


The Effectiveness of Early Rehabilitation in Limiting the Progression of Idiopathic Scoliosis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
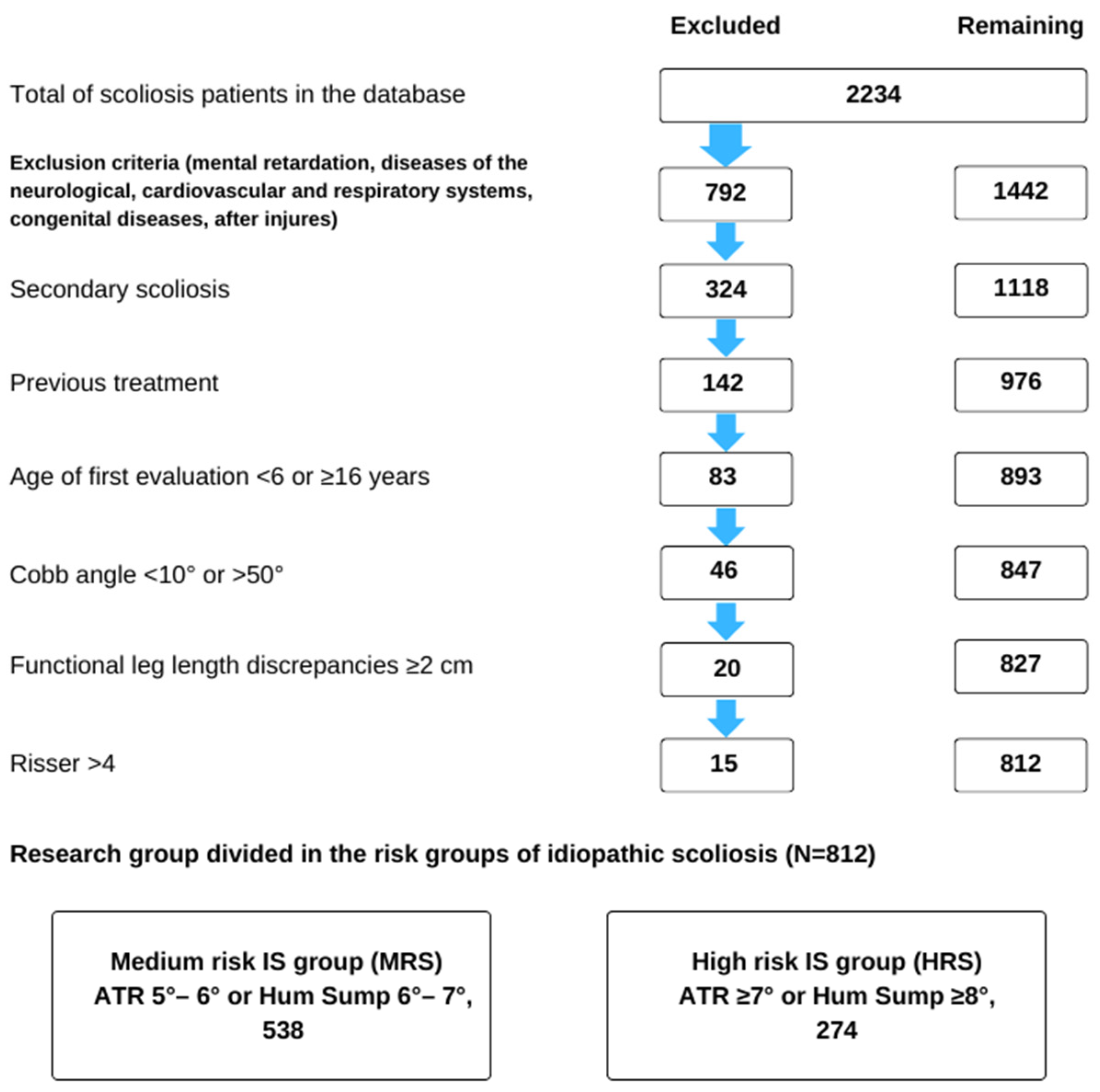
2.2. Population
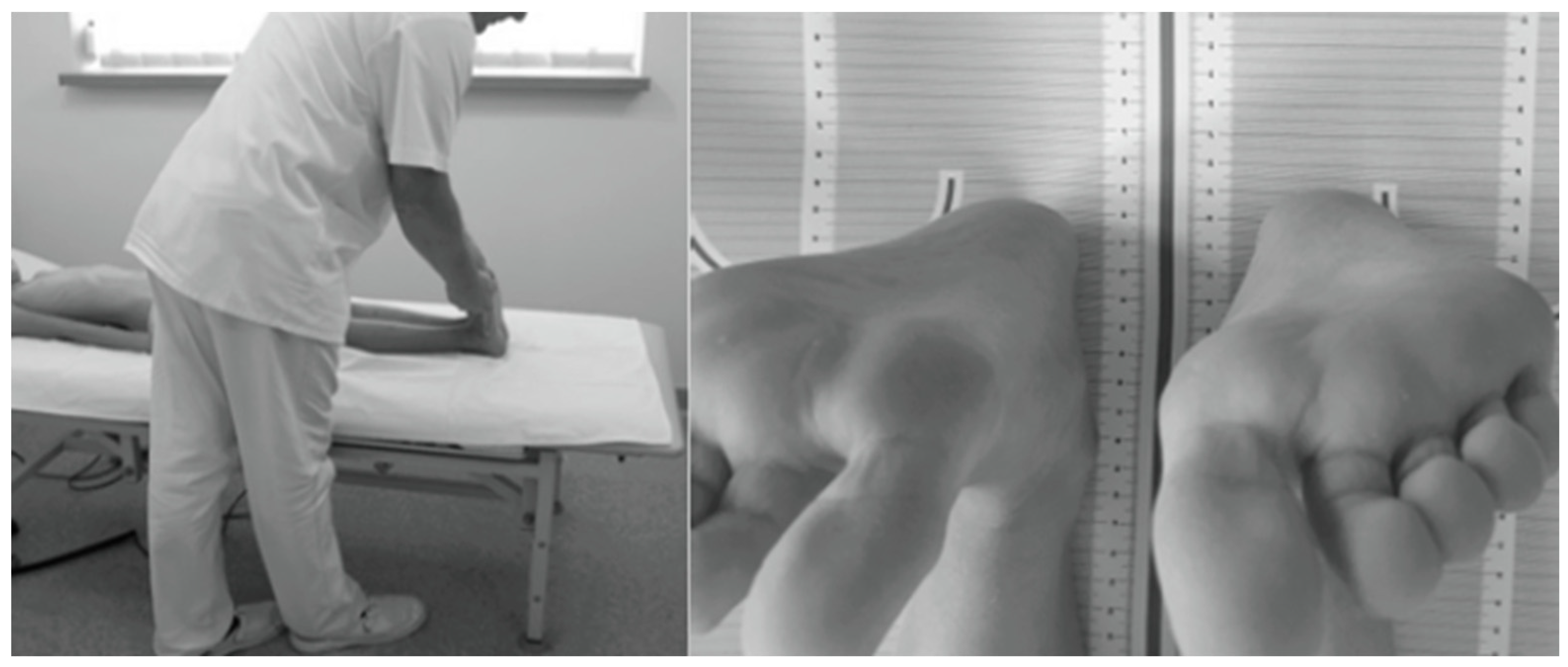
2.3. Methods
2.4. Data Analysis
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rigo, M.D.; Grivas, T.B. Rehabilitation Schools for Scoliosis Thematic Series: Describing the Methods and Results. Scoliosis 2010, 5, 27. [Google Scholar] [CrossRef]
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.; Danielsson, A.; Morcuende, J.A. Adolescent Idiopathic Scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.S.; Mayo, N.E.; Poitras, B.; Scott, S.; Hanley, J. The Ste-Justine Adolescent Idiopathic Scoliosis Cohort Study: Part I. Spine 1994, 19, 1551–1561. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Zaina, F. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef]
- Grivas, T.B.; Vasiliadis, E.; Chatziargiropoulos, T.; Polyzois, V.D.; Gatos, K. The effect of a modified Boston brace with anti-rotatory blades on the progression of curves in idiopathic scoliosis: Aetiologic implications. Pediatr. Rehabil. 2003, 6, 237–242. [Google Scholar] [CrossRef]
- Aulisa, A.; Guzzanti, V.; Falciglia, F.; Giordano, M.; Galli, M.; Aulisa, L. Brace treatment of idiopathic scoliosis is effective for a curve over 40 degrees, but is the evaluation of Cobb angle the only parameter for the indication of treatment? Eur. J. Phys. Rehabil. Med. 2019, 55, 231–240. [Google Scholar] [CrossRef]
- Dunn, J.; Henrikson, N.B.; Morrison, C.C. Report and Systematic Review for the US Preventive Services Task Force. JAMA 2018, 319, 173–187. [Google Scholar] [CrossRef]
- Rigo, M.; Reiter, C.; Weiss, H.-R. Effect of Conservative Management on the Prevalence of Surgery in Patients with Adolescent Idiopathic Scoliosis. Pediatr. Rehabil. 2003, 6, 209–214. [Google Scholar] [CrossRef]
- Kowalski, I.M.; van Dam, F.; Zarzycki, D.; Rymarczyk, A.; Sebastianowicz, P. Short-duration electrostimulation in the treatment of idiopathic scoliosis. Ortop. Traumatol. Rehabil. 2004, 6, 82–89. [Google Scholar]
- Lee, C.F.; Fong, D.Y.T.; Cheung, K.M.C.; Cheng, J.C.Y.; Ng, B.K.W.; Lam, T.P.; Mak, K.H.; Yip, P.S.F.; Luk, K.D.K. Referral Criteria for School Scoliosis Screening: Assessment and Recommendations Based on a Large Longitudinally Followed Cohort. Spine 2010, 35, E1492–E1498. [Google Scholar] [CrossRef]
- Côté, P.; Kreitz, B.G.; Cassidy, J.D.; Dzus, A.K.; Martel, J. A Study of the Diagnostic Accuracy and Reliability of the Scoliometer and Adam’s Forward Bend Test. Spine 1998, 23, 796–802. [Google Scholar] [CrossRef]
- Grivas, T.B.; Vasiliadis, E.S.; Koufopoulos, G.; Segos, D.; Triantafyllopoulos, G.; Mouzakis, V. Study of Trunk Asymmetry in Normal Children and Adolescents. Scoliosis 2006, 1, 19. [Google Scholar] [CrossRef] [PubMed]
- Kluszczyński, M.; Pilis, A.; Czaprowski, D. The Importance of the Size of the Trunk Inclination Angle in the Early Detection of Scoliosis in Children. BMC Musculoskelet. Disord. 2022, 23, 5. [Google Scholar] [CrossRef] [PubMed]
