

Tricuspid Regurgitation and TAVR: Outcomes, Risk Factors and Biomarkers

 , , , , ,
, , , , ,  , and
, and
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Patient Cohort and Evaluation of TR
2.3. Endpoints
2.4. Statistical Analysis
3. Results
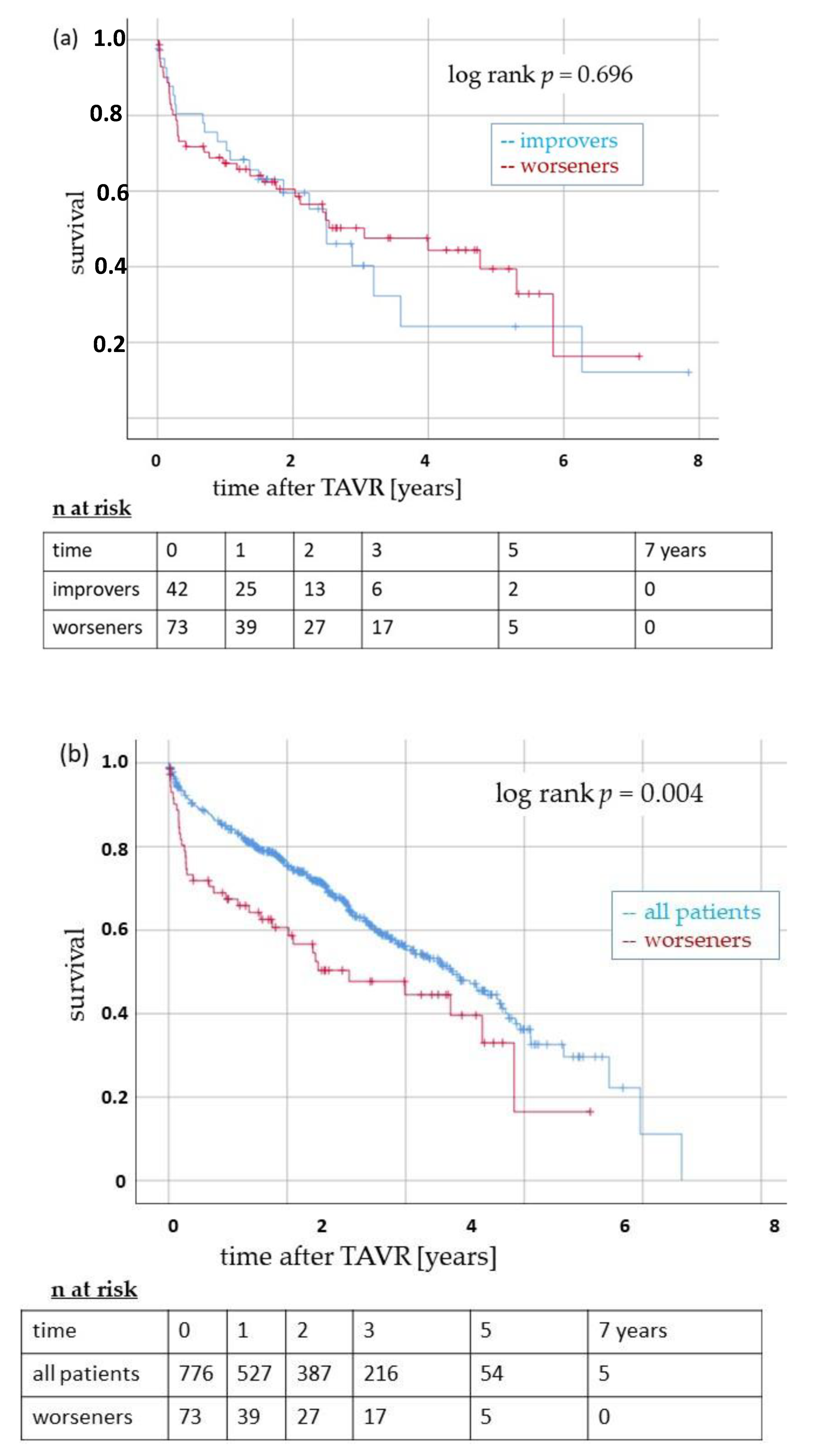
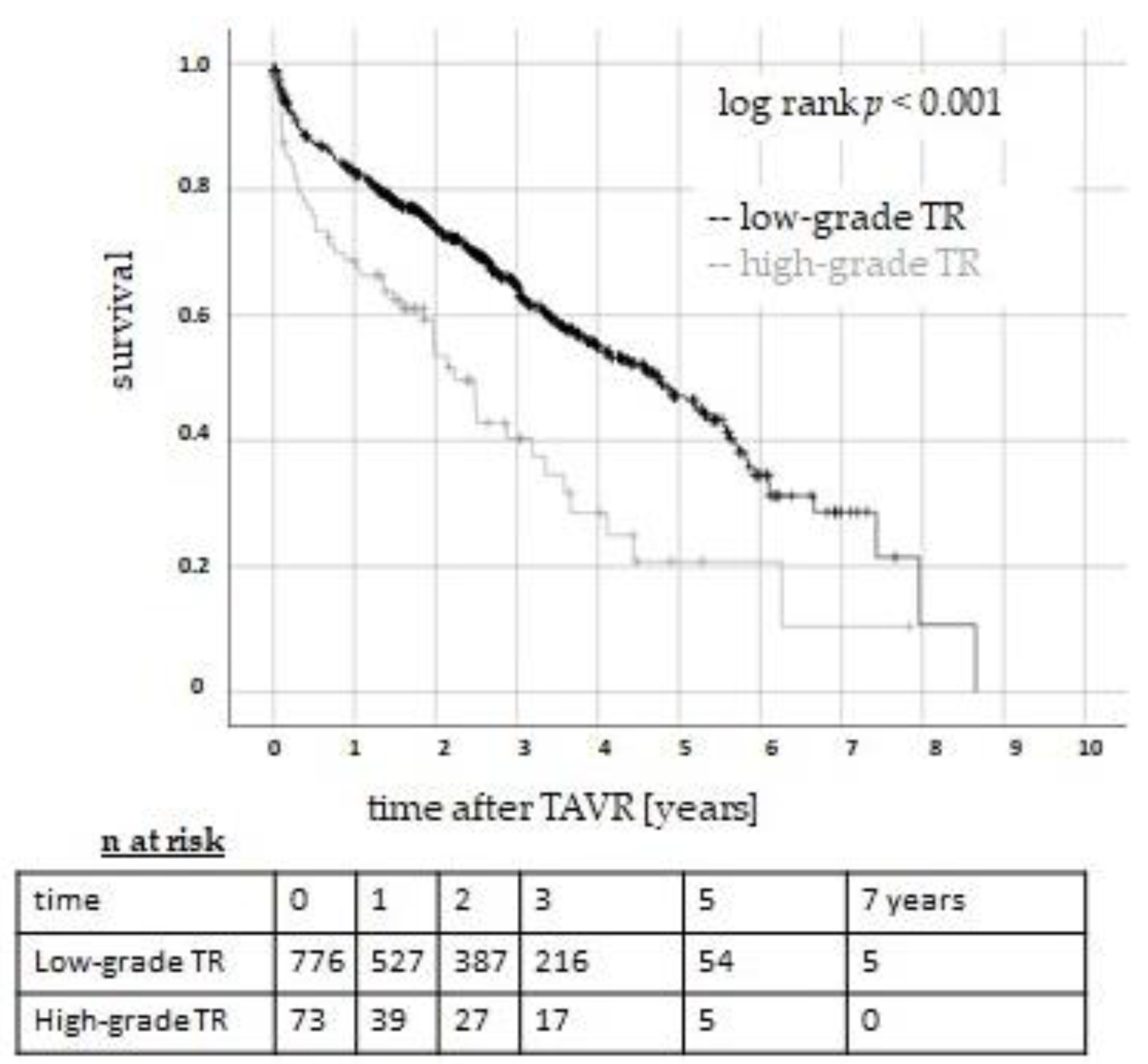
3.1. Survival after TAVR as a Function of Pre-Interventional TR
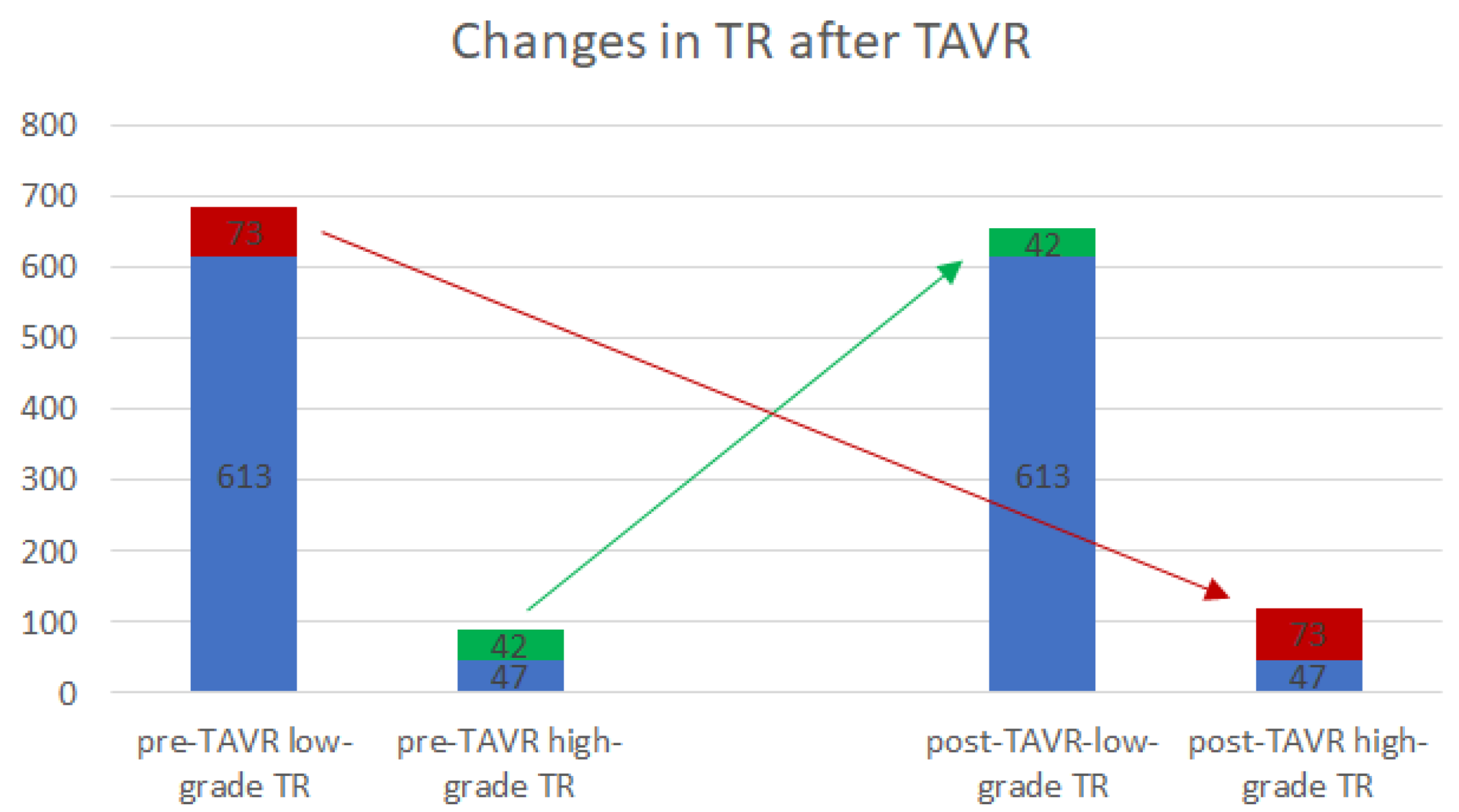
3.2. TR Changes after TAVR
4. Discussion
Limitations of the Study
5. Conclusions and Impact on Daily Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AS | Aortic valve stenosis |
| ES | EuroScore |
| ESC | European Society of Cardiology |
| Hs-TNT | high-sensitivity troponin T |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| STS-Score | Society of Thoracic Surgeons Score |
| TAVR | Transcatheter aortic valve replacement |
| TR | Tricuspid Regurgitation |
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 43, ehab395. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Okuno, T.; Malebranche, D.; Lanz, J.; Praz, F.; Stortecky, S.; Windecker, S.; Pilgrim, T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc. Interv. 2020, 13, 1503–1514. [Google Scholar] [CrossRef] [PubMed]
- D’Arcy, J.L.; Coffey, S.; Loudon, M.A.; Kennedy, A.; Pearson-Stuttard, J.; Birks, J.; Frangou, E.; Farmer, A.J.; Mant, D.; Wilson, J. Large-Scale Community Echocardiographic Screening Reveals a Major Burden of Undiagnosed Valvular Heart Disease in Older People: The OxVALVE Population Cohort Study. Eur. Heart J. 2016, 37, 3515–3522. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, M.; Binder, R.K.; Dvir, D.; Tan, J.; Freeman, M.; Thompson, C.R.; Cheung, A.; Wood, D.A.; Leipsic, J.; Webb, J.G. Prevalence and impact of preoperative moderate/severe tricuspid regurgitation on patients undergoing transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 2015, 85, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Tomii, D.; Okuno, T.; Praz, F.; Heg, D.; Wild, M.G.; Lanz, J.; Stortecky, S.; Reineke, D.; Windecker, S.; Pilgrim, T. Potential Candidates for Transcatheter Tricuspid Valve Intervention After Transcatheter Aortic Valve Replacement: Predictors and Prognosis. JACC Cardiovasc. Interv. 2021, 14, 2246–2256. [Google Scholar] [CrossRef] [PubMed]
- Shamekhi, J.; Sugiura, A.; Tabata, N.; Al-Kassou, B.; Weber, M.; Sedaghat, A.; Werner, N.; Grube, E.; Nickenig, G.; Sinning, J.-M. Impact of Tricuspid Regurgitation in Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 1135–1137. [Google Scholar] [CrossRef] [PubMed]
- Hutter, A.; Bleiziffer, S.; Richter, V.; Opitz, A.; Hettich, I.; Mazzitelli, D.; Ruge, H.; Lange, R. Transcatheter Aortic Valve Implantation in Patients with Concomitant Mitral and Tricuspid Regurgitation. Ann. Thorac. Surg. 2013, 95, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; Blackstone, E.H.; et al. Valve Academic Research Consortium 3: Updated Endpoint Definitions for Aortic Valve Clinical Research. J. Am. Coll. Cardiol. 2021, 77, 2717–2746. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.A.; Rozenbaum, Z.; Ghantous, E.; Kramarz, J.; Biner, S.; Ghermezi, M.; Shimiaie, J.; Finkelstein, A.; Banai, S.; Aviram, G.; et al. Impact of Right Ventricular Dysfunction and Tricuspid Regurgitation on Outcomes in Patients Undergoing Transcatheter Aortic Valve Replacement. J. Am. Soc. Echocardiogr. 2017, 30, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Wilbring, M.; Tugtekin, S.-M.; Ritzmann, M.; Arzt, S.; Schmidt, T.; Matschke, K.; Kappert, U.; Alexiou, K. Transcatheter aortic valve implantation reduces grade of concomitant mitral and tricuspid valve regurgitation and pulmonary hypertension. Eur. J. Cardiothorac Surg. 2014, 46, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Sathananthan, J.; Murdoch, D.J.; Lindman, B.R.; Zajarias, A.; Jaber, W.A.; Cremer, P.; Wood, D.; Moss, R.; Cheung, A.; Ye, J.; et al. Implications of Concomitant Tricuspid Regurgitation in Patients Undergoing Transcatheter Aortic Valve Replacement for Degenerated Surgical Aortic Bioprosthesis: Insights From the PARTNER 2 Aortic Valve-in-Valve Registry. JACC Cardiovasc. Interv. 2018, 11, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, J.; Ikenaga, H.; Hayashi, A.; Yamaguchi, S.; Nagaura, T.; Rader, F.; Siegel, R.J.; Makkar, R.R.; Shiota, T. Predictors and Outcomes of Persistent Tricuspid Regurgitation After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2019, 124, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Seoudy, H.; Lambers, M.; Winkler, V.; Dudlik, L.; Freitag-Wolf, S.; Frank, J.; Kuhn, C.; Rangrez, A.Y.; Puehler, T.; Lutter, G.; et al. Elevated high-sensitivity troponin T levels at 1-year follow-up are associated with increased long-term mortality after TAVR. Clin. Res. Cardiol. 