
Role of Transjugular Intrahepatic Portosystemic Shunt in the Liver Transplant Setting

 , , and
, , and 
{kind=link}
{kind=link}
Abstract
1. Introduction
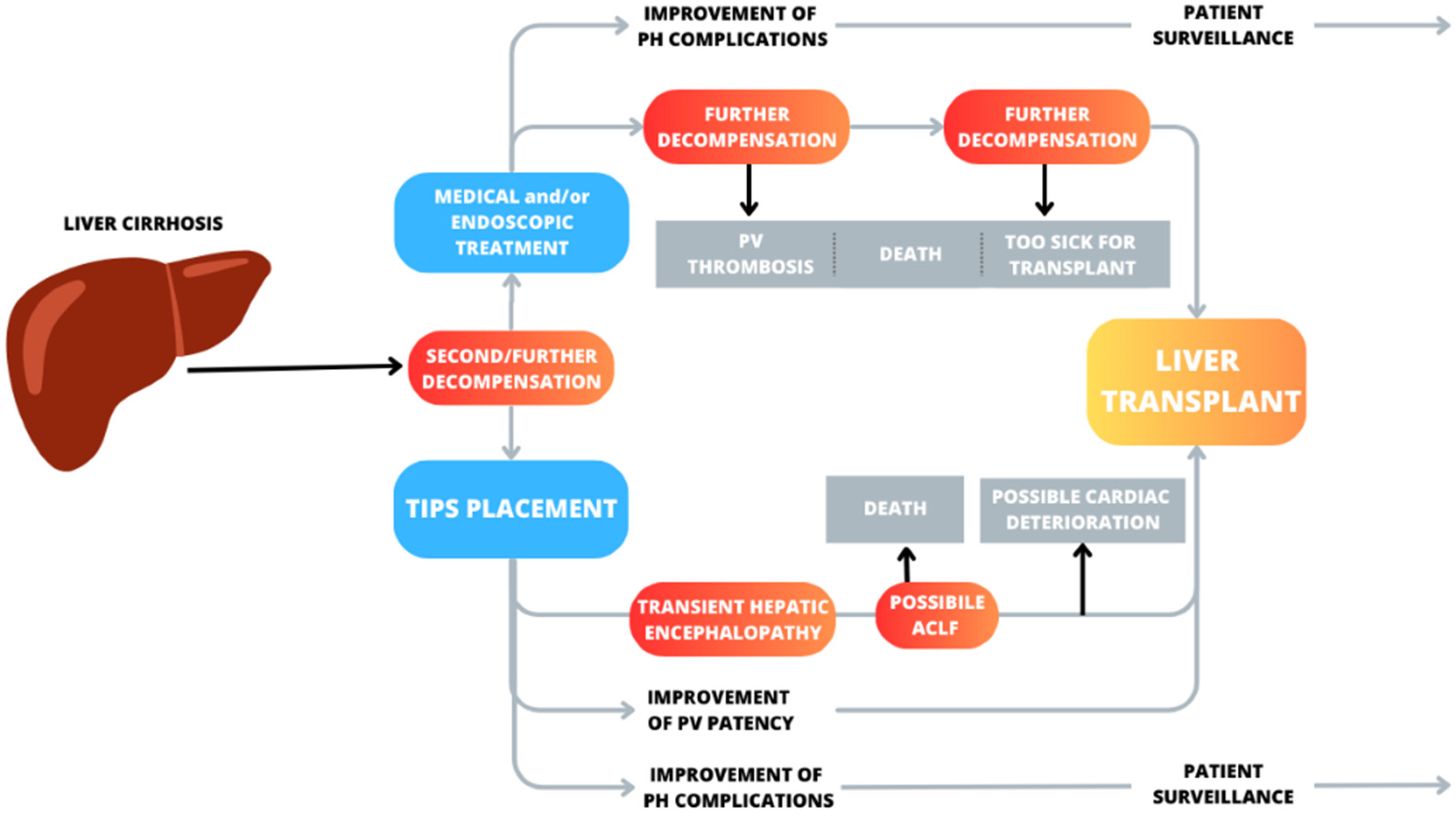
2. TIPS toward Liver Transplant: Role and Timing
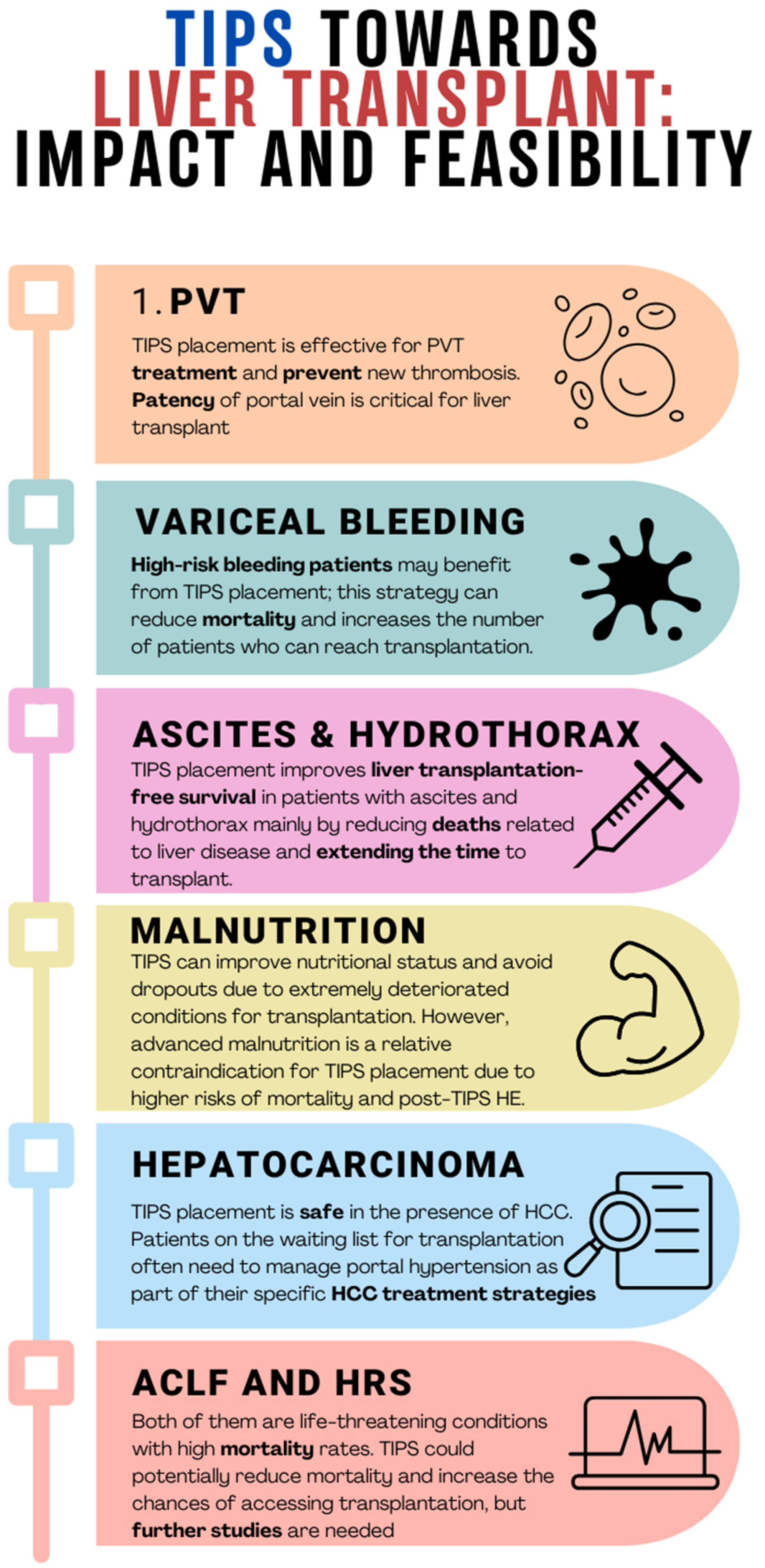
3. TIPS in “Special” Liver Transplant Settings
3.1. Hepatocellular Carcinoma (HCC)
3.2. Acute-on-Chronic Liver Failure (ACLF)
3.3. Hepatorenal Syndrome
3.4. Cirrhotic Cardiomyopathy
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 1 December 2023).
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Morabito, A.; D’Amico, M.; Pasta, L.; Malizia, G.; Rebora, P.; Valsecchi, M.G. Clinical states of cirrhosis and competing risks. J. Hepatol. 2018, 68, 563–576. [Google Scholar] [CrossRef] [PubMed]
- Rudler, M.; Mallet, M.; Sultanik, P.; Bouzbib, C.; Thabut, D. Optimal management of ascites. Liver Int. 2020, 40 (Suppl. 1), 128–135, Erratum in Liver Int. 2020, 40, 1247. [Google Scholar] [CrossRef] [PubMed]
- Jakab, S.S.; Garcia-Tsao, G. Evaluation and Management of Esophageal and Gastric Varices in Patients with Cirrhosis. Clin. Liver Dis. 2020, 24, 335–350. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Durham, J. Evolving Indications for Tips. Tech. Vasc. Interv. Radiol. 2016, 19, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Larrue, H.; D’Amico, G.; Olivas, P.; Lv, Y.; Bucsics, T.; Rudler, M.; Sauerbruch, T.; Hernandez-Gea, V.; Han, G.; Reiberger, T.; et al. TIPS prevents further decompensation and improves survival in patients with cirrhosis and portal hypertension in an individual patient data meta-analysis. J. Hepatol. 2023, 79, 692–703. [Google Scholar] [CrossRef] [PubMed]
- Bodzin, A.S.; Baker, T.B. Liver Transplantation Today: Where We Are Now and Where We Are Going. Liver Transplant. 2018, 24, 1470–1475. [Google Scholar] [CrossRef]
- De Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Baveno VII Faculty. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef]
- Tripathi, D.; Stanley, A.J.; Hayes, P.C.; Travis, S.; Armstrong, M.J.; Tsochatzis, E.A.; Rowe, I.A.; Roslund, N.; Ireland, H.; Lomax, M.; et al. Transjugular intrahepatic portosystemic stent-shunt in the management of portal hypertension. Gut 2020, 69, 1173–1192. [Google Scholar] [CrossRef]
- Villanueva, C.; Torres, F.; Sarin, S.K.; Shah, H.A.; Tripathi, D.; Brujats, A.; Rodrigues, S.G.; Bhardwaj, A.; Azam, Z.; Hayes, P.C.; et al. Carvedilol reduces the risk of decompensation and mortality in patients with compensated cirrhosis in a competing-risk meta-analysis. J. Hepatol. 2022, 77, 1014–1025. [Google Scholar] [CrossRef]
- Delacôte, C.; Favre, M.; El Amrani, M.; Ningarhari, M.; Lemaitre, E.; Ntandja-Wandji, L.C.; Bauvin, P.; Boleslawski, E.; Millet, G.; Truant, S.; et al. Morbid obesity increases death and dropout from the liver transplantation waiting list: A prospective cohort study. United Eur. Gastroenterol. J. 2022, 10, 396–408. [Google Scholar] [CrossRef] [PubMed]
- Montenovo, M.; Rahnemai-Azar, A.; Reyes, J.; Perkins, J. Clinical Impact and Risk Factors of Portal Vein Thrombosis for Patients on Wait List for Liver Transplant. Exp. Clin. Transplant. 2018, 16, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Ponziani, F.R.; Zocco, M.A.; Senzolo, M.; Pompili, M.; Gasbarrini, A.; Avolio, A.W. Portal vein thrombosis and liver transplantation: Implications for waiting list period, surgical approach, early and late follow-up. Transplant. Rev. 2014, 28, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Stine, J.G.; Shah, P.M.; Cornella, S.L.; Rudnick, S.R.; Ghabril, M.S.; Stukenborg, G.J.; Northup, P.G. Portal vein thrombosis, mortality and hepatic decompensation in patients with cirrhosis: A meta-analysis. World J. Hepatol. 2015, 7, 2774–2780. [Google Scholar] [CrossRef] [PubMed]
