 | 57 | |
| Age, years | 65.22 (10.24) | 67.52 (8.62) | 0.130 |
| Females, n (%) | 38 (26.0%) | 28 (49.1%) | 0.002 |
| BMI, kg/m2 | 28.2 (4.3) | 30.2 (4.6) | 0.004 |
| Waist circumference, cm | 101.0 (13.3) | 102.7 (13.9) | 0.390 |
| Waist–hip ratio | 0.96 (0.08) | 0.94 (0.10) | 0.110 |
| SBP, mmHg | 136 (21) | 144 (30) | 0.041 |
| DBP, mmHg | 76 (10) | 76 (11) | 0.700 |
| CVD, n (%) | 40 (27.4%) | 11 (19.3%) | 0.230 |
| Type 2 diabetes, n (%) | 28 (19.2%) | 16 (28.1%) | 0.170 |
| Hypertension, n (%) | 45 (31.3%) | 20 (36.4%) | 0.490 |
| Total cholesterol, mmol/L | 5.23 (1.09) | 5.39 (0.96) | 0.340 |
| Triglycerides, mmol/L | 112.1 (88.4, 157.9) | 115.4 (92.1, 134.4) | 0.970 |
| Plasma NT-proBNP, ng/L | 192 (90, 548) | 112 (68, 237) | 0.0320 |
| β-hydroxybutyrate, µmol/L | 150.3 (113.8, 237.3) | 156.5 (111.3, 233.6) | 0.890 |
| Acetoacetate, µmol/L | 46.5 (29.1, 74.8) | 46.6 (29.8, 74.8) | 0.890 |
| Acetone, µmol/L | 24.2 (15.39, 35.2) | 24.39 (16.8, 38.1) | 0.440 |
| Total ketone bodies, µmol/L | 217.9 (164.6, 329.3) | 230.2 (157.8, 372.8) | 0.950 |
| eGFR, mL/min/1.73 m2 | 76.6 (20.3) | 74.8 (19.5) | 0.560 |
| UAE, mg/24h | 17.0 (8.0, 59.8) | 14.38 (9.1, 54.6) | 0.940 |
| ACEi use, n (%) | 36 (24.8%) | 12 (21.4%) | 0.610 |
| ARB use, n (%) | 17 (11.7%) | 7 (12.5%) | 0.880 |
| Betablocker use, n (%) | 46 (31.7%) | 22 (39.3%) | 0.310 |
| Statin use, n (%) | 42 (29.0%) | 11 (19.6%) | 0.180 |
| Diuretic use, n (%) | 19 (13.1%) | 11 (19.6%) | 0.240 |
| (A) All Participants | p | (B) Participants with HF | p | (C) Participants without HF | p | (D) Participants with HFrEF | p | (E) Participants with HFpEF | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.167 | <0.001 | 0.122 | 0.122 | 0.158 | <0.001 | 0.125 | 0.133 | 0.051 | 0.706 |
| Female sex | −0.004 | 0.758 | 0.061 | 0.385 | −0.001 | 0.923 | 0.086 | 0.304 | −0.014 | 0.920 |
