
The Role of Anxiety and Depression in Shaping the Sleep–Pain Connection in Patients with Nonspecific Chronic Spinal Pain and Comorbid Insomnia: A Cross-Sectional Analysis

 , , , , , ,
, , , , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sociodemographic Information
2.3. Questionnaires
2.4. Statistical Analysis
3. Results
3.1. Descriptives
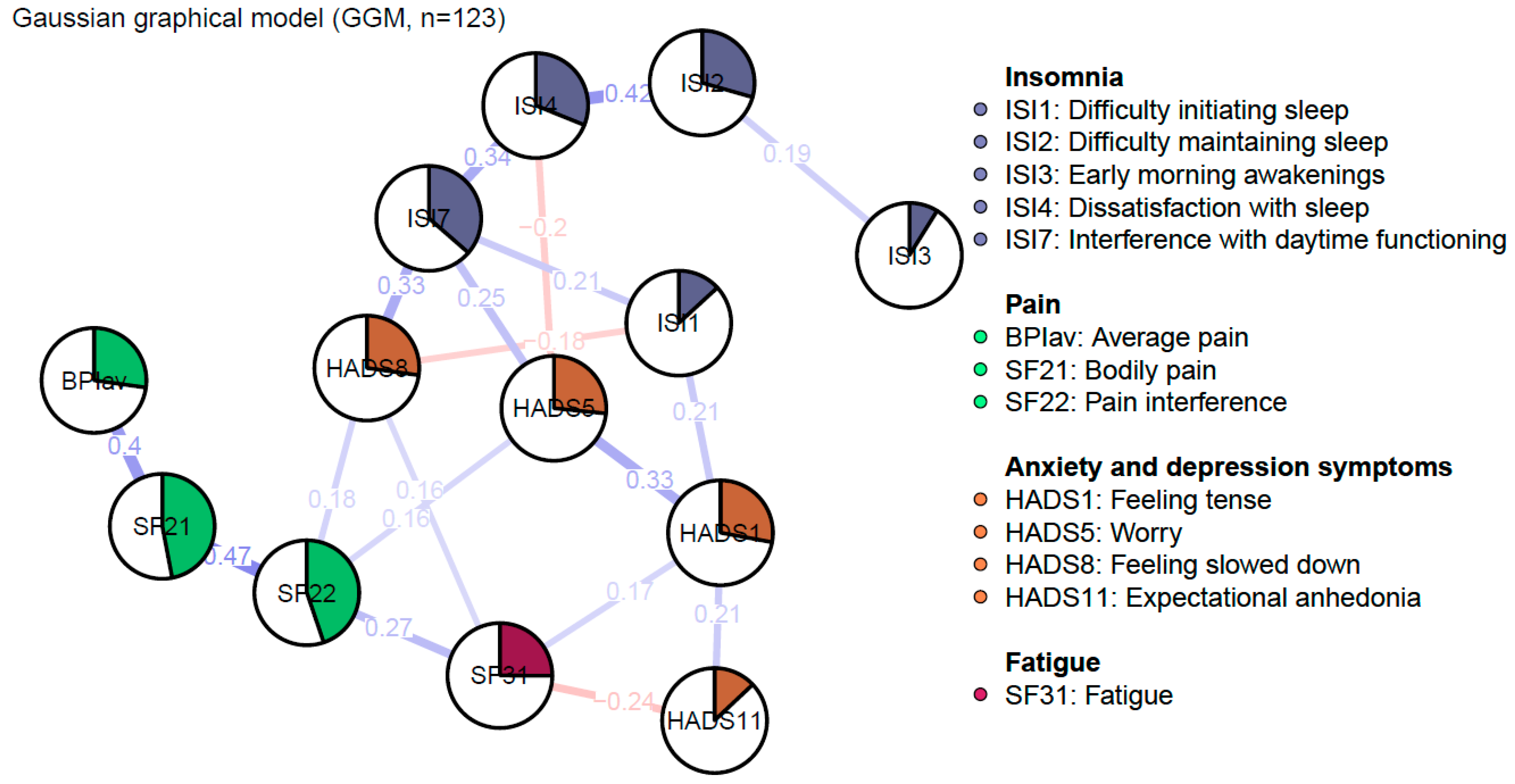
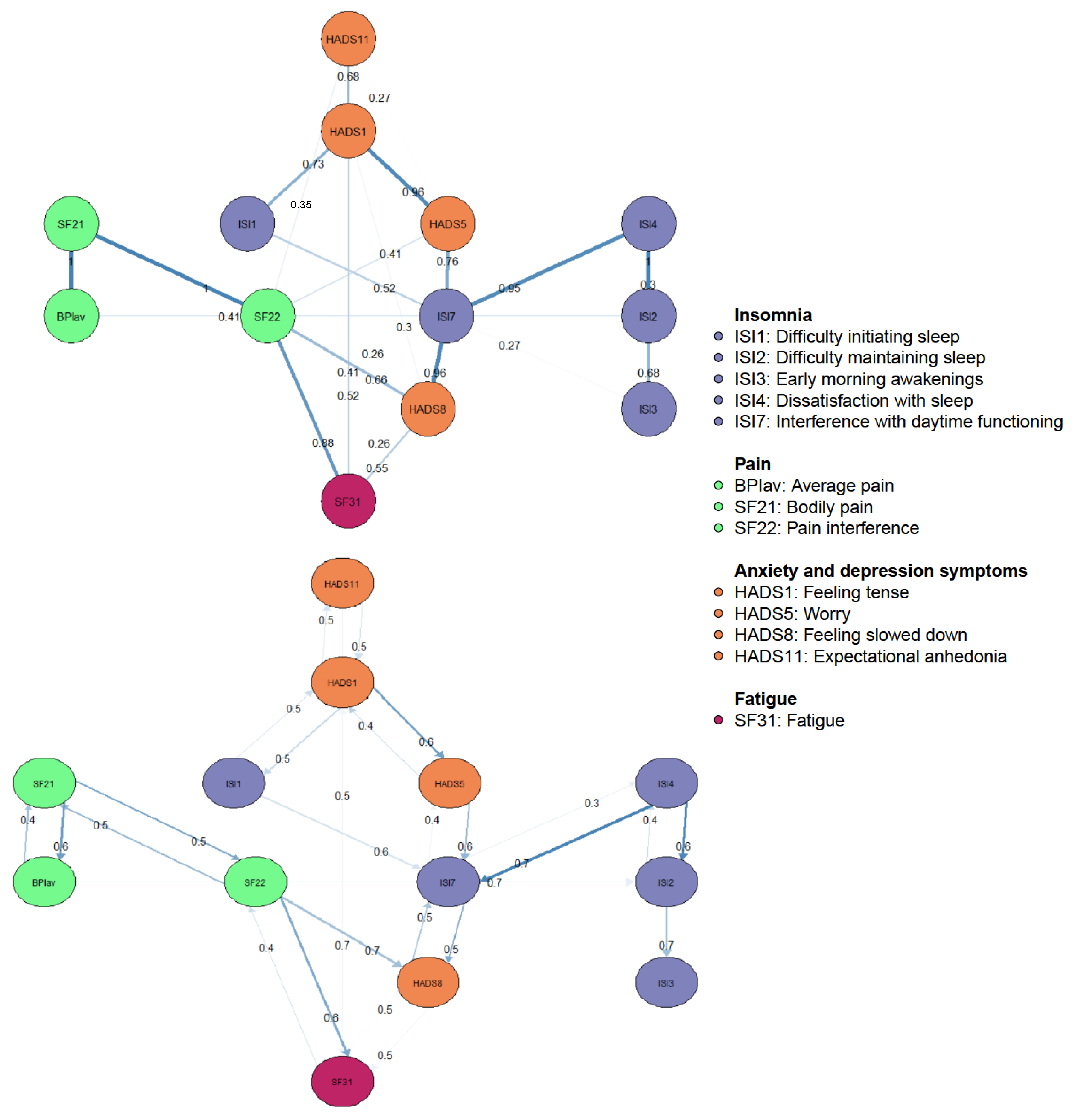
3.2. Regularized Gaussian Graphical Model
3.2.1. Description
3.2.2. Stability
3.2.3. Predictability
3.2.4. Edges
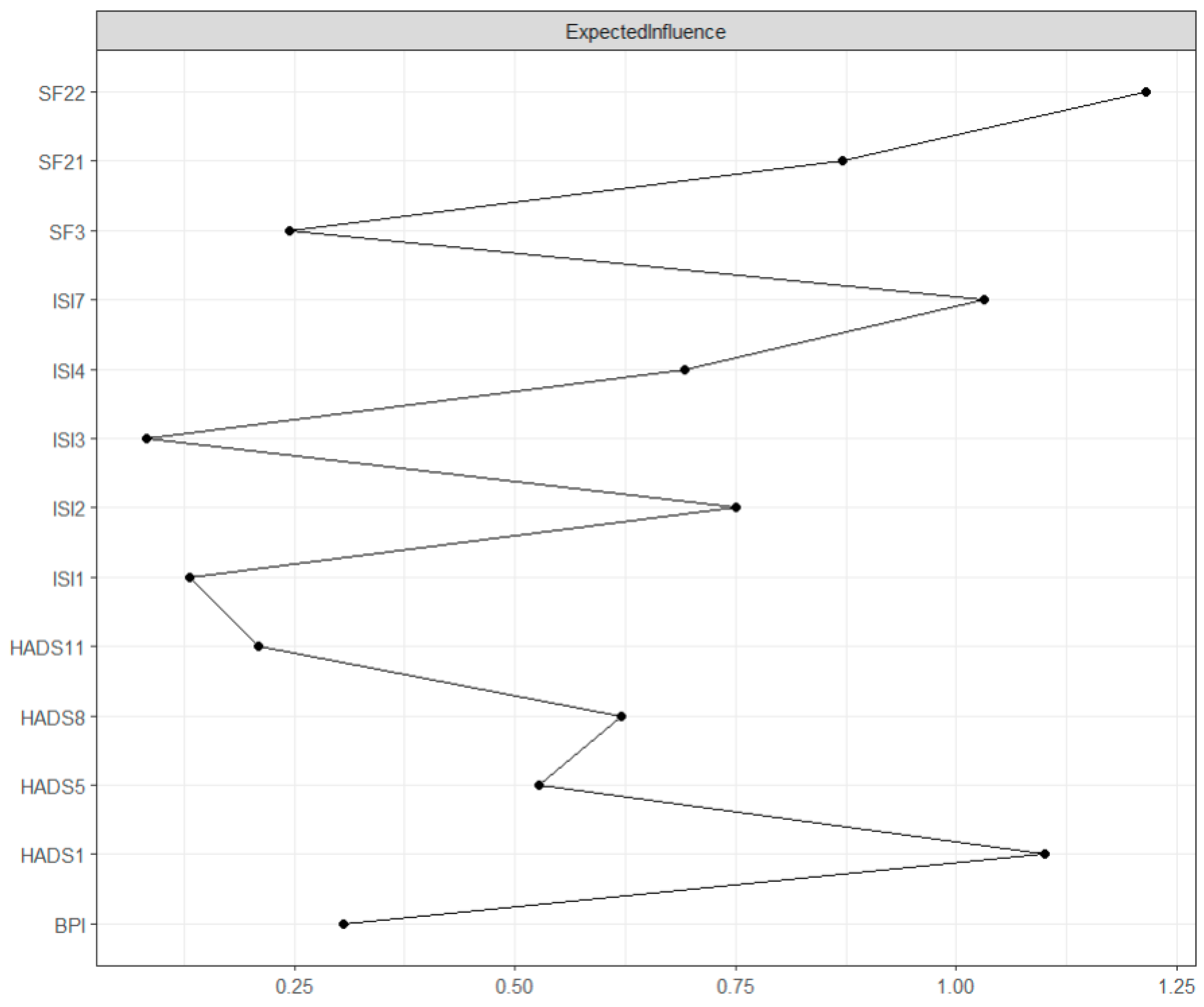
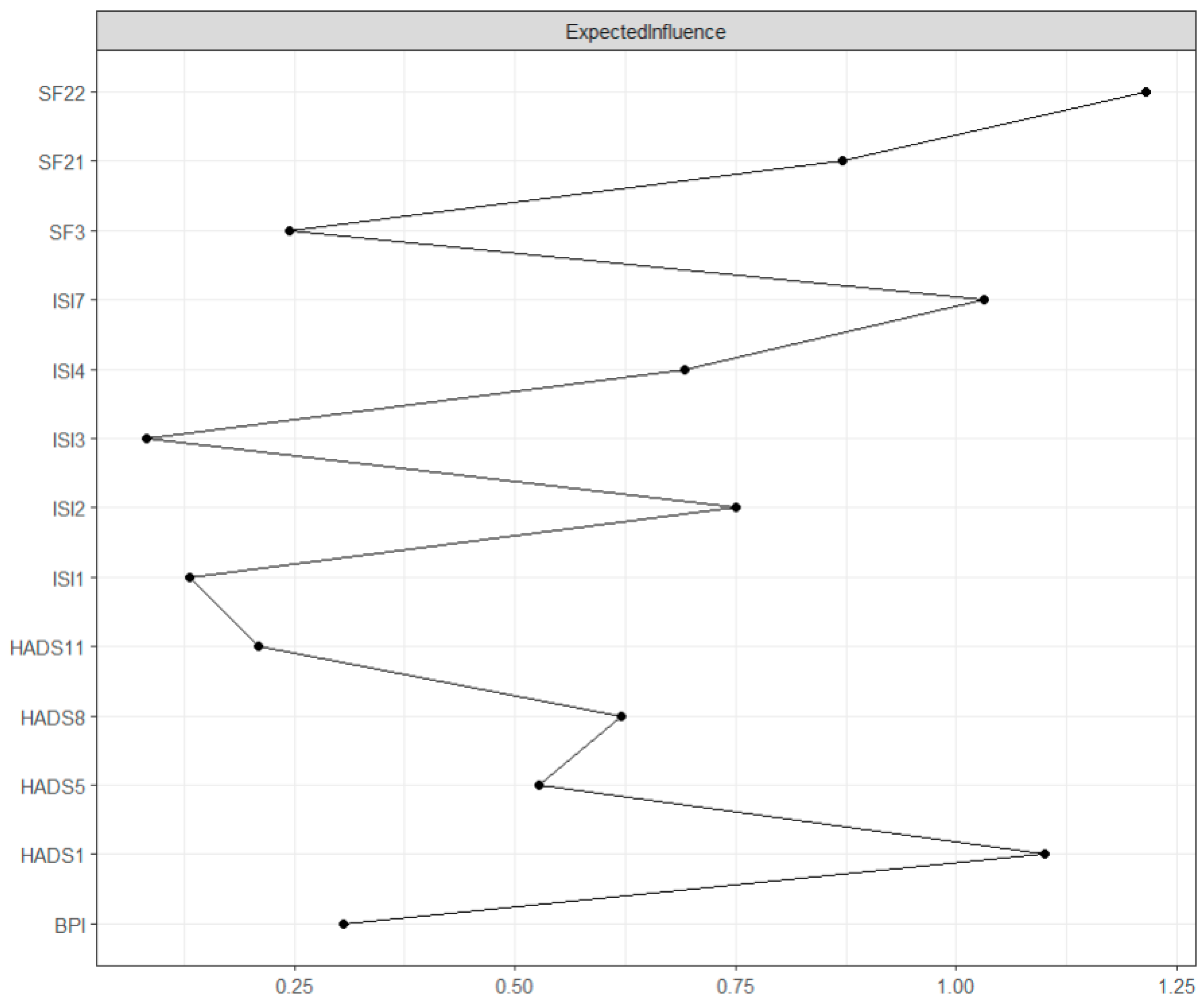
3.2.5. Centrality Measures
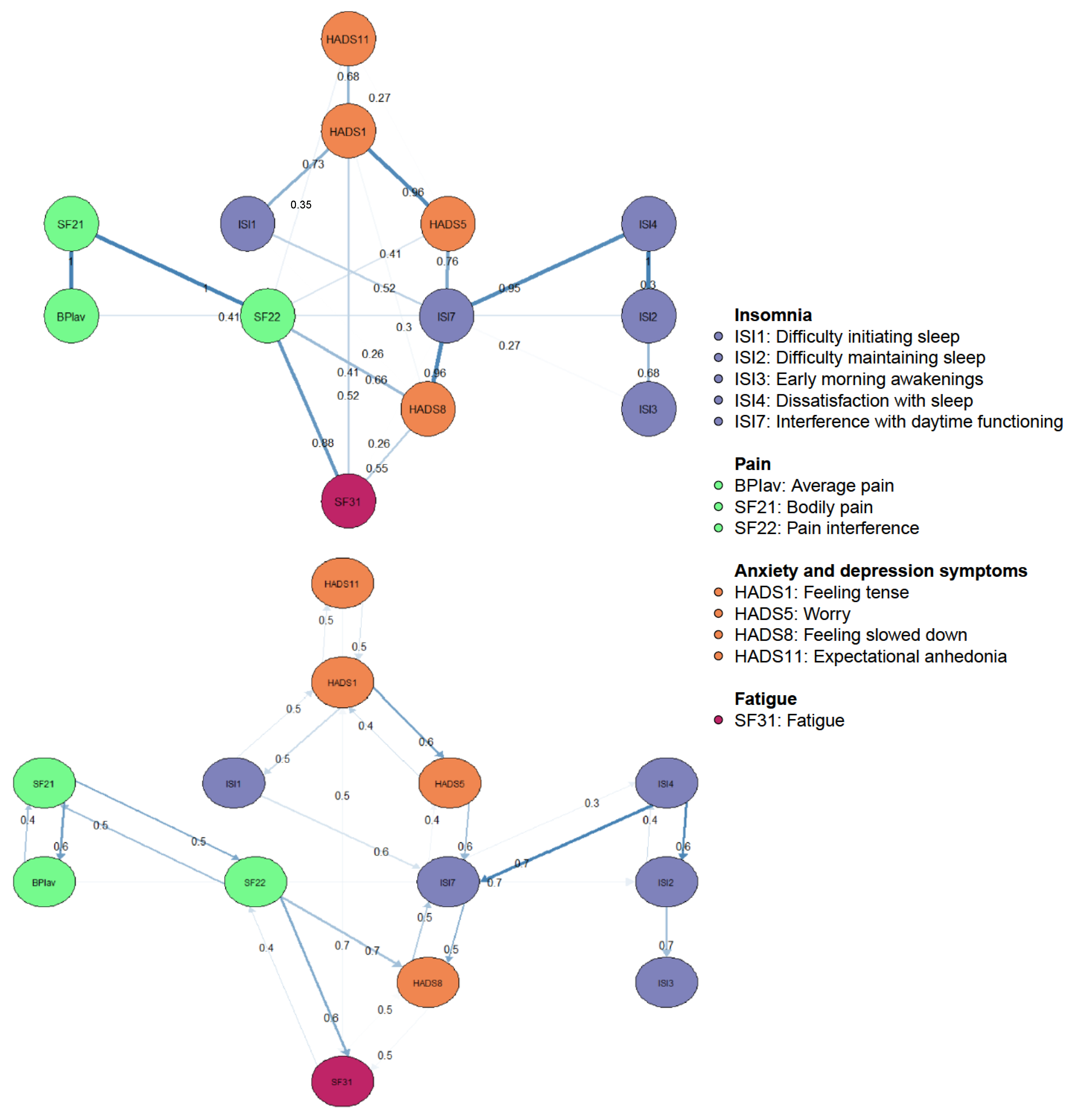
3.3. Directed Acyclic Graph
4. Discussion
4.1. Strengths and Limitations
Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bilterys, T.; Siffain, C.; De Maeyer, I.; Van Looveren, E.; Mairesse, O.; Nijs, J.; Meeus, M.; Ickmans, K.; Cagnie, B.; Goubert, D.; et al. Associates of Insomnia in People with Chronic Spinal Pain: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3175. [Google Scholar] [CrossRef]
- Kelly, G.A.; Blake, C.; Power, C.K.; O’keeffe, D.; Fullen, B.M. The Association Between Chronic Low Back Pain and Sleep A Systematic Review. Clin. J. Pain 2011, 27, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Malfliet, A.; Bilterys, T.; Van Looveren, E.; Meeus, M.; Danneels, L.; Ickmans, K.; Cagnie, B.; Mairesse, O.; Neu, D.; Moens, M.; et al. The added value of cognitive behavioral therapy for insomnia to current best evidence physical therapy for chronic spinal pain: Protocol of a randomized controlled clinical trial. Braz. J. Phys. Ther. 2019, 23, 62–70. [Google Scholar] [CrossRef]
- Langevin, H.M.; Sherman, K.J. Pathophysiological model for chronic low back pain integrating connective tissue and nervous system mechanisms. Med. Hypotheses 2007, 68, 74–80. [Google Scholar] [CrossRef]
- Dekker, K.; Blanken, T.F.; Van Someren, E.J.W. Insomnia and personality—A network approach. Brain Sci. 2017, 7, 28. [Google Scholar] [CrossRef]
- Hu, F.; Li, L.; Huang, X.; Yan, X.; Huang, P. Symptom distribution regularity of insomnia: Network and spectral clustering analysis. JMIR Med. Inform. 2020, 8, e16749. [Google Scholar] [CrossRef] [PubMed]