- Kluszczyński, M.; Mosler, D.; Wąsik, J. Morphological Differences in Scoliosis Curvatures as a Cause of Difficulties in Its Early Detection Based on Angle of Trunk Inclination. BMC Musculoskelet. Disord. 2022, 23, 948. [Google Scholar] [CrossRef] [PubMed]
- Burwell, R.G.; Aujla, R.K.; Grevitt, M.P.; Dangerfield, P.H.; Moulton, A.; Randell, T.L.; Anderson, S.I. Pathogenesis of Adolescent Idiopathic Scoliosis in Girls—A Double Neuro-Osseous Theory Involving Disharmony between Two Nervous Systems, Somatic and Autonomic Expressed in the Spine and Trunk: Possible Dependency on Sympathetic Nervous System and Hormones with Implications for Medical Therapy. Scoliosis 2009, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Ryu, J.S. Two Different Mechanisms of Adolescent Idiopathic Scoliosis: Asymmetrical Hyperactivation and Asymmetrical Weakness. Arch. Phys. Med. Rehabil. 2020, 101, e65. [Google Scholar] [CrossRef]
- Grivas, T.B.; Angouris, K.; Chandrinos, M.; Kechagias, V. Truncal Changes in Children with Mild Limb Length Inequality: A Surface Topography Study. Scoliosis 2018, 13, 27. [Google Scholar] [CrossRef]
- D’Amico, M.; Roncoletta, P.; Di Felice, F.; Porto, D.; Bellomo, R.; Saggini, R. Leg Length Discrepancy in Scoliotic Patients. Res. Spinal Deform 2012, 176, 146–150. [Google Scholar]
- Pasha, S.; Sangole, A.P.; Aubin, C.-E.; Parent, S.; Mac-Thiong, J.-M.; Labelle, H. Characterizing Pelvis Dynamics in Adolescent with Idiopathic Scoliosis. Spine 2010, 35, E820–E826. [Google Scholar] [CrossRef]
- Stylianides, G.A.; Beaulieu, M.; Dalleau, G.; Rivard, C.-H.; Allard, P. Iliac Crest Orientation and Geometry in Able-Bodied and Non-Treated Adolescent Idiopathic Scoliosis Girls with Moderate and Severe Spinal Deformity. Eur. Spine J. 2012, 21, 725–732. [Google Scholar] [CrossRef][Green Version]
- Schlösser, T.P.C.; Shah, S.A.; Reichard, S.J.; Rogers, K.; Vincken, K.L.; Castelein, R.M. Differences in Early Sagittal Plane Alignment between Thoracic and Lumbar Adolescent Idiopathic Scoliosis. Spine J. 2014, 14, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Gollogly, S.; Berthonnaud, E.; Dimnet, J. Classification of the Normal Variation in the Sagittal Alignment of the Human Lumbar Spine and Pelvis in the Standing Position. Spine 2005, 30, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Mac-Thiong, J.-M.; Labelle, H.; Berthonnaud, E.; Betz, R.R.; Roussouly, P. Sagittal Spinopelvic Balance in Normal Children and Adolescents. Eur. Spine J. 2007, 16, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Czaprowski, D.; Kotwicki, T.; Pawłowska, P.; Stoliński, L. Joint Hypermobility in Children with Idiopathic Scoliosis: SOSORT Award 2011 Winner. Scoliosis 2011, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- Smits-Engelsman, B.; Klerks, M.; Kirby, A. Beighton Score: A Valid Measure for Generalized Hypermobility in Children. J. Pediatr. 2011, 158, 119–123.e4. [Google Scholar] [CrossRef] [PubMed]
