
The Outcome of Local Excision of Rectal Adenomas with High-Grade Dysplasia by Transanal Endoscopic Microsurgery: A Single-Center Experience


Abstract
1. Introduction
2. Materials and Methods
3. Results
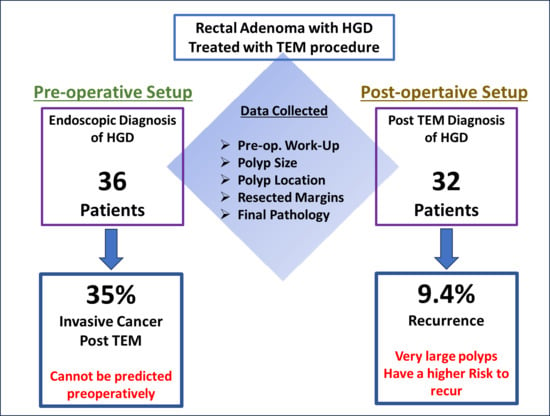
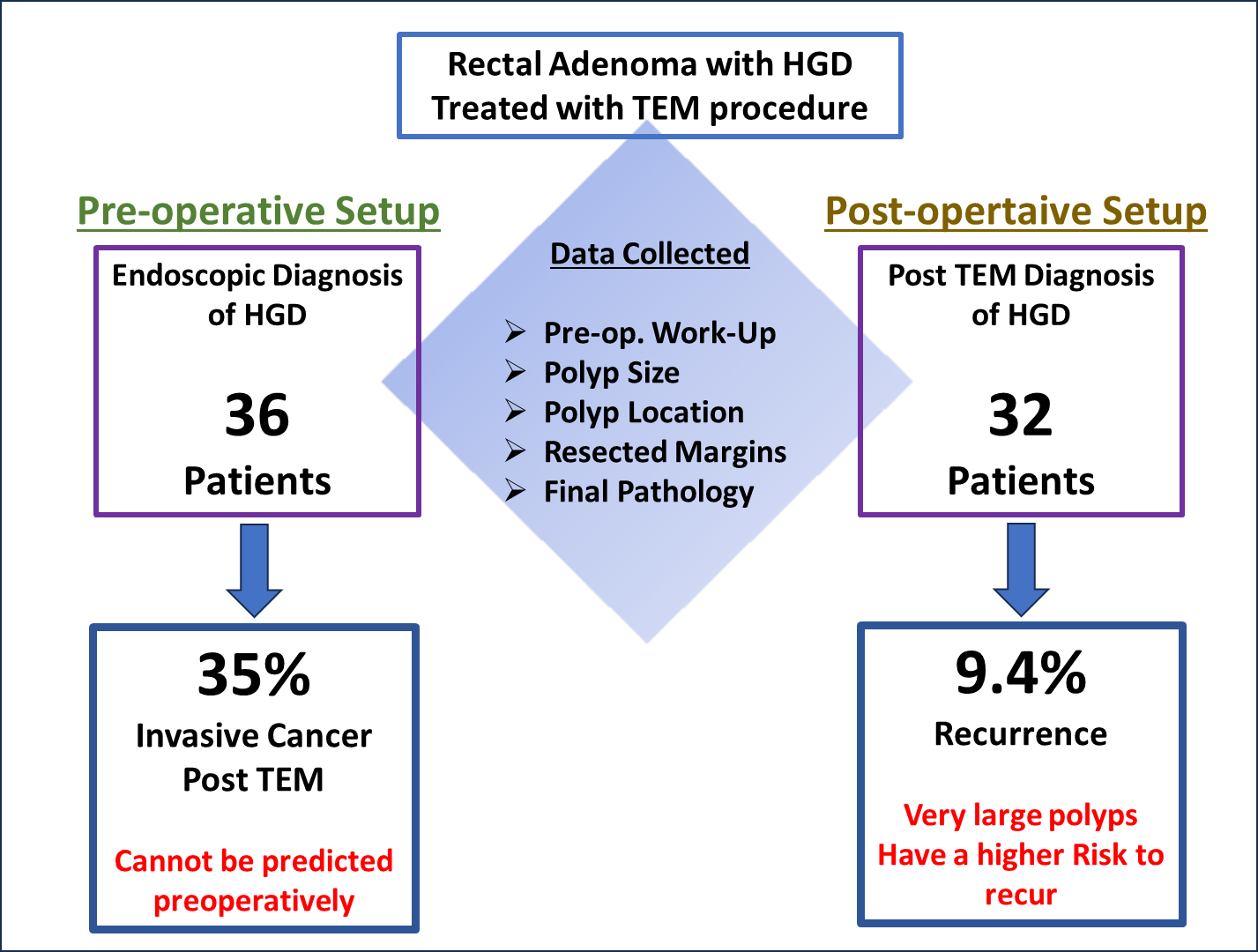
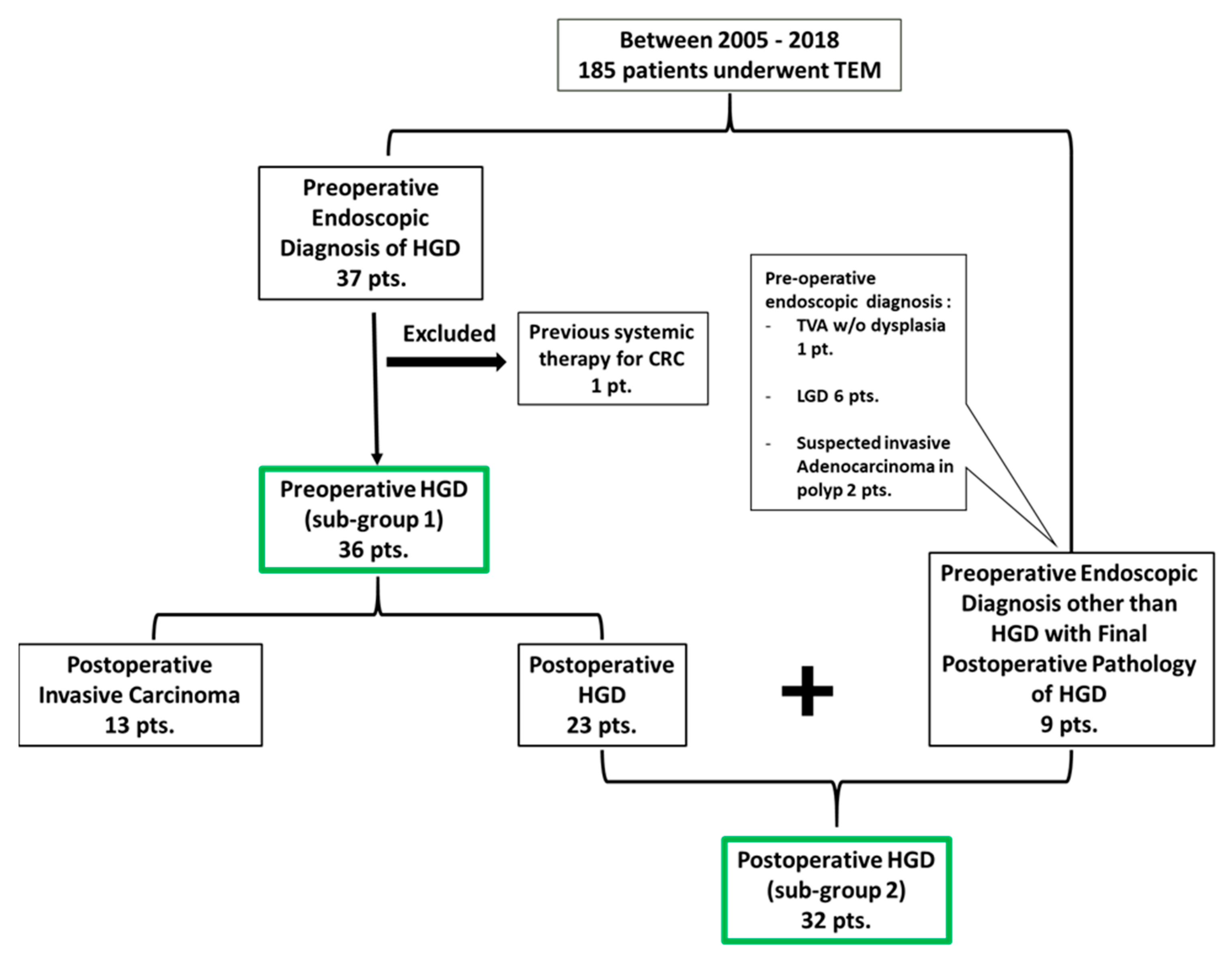
3.1. Preoperative HGD (Sub-Group 1) Analysis
3.2. Postoperative HGD (Sub-Group 2) Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atkin, W.S.; Morson, B.C.; Cuzick, J. Long-term risk of colorectal cancer after excision of rectosigmoid adenomas. N. Engl. J. Med. 1992, 326, 658–662. [Google Scholar] [CrossRef]
- O’Brien, M.J.; Winawer, S.J.; Zauber, A.G.; Gottlieb, L.S.; Sternberg, S.S.; Diaz, B.; Dickersin, G.R.; Ewing, S.; Geller, S.; Kasimian, D. The National Polyp Study. Patient and polyp characteristics associated with high-grade dysplasia in colorectal adenomas. Gastroenterology 1990, 98, 371–379. [Google Scholar]
- Jason, F. Management of Malignant Adenomas. Hall. Clin. Colon. Rectal Surg. 2015, 28, 215–219. [Google Scholar] [CrossRef][Green Version]
- Pigot, F.; Bouchard, D.; Mortaji, M.; Castinel, A.; Juguet, F.; Chaume, J.C.; Faivre, J. Local excision of larger rectal villous adenomas. Dis. Colon. Rectum. 2003, 46, 1345–1350. [Google Scholar] [CrossRef]
- Jahadi, M.R.; Baldwin, A., Jr. Villous adenoma of the colon and rectum. Am. J. Surg. 1975, 130, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Galandiuk, S.; Fazio, V.W.; Jagelman, D.G.; Lavery, I.C.; Weaikiey, F.A.; Petras, R.E.; Badhwar, K.; McGonagle, B.; Eastin, K.; Sutton, T. Villous and tubulovillous adenoma of the colon and rectum. A retrospective review, 1964–1985. Am J Surg. 1987, 153, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.S.; Spencer, R.J. Villous lesions of the colon. Dis. Colon. Rectum. 1978, 21, 493–495. [Google Scholar] [CrossRef]
- Parks, A.G.; Stuart, A.E. The management of villous tumors of the large bowel. Br. J. Surg. 1973, 60, 688–695. [Google Scholar] [CrossRef]