2021, 110, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Mas-Peiro, S.; Berkowitsch, A.; Boeckling, F.; Rasper, T.; Pieszko, K.; De Rosa, R.; Hiczkiewicz, J.; Burchardt, P.; Fichtlscherer, S.; et al. Inflammatory signatures are associated with increased mortality after transfemoral transcatheter aortic valve implantation. ESC Heart Fail. 2020, 7, 2597–2610. [Google Scholar] [CrossRef] [PubMed]
- Hahn, R.T.; Badano, L.P.; Bartko, P.E.; Muraru, D.; Maisano, F.; Zamorano, J.L.; Donal, E. Tricuspid regurgitation: Recent advances in understanding pathophysiology, severity grading and outcome. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 913–929. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 (Low-Grade TR) (n = 686) | Group 2 (High-Grade TR) (n = 89) | p-Value | |
|---|---|---|---|
| Age (years) | 81.3 ± 6.0 | 81.7 ± 6.4 | 0.431 |
| Gender, male (%) | 45.5 (n = 312) | 38.2 (n = 34) | 0.194 |
| BMI, median (kg/m2) | 26.0 (23.5–29.4) | 25.7 (22.9–29.1) | 0.268 |
| Chronic-obstructive pulmonary-disease (%) | 16.6 (n = 114) | 16.9 (n = 15) | 0.955 |
| Diabetes (%) | 32.1 (n = 220) | 27.0 (n = 24) | 0.330 |
| Dyslipidemia (%) | 53.2 (n = 365) | 51.7 (n = 46) | 0.787 |
| Cerebrovascular disease (%) | 19.9 (n = 136) | 16.9 (n = 15) | 0.506 |
| chronic atrial fibrillation (%) | 40.2 (n = 276) | 77.5 (n = 69) | 0.001 |
| Previous surgery (%) | 18.9 (n = 130) | 14.6 (n = 13) | 0.264 |
| Hypertension (%) | 91.0 (n = 624) | 91.0 (n = 81) | 0.988 |