- Ghabril, M.; Agarwal, S.; Lacerda, M.; Chalasani, N.; Kwo, P.; Tector, A.J. Portal Vein Thrombosis Is a Risk Factor for Poor Early Outcomes after Liver Transplantation: Analysis of Risk Factors and Outcomes for Portal Vein Thrombosis in Waitlisted Patients. Transplantation 2016, 100, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Englesbe, M.J.; Kubus, J.; Muhammad, W.; Sonnenday, C.J.; Welling, T.; Punch, J.D.; Lynch, R.J.; Marrero, J.A.; Pelletier, S.J. Portal vein thrombosis and survival in patients with cirrhosis. Liver Transpl. 2010, 16, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Thornburg, B.; Desai, K.; Hickey, R.; Kulik, L.; Ganger, D.; Baker, T.; Abecassis, M.; Lewandowski, R.J.; Salem, R. Portal Vein Recanalization and Transjugular Intrahepatic Portosystemic Shunt Creation for Chronic Portal Vein Thrombosis: Technical Considerations. Tech. Vasc. Interv. Radiol. 2016, 19, 52–60. [Google Scholar] [CrossRef]
- Salem, R.; Vouche, M.; Baker, T.; Herrero, J.I.; Caicedo, J.C.; Fryer, J.; Hickey, R.; Habib, A.; Abecassis, M.; Koller, F.; et al. Pretransplant Portal Vein Recanalization-Transjugular Intrahepatic Portosystemic Shunt in Patients with Complete Obliterative Portal Vein Thrombosis. Transplantation 2015, 99, 2347–2355. [Google Scholar] [CrossRef]
- Lv, Y.; Qi, X.; He, C.; Wang, Z.; Yin, Z.; Niu, J.; Guo, W.; Bai, W.; Zhang, H.; Xie, H.; et al. Covered TIPS versus endoscopic band ligation plus propranolol for the prevention of variceal rebleeding in cirrhotic patients with portal vein thrombosis: A randomised controlled trial. Gut 2018, 67, 2156–2168. [Google Scholar] [CrossRef]
- Davis, J.P.E.; Ogurick, A.G.; Rothermel, C.E.; Sohn, M.W.; Intagliata, N.M.; Northup, P.G. Anticoagulation and Transjugular Intrahepatic Portosystemic Shunting for Treatment of Portal Vein Thrombosis in Cirrhosis: A Systematic Review and Meta-Analysis. Clin. Appl. Thromb./Hemost. 2019, 25, 1076029619888026. [Google Scholar] [CrossRef]
- Lv, Y.; Bai, W.; Li, K.; Wang, Z.; Guo, W.; Luo, B.; Wang, J.; Wang, Q.; Wang, E.; Xia, D.; et al. Anticoagulation and Transjugular Intrahepatic Portosystemic Shunt for the Management of Portal Vein Thrombosis in Cirrhosis: A Prospective Observational Study. Am. J. Gastroenterol. 2022, 116, 1447–1464, Erratum in Am. J. Gastroenterol. 2022, 117, 200. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.G.; Sixt, S.; Abraldes, J.G.; De Gottardi, A.; Klinger, C.; Bosch, J.; Baumgartner, I.; Berzigotti, A. Systematic review with meta-analysis: Portal vein recanalisation and transjugular intrahepatic portosystemic shunt for portal vein thrombosis. Aliment. Pharmacol. Ther. 2019, 49, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.W.; Eghtesad, B.; Garcia-Tsao, G.; Haskal, Z.J.; Hernandez-Gea, V.; Jalaeian, H.; Kalva, S.P.; Mohanty, A.; Thabut, D.; Abraldes, J.G. AASLD Practice Guidance on the use of TIPS, variceal embolization, and retrograde transvenous obliteration in the management of variceal hemorrhage. Hepatology 2024, 79, 224–250. [Google Scholar] [CrossRef] [PubMed]
- Asrani, S.K.; Kamath, P.S. Natural history of cirrhosis. Curr. Gastroenterol. Rep. 2013, 15, 308. [Google Scholar] [CrossRef] [PubMed]
- Monescillo, A.; Martínez-Lagares, F.; Ruiz-del-Arbol, L.; Sierra, A.; Guevara, C.; Jiménez, E.; Marrero, J.M.; Buceta, E.; Sánchez, J.; Castellot, A.; et al. Influence of portal hypertension and its early decompression by TIPS placement on the outcome of variceal bleeding. Hepatology 2004, 40, 793–801. [Google Scholar] [CrossRef] [PubMed]
