Drawing as a Way of Knowing: How a Mapping Model Assists Preoperative Evaluation of Patients with Thyroid Carcinoma †

 , , ,
, , ,  , , and
, , and
Abstract
1. Introduction
Aim of the Study
- Both the adequacy and accuracy of US exploration of the LN, as they were observed throughout the process of mapping.
- Personal characteristics of the patient that could predict LN malignancy or provide additional information to the US, such as age, sex, and BMI, especially regarding the malignancy of the nodules.
2. Materials and Methods
2.1. Inclusion Criteria
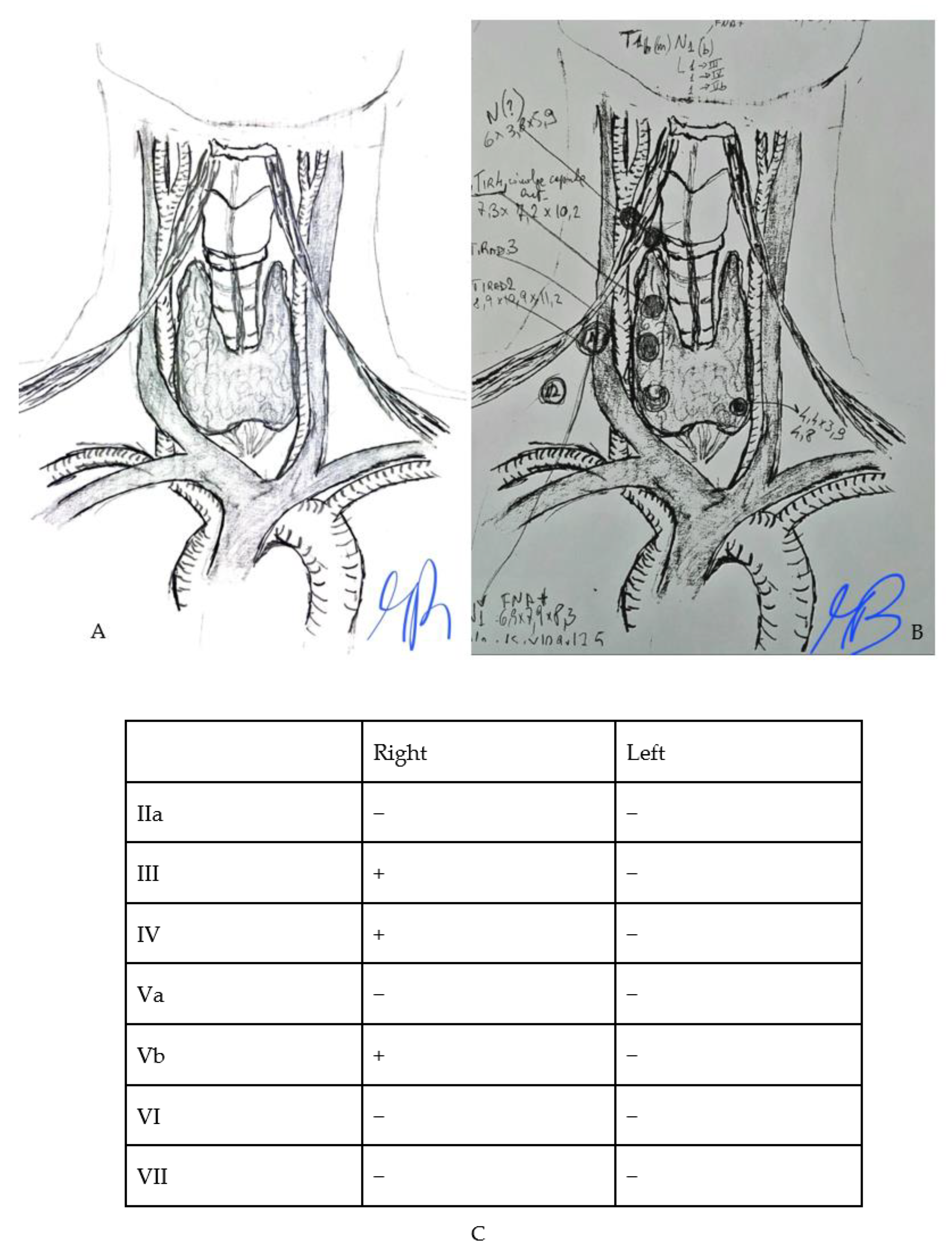
2.2. Preoperative Mapping Procedure
2.3. Thyroid Nodule Evaluation
- -
- Size, expressed in mm.