- Morino, M.; Arezzo, A. Transanal Local Excision or Endoscopic Dissection for Benign and Large Lesions of the Rectum. Clin. Colon. Rectal Surg. 2022, 35, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Arezzo, A.; Arolfo, S.; Allaix, M.E.; Bullano, A.; Miegge, A.; Marola, S.; Morino, M. Transanal endoscopic microsurgery for giant circumferential rectal adenomas. Color. Dis. 2016, 18, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Buess, G.; Kipfmüller, K.; Naruhn, M.; Braunstein, S.; Junginger, T. Endoscopic microsurgery of rectal tumors. Endoscopy 1987, 19 (Suppl. 1), 38–42. [Google Scholar] [CrossRef]
- Slater, A.; Betts, M.; Anderson, E.M.; Cunningham, C. Transanal endoscopic microsurgery for rectal cancer. Clin. Radiol. 2016, 71, e121–e129. [Google Scholar] [CrossRef]
- Atallah, S.; Albert, M.; Larach, S. Transanal minimally invasive surgery: A giant leap forward. Surg. Endosc. 2010, 24, 2200–2205. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.R.; Atallah, S.B.; de Beche-Adams, T.C.; Larach, S.W. Transanal Minimally Invasive Surgery (TAMIS) for Local Excision of Benign Neoplasms and Early-stage Rectal Cancer: Efficacy and Outcomes in the First 50 Patients. Dis. Colon. Rectum 2013, 56, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Mellgren, A.; Sirivongs, P.; Rothenberger, D.A.; Madoff, R.D.; García-Aguilar, J. Is local excision adequate therapy for early rectal cancer? Dis. Colon. Rectum. 2000, 43, 1064–1071. [Google Scholar] [CrossRef]
- Lee, W.; Lee, D.; Choi, S.; Chun, H. Transanal endoscopic microsurgery and radical surgery for T1 and T2 rectal cancer. Surg. Endosc. 2003, 17, 1283–1287. [Google Scholar] [CrossRef] [PubMed]
- Winde, G.; Nottberg, H.; Keller, R.; Schmid, K.W.; Bünte, H. Surgical cure for early rectal carcinomas (T1). Dis. Colon. Rectum. 1996, 39, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Dulskas, A.; Kilius, A.; Petrulis, K.; Samalavicius, N.E. Transanal Endoscopic Microsurgery for Patients with Rectal Tumors: A Single Institution’s Experience. Ann. Coloproctol. 2017, 33, 23–27. [Google Scholar] [CrossRef]