- García-Pagán, J.C.; Caca, K.; Bureau, C.; Laleman, W.; Appenrodt, B.; Luca, A.; Abraldes, J.G.; Nevens, F.; Vinel, J.P.; Mössner, J.; et al. Early use of TIPS in patients with cirrhosis and variceal bleeding. N. Engl. J. Med. 2010, 362, 2370–2379. [Google Scholar] [CrossRef] [PubMed]
- Manning, C.; Elzubeir, A.; Alam, S. The role of pre-emptive Transjugular Intrahepatic Portosystemic Shunt in acute variceal bleeding: A literature review. Ther. Adv. Chronic Dis. 2021, 12, 2040622321995771. [Google Scholar] [CrossRef]
- Hussain, I.; Wong, Y.J.; Lohan, R.; Lin, S.; Kumar, R. Does preemptive transjugular intrahepatic portosystemic shunt improve survival after acute variceal bleeding? Systematic review, meta-analysis, and trial sequential analysis of randomized trials. J. Gastroenterol. Hepatol. 2022, 37, 455–463. [Google Scholar] [CrossRef]
- Nicoară-Farcău, O.; Han, G.; Rudler, M.; Angrisani, D.; Monescillo, A.; Torres, F.; Casanovas, G.; Bosch, J.; Lv, Y.; Thabut, D.; et al. Effects of Early Placement of Transjugular Portosystemic Shunts in Patients with High-Risk Acute Variceal Bleeding: A Meta-analysis of Individual Patient Data. Gastroenterology 2021, 160, 193–205.e10. [Google Scholar] [CrossRef]
- Arroyo, V.; Colmenero, J. Ascites and hepatorenal syndrome in cirrhosis: Pathophysiological basis of therapy and current management. J. Hepatol. 2003, 38 (Suppl. 1), S69–S89. [Google Scholar] [CrossRef]
- Ginès, P.; Uriz, J.; Calahorra, B.; Garcia-Tsao, G.; Kamath, P.S.; Del Arbol, L.R.; Planas, R.; Bosch, J.; Arroyo, V.; Rodés, J. Transjugular intrahepatic portosystemic shunting versus paracentesis plus albumin for refractory ascites in cirrhosis. Gastroenterology 2002, 123, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Narahara, Y.; Kanazawa, H.; Fukuda, T.; Matsushita, Y.; Harimoto, H.; Kidokoro, H.; Katakura, T.; Atsukawa, M.; Taki, Y.; Kimura, Y.; et al. Transjugular intrahepatic portosystemic shunt versus paracentesis plus albumin in patients with refractory ascites who have good hepatic and renal function: A prospective randomized trial. J. Gastroenterol. 2011, 46, 78–85. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Luca, A.; Morabito, A.; Miraglia, R.; D’Amico, M. Uncovered transjugular intrahepatic portosystemic shunt for refractory ascites: A meta-analysis. Gastroenterology 2005, 129, 1282–1293. [Google Scholar] [CrossRef] [PubMed]
- Salerno, F.; Cammà, C.; Enea, M.; Rössle, M.; Wong, F. Transjugular intrahepatic portosystemic shunt for refractory ascites: A meta-analysis of individual patient data. Gastroenterology 2007, 133, 825–834, Erratum in Gastroenterology 2007, 133, 1746. [Google Scholar] [CrossRef] [PubMed]
- Bai, M.; Qi, X.S.; Yang, Z.P.; Yang, M.; Fan, D.M.; Han, G.H. TIPS improves liver transplantation-free survival in cirrhotic patients with refractory ascites: An updated meta-analysis. World J. Gastroenterol. 2014, 20, 2704–2714. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Genning, C.; Reddy, K.R.; Wong, F.; Kowdley, K.V.; Benner, K.; McCashland, T.; North American Study for the Treatment of Refractory Ascites Group. The North American Study for the Treatment of Refractory Ascites. Gastroenterology 2003, 124, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Salerno, F.; Cazzaniga, M.; Pagnozzi, G.; Cirello, I.; Nicolini, A.; Meregaglia, D.; Burdick, L. Humoral and cardiac effects of TIPS in cirrhotic patients with different “effective” blood volume. Hepatology 2003, 38, 1370–1377. [Google Scholar] [CrossRef]