- Mallik, A.K.; Ferrell, W.R.; McDONALD, A.G.; Sturrock, R.D. Impaired Proprioceptive Acuity at the Proximal Interphalangeal Joint en Patients with the Hypermobility Syndrome. Rheumatology 1994, 33, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Barrack, R.L.; Whitecloud, T.S.; Burke, S.W.; Cook, S.D.; Harding, A.F. Proprioception in Idiopathic Scoliosis. Spine 1984, 9, 681–685. [Google Scholar] [CrossRef]
- Simoneau, M.; Mercier, P.; Blouin, J.; Allard, P.; Teasdale, N. Altered Sensory-Weighting Mechanisms Is Observed in Adolescents with Idiopathic Scoliosis. BMC Neurosci. 2006, 7, 68. [Google Scholar] [CrossRef]
- Smania, N.; Picelli, A.; Romano, M.; Negrini, S. Neurophysiological Basis of Rehabilitation of Adolescent Idiopathic Scoliosis. Disabil. Rehabil. 2008, 30, 763–771. [Google Scholar] [CrossRef]
- Adler, N.; Bleck, E.E.; Rinsky, L.A.; Young, W. Balance Reactions and Eye–Hand Coordination in Idiopathic Scoliosis. J. Orthop. Res. 1986, 4, 102–107. [Google Scholar] [CrossRef]
- Byl, N.N.; Gray, J.M. Complex Balance Reactions in Different Sensory Conditions: Adolescents with and without Idiopathic Scoliosis. J. Orthop. Res. 1993, 11, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Hawes, M.C.; O’Brien, J.P. The Transformation of Spinal Curvature into Spinal Deformity: Pathological Processes and Implications for Treatment. Scoliosis 2006, 1, 3. [Google Scholar] [CrossRef]
- Raczkowski, J.W.; Daniszewska, B.; Zolynski, K. Clinical Research Functional Scoliosis Caused by Leg Length Discrepancy. Arch. Med. Sci. 2010, 3, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Brady, R.J.; Dean, J.B.; Skinner, T.M.; Gross, M.T. Limb Length Inequality: Clinical Implications for Assessment and Intervention. J. Orthop. Sports Phys. Ther. 2003, 33, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Moseley, C.F. Leg-Length Discrepancy. Pediatr. Clin. N. Am. 1986, 33, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Sekiya, T.; Aota, Y.; Yamada, K.; Kaneko, K.; Ide, M.; Saito, T. Evaluation of Functional and Structural Leg Length Discrepancy in Patients with Adolescent Idiopathic Scoliosis Using the EOS Imaging System: A Prospective Comparative Study. Scoliosis 2018, 13, 7. [Google Scholar] [CrossRef]
- Mannello, D. Leg Length Inequality. J. Manip. Physiol. Ther. 1992, 15, 576–590. [Google Scholar] [PubMed]
- Stricker, S.; Hunt, T. Evaluation of Leg Length Discrepancy in Children. Int. Pediatr. 2004, 19, 134–146. [Google Scholar]
- Kotwicki, T.; Kubiak, A.; Szulc, A. Static Pelvic Obliquity Can Influence Clinical Assessment of Trunk Rotation in Idiopathic Scoliosis. Scoliosis 2009, 4, O2. [Google Scholar] [CrossRef][Green Version]
- Stokes, I.A.F.; Spence, H.; Aronsson, D.D.; Kilmer, N. Mechanical Modulation of Vertebral Body Growth: Implications for Scoliosis Progression. Spine 1996, 21, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Rigo, M.; Weiss, H.R.; the members of the Scientific society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). Why Do We Treat Adolescent Idiopathic Scoliosis? What We Want to Obtain and to Avoid for Our Patients. SOSORT 2005 Consensus Paper. Scoliosis 2006, 1, 4. [Google Scholar] [CrossRef]