- -
- Composition.
- -
- Echogenicity.
- -
- Margin.
- -
- Shape/direction of growth.
- -
- Echogenic foci/calcification.
- -
- Extrathyroidal extension.
- -
- Lymph nodes.
2.4. Neck Lymph Nodes Evaluation
- -
- Microcalcifications.
- -
- Partially cystic appearance.
- -
- Peripheral or diffusely increased vascularization.
- -
- Hyperechoic tissue looking like the thyroid [8].
2.5. Data Analysis
3. Results
3.1. Clinical and Pre-Surgical Features
3.2. Results of Preoperative Mapping for Nodular Assessment
- -
- The size of the nodule on which the needle aspiration had been performed.
- -
- The Sonographic features of the needle aspiration nodule.
- -
- Whether a lymph node is suspicious for neoplastic metastasis.
- -
- The size of the major lymph node observed for each lymph node level.
3.3. Results from Performing a Preoperative Mapping and Multivariate Analysis
- -
- Central compartment model: sensitivity (56.0%), specificity (87.3%), and PPV (66.7%) compared with the values obtained from ultrasound mapping alone (sensitivity 45.7%, specificity 95.6%, PPV 84.2%, NPV 77.4%).
- -
- Model of the lateral cervical compartment: sensitivity (33.3%), specificity (95.4%), and PPV (62.5%) compared with values obtained from ultrasound mapping alone (sensitivity 100%, specificity 88.8%, PPV 71.9%, NPV 100%).
4. Discussion
4.1. Our Findings and the Literature
4.2. The Challenge in Diagnosing Carcinoma in Different Compartments of the Thyroid
4.3. Patients’ Characteristics and Whether They Affect the Preoperative Evaluation of Nodal Metastasis
4.4. Strengths of the Study
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, N.; Zhang, X.; Wan, W.; Zhang, C.; Zhang, X. The Preciseness in Diagnosing Thyroid Malignant Nodules Using Shear-Wave Elastography. Med. Sci. Monit. 2018, 24, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.N.; Yip, L.; Lubitz, C.C.; Grubbs, E.G.; Miller, B.S.; Shen, W.; Angelos, P.; Chen, H.; Doherty, G.M.; Fahey, T.J., 3rd; et al. The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults. Ann. Surg. 2020, 271, e21–e93. [Google Scholar] [CrossRef]
- Kumbhar, S.S.; O’Malley, R.B.; Robinson, T.J.; Maximin, S.; Lalwani, N.; Byrd, D.R.; Wang, C.L. Why Thyroid Surgeons Are Frustrated with Radiologists: Lessons Learned from Pre- and Postoperative US. Radiographics 2016, 36, 2141–2153. [Google Scholar] [CrossRef] [PubMed]
- Cisco, R.M.; Shen, W.T.; Gosnell, J.E. Extent of surgery for papillary thyroid cancer: Preoperative imaging and role of prophylactic and therapeutic neck dissection. Curr. Treat. Options Oncol. 2012, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Ji, Y.B.; Sung, E.S.; Park, J.S.; Lee, Y.J.; Park, D.W.; Tae, K. Roles of ultrasonography and computed tomography in the surgical management of cervical lymph node metastases in papillary thyroid carcinoma. Eur. J. Surg. Oncol. 2013, 39, 191–196. [Google Scholar] [CrossRef] [PubMed]