- Gaba, R.C.; Parvinian, A.; Casadaban, L.C.; Couture, P.M.; Zivin, S.P.; Lakhoo, J.; Minocha, J.; Ray, C.E., Jr.; Knuttinen, M.G.; Bui, J.T. Survival benefit of TIPS versus serial paracentesis in patients with refractory ascites: A single institution case-control propensity score analysis. Clin. Radiol. 2015, 70, e51–e57. [Google Scholar] [CrossRef]
- Ronald, J.; Rao, R.; Choi, S.S.; Kappus, M.; Martin, J.G.; Sag, A.A.; Pabon-Ramos, W.M.; Suhocki, P.V.; Smith, T.P.; Kim, C.Y. No Increased Mortality After TIPS Compared with Serial Large Volume Paracenteses in Patients with Higher Model for End-Stage Liver Disease Score and Refractory Ascites. Cardiovasc. Interv. Radiol. 2019, 42, 720–728. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Plauth, M. ESPEN practical guideline: Clinical nutrition in liver disease. Clin. Nutr. 2020, 39, 3533–3562. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Bemeur, C.; Butterworth, R.; Cordoba, J.; Kato, A.; Montagnese, S.; Uribe, M.; Vilstrup, H.; Morgan, M.Y. The nutritional management of hepatic encephalopathy in patients with cirrhosis: International Society for Hepatic Encephalopathy and Nitrogen Metabolism Consensus. Hepatology 2013, 58, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Giusto, M.; Molfino, A.; Bonetto, A.; Rossi, M.; Ginanni Corradini, S.; Baccino, F.M.; Rossi Fanelli, F.; Costelli, P.; Muscaritoli, M. MuRF-1 and p-GSK3β expression in muscle atrophy of cirrhosis. Liver Int. 2013, 33, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kang, S.H.; Kim, M.Y.; Baik, S.K. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186990. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, B.; Nardelli, S.; Pigliacelli, A.; Di Cola, S.; Farcomeni, A.; D’Ambrosio, D.; Gioia, S.; Ginanni Corradini, S.; Lucidi, C.; Mennini, G.; et al. The additive value of sarcopenia, myosteatosis and hepatic encephalopathy in the predictivity of model for end-stage liver disease. Dig. Liver Dis. 2019, 51, 1508–1512. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Giusto, M.; Giannelli, V.; Lucidi, C.; Riggio, O. Nutritional status and liver transplantation. J. Clin. Exp. Hepatol. 2011, 1, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Mangana Del Rio, T.; Sacleux, S.C.; Vionnet, J.; Ichaï, P.; Denys, A.; Schneider, A.; Coilly, A.; Fraga, M.; Wetzel, A.; Koerfer, J.; et al. Body composition and short-term mortality in patients critically ill with acute-on-chronic liver failure. JHEP Rep. 2023, 5, 100758. [Google Scholar] [CrossRef]
- Nardelli, S.; Lattanzi, B.; Torrisi, S.; Greco, F.; Farcomeni, A.; Gioia, S.; Merli, M.; Riggio, O. Sarcopenia Is Risk Factor for Development of Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt Placement. Clin. Gastroenterol. Hepatol. 2017, 15, 934–936. [Google Scholar] [CrossRef]
- Praktiknjo, M.; Clees, C.; Pigliacelli, A.; Fischer, S.; Jansen, C.; Lehmann, J.; Pohlmann, A.; Lattanzi, B.; Krabbe, V.K.; Strassburg, C.P.; et al. Sarcopenia Is Associated with Development of Acute-on-Chronic Liver Failure in Decompensated Liver Cirrhosis Receiving Transjugular Intrahepatic Portosystemic Shunt. Clin. Transl. Gastroenterol. 2019, 10, e00025. [Google Scholar] [CrossRef]
- Gazda, J.; Di Cola, S.; Lapenna, L.; Khan, S.; Merli, M. The Impact of Transjugular Intrahepatic Portosystemic Shunt on Nutrition in Liver Cirrhosis Patients: A Systematic Review. Nutrients 2023, 15, 1617. [Google Scholar] [CrossRef]