- Jansson-Fröjmark, M.; Boersma, K. Bidirectionality between pain and insomnia symptoms: A prospective study. Br. J. Health Psychol. 2012, 17, 420–431. [Google Scholar] [CrossRef]
- Agmon, M.; Armon, G. Increased Insomnia Symptoms Predict the Onset of Back Pain among Employed Adults. PLoS ONE 2014, 9, e103591. [Google Scholar] [CrossRef] [PubMed]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep deficiency and chronic pain: Potential underlying mechanisms and clinical implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef]
- Koffel, E.; Kroenke, K.; Bair, M.J.; Leverty, D.; Polusny, M.A.; Krebs, E.E. The bidirectional relationship between sleep complaints and pain: Analysis of data from a randomized trial. Health Psychol. 2016, 35, 41–49. [Google Scholar] [CrossRef]
- Skarpsno, E.S.; Mork, P.J.; Marcuzzi, A.; Lund Nilsen, T.I.; Meisingset, I. Subtypes of insomnia and the risk of chronic spinal pain: The HUNT study. Sleep Med. 2021, 85, 15–20. [Google Scholar] [CrossRef]
- Herrero Babiloni, A.; de Koninck, B.P.; Beetz, G.; de Beaumont, L.; Martel, M.O.; Lavigne, G.J. Sleep and pain: Recent insights, mechanisms, and future directions in the investigation of this relationship. J. Neural Transm. 2020, 127, 647–660. [Google Scholar] [CrossRef]
- de la Vega, R.; Racine, M.; Castarlenas, E.; Solé, E.; Roy, R.; Jensen, M.P.; Miró, J.; Cane, D. The Role of Sleep Quality and Fatigue on the Benefits of an Interdisciplinary Treatment for Adults With Chronic Pain. Pain Pract. 2019, 19, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Dzierzewski, J.M.; Ravyts, S.; Griffin, S.C.; Rybarczyk, B. Sleep and Pain: The Role of Depression. Curr. Sleep Med. Rep. 2019, 5, 173–180. [Google Scholar] [CrossRef]
- De Baets, L.; Runge, N.; Labie, C.; Mairesse, O.; Malfliet, A.; Verschueren, S.; Van Assche, D.; de Vlam, K.; Luyten, F.P.; Coppieters, I.; et al. The interplay between symptoms of insomnia and pain in people with osteoarthritis: A narrative review of the current evidence. Sleep Med. Rev. 2023, 70, 101793. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.L.; Edwards, P.S.; Atchison, J.W.; Lafayette-Lucey, A.; Wittmer, V.T.; Robinson, M.E. Defining patient-centered, multidimensional success criteria for treatment of chronic spine pain. Pain Med. 2008, 9, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.B.; Gu, J.; Henry, A.L.; Davis, M.L.; Espie, C.A.; Stott, R.; Heinz, A.J.; Bentley, K.H.; Goodwin, G.M.; Gorman, B.S.; et al. Feasibility and efficacy of a digital CBT intervention for symptoms of Generalized Anxiety Disorder: A randomized multiple-baseline study. J. Behav. Ther. Exp. Psychiatry 2021, 70, 101609. [Google Scholar] [CrossRef] [PubMed]
- Mason, E.C.; Harvey, A.G. Insomnia before and after treatment for anxiety and depression. J. Affect. Disord. 2014, 168, 415–421. [Google Scholar] [CrossRef]
- Fried, E.I.; Cramer, A.O.J. Illness pathways between eating disorder and post-traumatic stress disorder symptoms: Understanding comorbidity with network analysis. Eur. Eat. Disord. Rev. 2019, 27, 147–160. [Google Scholar]
- Cramer, A.O.J.; Waldorp, L.J.; Van Der Maas, H.L.J.; Borsboom, D. Comorbidity: A network perspective. Behav. Brain Sci. 2010, 33, 137–150. [Google Scholar] [CrossRef]
- Robinaugh, D.J.; Millner, A.J.; McNally, R.J. Identifying highly influential nodes in the complicated grief network. J. Abnorm. Psychol. 2016, 125, 747–757. [Google Scholar] [CrossRef]
- McNally, R.J.; Robinaugh, D.J.; Deckersbach, T.; Sylvia, L.G.; Nierenberg, A.A. Estimating the Symptom Structure of Bipolar Disorder via Network Analysis: Energy Dysregulation as a Central Symptom. J. Psychopathol. Clin. Sci. 2022, 131, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Borsboom, D.; Cramer, A.O.J. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav Res Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; Waldorp, L.J.; Mõttus, R.; Borsboom, D. The Gaussian Graphical Model in Cross-Sectional and Time-Series Data. Multivar. Behav Res. 2018, 53, 453–480. [Google Scholar] [CrossRef]
- Epskamp, S.; Maris, G.K.J.; Waldorp, L.J.; Borsboom, D. Network Psychometrics. arXiv 2016, arXiv:1609.02818. [Google Scholar] [CrossRef]
- Dalege, J.; Borsboom, D.; van Harreveld, F.; van der Maas, H.L.J. Network Analysis on Attitudes: A Brief Tutorial. Soc. Psychol. Personal. Sci. 2017, 8, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Iber, C. The AASM manual for the scoring of sleep and associated events: Rules, terminology, and technical specification. (No Title). 2007. Available online: https://scholar.google.com/citations?view_op=view_citation&hl=en&user=mLTec7cAAAAJ&citation_for_view=mLTec7cAAAAJ:tOudhMTPpwUC (accessed on 15 January 2024).