| BMI | 0.074 | 0.012 | −0.019 | 0.788 | 0.071 | <0.001 | 0.076 | 0.365 | −0.263 | 0.048 |
| Waist circumference | 0.090 | <0.001 | −0.012 | 0.865 | 0.085 | <0.001 | 0.071 | 0.399 | −0.223 | 0.098 |
| Waist–hip ratio | 0.072 | <0.001 | −0.041 | 0.565 | 0.068 | <0.001 | 0.024 | 0.779 | −0.174 | 0.199 |
| SBP | 0.123 | <0.001 | 0.105 | 0.138 | 0.116 | <0.001 | 0.149 | 0.074 | −0.027 | 0.840 |
| DBP | 0.077 | <0.001 | 0.004 | 0.958 | 0.076 | <0.001 | 0.048 | 0.569 | 0.018 | 0.896 |
| CVD | 0.035 | 0.006 | 0.047 | 0.505 | 0.020 | 0.127 | −0.011 | 0.897 | 0.225 | 0.092 |
| Type 2 diabetes | 0.130 | <0.001 | 0.184 | 0.009 | 0.119 | <0.001 | 0.162 | 0.051 | 0.221 | 0.098 |
| Total cholesterol | −0.002 | 0.856 | −0.075 | 0.293 | 0.002 | 0.859 | −0.082 | 0.328 | −0.066 | 0.753 |
| Triglycerides | 0.047 | <0.001 | 0.163 | 0.020 | 0.041 | 0.001 | 0.211 | 0.011 | 0.045 | 0.736 |
| NT-proBNP | 0.133 | <0.001 | 0.185 | 0.008 | 0.116 | <0.001 | 0.195 | 0.019 | 0.182 | 0.173 |
| eGFR | −0.135 | <0.001 | −0.184 | 0.009 | −0.121 | <0.001 | −0.213 | 0.010 | −0.106 | 0.430 |
| UAE | 0.110 | <0.001 | 0.129 | 0.067 | 0.100 | <0.001 | 0.132 | 0.112 | 0.124 | 0.356 |
| ACEi use | 0.062 | <0.001 | −0.015 | 0.835 | 0.058 | <0.001 | −0.012 | 0.890 | −0.017 | 0.897 |
| ARB use | 0.033 | 0.011 | 0.058 | 0.415 | 0.021 | 0.107 | 0.109 | 0.192 | −0.064 | 0.640 |
| Beta-blocker use | 0.034 | 0.009 | −0.006 | 0.928 | 0.025 | 0.058 | −0.016 | 0.853 | 0.004 | 0.971 |
| Statin use | 0.063 | <0.001 | −0.012 | 0.869 | 0.059 | <0.001 | 0.016 | 0.849 | −0.074 | 0.589 |
| Diuretic use | 0.039 | 0.002 | −0.002 | 0.979 | 0.034 | 0.009 | 0.016 | 0.848 | −0.048 | 0.725 |
| Total Ketone Bodies | β-Hydroxybutyrate | Acetoacetate | Acetone | |||||
|---|---|---|---|---|---|---|---|---|
| Std β | p-Value | Std β | p-Value | Std β | p-Value | Std β | p-Value | |