- Montomoli, J.; Holland-Fischer, P.; Bianchi, G.; Grønbaek, H.; Vilstrup, H.; Marchesini, G.; Zoli, M. Body composition changes after transjugular intrahepatic portosystemic shunt in patients with cirrhosis. World J. Gastroenterol. 2010, 16, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Bañares, R.; Albillos, A.; Nakum, M.; Gea, S.; Varghese, A.; Green, W. An Economic Analysis of Transjugular Intrahepatic Portosystemic Covered Stent Shunt for Variceal Bleeding and Refractory Ascites in a Spanish Setting. Adv. Ther. 2023, 40, 3006–3020. [Google Scholar] [CrossRef] [PubMed]
- Casadaban, L.C.; Parvinian, A.; Couture, P.M.; Minocha, J.; Knuttinen, M.G.; Bui, J.T.; Gaba, R.C. Characterization of liver function parameter alterations after transjugular intrahepatic portosystemic shunt creation and association with early mortality. AJR Am. J. Roentgenol. 2014, 203, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Vizzutti, F.; Arena, U.; Rega, L.; Zipoli, M.; Abraldes, J.G.; Romanelli, R.G.; Tarquini, R.; Laffi, G.; Pinzani, M. Liver failure complicating segmental hepatic ischaemia induced by a PTFE-coated TIPS stent. Gut 2009, 58, 582–584. [Google Scholar] [CrossRef] [PubMed]
- Cazzaniga, M.; Salerno, F.; Pagnozzi, G.; Dionigi, E.; Visentin, S.; Cirello, I.; Meregaglia, D.; Nicolini, A. Diastolic dysfunction is associated with poor survival in patients with cirrhosis with transjugular intrahepatic portosystemic shunt. Gut 2007, 56, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Billey, C.; Billet, S.; Robic, M.A.; Cognet, T.; Guillaume, M.; Vinel, J.P.; Péron, J.M.; Lairez, o.; Bureau, C. A prospective study identifying predictive factors of cardiac decompensation after TIPS: The Toulouse algorithm. Hepatology 2019, 70, 1928–1941. [Google Scholar] [CrossRef] [PubMed]
- Riggio, O.; Angeloni, S.; Salvatori, F.M.; De Santis, A.; Cerini, F.; Farcomeni, A.; Attili, A.F.; Merli, M. Incidence, natural history, and risk factors of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt with polytetrafluoroethylene-covered stent grafts. Am. J. Gastroenterol. 2008, 103, 2738–2746. [Google Scholar] [CrossRef]
- Riggio, O.; Nardelli, S.; Moscucci, F.; Pasquale, C.; Ridola, L.; Merli, M. Hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Clin. Liver Dis. 2012, 16, 133–146. [Google Scholar] [CrossRef]
- Bureau, C.; Thabut, D.; Jezequel, C.; Archambeaud, I.; D’Alteroche, L.; Dharancy, S.; Borentain, P.; Oberti, F.; Plessier, A.; De Ledinghen, V.; et al. The Use of Rifaximin in the Prevention of Overt Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt: A Randomized Controlled Trial. Ann. Intern. Med. 2021, 174, 633–640. [Google Scholar] [CrossRef]
- Nardelli, S. Hepatic encephalopathy after transjugular intrahepatic portosystemic shunt does not increase mortality in patients with cirrhosis. In Proceedings of the EASL Congress 2023, Vienna, Austria, 21–24 June 2023. [Google Scholar]
- Unger, L.W.; Stork, T.; Bucsics, T.; Rasoul-Rockenschaub, S.; Staufer, K.; Trauner, M.; Maschke, S.; Pawloff, M.; Soliman, T.; Reiberger, T.; et al. The role of TIPS in the management of liver transplant candidates. United Eur. Gastroenterol. J. 2017, 5, 1100–1107. [Google Scholar] [CrossRef]
- Freeman, R.B., Jr.; FitzMaurice, S.E.; Greenfield, A.E.; Halin, N.; Haug, C.E.; Rohrer, R.J. Is the transjugular intrahepatic portocaval shunt procedure beneficial for liver transplant recipients? Transplantation 1994, 58, 297–300, Erratum in Transplantation 1994, 58, 1144. [Google Scholar] [CrossRef] [PubMed]
- Menegaux, F.; Baker, E.; Keeffe, E.B.; Monge, H.; Egawa, H.; Esquivel, C.O. Impact of transjugular intrahepatic portosystemic shunt on orthotopic liver transplantation. World J. Surg. 1994, 18, 866–870, discussion 870–871. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Zajko, A.B.; Orons, P.D.; Dodd, G.; Wright, H.; Colangelo, J.; Tartar, R. Transjugular intrahepatic portosystemic shunt in the management of variceal bleeding: Indications and clinical results. Surgery 1993, 114, 719–726, discussion 726–727. [Google Scholar] [PubMed]