- Jun, J.; Park, C.G.; Kapella, M.C. Psychometric properties of the Insomnia Severity Index for people with chronic obstructive pulmonary disease. Sleep Med. 2022, 95, 120–125. [Google Scholar] [CrossRef]
- Hinz, A.; Glaesmer, H.; Brähler, E.; Löffler, M.; Engel, C.; Enzenbach, C.; Hegerl, U.; Sander, C. Sleep quality in the general population: Psychometric properties of the Pittsburgh Sleep Quality Index, derived from a German community sample of 9284 people. Sleep Med. 2017, 30, 57–63. [Google Scholar] [CrossRef]
- Morin, C.M.; Drake, C.L.; Harvey, A.G.; Krystal, A.D.; Manber, R.; Riemann, D. Insomnia disorder. Nat. Rev. Dis. Primers 2015, 1, 15026. [Google Scholar]
- Sateia, M.J. International classification of sleep disorders. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Riemann, D.; Espie, C.A.; Altena, E.; Arnardottir, E.S.; Baglioni, C.; Bassetti, C.L.A.; Bastien, C.; Berzina, N.; Bjorvatn, B.; Dikeos, D.; et al. The European Insomnia Guideline: An update on the diagnosis and treatment of insomnia. J. Sleep Res. 2023, 32, e14035. [Google Scholar]
- Mairesse, O.; Damen, V.; Newell, J.; Kornreich, C.; Verbanck, P.; Neu, D. The Brugmann Fatigue Scale: An Analogue to the Epworth Sleepiness Scale to Measure Behavioral Rest Propensity. Behav. Sleep Med. 2019, 17, 437–458. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional Beliefs and Attitudes about Sleep (DBAS): Validation of a Brief Version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, T.M.; Rosenfeld, B.D.; Sit, L.; Mendoza, T.R.; Fruscione, M.; Lavene, D.; Shaw, M.; Li, Y.; Hay, J.; Cleeland, C.S.; et al. Using confirmatory factor analysis to evaluate construct validity of the Brief Pain Inventory (BPI). J. Pain Symptom Manag. 2011, 41, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Kregel, J.; Vuijk, P.J.; Descheemaeker, F.; Keizer, D.; Van Der Noord, R.; Nijs, J.; Cagnie, B.; Meeus, M.; van Wilgen, P. The Dutch Central Sensitization Inventory (CSI). Clin. J. Pain 2016, 32, 624–630. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.F. The Hospital Anxiety and Depression Scale. Occup. Med. 2014, 64, 393–394. [Google Scholar] [CrossRef]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef]