| pAVD (%) | 17.8 (n = 122) | 11.2 (n = 10) | 0.122 |
| NYHA functional class (%) | (n = 681) | (n = 89) | 0.003 |
| I | 4.1 (n = 28) | 1.1 (n = 1) | |
| II | 24.9 (n = 171) | 14.6 (n = 13) | |
| III | 56.6 (n = 388) | 62.9 (n = 56) | |
| IV | 13.8 (n = 95) | 21.3 (n = 19) | |
| Risk-scores | (n = 686) | (n = 89) | |
| Median STS-Score (%) | 4.6 (2.9–7.0) | 5.1 (3.8–7.9) | 0.025 |
| ≤10% | 89.5 (n = 613) | 87.5 (n = 78) | |
| >10% | 10.5 (n = 72) | 12.5 (n = 11) | |
| Median EuroScore II | 4.7 (3.0–7.8) | 6.5 (4.0–9.7) | 0.001 |
| ≤10.3% | 84.2 (n = 577) | 80.9 (n = 72) | |
| >10.3% | 15.8 (n = 108) | 19.1 (n = 17) | |
| EF (%) | (n = 636) | (n = 87) | 0.003 |
| <35% | 8.6 (n = 59) | 10.1 (n = 9) | |
| 35–45% | 13.3 (n = 91) | 16.9 (n = 15) | |
| 46–54% | 17.2 (n = 118) | 34.8 (n = 31) | |
| ≥55% | 53.6 (n = 368) | 36.0 (n = 32) | |
| RA dilatation (%) | (n = 628) 20.1 (n = 130) | (n = 85) 48.2 (n = 41) | 0.001 |
| RV dilatation (%) | (n = 627) 14.5 (n = 91) | (n = 85) 41.2 (n = 35) | 0.001 |
| TAPSE < 17 mm (%) | (n = 613) 18.8 (n = 115) | (n = 85) 45.9 (n = 39) | 0.001 |
| PAPsys > 45 mmHg (%) | (n = 570) 26.5 (n = 151) | (n = 80) 53.8 (n = 43) | 0.001 |
| GFR (%) | (n = 682) | (n = 89) | 0.313 |
| <30 mL/min | 12.1 (n = 83) | 14.6 (n = 13) | |
| 30–45 mL/min | 21.6 (n = 148) | 24.7 (n = 22) | |
| 45–60 mL/min | 35.4 (n = 243) | 33.7 (n = 30) | |
| >60 mL/min | 30.3 (n = 208) | 27.0 (n = 24) | |
| (n = 684) | (n = 89) | ||
| Median Creatinine (mg/dL) | 101.6 (79.7–130.1) | 104.4 (82.2–133.5) | 0.409 |
| TAVR-access site (%) | 0.877 | ||