- American Thyroid Association Surgery Working Group; American Association of Endocrine Surgeons; American Academy of Otolaryngology Head and Neck Surgery. Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid 2009, 19, 1153–1158. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Leenhardt, L.; Erdogan, M.F.; Hegedus, L.; Mandel, S.J.; Paschke, R.; Rago, T.; Russ, G. 2013 European thyroid association guidelines for cervical ultrasound scan and ultrasound-guided techniques in the postoperative management of patients with thyroid cancer. Eur. Thyroid. J. 2013, 2, 147–159. [Google Scholar] [CrossRef]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur. Thyroid. J. 2017, 6, 225–237. [Google Scholar] [CrossRef]
- Stack, B.C., Jr.; Ferris, R.L.; Goldenberg, D.; Haymart, M.; Shaha, A.; Sheth, S.; Sosa, J.A.; Tufano, R.P.; American Thyroid Association Surgical Affairs Committee. American Thyroid Association consensus review and statement regarding the anatomy, terminology, and rationale for lateral neck dissection in differentiated thyroid cancer. Thyroid 2012, 22, 501–508. [Google Scholar] [CrossRef]
- Moon, H.J.; Kim, E.K.; Yoon, J.H.; Kwak, J.Y. Differences in the diagnostic performances of staging US for thyroid malignancy according to experience. Ultrasound Med. Biol. 2012, 38, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Ramundo, V.; Di Gioia, C.R.T.; Falcone, R.; Lamartina, L.; Biffoni, M.; Giacomelli, L.; Filetti, S.; Durante, C.; Grani, G. Diagnostic Performance of Neck Ultrasonography in the Preoperative Evaluation for Extrathyroidal Extension of Suspicious Thyroid Nodules. World J. Surg. 2020, 44, 2669–2674. [Google Scholar] [CrossRef] [PubMed]
- Grani, G.; Cera, G.; Conzo, G.; Del Gatto, V.; di Gioia, C.R.T.; Maranghi, M.; Lucia, P.; Cantisani, V.; Metere, A.; Melcarne, R.; et al. Preoperative Ultrasonography in the Evaluation of Suspected Familial Non-Medullary Thyroid Cancer: Are We Able to Predict Multifocality and Extrathyroidal Extension? J. Clin. Med. 2021, 10, 5277. [Google Scholar] [CrossRef] [PubMed]
- Abboud, B.; Smayra, T.; Jabbour, H.; Ghorra, C.; Abadjian, G. Correlations of neck ultrasound and pathology in cervical lymph node of papillary thyroid carcinoma. Acta Chir. Belg. 2020, 120, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, M.; Chen, P.; Tong, J.; Zhang, Y.; Yang, G. Diagnostic performance of ultrasound and computed tomography in parallel for the diagnosis of lymph node metastasis in patients with thyroid cancer: A systematic review and meta-analysis. Gland. Surg. 2022, 11, 1212–1223. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Yan, W.; Zhang, S.; Wu, Y.; Guo, H.; Liang, K.; Xia, W.; Cong, S. Real-Time Elastography: A Web-Based Nomogram Improves the Preoperative Prediction of Central Lymph Node Metastasis in cN0 PTC. Front. Oncol. 2022, 11, 755273. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Li, C.; Tang, S.; Lv, W.; Yi, A.; Wang, B.; Yu, S.; Cui, X.; Dietrich, C.F. Nomogram Based on Shear-Wave Elastography Radiomics Can Improve Preoperative Cervical Lymph Node Staging for Papillary Thyroid Carcinoma. Thyroid 2020, 30, 885–897. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Zhang, Z.; Guo, S.; Zhao, Y.; Zhou, P. Clinical-Radiomics Nomogram Based on Contrast-Enhanced Ultrasound for Preoperative Prediction of Cervical Lymph Node Metastasis in Papillary Thyroid Carcinoma. Cancers 2023, 15, 1613. [Google Scholar] [CrossRef]