- Zorcolo, L.; Fantola, G.; Cabras, F.; Marongiu, L.; D’alia, G.; Casula, G. Preoperative staging of patients with rectal tumors suitable for transanal endoscopic microsurgery (TEM): Comparison of endorectal ultrasound and histopathologic findings. Surg. Endosc. 2009, 23, 1384–1389. [Google Scholar] [CrossRef]
- Doornebosch, P.G.; Bronkhorst, P.J.B.; Hop, W.C.J.; Bode, W.A.; Sing, A.K.; De Graaf, E.J.R. The role of ERUS in therapeutic decision-making for local vs. transabdominal resection of rectal tumours. Dis. Colon. Rectum 2008, 51, 38–42. [Google Scholar] [CrossRef]
- Letarte, F.; Drolet, S.; Laliberté, A.S.; Bouchard, P.; Bouchard, A. Transanal endoscopic microsurgery for rectal villous tumours: Can we rely solely on preoperative biopsies and the surgeon’s experience? Can. J. Surg. 2019, 62, 454–459. [Google Scholar] [CrossRef]
- Affi Koprowski, M.; Lu, K.C. Colorectal Cancer Screening and Postpolypectomy Surveillance. Dis. Colon. Rectum 2021, 64, 932–935. [Google Scholar] [CrossRef]
- Ramirez, J.M.; Aguilella, V.; Gracia, J.A.; Ortego, J.; Escudero, P.; Valencia, J.; Esco, R.; Martinez, M. Local Full-Thickness Excision as First Line Treatment for Sessile Rectal Adenomas. Ann. Surg. 2009, 249, 225–228. [Google Scholar] [CrossRef]
- Scala, A.; Gravante, G.; Dastur, N.; Sorge, R.; Simson, J.N. Transanal Endoscopic Microsurgery in Small, Large, and Giant Rectal Adenomas. Arch. Surg. 2012, 147, 1093–1100. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Olson, R.O., Jr.; Davis, W.C. Villous adenomas of the colon, benign or malignant? Arch. Surg. 1969, 98, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, J.; Kirkegaard, P.; Ibsen, J. Prognosis after treatment of villous adenomas of the colon and rectum. Ann. Surg. 1979, 189, 404–408. [Google Scholar] [PubMed]