- Woodle, E.S.; Darcy, M.; White, H.M.; Perdrizet, G.A.; Vesely, T.M.; Picus, D.; Hicks, M.; So, S.K.; Jendrisak, M.D.; McCullough, C.S.; et al. Intrahepatic portosystemic vascular stents: A bridge to hepatic transplantation. Surgery 1993, 113, 344–351. [Google Scholar] [PubMed]
- Moreno, A.; Meneu, J.C.; Moreno, E.; Fraile, M.; García, I.; Loinaz, C.; Abradelo, M.; Jiménez, C.; Gomez, R.; García-Sesma, A.; et al. Liver transplantation and transjugular intrahepatic portosystemic shunt. Transplant. Proc. 2003, 35, 1869–1870. [Google Scholar] [CrossRef] [PubMed]
- Dell’Era, A.; Grande, L.; Barros-Schelotto, P.; Turnes, J.; Fuster, J.; Charco, R.; García-Valdecasas, J.C.; Bosch, J.; García-Pagán, J.C. Impact of prior portosystemic shunt procedures on outcome of liver transplantation. Surgery 2005, 137, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Guerrini, G.P.; Pleguezuelo, M.; Maimone, S.; Calvaruso, V.; Xirouchakis, E.; Patch, D.; Rolando, N.; Davidson, B.; Rolles, K.; Burroughs, A. Impact of tips preliver transplantation for the outcome posttransplantation. Am. J. Transplant. 2009, 9, 192–200. [Google Scholar] [CrossRef]
- Barbier, L.; Hardwigsen, J.; Borentain, P.; Biance, N.; Daghfous, A.; Louis, G.; Botta-Fridlund, D.; Le Treut, Y.P. Impact of transjugular intrahepatic portosystemic shunting on liver transplantation: 12-year single-center experience. Clin. Res. Hepatol. Gastroenterol. 2014, 38, 155–163. [Google Scholar] [CrossRef]
- Fagiuoli, S.; Bruno, R.; Debernardi Venon, W.; Schepis, F.; Vizzutti, F.; Toniutto, P.; Senzolo, M.; Caraceni, P.; Salerno, F.; Angeli, P.; et al. Consensus conference on TIPS management: Techniques, indications, contraindications. Dig. Liver Dis. 2017, 49, 121–137. [Google Scholar] [CrossRef]
- Dariushnia, S.R.; Haskal, Z.J.; Midia, M.; Martin, L.G.; Walker, T.G.; Kalva, S.P.; Clark, T.W.; Ganguli, S.; Krishnamurthy, V.; Saiter, C.K.; et al. Quality Improvement Guidelines for Transjugular Intrahepatic Portosystemic Shunts. J. Vasc. Interv. Radiol. 2016, 27, 1–7. [Google Scholar] [CrossRef]
- Sellers, C.M.; Nezami, N.; Schilsky, M.L.; Kim, H.S. Transjugular intrahepatic portosystemic shunt as a bridge to liver transplant: Current state and future directions. Transplant. Rev. 2019, 33, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Balducci, D.; Montori, M.; De Blasio, F.; Di Bucchianico, A.; Argenziano, M.E.; Baroni, G.S.; Scarpellini, E. The Role of Transjugular Intrahepatic Portosystemic Shunt (TIPS) in Treating Portal Hypertension in Patients with Hepatocellular Carcinoma. Medicina 2023, 59, 1150. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.X.; Qiu, Z.K.; Wang, G.B.; Wang, G.S.; Jiang, W.W.; Gao, F. Safety and effectiveness of transjugular intrahepatic portosystemic shunt in hepatocellular carcinoma patients with portal hypertension: A systematic review and meta-analysis. Clin. Radiol. 2023, 78, 209–218. [Google Scholar] [CrossRef]
- Bjørneboe, M.; Andersen, J.R.; Christensen, U.; Skinhøj, P.; Jensen, O.M. Does a portal-systemic shunt increase the risk of primary hepatic carcinoma in cirrhosis of the liver? Scand J. Gastroenterol. 1985, 20, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Bañares, R.; Núñez, O.; Escudero, M.; Fernández, C.; Vaquero, J.; Beceiro, I.; Echenagusía, A.; Clemente, G.; Santos, L. Patients with cirrhosis and bare-stent TIPS may have increased risk of hepatocellular carcinoma. Hepatology 2005, 41, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Pang, L.; Chen, H.B.; Wu, D.B.; Wang, Y.H.; Chen, E.Q. TIPS Is Not Associated with a Higher Risk of Developing HCC in Cirrhotic Patients: A Systematic Review and Meta-analysis. J. Clin. Transl. Hepatol. 2019, 7, 232–237. [Google Scholar] [CrossRef]