- Zhao, H.; Li, H. Meta-analysis of ultrasound for cervical lymph nodes in papillary thyroid cancer: Diagnosis of central and lateral compartment nodal metastases. Eur. J. Radiol. 2019, 112, 14–21. [Google Scholar] [CrossRef]
- Dobrinja, C.; Troian, M.; Cipolat Mis, T.; Rebez, G.; Bernardi, S.; Fabris, B.; Piscopello, L.; Makovac, P.; Di Gregorio, F.; de Manzini, N. Rationality in prophylactic central neck dissection in clinically node-negative (cN0) papillary thyroid carcinoma: Is there anything more to say? A decade experience in a single-center. Int. J. Surg. 2017, 41 (Suppl. S1), S40–S47. [Google Scholar] [CrossRef]
- Said, M.; Fujimoto, M.; Franken, C.; Woo, S.; Vuong, B.; Haigh, P.I. Preferential Use of Total Thyroidectomy without Prophylactic Central Lymph Node Dissection for Early-Stage Papillary Thyroid Cancer: Oncologic Outcomes in an Integrated Health Plan. Perm. J. 2016, 20, 15–251. [Google Scholar] [CrossRef] [PubMed]
- Asimakopoulos, P.; Shaha, A.R.; Nixon, I.J.; Shah, J.P.; Randolph, G.W.; Angelos, P.; Zafereo, M.E.; Kowalski, L.P.; Hartl, D.M.; Olsen, K.D.; et al. Management of the Neck in Well-Differentiated Thyroid Cancer. Curr. Oncol. Rep. 2020, 23, 1. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, X.; Liu, L. Clinical application of carbon nanoparticles suspension in operation of papillary thyroid carcinoma. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2020, 34, 165–169. (In Chinese) [Google Scholar] [CrossRef] [PubMed]
- Huang, N.S.; Chen, J.Y.; Ma, B.; Guo, K.P.; Wang, G.R.; Guan, Q.; Zhao, Z.H.; Wang, W.J.; Zhang, J.S.; Wang, Y.J.; et al. A multicenter prospective study of lateral neck lymph node mapping in papillary thyroid cancer. Gland. Surg. 2023, 12, 1500–1507. [Google Scholar] [CrossRef] [PubMed]
- Díez, J.J.; Galofré, J.C.; Oleaga, A.; Grande, E.; Mitjavila, M.; Moreno, P.; Grupo de Trabajo de Cáncer de Tiroides de la Sociedad Española de Endocrinología y Nutrición. Declaración de consenso para la acreditación de unidades multidisciplinares en cáncer de tiroides [Consensus statement for accreditation of multidisciplinary thyroid cancer units]. Endocrinol. Y Nutr. 2016, 63, e1–e15. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Díez, J.J.; Galofré, J.C.; Oleaga, A.; Grande, E.; Mitjavila, M.; Moreno, P. Characteristics of professionalism of specialists and advantages of multidisciplinary teams in thyroid cancer: Results of a national opinion survey. Endocrinol. Diabetes y Nutr. 2019, 66, 74–82, (In English and Spanish). [Google Scholar] [CrossRef] [PubMed]
- Hong, N.J.; Wright, F.C.; Gagliardi, A.R.; Paszat, L.F. Examining the potential relationship between multidisciplinary cancer care and patient survival: An international literature review. J. Surg. Oncol. 2010, 102, 125–134. [Google Scholar] [CrossRef]