| Transfemoral (%) | 67.2 (n = 460) | 65.9 (n = 59) | |
| Transaortal (%) | 20.0 (n = 137) | 21.6 (n = 19) | |
| Transapical (%) | 12.8 (n = 89) | 12.5 (n = 11) |
| Low-Grade TR (n = 686) | High-Grade TR (n = 89) | p-Value | |
|---|---|---|---|
| 30-day all-cause mortality (%) | 19.1 (n = 131) | 28.1 (n = 25) | 0.04 |
| Myocardial infarction (%) | 1.2 (n = 8) | 0 (n = 0) | 0.31 |
| Stroke (%) | 3.1 (n = 21) | 6.7 (n = 6) | 0.49 |
| Bleeding (%) | 12.1 (n = 83) | 20.2 (n = 18) | 0.03 |
| Acute kidney injury (%) | 6.6 (n = 45) | 16.9 (n = 5) | 0.96 |
| Complications vascular access site (%) | 10.1 (n = 69) | 11.2 (n = 10) | 0.43 |
| New pacemaker implantation (%) | 7.2 (n = 50) | 5.3 (n = 6) | 0.53 |
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age (years) | 1.058 | 1.022–1.096 | 0.002 |
| Atrial fibrillation | 1.787 | 1.210–2.641 | 0.004 |
| Pre-interventional creatinine | 1.003 | 1.000–1.005 | 0.002 |
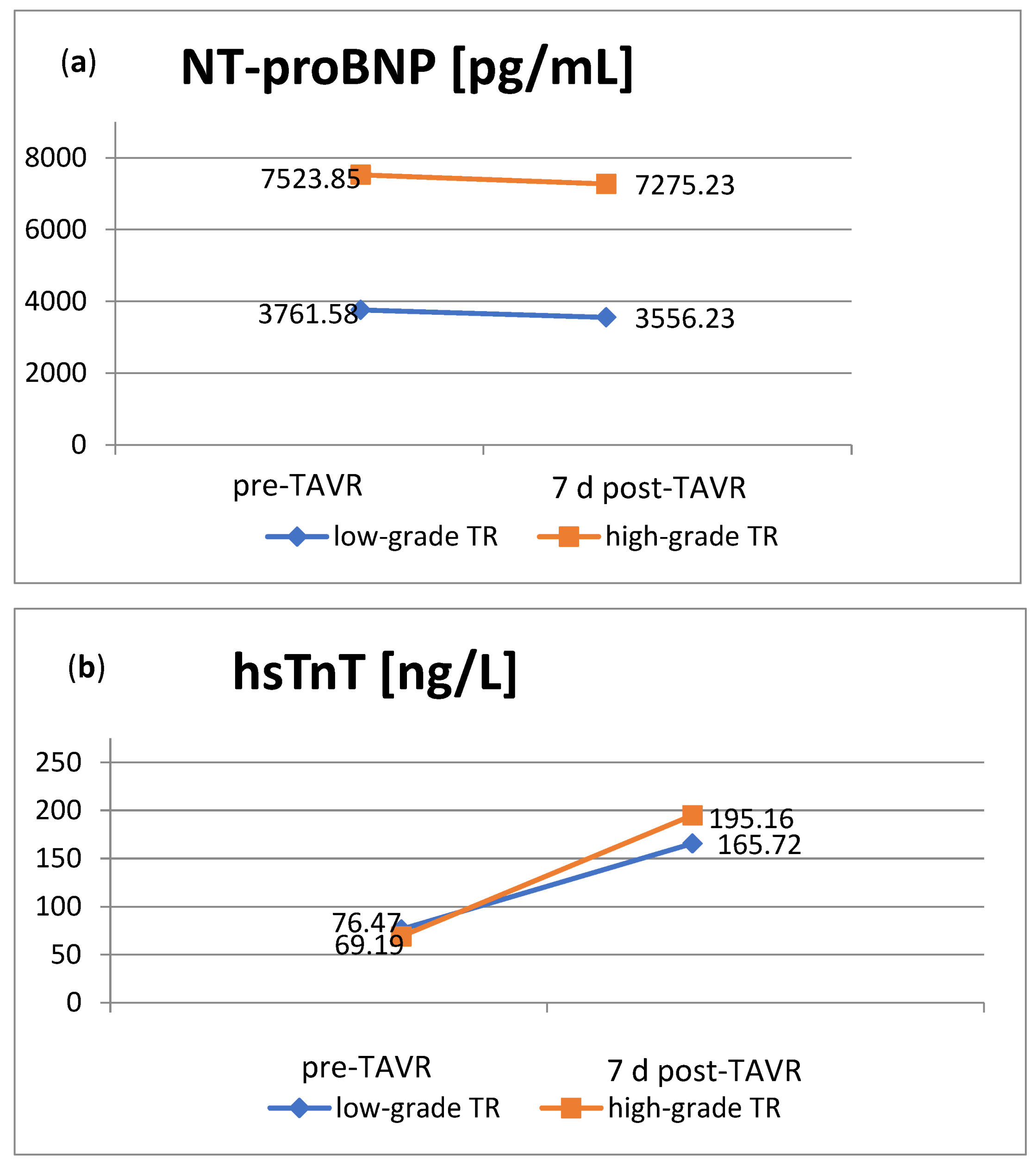
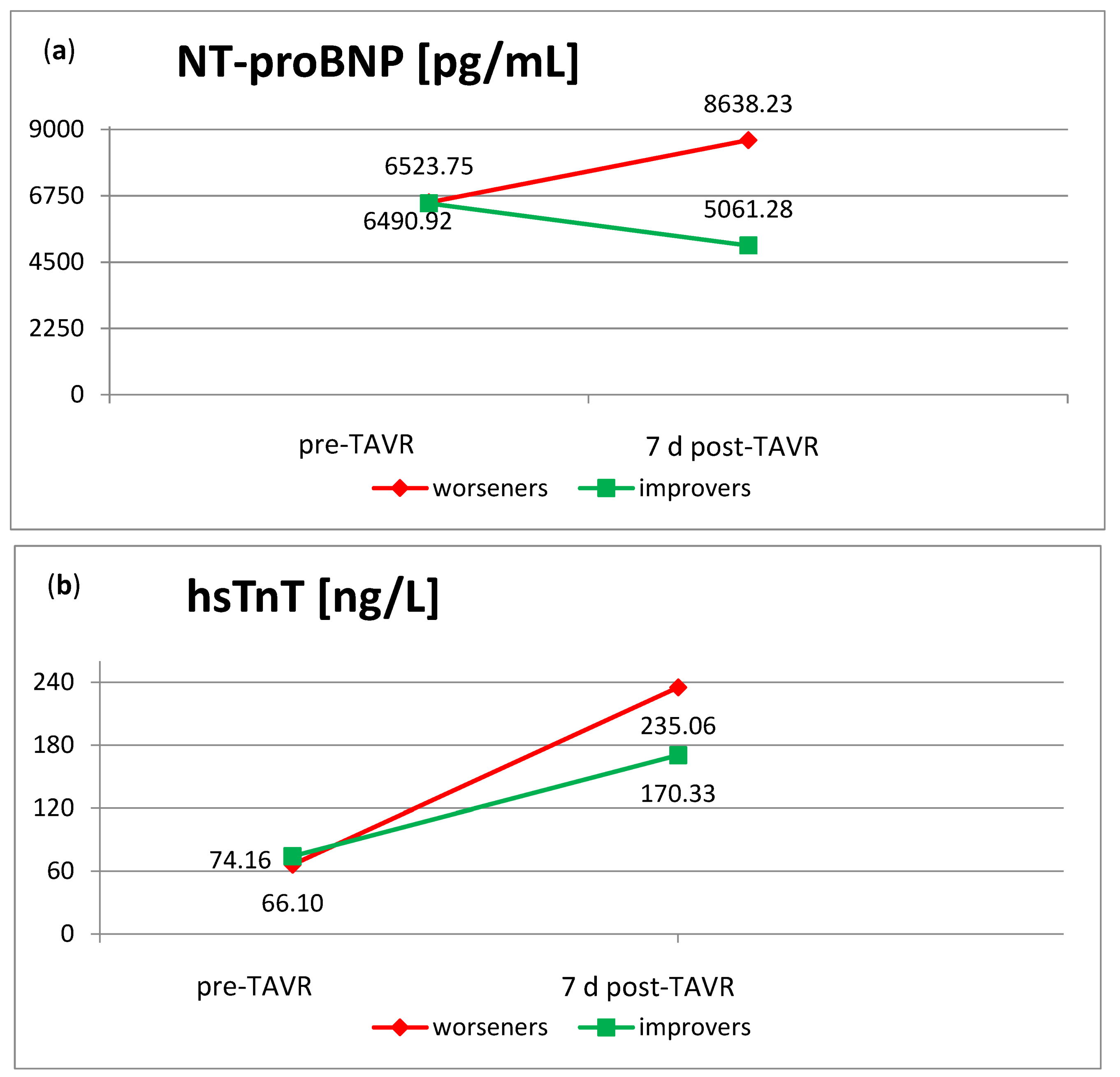
| Pre-interventional hsTNT | 1.368 | 1.122–1.670 | 0.002 |
| Arterial hypertension | 3.245 | 1.190–8.846 | 0.021 |
| COPD | 2.189 | 1.391–3.446 | 0.001 |
| Pre-interventional NT-proBNP | 1.429 | 1.236–2.451 | 0.001 |
| TR Worseners (n = 73) | p-Value (Worseners vs. Low-Grade TR n = 686) | p-Value (Worseners vs. All Patients n = 775) | TR Improvers (n = 42) | p-Value (Improvers vs. High-Grade TR n = 89) | p-Value (Improvers vs. All Patients n = 775) | |
|---|---|---|---|---|---|---|
| 30-day all-cause mortality (%) | 31.5 (n = 23) | 0.014 | 0.022 | 26.2 (n = 11) | 0.591 | 0.191 |