| (A) All participants | ||||||||
| Crude | 0.13 | <0.001 | 0.16 | <0.001 | 0.07 | <0.001 | 0.01 | 0.318 |
| Model 1 | 0.08 | <0.001 | 0.09 | <0.001 | 0.05 | 0.002 | 0.01 | 0.357 |
| Model 2 | 0.08 | <0.001 | 0.09 | <0.001 | 0.05 | 0.002 | 0.01 | 0.683 |
| Model 3 | 0.08 | <0.001 | 0.09 | <0.001 | 0.05 | 0.002 | 0.01 | 0.637 |
| Model 4 | 0.08 | <0.001 | 0.09 | <0.001 | 0.05 | 0.002 | 0.01 | 0.611 |
| Model 5 | 0.08 | <0.001 | 0.09 | <0.001 | 0.05 | 0.002 | 0.01 | 0.627 |
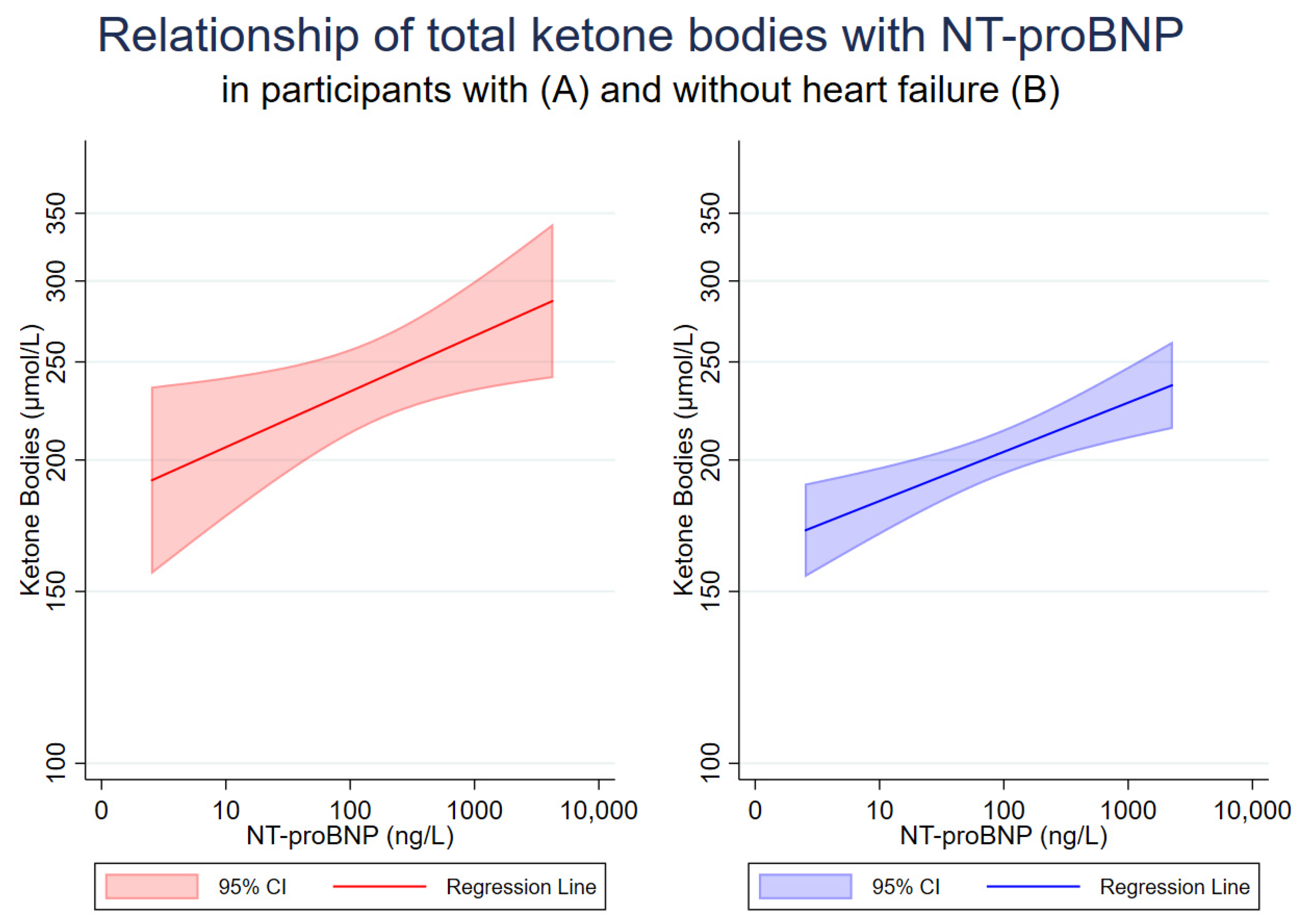
| (B) Participants with HF | ||||||||
| Crude | 0.19 | 0.008 | 0.20 | 0.005 | 0.12 | 0.098 | 0.17 | 0.019 |
| Model 1 | 0.17 | 0.024 | 0.19 | 0.014 | 0.09 | 0.224 | 0.15 | 0.042 |
| Model 2 | 0.15 | 0.060 | 0.17 | 0.036 | 0.08 | 0.365 | 0.16 | 0.062 |
| Model 3 | 0.15 | 0.078 | 0.16 | 0.047 | 0.06 | 0.436 | 0.15 | 0.076 |
| Model 4 | 0.16 | 0.052 | 0.18 | 0.030 | 0.08 | 0.378 | 0.16 | 0.056 |
| Model 5 | 0.16 | 0.049 | 0.18 | 0.030 | 0.08 | 0.357 | 0.17 | 0.047 |
| (C) Participants without HF | ||||||||
| Crude | 0.12 | <0.001 | 0.15 | <0.001 | 0.06 | <0.001 | −0.01 | 0.502 |
| Model 1 | 0.07 | <0.001 | 0.09 | <0.001 | 0.04 | 0.014 | −0.01 | 0.930 |
| Model 2 | 0.07 | <0.001 | 0.08 | <0.001 | 0.04 | 0.008 | −0.01 | 0.691 |
| Model 3 | 0.07 | <0.001 | 0.08 | <0.001 | 0.04 | 0.007 | −0.01 | 0.750 |
| Model 4 | 0.07 | <0.001 | 0.08 | <0.001 | 0.04 | 0.006 | −0.01 | 0.793 |
| Model 5 | 0.07 | <0.001 | 0.08 | <0.001 | 0.04 | 0.006 | −0.01 | 0.765 |
| (D) Participants with HFrEF | ||||||||
| Crude | 0.19 | 0.019 | 0.21 | 0.011 | 0.10 | 0.249 | 0.19 | 0.020 |
| Model 1 | 0.16 | 0.068 | 0.18 | 0.043 | 0.05 | 0.569 | 0.18 | 0.050 |
| Model 2 | 0.17 | 0.086 | 0.19 | 0.049 | 0.05 | 0.610 | 0.18 | 0.069 |
| Model 3 | 0.18 | 0.063 | 0.21 | 0.032 | 0.06 | 0.585 | 0.19 | 0.057 |
| Model 4 | 0.19 | 0.052 | 0.22 | 0.025 | 0.06 | 0.557 | 0.19 | 0.061 |