- Levinson, C.A.; Brosof, L.C.; Vanzhula, I.; Christian, C.; Jones, P.; Rodebaugh, T.L.; Langer, J.K.; White, E.K.; Warren, C.; Weeks, J.W.; et al. Social anxiety and eating disorder comorbidity and underlying vulnerabilities: Using network analysis to conceptualize comorbidity. Int. J. Eat. Disord. 2018, 51, 693–709. [Google Scholar] [CrossRef]
- Heeren, A.; Mouguiama-Daouda, C.; McNally, R.J. A network approach to climate change anxiety and its key related features. J. Anxiety Disord. 2023, 93, 102625. [Google Scholar] [CrossRef] [PubMed]
- Tsang, S.; Royse, C.F.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J. Anaesth. 2017, 11, S80–S89. [Google Scholar] [CrossRef]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Methods Primers 2021, 1, 58. [Google Scholar] [CrossRef]
- Carter, J.S.; Rossell, D.; Smith, J.Q. Partial Correlation Graphical LASSO. arXiv 2021, arXiv:arXiv:2104.10099. [Google Scholar] [CrossRef]
- Heeren, A.; Bernstein, E.E.; McNally, R.J. Bridging maladaptive social self-beliefs and social anxiety: A network perspective. J. Anxiety Disord. 2020, 74, 102267. [Google Scholar] [CrossRef] [PubMed]
- Briganti, G.; Scutari, M.; Mcnally, R.J. A tutorial on Bayesian Networks for psychopathology researchers. Network theory comes with. Psychol. Methods 2022, 28, 947–961. [Google Scholar] [CrossRef]
- Lehrer, H.M.; Yao, Z.; Krafty, R.T.; Evans, M.A.; Buysse, D.J.; Kravitz, H.M.; Matthews, K.A.; Gold, E.B.; Harlow, S.D.; Samuelsson, L.B.; et al. Comparing polysomnography, actigraphy, and sleep diary in the home environment: The Study of Women’s Health Across the Nation (SWAN) Sleep Study. Sleep Adv. 2022, 3, zpac001. [Google Scholar] [CrossRef] [PubMed]
- Alsaadi, S.M.; McAuley, J.H.; Hush, J.M.; Lo, S.; Bartlett, D.J.; Grunstein, R.R.; Maher, C.G. The bidirectional relationship between pain intensity and sleep disturbance/quality in patients with low back pain. Clin. J. Pain 2014, 30, 755–765. [Google Scholar] [CrossRef]
- Tang, N.K.Y.; Goodchild, C.E.; Sanborn, A.N.; Howard, J.; Salkovskis, P.M. Deciphering the temporal link between pain and sleep in a heterogeneous chronic pain patient sample: A multilevel daily process study. Sleep 2012, 35, 675–687. [Google Scholar] [CrossRef]