| Myocardial infarction (%) | 1.4 (n = 1) | 0.44 | 0.405 | 0 (n = 0) | 0.500 | 0.998 |
| Stroke (%) | 1.4 (n = 1) | 0.868 | 0.919 | 4.8 (n = 2) | 0.680 | 0.351 |
| Bleeding (%) | 12.3 (n = 9) | 0.477 | 0.569 | 11.9 (n = 5) | 0.098 | 0.587 |
| Acute kidney injury (%) | 9.6 (n = 7) | 0.198 | 0.189 | 0 (n = 0) | 0.989 | 1.000 |
| Complications vascular access site (%) | 8.2 (n = 6) | 0.705 | 0.720 | 7.1 (n = 3) | 0.785 | 0.771 |
| New pacemaker implantation (%) | 2.7 (n = 2) | 0.983 | 0.982 | 9.5 (n = 4) | 0.680 | 0.310 |
| Worseners | All Patients | p-Value (Worseners Compared to All Patients) | Low-Grade TR | p-Value (Worseners Compared to Low-Grade TR) | |
|---|---|---|---|---|---|
| RA dilatation (%) | 55.1 (38/69) | 23.9 (171/714) | 0.001 | 20.1 (130/628) | 0.001 |
| RV dilatation (%) | 42.0 (29/69) | 17.7 (126/713) | 0.001 | 14.5 (91/627) | 0.001 |
| PAPsys > 45 mmHg (%) | 60.3 (41/68) | 29.8 (194/651) | 0.001 | 18.8 (115/613) | 0.001 |
| TAPSE < 17 mm (%) | 47.6 (30/63) | 22.0 (154/699) | 0.001 | 26.5 (151/570) | 0.001 |
| improvers | all patients | p-value (improvers compared to all patients) | high-grade TR | p-value (improvers compared to high-grade TR) | |
| RA dilatation (%) | 36.6 (15/41) | 23.9 (171/714) | 0.05 | 48.2 (41/85) | 0.900 |
| RV dilatation (%) | 34.1 (14/41) | 17.7 (126/713) | 0.02 | 41.2 (35/85) | 0.779 |
| PAPsys > 45 mmHg (%) | 33.3 (13/39) | 29.8 (194/651) | 0.324 | 45.9 (39/85) | 0.911 |
| TAPSE < 17 mm (%) | 30.0 (12/40) | 22.0 (154/699) | 0.142 | 53.8 (43/80) | 0.995 |