- Kesson, E.M.; Allardice, G.M.; George, W.D.; Burns, H.J.; Morrison, D.S. Effects of multidisciplinary team working on breast cancer survival: Retrospective, comparative, interventional cohort study of 13,722 women. BMJ 2012, 344, e2718. [Google Scholar] [CrossRef]
- Economides, A.; Giannakou, K.; Mamais, I.; Economides, P.A.; Papageorgis, P. Association Between Aggressive Clinicopathologic Features of Papillary Thyroid Carcinoma and Body Mass Index: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2021, 12, 692879. [Google Scholar] [CrossRef]
- Kim, S.H.; Park, H.S.; Kim, K.H.; Yoo, H.; Chae, B.J.; Bae, J.S.; Jung, S.S.; Song, B.J. Correlation between obesity and clinicopathological factors in patients with papillary thyroid cancer. Surg. Today 2015, 45, 723–729. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N. | % | ||
|---|---|---|---|
| Clinical Features | |||
| Gender, male | 26 | 24.80% | |
| Gender, female | 79 | 75.20% | |
| BMI (Classes) | |||
| Normal weight | 52 | 49.50% | |
| Overweight | 38 | 36.20% | |
| Obesity I | 11 | 10.50% | |
| Obesity II | 3 | 2.90% | |
| Obesity III | 1 | 1.00% | |
| Pre-Surgical Citology | |||
| Tir 1 | 1 | 1.00% | |
| Tir 2 | 0 | 0.00% | |
| Tir 3A/B | 38 | 36.20% | |
| Tir 4 | 29 | 27.60% | |
| Tir 5 | 30 | 28.60% | |
| Absent | 7 | 6.70% | |
| Sonographic Features of Main Nodule | |||
| Extrathyroidal extension (ETE) | 35 | 33.30% | |
| Microcalcifications | 31 | 29.50% | |
| Vascularity | Pattern 1 | 6 | 5.70% |
| Pattern 2 | 11 | 10.50% | |
| Pattern 3 | 51 | 48.60% | |
| N/A | 37 | 35.20% | |
| Margins | Defined | 18 | 17.10% |
| Lobulated | 23 | 21.90% | |
| Irregular | 11 | 10.50% | |
| Ragged | 7 | 6.70% | |
| Blurred | 8 | 7.60% | |
| N/A | 38 | 36.20% | |
| Halo | Hypoechogenic | 19 | 18.10% |
| Hyperechogenic | 2 | 1.90% | |
| Not specified | 84 | 80.00% | |
| Hyperechogenic spots | 42 | 40.00% | |
| Composition | Solid | 50 | 47.60% |
| Mixed | 10 | 9.50% | |
| Almost completely solid | 23 | 21.90% | |
| Not specified | 22 | 21.00% | |
| Echogenicity | Hypoechogenic | 57 | 54.30% |
| Hyperechogenic | 2 | 1.90% | |
| Isoecogen | 39 | 37.10% | |
| N/A | 7 | 6.70% | |
| Maximum lymph-nodes size (mm) on US | ||
|---|---|---|
| Right | Left | |
| Level 1 | 19 | 26 |
| Level 2 | 48.5 | 47 |
| Level 3 | 37.3 | 33 |
| Level 4 | 44.5 | 35.4 |
| Level 5 | 17.6 | 42.6 |
| Level 6 | 35.2 | 36.7 |
| Level 7 | 28 | 13 |
| Suspected lymph-nodes (n.) on US | ||
| Yes | No | |
| Lateral-cervical Compartment (LC-LN) | 34 | 71 |
| Central Compartment (CC-LN) | 20 | 85 |
| Level 1 | 1 | 104 |
| Level 2 | 10 | 95 |
| Level 3 | 14 | 91 |
| Level 4 | 25 | 80 |
| Level 5 | 6 | 99 |
| Level 6 | 20 | 85 |
| Level 7 | 2 | 103 |
| Endocrine Surgical Procedures Performed | ||
|---|---|---|
| N. | % | |
| Hemithyroidectomy (HT) | 17 | 16.20% |
| Total Thyroidectomy (TT) | 45 | 42.90% |
| TT + Nodal dissection (ND) | 37 | 35.20% |
| ND | 6 | 5.70% |
| Malignant Histopathology Diagnosis | |||||||