- Pasha, S.; Aubin, C.-E.; Sangole, A.P.; Labelle, H.; Parent, S.; Mac-Thiong, J.-M. Three-Dimensional Spinopelvic Relative Alignment in Adolescent Idiopathic Scoliosis. Spine 2014, 39, 564–570. [Google Scholar] [CrossRef]
- Miyagi, M.; Saito, W.; Imura, T.; Nakazawa, T.; Shirasawa, E.; Kawakubo, A.; Uchida, K.; Akazawa, T.; Inage, K.; Ohtori, S.; et al. Body Composition in Japanese Girls with Adolescent Idiopathic Scoliosis. Spine Surg. Relat. Res. 2020, 5, 68–74. [Google Scholar] [CrossRef]
- Kluszczyński, M.; Czernicki, J. Incidence of Asymmetry of the Back and Pelvis in School Children with Hip Dysplasia in the Neonatal and Infancy Period. Quarter. Ortop. 2008, 197–209. [Google Scholar]
- Wang, Z.W.; Wang, W.J.; Sun, M.H.; Liu, Z.; Zhu, Z.Z.; Zhu, F.; Qiu, X.S.; Qian, B.P.; Wang, S.F.; Qiu, Y. Characteristics of the pelvic axial rotation in adolescent idiopathic scoliosis: A comparison between major thoracic curve and major thoracolumbar/lumbar curve. Spine J. 2014, 14, 1873–1878. [Google Scholar] [CrossRef]
- Sabharwal, S.; Kumar, A. Methods for Assessing Leg Length Discrepancy. Clin. Orthop. Relat. Res. 2008, 466, 2910–2922. [Google Scholar] [CrossRef] [PubMed]
- Woerman, A.L.; Binder-Macleod, S.A. Leg Length Discrepancy Assessment: Accuracy and Precision in Five Clinical Methods of Evaluation. J. Orthop. Sports Phys. Ther. 1984, 5, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Badii, M.; Wade, A.N.; Collins, D.R.; Nicolaou, S.; Kobza, B.J.; Kopec, J.A. Comparison of Lifts Versus Tape Measure in Determining Leg Length Discrepancy. J. Rheumatol. 2014, 41, 1689–1694. [Google Scholar] [CrossRef] [PubMed]
- Cooperstein, R.; Lisi, A. Pelvic Torsion: Anatomic Considerations, Construct Validity, and Chiropractic Examination Procedures. Top. Clin. Chiropr. 2000, 7, 38–49. [Google Scholar]
- Travell, J.G.; Simons, D.G. Myofascial Pain and Dysfunction: The Trigger Point Manual; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1992; ISBN 978-0-683-08367-5. [Google Scholar]
- Fryer, G. Factors Affecting the Intra-Examiner and Inter-Examiner Reliability of Palpation for Supine Medial Malleoli Asymmetry. Int. J. Osteopath. Med. 2006, 9, 58–65. [Google Scholar] [CrossRef]
- Korovessis, P.; Piperos, G.; Sidiropoulos, P.; Dimas, A. Adult idiopathic lumbar scoliosis: A formula for prediction of progression and review of the literature. Spine 1994, 19, 1926–1932. [Google Scholar] [CrossRef]
- Negrini, S.; Atanasio, S.; Fusco, C.; Zaina, F. Effectiveness of Complete Conservative Treatment for Adolescent Idiopathic Scoliosis (Bracing and Exercises) Based on SOSORT Management Criteria: Results According to the SRS Criteria for Bracing Studies—SOSORT Award 2009 Winner. Scoliosis 2009, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Kotwicki, T.; Negrini, S.; Grivas, T.B.; Rigo, M.; Maruyama, T.; Durmala, J.; Zaina, F. Methodology of evaluation of morphology of the spine and the trunk in idiopathic scoliosis and other spinal deformities—6th SOSORT consensus paper. Scoliosis 2009, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Lonstein, J.E.; Carlson, J.M. The Prediction of Curve Progression in Untreated Idiopathic Scoliosis during Growth. J. Bone Jt. Surg. 1984, 66, 1061–1071. [Google Scholar] [CrossRef]