- Quan, S.H.; Castro, E.B. Papillary adenomas (villous tumors): A review of 215 cases. Dis. Colon. Rectum. 1971, 14, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Glimelius, B.; Palman, L.; Cervantes, A. Rectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow up. Ann. Oncol. 2010, 21 (Suppl. 5), v82–v86. [Google Scholar] [CrossRef]
- Maeda, K.; Koide, Y.; Katsuno, H. When is local excision appropriate for “early” rectal cancer? Surg. Today 2014, 44, 2000–2014. [Google Scholar] [CrossRef]
- You, Y.N.; Baxter, N.N.; Stewart, A.; Nelson, H. In the increasing rate of local excision for stage 1 rectal cancer in the United States justified? Ann. Surg. 2007, 245, 726–733. [Google Scholar] [CrossRef]
- Baxter, N.N.; Garcia-Aguilar, J. Organ preservation for rectal cancer. J. Clin. Oncol. 2007, 25, 1014–1020. [Google Scholar] [CrossRef]
- Bretagnol, F.; Rullier, E.; George, B.; Warren, B.F.; Mortensen, N.J. Local therapy for rectal cancer: Still controversial? Dis. Colon. Rectum. 2007, 50, 523–533. [Google Scholar] [CrossRef]
- Kaneko, I.; Tanaka, S.; Oka, S.; Kawamura, T.; Hiyama, T.; Ito, M.; Yoshihara, M.; Shimamoto, F.; Chayama, K. Lymphatic vessel dentisty at the site of deepest penetration as a predictor of lymph node metastasis in submucosal colorectal cancer. Dis. Colon. Rectum. 2006, 50, 13–21. [Google Scholar] [CrossRef]
- Borschitz, T.; Wachtlin, D.; Möhler, M.; Schmidberger, H.; Junginger, T. Neoadjuvant chemoradiation and local excision for T2-3 rectal cancer. Ann. Surg. Oncol. 2008, 15, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Hahnloser, D.; Wolff, B.G.; Larson, D.W.; Ping, J.; Nivatvongs, S. Immediate radical resection after local excision of rectal cancer: An oncologic compromise? Dis. Colon. Rectum 2005, 48, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, G.; Newton, T.R.; Bailey, H.R. Local excision of rectal cancer followed by radical surgery because of poor prognostic features does not compromise the long termoncologic outcome. Color. Dis. 2013, 15, e659–e664. [Google Scholar] [CrossRef] [PubMed]