- McNally, R.J.; Robinaugh, D.J.; Wu, G.W.Y.; Wang, L.; Deserno, M.K.; Borsboom, D. Mental disorders as causal systems: A network approach to posttraumatic stress disorder. Clin. Psychol. Sci. 2015, 3, 836–849. [Google Scholar] [CrossRef]
- Briganti, G.; Kornreich, C.; Linkowski, P. A network structure of manic symptoms. Brain Behav. 2021, 11, e02010. [Google Scholar] [CrossRef] [PubMed]
- Rodebaugh, T.L.; Tonge, N.A.; Piccirill, M.L.; Fried, E.; Horenstein, A.; Morrison, A.S.; Goldin, P.G.; James, J.L.; Michelle, H.; Fernandez, K.C.; et al. Does centrality in a cross-sectional network suggest intervention targets for social anxiety disorder? J. Consult. Clin. Psychol. 2018, 86, 831–844. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Aged between 18 and 65 years | Body Mass Index > 30, since this study used the baseline data of an RCT investigating an intervention |
| Native Dutch speaker | Being diagnosed with chronic widespread pain syndrome (e.g., fibromyalgia and chronic fatigue syndrome) |
| Experiencing nonspecific spinal pain for at least 3 months, at least 3 days/week, including chronic low back pain (CLBP), failed back surgery syndrome (i.e., surgery more than 3 years ago and anatomically successful surgery without symptom disappearance), and chronic traumatic and nontraumatic neck pain | Thoracic pain in the absence of neck or low back pain Neuropathic pain |
| Experiencing insomnia: self-reported sleep difficulties defined as >30 min of wake during the night [including sleep latency, wake after sleep onset, early morning awakenings, or a combination] for >3 days/week for >6 months, which cause distress or impairment in daytime functioning (despite having adequate opportunity and circumstances to sleep) in the absence of intrinsic sleep disorders and shift work | History of specific spinal surgery (i.e., surgery for spinal stenosis) to ensure the exclusion of degenerative (joint) diseases. |
| Not undertaking exercise (>3 metabolic equivalents) 3 days before the assessments | Severe underlying sleep pathology (identified through polysomnography), This includes sleep apnea (AHI > 15) and periodic limb movement disorder (>15/h). |