- Masso, P.D.; Meeropol, E.; Lennon, E. Juvenile onset scoliosis followed up to adulthood: Orthopedic and functional outcomes. J. Pediatr. Orthop. 2002, 22, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Meade, K.P.; Bunch, W.; Vanderby, R.; Patwardhan, A.G.; Knight, G. Progression of unsupported curves in AIS. Spine 1987, 12, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Mehta, M. The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J. Bone Jt. Surg. 1972, 54B, 230–243. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Lusini, M.; Minnella, S.; Zaina, F. The Effectiveness of Combined Bracing and Exercise in Adolescent Idiopathic Scoliosis Based on SRS and SOSORT Criteria: A Prospective Study. BMC Musculoskelet. Disord. 2014, 15, 263. [Google Scholar] [CrossRef]
- Coillard, C.; Vachon, V.; Circo, A.B.; Beauséjour, M.; Rivard, C.H. Effectiveness of the SpineCor Brace Based on the New Standardized Criteria Proposed by the Scoliosis Research Society for Adolescent Idiopathic Scoliosis. J. Pediatr. Orthop. 2007, 27, 375–379. [Google Scholar] [CrossRef]
- Aulisa, A.G.; Guzzanti, V.; Galli, M.; Perisano, C.; Falciglia, F.; Aulisa, L. Treatment of Thoraco-Lumbar Curves in Adolescent Females Affected by Idiopathic Scoliosis with a Progressive Action Short Brace (PASB): Assessment of Results According to the SRS Committee on Bracing and Nonoperative Management Standardization Criteria. Scoliosis 2009, 4, 21. [Google Scholar] [CrossRef]
- Maruyama, T.; Kitagawa, T.; Takeshita, K.; Mochizuki, K.; Nakamura, K. Conservative Treatment for Adolescent Idiopathic Scoliosis: Can It Reduce the Incidence of Surgical Treatment? Pediatr. Rehabil. 2003, 6, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Donzelli, S.; Negrini, A.; Parzini, S.; Romano, M.; Zaina, F. End Growth Results of Exercise Treatment to Avoid Bracing in Adolescents with Idiopathic Scoliosis: A Prospective Cohort Controlled Study. Scoliosis 2014, 9, O71. [Google Scholar] [CrossRef][Green Version]
- Guan, T.; Zhang, Y.; Anwar, A.; Zhang, Y.; Wang, L. Determination of Three-Dimensional Corrective Force in Adolescent Idiopathic Scoliosis and Biomechanical Finite Element Analysis. Front. Bioeng. Biotechnol. 2020, 8, 963. [Google Scholar] [CrossRef] [PubMed]
- Kwan, K.Y.H.; Cheng, A.C.S.; Koh, H.Y.; Chiu, A.Y.Y.; Cheung, K.M.C. Effectiveness of Schroth Exercises during Bracing in Adolescent Idiopathic Scoliosis: Results from a Preliminary Study—SOSORT Award 2017 Winner. Scoliosis 2017, 12, 32. [Google Scholar] [CrossRef]
- Monticone, M.; Ambrosini, E.; Cazzaniga, D.; Rocca, B.; Ferrante, S. Active Self-Correction and Task-Oriented Exercises Reduce Spinal Deformity and Improve Quality of Life in Subjects with Mild Adolescent Idiopathic Scoliosis. Results of a Randomised Controlled Trial. Eur. Spine J. 2014, 23, 1204–1214. [Google Scholar] [CrossRef] [PubMed]