|---|---|---|---|---|---|---|---|
| Number | Multifocality | No Citology | TIR1 | TIR3A/B | TIR4 | TIR5 | |
| PTC | 75 | 37 | 6 | 0 | 15 | 26 | 28 |
|
PTC (incidental nodule) | 2 | 0 | 0 | 0 | 2 | 0 | 0 |
| FTC | 4 | 2 | 0 | 0 | 4 | 0 | 0 |
| MTC | 3 | 1 | 1 | 0 | 0 | 0 | 2 |
| NIFTP * | 4 | 0 | 0 | 0 | 4 | 0 | 0 |
| Histo-pathology features | |||||||
| N. | % | ||||||
| ETE | 46 | 43.80% | |||||
| Muscle Infiltration | 6 | 5.70% | |||||
| Angioinvasion | 13 | 12.40% | |||||
| DIAGNOSTIC PERFORMANCE PREOPERATIVE MAPPING | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Se | IC95% | Sp | IC95% | PPV | IC95% | NPV | IC95% | ||||||
| LC-LN | All Patients | 100% | 85.20% | 100% | 88.80% | 79.70% | 94.70% | 71.90% | 53.30% | 86.25% | 100% | 94.90% | 100% |
| Normal weight | 100% | 69.20% | 100% | 87.50% | 73.20% | 95.80% | 67% | 38.90% | 88.20% | 100% | 90% | 100% | |
| Obesity I | 100% | 15.80% | 100% | 88.90% | 51.80% | 99.70% | 67% | 9.43% | 99.16% | 100% | 63.10% | 100% | |
| Overweight | 100% | 71.50% | 100% | 88.90% | 70.80% | 97.60% | 79% | 49.20% | 95.34% | 100% | 85.75% | 100% | |
| Males | 100% | 75.30% | 100% | 66.70% | 34.90% | 90.10% | 76.47% | 50.10% | 93.19% | 100% | 63.06% | 100% | |
| Females | 100% | 69.20% | 100% | 92.60% | 83.70% | 97.60% | 66.70% | 38.90% | 88.20% | 100% | 94.31% | 100% | |
| Age 20–35 | 100% | 59.00% | 100% | 86.70% | 59.50% | 98.30% | 77.80% | 40% | 97.20% | 100% | 75.30% | 100% | |
| Age 36–60 | 100% | 76.80% | 100% | 87.80% | 73.80% | 95.90% | 73.70% | 49% | 90.10% | 100% | 90.30% | 100% | |
| Age > 60 | 100% | 15.80% | 100% | 91.30% | 72.00% | 98.90% | 50% | 6.80% | 93.24% | 100% | 83.90% | 100% | |
| CC-LN | All Patients | 45.70% | 28.80% | 63.40% | 95.60% | 87.60% | 99.10% | 84.20% | 60.42% | 96.62% | 77.40% | 67% | 86% |
| Normal weight | 33.30% | 13.30% | 59.00% | 96.90% | 83.80% | 99.90% | 85.71% | 42.12% | 99.64% | 72.10% | 56.33% | 84.70% | |
| Obesity I class | 0.00% | 0.00% | 84.20% | 88.90% | 51.80% | 99.70% | 0.00% | 0.00% | 97.50% | 80.00% | 44.40% | 97.50% | |
| Overweight | 71.40% | 41.90% | 91.60% | 95.80% | 78.90% | 99.90% | 91% | 59% | 99.77% | 85% | 66.30% | 95.80% | |
| Males | 76.90% | 46.20% | 95.00% | 75.00% | 42.80% | 94.50% | 76.92% | 46.20% | 94.96% | 75% | 42.81% | 94.51% | |
| Females | 27.30% | 10.70% | 50.20% | 100% | 93.60% | 100% | 100% | 54.07% | 100% | 77.80% | 66.44% | 86.73% | |
| Age 20–35 | 40.00% | 16.30% | 67.70% | 85.70% | 42.10% | 99.60% | 85.70% | 42.13% | 99.64% | 40% | 16.34% | 67.71% | |
| Age 36–60 | 55.60% | 30.80% | 78.50% | 100% | 90.50% | 100% | 100% | 69.15% | 100% | 82.22% | 67.95% | 92% | |
| Age > 60 | 0.00% | 0.00% | 84.20% | 91.30% | 72.00% | 98.90% | 0% | 0% | 84.20% | 91.30% | 71.96% | 98.93% | |
| MULTIVARIATE ANALYSIS CC-LN | ||||
|---|---|---|---|---|
| COEFFICIENTS | Estimate | p Value | Lower Bound (O.R.s.) | Upper Bound (O.R.s.) |
| (Intercept) | −15.332 | 0.995 | 0 | ∞ |
| BMI | −0.01 | 0.885 | 0.868 | 1.13 |
| Cytology (Tir 4) | 15.547 | 0.995 | 0 | ∞ |
| Cytology (Tir 5) | 16.657 | 0.994 | 0 | ∞ |