| Refraining from analgesics, caffeine, alcohol, or nicotine for 48 h before the assessments, since this study used the baseline data of an RCT investigating an intervention | Shift workers |
| Willing to participate in therapy sessions and not allowed to continue any other therapies (i.e., other physical therapy treatments, acupuncture, osteopathy, etc.), except for usual medication; and not having received any form of pain neuroscience education or sleep training before | Being pregnant or being a parent within one year post partum |
| Not starting new treatments or medication and continuing their usual care 6 weeks before and during study participation (to obtain a steady state) | Presence of a current clinical depression diagnosed by a doctor |
| Suffering from any specific medical condition possibly related to their pain (e.g., neuropathic pain, a history of neck or back surgery in the past 3 years, osteoporotic vertebral fractures, and rheumatologic diseases) | |
| People living more than 50 km away from the treatment location were excluded to avoid dropout because of practical considerations. |
| Number | Variable Name | Question | Answer Options |
|---|---|---|---|
| 1 | ISI1 | Difficulty falling asleep? | None/mild/moderate/severe/very severe |
| 2 | ISI2 | Difficulty staying asleep? | None/mild/moderate/severe/very severe |
| 3 | ISI3 | Problems waking up too early? | None/mild/moderate/severe/very severe |
| 4 | ISI4 | How satisfied/dissatisfied are you with your current sleep pattern? | Very satisfied/satisfied/neutral/dissatisfied/very dissatisfied |
| 5 | ISI7 | To what extent do you consider your sleep problem to interfere with your daily functioning (e.g., daytime fatigue, mood, ability to function at work, daily chores, concentration, memory, mood, etc.) currently? | Not at all interfering/a little/somewhat/much/very much interfering |
| 6 | BPIav | Please rate your pain by marking the box beside the number that best describes your pain on average. | 0 (No pain)–10 (pain as bad as you can imagine) |
| 7 | SF21 | How much bodily pain have you had during the past 4 weeks? | Not at all/slightly/moderately/severe/very severe |
| 8 | SF22 | During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)? | Not at all/a little bit/moderately/quite a bit/extremely |