- Knutson, G.A. Anatomic and functional leg-length inequality: A review and recommendation for clinical decision-making. Part I. Anatomic leg-length inequality: Prevalence, magnitude, effects and clinical significance. Chiropr. Osteopat. 2005, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Landauer, F. Diagnosis and Treatment of Leg-Length Discrepancy in Scoliosis. Scoliosis 2013, 8, O41. [Google Scholar] [CrossRef][Green Version]
- McCaw, S.T.; Bates, B.T. Biomechanical implications of mild leg length inequality. Br. J. Sp. Med. 1991, 25, 10–13. [Google Scholar] [CrossRef]
- Cummings, G.; Scholz, J.P.; Barnes, K. The effect of imposed leg length difference on pelvic bone symmetry. Spine 1993, 18, 368–373. [Google Scholar] [CrossRef]
- Marsiolo, M.; Careri, S.; Bandinelli, D.; Toniolo, R.M.; Aulisa, A.G. Vertebral Rotation in Functional Scoliosis Caused by Limb-Length Inequality: Correlation between Rotation, Limb Length Inequality, and Obliquity of the Sacral Shelf. J. Clin. Med. 2023, 12, 5571. [Google Scholar] [CrossRef]
- Gurney, B. Leg length discrepancy. Rev. Gait. Posture 2002, 15, 195–206. [Google Scholar] [CrossRef]
- Walsh, M.; Connolly, P.; Jenkinson, A.; O’Brien, T. Leg length discrepancy—An experimental study of compensatory changes in three dimensions using gait analysis. Gait Posture 2000, 12, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Rannisto, S.; Okuloff, A.; Uitti, J.; Paananen, M.; Rannisto, P.; Malmivaara, A.; Karppinen, J. Leg-length discrepancy is associated with low back pain among those who must stand while working. BMC Musculoskelet. Disord. 2015, 16, 110. [Google Scholar] [CrossRef] [PubMed]
- Soukka, A.; Alaranta, H.; Tallroth, K.; Heliovaara, M. Leg-length inequality in people of working age. The association between mild inequality and lowback pain is questionable. Spine 1991, 16, 429–431. [Google Scholar] [CrossRef]
- Betsch, M.; Rapp, W.; Przibylla, A.; Jungbluth, P.; Hakimi, M.; Schneppendahl, J.; Thelen, S.; Wild, M. Determination of the amount of leg length inequality that alters spinal posture in healthy subjects using rasterstereography. Eur. Spine J. 2013, 22, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Lehnert-Schroth, C.H. Drei Dimensionale Skoliose Behandlung, 6th ed.; Urban & Fischer: Stuttgart, Germany, 2000. [Google Scholar]
- Karnath, H.O.; Ferber, S.; Dichgans, J. Neural representation of postural control in humans. Proc. Natl. Acad. Sci. USA 2000, 97, 13931–13936. [Google Scholar] [CrossRef]
- Zabjek, K.F.; Leroux, M.A.; Coillard, C.; Rivard, C.-H.; Prince, F. Evaluation of Segmental Postural Characteristics during Quiet Standingin Control and Idiopathic Scoliosis Patients. Clin. Biomech. 2005, 20, 483–490. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Parameter | Total (n = 812) |
|---|---|---|
| Study group | n | 812 |
| Mean age (SD) | 10.66 (3.16) | |
| Median (Q1–Q3) | 10 (8–13) | |
| Range | 6–16 | |
| Age division [years] | 6–9 | 27% (n = 219) |
| 10–12 | 32.3% (n = 262) | |
| 13–16 | 40.8% (n = 331) | |
| Gender | Girls | 65.5% (n = 532) |
| Boys | 34.5% (n = 280) | |
| Risk groups for IS | Medium (ATR 5–6° or Hum Sump ≤ 7°) | 66.3% (n = 538) |
| High (ATR ≥ 7° or Hum Sump ≥ 8) | 33.7% (n = 274) | |
| X-ray patients from the HRS | 33.7% (n = 274). | |
| Only one X-ray | 11.4% (n = 93) | |