| Model 5 | 0.18 | 0.060 | 0.21 | 0.032 | 0.06 | 0.542 | 0.19 | 0.066 |
| (E) Participants with HFpEF | ||||||||
| Crude | 0.18 | 0.173 | 0.18 | 0.170 | 0.18 | 0.192 | 0.11 | 0.412 |
| Model 1 | 0.19 | 0.195 | 0.20 | 0.168 | 0.17 | 0.244 | 0.11 | 0.478 |
| Model 2 | 0.07 | 0.725 | 0.08 | 0.660 | 0.06 | 0.774 | 0.03 | 0.861 |
| Model 3 | 0.12 | 0.513 | 0.13 | 0.462 | 0.09 | 0.619 | 0.08 | 0.680 |
| Model 4 | 0.12 | 0.530 | 0.13 | 0.473 | 0.10 | 0.615 | 0.06 | 0.752 |
| Model 5 | 0.05 | 0.802 | 0.06 | 0.746 | 0.03 | 0.882 | 0.06 | 0.779 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palm, C.L.; Shalaurova, I.; Connelly, M.A.; Bakker, S.J.L.; Westenbrink, B.D.; Dullaart, R.P.F. Fasting Plasma Ketone Bodies Are Associated with NT-proBNP: A Potential Mechanism to Provide Fuel for the Failing Heart. J. Clin. Med. 2024, 13, 1541. https://doi.org/10.3390/jcm13061541
Palm CL, Shalaurova I, Connelly MA, Bakker SJL, Westenbrink BD, Dullaart RPF. Fasting Plasma Ketone Bodies Are Associated with NT-proBNP: A Potential Mechanism to Provide Fuel for the Failing Heart. Journal of Clinical Medicine. 2024; 13(6):1541. https://doi.org/10.3390/jcm13061541
Chicago/Turabian StylePalm, Constantin L., Irina Shalaurova, Margery A. Connelly, Stephan J. L. Bakker, Berend Daan Westenbrink, and Robin P. F. Dullaart. 2024. "Fasting Plasma Ketone Bodies Are Associated with NT-proBNP: A Potential Mechanism to Provide Fuel for the Failing Heart" Journal of Clinical Medicine 13, no. 6: 1541. https://doi.org/10.3390/jcm13061541
APA StylePalm, C. L., Shalaurova, I., Connelly, M. A., Bakker, S. J. L., Westenbrink, B. D., & Dullaart, R. P. F. (2024). Fasting Plasma Ketone Bodies Are Associated with NT-proBNP: A Potential Mechanism to Provide Fuel for the Failing Heart. Journal of Clinical Medicine, 13(6), 1541. https://doi.org/10.3390/jcm13061541