| 9 | HADS1 | In the past week I have been feeling tense or ‘wound up’ | 0 (Not at all)–3 (most of the time) |
| 10 | HADS5 | In the past week I had worrying thoughts go through my mind | 0 (Only occasionally)–3 (a great deal of the time) |
| 11 | HADS8 | In the past week I have been feeling as if I am slowed down | 0 (Not at all)–3 (nearly all the time) |
| 12 | HADS11 | In the past week I have been looking forward with enjoyment to things | 0 (As much as I ever did)–3 (hardly at all) |
| 13 | SF31 | Did you feel tired? | All of the time/most of the time/some of the time/a little bit of the time/none of the time |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goossens, Z.; Bilterys, T.; Van Looveren, E.; Malfliet, A.; Meeus, M.; Danneels, L.; Ickmans, K.; Cagnie, B.; Roland, A.; Moens, M.; et al. The Role of Anxiety and Depression in Shaping the Sleep–Pain Connection in Patients with Nonspecific Chronic Spinal Pain and Comorbid Insomnia: A Cross-Sectional Analysis. J. Clin. Med. 2024, 13, 1452. https://doi.org/10.3390/jcm13051452
Goossens Z, Bilterys T, Van Looveren E, Malfliet A, Meeus M, Danneels L, Ickmans K, Cagnie B, Roland A, Moens M, et al. The Role of Anxiety and Depression in Shaping the Sleep–Pain Connection in Patients with Nonspecific Chronic Spinal Pain and Comorbid Insomnia: A Cross-Sectional Analysis. Journal of Clinical Medicine. 2024; 13(5):1452. https://doi.org/10.3390/jcm13051452
Chicago/Turabian StyleGoossens, Zosia, Thomas Bilterys, Eveline Van Looveren, Anneleen Malfliet, Mira Meeus, Lieven Danneels, Kelly Ickmans, Barbara Cagnie, Aurore Roland, Maarten Moens, and et al. 2024. "The Role of Anxiety and Depression in Shaping the Sleep–Pain Connection in Patients with Nonspecific Chronic Spinal Pain and Comorbid Insomnia: A Cross-Sectional Analysis" Journal of Clinical Medicine 13, no. 5: 1452. https://doi.org/10.3390/jcm13051452
APA StyleGoossens, Z., Bilterys, T., Van Looveren, E., Malfliet, A., Meeus, M., Danneels, L., Ickmans, K., Cagnie, B., Roland, A., Moens, M., Nijs, J., De Baets, L., & Mairesse, O. (2024). The Role of Anxiety and Depression in Shaping the Sleep–Pain Connection in Patients with Nonspecific Chronic Spinal Pain and Comorbid Insomnia: A Cross-Sectional Analysis. Journal of Clinical Medicine, 13(5), 1452. https://doi.org/10.3390/jcm13051452