| More than one X-ray 22.3% (n = 181) | ||
| Mean cobb angle (SD) | 23.4° (7.83°) | |
| Median (Q1–Q3) | 21° (15–30°) | |
| Range | 10–50° | |
| ATR angle | n | 1113 |
| Mean ATR (SD) | 5.36° (2.35°) | |
| Median (Q1–Q3) | 5° (4–6°) | |
| Range | 3–25° | |
| Functional shortening of the lower limb | Left | 15.4% (n = 125) |
| Right | 25.4% (n = 206) | |
| Equal | 59.2% (n = 481) | |
| Duration of treatment and observation [months] | n | 812 |
| Mean (SD) | 28.1 (14.5) | |
| Median (Q1–Q3) | 18 (9–40) | |
| Range | 1–67 | |
| Age (Sample Size) | Time Point | Risk Groups for IS | Patients Referred for Observation | |
|---|---|---|---|---|
| High: ATR ≥ 7° or Hum Sump ≥ 8° | Medium: ATR 5–6° or Hum Sump ≤ 7° | |||
| 6–9 years old (n = 219) | Before therapy | 33.8% (n = 74) | 66.2% (n = 145) | |
| After therapy | 11.4% (n = 25) | 66.2% (n = 145) | 22.4% (n = 49) | |
| 10–12 years old (n = 262) | Before therapy | 30.9% (n = 81) | 69.1% (n = 181) | |
| After therapy | 27.6% (n = 73) | 69% (n= 180) | 3.4% (n = 9) | |
| 13–16 years old (n = 331) | Before therapy | 36% (n = 119) | 64% (n = 177) | |
| After therapy | 25.4% (n = 84) | 64% (n = 212) | 10.6% (n = 35) | |
| Total n = 812 | Before therapy | 33.7% (n = 274) | 66.3% (n = 538) | |
| After therapy | 22.3% (n = 181) | 66.6% (n = 539) | 11.5% (n = 93) | |
| Age | Time Points | Before Therapy | p-Value | ||
|---|---|---|---|---|---|
| MRS | HRS | ||||
| 6–9 years (n = 219) | After therapy | MRS | 66.2% (n = 145) | 22.4% (n = 49) | <0.001 |
| HRS | 0% (n = 0) | 11.4% (n = 25) | |||
| 10–12 (n = 262) | MRS | 69% (n = 180) | 3.4% (n = 9) | 0.0133 | |
| HRS | 0% (n = 0) | 27.6% (n = 73) | |||
| 13–16 (n = 331) | MRS | 64% (n = 212) | 10.6% (n = 35) | <0.001 | |
| HRS | 0% (n = 0) | 25.4% (n = 84) | |||
| Total (n = 812) | MRS | 66.3% (n = 538) | 11.5% (n = 92) | <0.001 | |
| HRS | 0% (n = 0) | 22.3% (n = 181) | |||
| Parameter ATR Angle | Before Treatment | After Treatment | p-Value | |
|---|---|---|---|---|
| Thoracic section (Th) | n | 352 | 352 | <0.001 |
| Mean (SD) | 5.42 (2.78) | 4.83 (2.94) | ||
| Median (Q1–Q3) | 5 (4–5) | 4 (3–5) | ||
| Range | 3–25 | 0–23 | ||
| Thoracolumbar section (Th-L) | n | 396 | 396 | <0.001 |
| Mean (SD) | 5.29 (1.91) | 4.07 (1.93) | ||
| Median (Q1–Q3) | 5 (4–6) | 4 (3–5) | ||
| Range | 3–16 | 0–14 | ||
| Lumbar section (L) | n | 267 | 267 | <0.001 |
| Mean (SD) | 5.36 (2.08) | 4.52 (2.59) | ||
| Median (Q1–Q3) | 5 (4–6) | 4 (3–5) | ||
| Range | 3–14 | 0–12 |
| Parameter: Cobb Angle | Before Treatment | After Treatment | p-Value | |
|---|---|---|---|---|
| Thoracic section (Th) | n | 75 | 75 | 0.2543 |
| Mean (SD) | 24.53 (12.33) | 23.49 (13.02) | ||
| Median (Q1–Q3) | 22 (15.5–30) | 21 (14.5–30) | ||
| Range | 10–50 | 5–66 | ||
| Thoracolumbar section (Th-L) | n | 37 | 37 | 0.0061 |
| Mean (SD) | 21.49 (7.86) | 18.94 (8.23) | ||
| Median (Q1–Q3) | 21 (15–25) | 18 (12–24) | ||
| Range | 10–45 | 8–41 | ||
| Lumbar section (L) | n | 69 | 69 | 0.7505 |
| Mean (SD) | 23.35 (11.51) | 23.17 (12.31) | ||
| Median (Q1–Q3) | 20 (15–30) | 23 (14–32) | ||
| Range | 10–50 | 5–63 |