- Kang, J.W.; Kim, J.H.; Ko, G.Y.; Gwon DIl Yoon, H.K.; Sung, K.B. Transarterial chemoembolization for hepatocellular carcinoma after transjugular intrahepatic portosystemic shunt. Acta Radiol. 2012, 53, 545–550. [Google Scholar] [CrossRef]
- Tesdal, I.K.; Wikström, M.; Flechtenmacher, C.; Filser, T.; Dueber, C. Percutaneous treatment of hepatocellular carcinoma in patients with transjugular intrahepatic portosystemic shunts. Cardiovasc. Interv. Radiol. 2006, 29, 778–784. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, H.; Zhao, H.; Wang, X.; Tsauo, J.; Luo, X.; Li, X. Repeated transcatheter arterial chemoembolization is safe for hepatocellular carcinoma in cirrhotic patients with transjugular intrahepatic portosystemic shunt. Diagn. Interv. Radiol. 2014, 20, 487–491. [Google Scholar] [CrossRef]
- Donahue, L.A.; Kulik, L.; Baker, T.; Ganger, D.R.; Gupta, R.; Memon, K.; Abecassis, M.M.; Salem, R.; Lewandowski, R.J. Yttrium-90 radioembolization for the treatment of unresectable hepatocellular carcinoma in patients with transjugular intrahepatic portosystemic shunts. J. Vasc. Interv. Radiol. 2013, 24, 74–80. [Google Scholar] [CrossRef]
- Park, J.K.; Al-Tariq, Q.Z.; Zaw, T.M.; Raman, S.S.; Lu, D.S. Radiofrequency Ablation for the Treatment of Hepatocellular Carcinoma in Patients with Transjugular Intrahepatic Portosystemic Shunts. Cardiovasc. Interv. Radiol. 2015, 38, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Kohi, M.P.; Fidelman, N.; Naeger, D.M.; LaBerge, J.M.; Gordon, R.L.; Kerlan, R.K., Jr. Hepatotoxicity after transarterial chemoembolization and transjugular intrahepatic portosystemic shunt: Do two rights make a wrong? J. Vasc. Interv. Radiol. 2013, 24, 68–73. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kuo, Y.C.; Kohi, M.P.; Naeger, D.M.; Tong, R.T.; Kolli, K.P.; Taylor, A.G.; Laberge, J.M.; Kerlan, R.K., Jr.; Fidelman, N. Efficacy of TACE in TIPS patients: Comparison of treatment response to chemoembolization for hepatocellular carcinoma in patients with and without a transjugular intrahepatic portosystemic shunt. Cardiovasc. Interv. Radiol. 2013, 36, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013, 144, 1426–1437.e9. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460, Erratum in J. Hepatol. 2018, 69, 1207. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Kimmann, M.; Laleman, W.; Praktiknjo, M.; Trebicka, J. To TIPS or Not to TIPS in High Risk of Variceal Rebleeding and Acute-on-Chronic Liver Failure. Semin. Liver Dis. 2023, 43, 189–205. [Google Scholar] [CrossRef] [PubMed]
- Wong, F.; Pantea, L.; Sniderman, K. Midodrine, octreotide, albumin, and TIPS in selected patients with cirrhosis and type 1 hepatorenal syndrome. Hepatology 2004, 40, 55–64. [Google Scholar] [CrossRef]
- Testino, G.; Leone, S.; Ferro, C.; Borro, P. Severe acute alcoholic hepatitis and hepatorenal syndrome: Role of transjugular intrahepatic portosystemic stent shunt. J. Med. Life 2012, 5, 203–205. [Google Scholar]
- Brensing, K.A.; Textor, J.; Perz, J.; Schiedermaier, P.; Raab, P.; Strunk, H.; Klehr, H.U.; Kramer, H.J.; Spengler, U.; Schild, H.; et al. Long term outcome after transjugular intrahepatic portosystemic stent-shunt in non-transplant cirrhotics with hepatorenal syndrome: A phase II study. Gut 2000, 47, 288–295. [Google Scholar] [CrossRef]