- Bikhchandani, J.; Ong, G.K.; Dozois, E.J.; Mathis, K.L. Outcomes of salvage surgery for cure in patients with locally recurrent disease after local excision of rectal cancer. Dis. Colon. Rectum 2015, 58, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Issa, N.; Fenig, Y.; Gingold-Belfer, R.; Khatib, M.; Khoury, W.; Wolfson, L.; Schmilovitz-Weiss, H. Laparoscopic total mesorectal excision following trans anal endoscopic microsurgery for rectal cancer. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Middleton, P.F.; Sutherland, L.M.; Maddern, G.J. Transanal endoscopic microsurgery: A systematic review. Dis. Colon. Rectum. 2005, 48, 270–284. [Google Scholar] [CrossRef]
- Bretagnol, F.; Merrie, A.; George, B.; Warren, B.F.; Mortensen, N.J. Local excision of rectal tumours by transanal endoscopic microsurgery. Br. J. Surg. 2007, 94, 627–633. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| N = 45 | |
|---|---|
| Age | 69 ± 11 |
| Male | 22 (49) |
| ASA score | |
| 1–2 | 29 (64) |
| 3–4 | 16 (36) |
| Preoperative tumor characteristics | |
| Villous component (n, %) | 25 (55%) |
| Largest dimension (cm) | 3 ± 1.7 (0.6–8) |
| Distance from AV (cm) | 9 ± 3.5 (2–18) |
| Location (%) | |
| Anterior | 12 (27) |
| Posterior | 12 (27) |
| Right | 8 (17) |
| Left | 12 (27) |
| NR | 1 (2) |
| Preoperative imaging (%) | |
| ERUS | 23 (51) |
| CT | 3 (7) |
| MRI | 2 (2) |
| Follow-up, mean, months | 60 ± 52 |
| Preoperative HGD (Sub-Group 1) N = 36 | |
|---|---|
| Final Pathology | Value |
| HGD | 23 (64%) |
| Invasive Carcinoma | 13 (36%) |
| Well Diff. | 11 (85%) |
| Mod Diff. | 2 (15%) |
| Poor Diff | 0 |
| T1 | 9/13 (69%) |
| T2 | 3/13 (23%) |
| T3 | 1/13 (8%) |
| LVI | 0 |
| Mucinous | 3 (23%) |
| Risk of Invasive Carcinoma | p Value |
| Tumor Size > 3 cm | 0.73 |
| Distance from AV < 6 | 1 |
| Villous Component | 0.26 |
| HGD on Final Pathology | Recurrence (n) | p Value |