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Body mass index | 1.128 | 1.041–1.223 | 0.003 |
| TAPSE < 17 mm | 4.371 | 2.4022–16.7988 | 0.006 |
| Pre-interventional TR | 1.330 | 1.041–1.622 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puehler, T.; Pommert, N.S.; Freitag-Wolf, S.; Seoudy, H.; Ernst, M.; Haneya, A.; Sathananthan, J.; Sellers, S.L.; Meier, D.; Schöttler, J.; et al. Tricuspid Regurgitation and TAVR: Outcomes, Risk Factors and Biomarkers. J. Clin. Med. 2024, 13, 1474. https://doi.org/10.3390/jcm13051474
Puehler T, Pommert NS, Freitag-Wolf S, Seoudy H, Ernst M, Haneya A, Sathananthan J, Sellers SL, Meier D, Schöttler J, et al. Tricuspid Regurgitation and TAVR: Outcomes, Risk Factors and Biomarkers. Journal of Clinical Medicine. 2024; 13(5):1474. https://doi.org/10.3390/jcm13051474
Chicago/Turabian StylePuehler, Thomas, Nina Sophie Pommert, Sandra Freitag-Wolf, Hatim Seoudy, Markus Ernst, Assad Haneya, Janarthanan Sathananthan, Stephanie L. Sellers, David Meier, Jan Schöttler, and et al. 2024. "Tricuspid Regurgitation and TAVR: Outcomes, Risk Factors and Biomarkers" Journal of Clinical Medicine 13, no. 5: 1474. https://doi.org/10.3390/jcm13051474
APA StylePuehler, T., Pommert, N. S., Freitag-Wolf, S., Seoudy, H., Ernst, M., Haneya, A., Sathananthan, J., Sellers, S. L., Meier, D., Schöttler, J., Müller, O. J., Salehi Ravesh, M., Saad, M., Frank, D., & Lutter, G. (2024). Tricuspid Regurgitation and TAVR: Outcomes, Risk Factors and Biomarkers. Journal of Clinical Medicine, 13(5), 1474. https://doi.org/10.3390/jcm13051474