- Song, T.; Rössle, M.; He, F.; Liu, F.; Guo, X.; Qi, X. Transjugular intrahepatic portosystemic shunt for hepatorenal syndrome: A systematic review and meta-analysis. Dig. Liver Dis. 2018, 50, 323–330. [Google Scholar] [CrossRef]
- Ripoll, C.; Platzer, S.; Franken, P.; Aschenbach, R.; Wienke, A.; Schuhmacher, U.; Teichgräber, U.; Stallmach, A.; Steighardt, J.; Zipprich, A.; et al. Liver-HERO: Hepatorenal syndrome-acute kidney injury (HRS-AKI) treatment with transjugular intrahepatic portosystemic shunt in patients with cirrhosis-a randomized controlled trial. Trials 2023, 24, 258. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, M.; Devurgowda, D.; Vyas, T.; Shasthry, S.M.; Khumuckham, J.S.; Goyal, R.; Thomas, S.S.; Kumar, G. Left Ventricular Diastolic Dysfunction is Associated with Renal Dysfunction, Poor Survival and Low Health Related Quality of Life in Cirrhosis. J. Clin. Exp. Hepatol. 2019, 9, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Valeriano, V.; Funaro, S.; Attili, A.F.; Masini, A.; Efrati, C.; De, C.S.; Riggio, O. Modifications of cardiac function in cirrhotic patients treated with transjugular intrahepatic portosystemic shunt (TIPS). Am. J. Gastroenterol. 2002, 97, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Radunski, U.K.; Kluwe, J.; Klein, M.; Galante, A.; Lund, G.K.; Sinning, C.; Bohnen, S.; Tahir, E.; Starekova, J.; Bannas, P.; et al. Cardiovascular magnetic resonance demonstrates structural cardiac changes following transjugular intrahepatic portosystemic shunt. Sci. Rep. 2021, 11, 12719. [Google Scholar] [CrossRef]
- Filì, D.; Falletta, C.; Luca, A.; Hernandez Baravoglia, C.; Clemenza, F.; Miraglia, R.; Scardulla, C.; Tuzzolino, F.; Vizzini, G.; Gridelli, B.; et al. Circulatory response to volume expansion and transjugular intrahepatic portosystemic shunt in refractory ascites: Relationship with diastolic dysfunction. Dig. Liver Dis. 2015, 47, 1052–1058. [Google Scholar] [CrossRef]
- Meucci, M.C.; Hoogerduijn Strating, M.M.; Butcher, S.C.; van Rijswijk, C.S.P.; Van Hoek, B.; Delgado, V.; Bax, J.J.; Tushuizen, M.E.; Marsan, N.A. Left atrial dysfunction is an independent predictor of mortality in patients with cirrhosis treated by transjugular intrahepatic portosystemic shunt. Hepatol. Commun. 2022, 6, 3163–3174. [Google Scholar] [CrossRef]
- Rabie, R.N.; Cazzaniga, M.; Salerno, F.; Wong, F. The use of E/A ratio as a predictor of outcome in cirrhotic patients treated with transjugular intrahepatic portosystemic shunt. Am. J. Gastroenterol. 2009, 104, 2458–2466. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Cola, S.; Lapenna, L.; Gazda, J.; Fonte, S.; Cusi, G.; Esposito, S.; Mattana, M.; Merli, M. Role of Transjugular Intrahepatic Portosystemic Shunt in the Liver Transplant Setting. J. Clin. Med. 2024, 13, 600. https://doi.org/10.3390/jcm13020600
Di Cola S, Lapenna L, Gazda J, Fonte S, Cusi G, Esposito S, Mattana M, Merli M. Role of Transjugular Intrahepatic Portosystemic Shunt in the Liver Transplant Setting. Journal of Clinical Medicine. 2024; 13(2):600. https://doi.org/10.3390/jcm13020600
Chicago/Turabian StyleDi Cola, Simone, Lucia Lapenna, Jakub Gazda, Stefano Fonte, Giulia Cusi, Samuele Esposito, Marco Mattana, and Manuela Merli. 2024. "Role of Transjugular Intrahepatic Portosystemic Shunt in the Liver Transplant Setting" Journal of Clinical Medicine 13, no. 2: 600. https://doi.org/10.3390/jcm13020600
APA StyleDi Cola, S., Lapenna, L., Gazda, J., Fonte, S., Cusi, G., Esposito, S., Mattana, M., & Merli, M. (2024). Role of Transjugular Intrahepatic Portosystemic Shunt in the Liver Transplant Setting. Journal of Clinical Medicine, 13(2), 600. https://doi.org/10.3390/jcm13020600