|---|---|---|
| Tumor Size | ||
| >5 cm | 2 | 0.03 |
| <5 cm | 1 | |
| Margins | ||
| ≤3 mm | 0 | 0.99 |
| >3 mm | 3 | |
| Distance from AV | ||
| ≤6 cm | 2 | 0.18 |
| >6 cm | 1 |
| Patients | Endoscopic Pathology | Final Pathology | Tumor Size | Distance from AV | Margins | Recurrence | Intervention | Follow-up |
|---|---|---|---|---|---|---|---|---|
| Pt. 1 | HGD | HGD | 2 × 1.8 cm | 5 cm | >5 mm | Local recurrence after 12 months, HGD | Re-TEM | No recurrence in 6 years |
| Pt. 2 | HGD | HGD | 7 × 5.5 cm | 10 cm | >5 mm | Local recurrence after 24 months, well-mod. AC | LAR with TME | No recurrence in 5 years |
| Pt. 3 | HGD | HGD | 6 × 5.8 cm | 6 cm | >5 mm | Local recurrence after 60 months, invasive carcinoma | Neoadjuvant CRT followed by TME | Recently lung mets and suspected local recurrence. On biologic treatment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khalifa, M.; Gingold-Belfer, R.; Issa, N. The Outcome of Local Excision of Rectal Adenomas with High-Grade Dysplasia by Transanal Endoscopic Microsurgery: A Single-Center Experience. J. Clin. Med. 2024, 13, 1419. https://doi.org/10.3390/jcm13051419
Khalifa M, Gingold-Belfer R, Issa N. The Outcome of Local Excision of Rectal Adenomas with High-Grade Dysplasia by Transanal Endoscopic Microsurgery: A Single-Center Experience. Journal of Clinical Medicine. 2024; 13(5):1419. https://doi.org/10.3390/jcm13051419
Chicago/Turabian StyleKhalifa, Muhammad, Rachel Gingold-Belfer, and Nidal Issa. 2024. "The Outcome of Local Excision of Rectal Adenomas with High-Grade Dysplasia by Transanal Endoscopic Microsurgery: A Single-Center Experience" Journal of Clinical Medicine 13, no. 5: 1419. https://doi.org/10.3390/jcm13051419
APA StyleKhalifa, M., Gingold-Belfer, R., & Issa, N. (2024). The Outcome of Local Excision of Rectal Adenomas with High-Grade Dysplasia by Transanal Endoscopic Microsurgery: A Single-Center Experience. Journal of Clinical Medicine, 13(5), 1419. https://doi.org/10.3390/jcm13051419