| Cytology (Tir 3A) | 14.859 | 0.995 | 0 | ∞ |
| Cytology (Tir 3B) | 14.614 | 0.995 | 0 | ∞ |
| Maximum FNAB lymph nodes size (mm) on US | 0.009 | 0.742 | 0.957 | 1.063 |
| Hypoechogenic | −0.846 | 0.183 | 0.123 | 1.491 |
| Hyperechogenic | −15.353 | 0.995 | 0 | ∞ |
| Hyperechogenic spot | −0.363 | 0.517 | 0.232 | 2.086 |
| Mixed composition | 0.267 | 0.763 | 0.23 | 7.407 |
| Solid composition | −1.583 | 0.051 | 0.042 | 1.006 |
| MULTIVARIATE ANALYSIS LC-LN | ||||
| COEFFICIENTS | Estimate | p Value | Lower Bound (O.R.s.) | Upper Bound (O.R.s.) |
| (Intercept) | −17.346 | 0.998 | 0 | ∞ |
| BMI | −0.032 | 0.689 | 0.826 | 1.134 |
| Cytology (Tir 4) | 15.912 | 0.998 | 0 | ∞ |
| Cytology (Tir 5) | 18.14 | 0.998 | 0 | ∞ |
| Cytology (Tir 3A) | 0.166 | 1 | 0 | ∞ |
| Cytology (Tir 3B) | 16.466 | 0.998 | 0 | ∞ |
| Maximum FNAB lymph nodes size (mm) on US | 0.018 | 0.553 | 0.959 | 1.082 |
| Hypoechogenic | −0.111 | 0.878 | 0.219 | 3.66 |
| Hyperechogenic | −16.346 | 0.998 | 0 | ∞ |
| Hyperechogenic spot | −0.745 | 0.264 | 0.129 | 1.754 |
| Mixed composition | 0.567 | 0.594 | 0.219 | 14.192 |
| Solid composition | −1.107 | 0.225 | 0.055 | 1.976 |
| PERFORMANCE METRICS LC-LN | ||||
| Accuracy | 0.838 | |||
| AUC | 0.803 | |||
| Sensitivity | 0.333 | |||
| Specificity | 0.954 | |||
| Precision | 0.625 | |||
| PERFORMANCE METRICS CC-LN | ||||
| Accuracy | 0.775 | |||
| AUC | 0.775 | |||
| Sensitivity | 0.56 | |||
| Specificity | 0.873 | |||
| Precision | 0.667 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biffoni, M.; Grani, G.; Melcarne, R.; Geronzi, V.; Consorti, F.; Ruggieri, G.D.; Galvano, A.; Razlighi, M.H.; Iannuzzi, E.; Engel, T.D.; et al. Drawing as a Way of Knowing: How a Mapping Model Assists Preoperative Evaluation of Patients with Thyroid Carcinoma. J. Clin. Med. 2024, 13, 1389. https://doi.org/10.3390/jcm13051389
Biffoni M, Grani G, Melcarne R, Geronzi V, Consorti F, Ruggieri GD, Galvano A, Razlighi MH, Iannuzzi E, Engel TD, et al. Drawing as a Way of Knowing: How a Mapping Model Assists Preoperative Evaluation of Patients with Thyroid Carcinoma. Journal of Clinical Medicine. 2024; 13(5):1389. https://doi.org/10.3390/jcm13051389
Chicago/Turabian StyleBiffoni, Marco, Giorgio Grani, Rossella Melcarne, Valerio Geronzi, Fabrizio Consorti, Giuseppe De Ruggieri, Alessia Galvano, Maryam Hosseinpour Razlighi, Eva Iannuzzi, Tal Deborah Engel, and et al. 2024. "Drawing as a Way of Knowing: How a Mapping Model Assists Preoperative Evaluation of Patients with Thyroid Carcinoma" Journal of Clinical Medicine 13, no. 5: 1389. https://doi.org/10.3390/jcm13051389
APA StyleBiffoni, M., Grani, G., Melcarne, R., Geronzi, V., Consorti, F., Ruggieri, G. D., Galvano, A., Razlighi, M. H., Iannuzzi, E., Engel, T. D., Pace, D., Di Gioia, C. R. T., Boniardi, M., Durante, C., & Giacomelli, L. (2024). Drawing as a Way of Knowing: How a Mapping Model Assists Preoperative Evaluation of Patients with Thyroid Carcinoma. Journal of Clinical Medicine, 13(5), 1389. https://doi.org/10.3390/jcm13051389