| Parameter and Sample Size | Results after Treatment | Thoracic Section (Th) | Thoracolumbar Section (Th-L) | Lumbar Section (L) |
|---|---|---|---|---|
| X-ray (Cobb angle) n = 181 | n = 75 | n = 37 | n = 69 | |
| stabilization | 38% (n = 69) | 30% (n = 54) | 34% (n = 62) | |
| worsened | 17.3% (n = 31) | 8.9% (n = 16) | 21.8% (n = 39) | |
| improvement | 44.7% (n = 81) | 61.1% (n = 111) | 44.2% (n = 80) | |
| ATR angle n = 812 | n = 352 | n = 396 | n = 267 | |
| stabilization | 24.7% (n = 87) | 19.2% (n = 76) | 26.6% (n = 71) | |
| worsened | 23.6% (n = 83) | 16.2% (n = 64) | 16.5% (n = 44) | |
| improvement | 51.7% (n = 182) | 64.6% (n = 256) | 56.9% (n = 152) | |
| Change in FLLDs after treatment n = 812 | n = 352 | n = 396 | n = 267 | |
| FLLD = 0 before and after treatment | 65.3% (n = 230) | 57.3% (n = 227) | 61.8% (n = 165) | |
| Left | 1.4% (n = 5) | 1.3% (n = 5) | 1.1% (n = 3) | |
| It withdrew after treatment | 33.2% (n = 117) | 41.4% (n = 164) | 37.1% (n = 99) |
| Shortening side | Shortening of the lower limb before treatment | p-value | |||
| Thoracic (Th), n = 352 | |||||
| Left: 13.6%, n = 48 | Equal: 64.6%, n = 227 | Right: 21.8%, n = 77 | <0.001 | ||
| Shortening of the lower limb after treatment | Left (n = 8) | 2%, n = 7 | 0.3%, n = 1 | 0%, n = 0 | |
| Equal (n = 328) | 11.6%, n = 41 | 63.6%, n = 224 | 17.9%, n = 63 | ||
| Right (n = 16) | 0%, n = 0 | 0.6%, n = 2 | 4%, n = 14 | ||
| Thoracolumbar (Th-L), n = 396 | <0.001 | ||||
| Left: 15.2%, n = 60 | Equal: 56.1%, n = 222 | Right: 28.8%, n = 114 | |||
| Left (n = 14) | 3.5%, n = 14 | 0%, n = 0 | 0%, n = 0 | ||
| Equal (n = 348) | 11.6%, n = 46 | 55.3%, n = 219 | 21%, n = 83 | ||
| Right (n = 34) | 0%, n = 0 | 0.8%, n = 3 | 7.8%, n = 31 | ||
| Lumbar (L) (n = 267) | <0.001 | ||||
| Left: 18%, n = 48 | Equal: 60.7%, n = 162 | Right: 21.3%, n = 57 | |||
| Left (n = 12) | 4.1%, n = 11 | 0.4%, n = 1 | 0%, n = 0 | ||
| Equal (n = 239) | 13.9%, n = 37 | 60.3%, n = 161 | 15.4%, n = 41 | ||
| Right (n = 16) | 0%, n = 0 | 0%, n = 0 | 6%, n = 16 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kluszczyński, M.; Zaborowska-Sapeta, K.; Kowalski, I.; Karpiel, I. The Effectiveness of Early Rehabilitation in Limiting the Progression of Idiopathic Scoliosis. J. Clin. Med. 2024, 13, 1422. https://doi.org/10.3390/jcm13051422
Kluszczyński M, Zaborowska-Sapeta K, Kowalski I, Karpiel I. The Effectiveness of Early Rehabilitation in Limiting the Progression of Idiopathic Scoliosis. Journal of Clinical Medicine. 2024; 13(5):1422. https://doi.org/10.3390/jcm13051422
Chicago/Turabian StyleKluszczyński, Marek, Katarzyna Zaborowska-Sapeta, Ireneusz Kowalski, and Ilona Karpiel. 2024. "The Effectiveness of Early Rehabilitation in Limiting the Progression of Idiopathic Scoliosis" Journal of Clinical Medicine 13, no. 5: 1422. https://doi.org/10.3390/jcm13051422
APA StyleKluszczyński, M., Zaborowska-Sapeta, K., Kowalski, I., & Karpiel, I. (2024). The Effectiveness of Early Rehabilitation in Limiting the Progression of Idiopathic Scoliosis. Journal of Clinical Medicine, 13(5), 1422. https://doi.org/10.3390/jcm13051422