
Atrial Fibrillation and Early Vascular Aging: Clinical Implications, Methodology Issues and Open Questions—A Review from the VascAgeNet COST Action

 ,
,  ,
,  ,
,  , , , , , ,
, , , , , ,  ,
,  and
and 
Abstract
1. Introduction
1.1. Structural Arterial Properties: The Arterial Stiffness
1.2. Functional Arterial Properties: The Endothelial Dysfunction
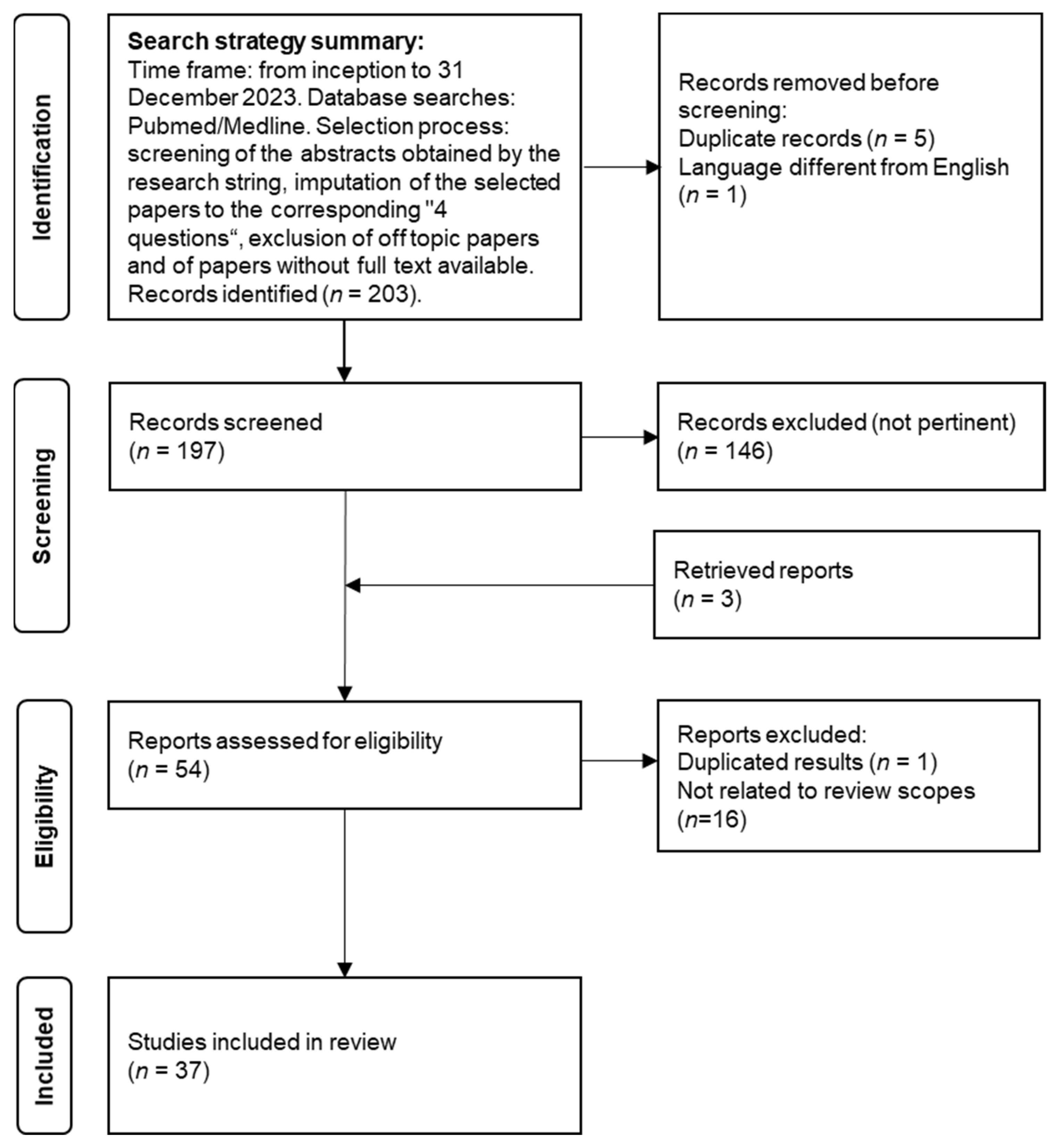
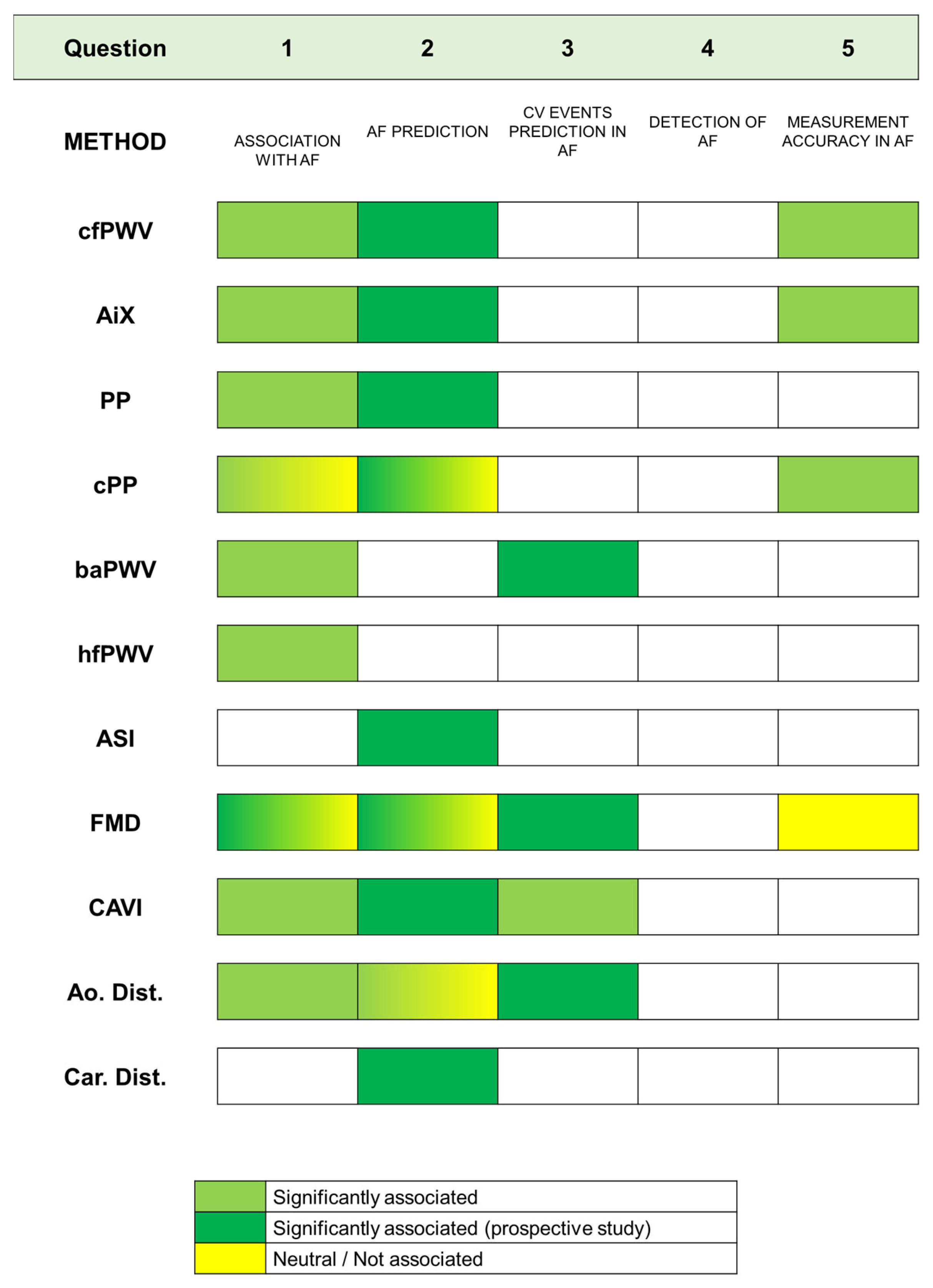
- Are VA biomarkers associated with AF?
- Does early VA predict AF occurrence better than chronological aging?
- Is early VA a risk enhancer for the occurrence of CV events in AF patients?
- Are devices measuring VA suitable to perform subclinical AF detection?
- Is the measurement of VA negatively influenced by AF-related rhythm irregularities?
2. Materials and Methods
3. Results
3.1. Question 1—Are VA Biomarkers Associated with AF?
3.2. Question 2—Does VA Predict the Occurrence of AF Better Than Chronological Aging?
Indirect Markers of AF
3.3. Question 3—Is Early VA a Risk Enhancer for the Occurrence of CV Events in AF Patients?
3.4. Question 4—Are Devices Measuring VA Suitable to Perform Subclinical AF Detection?
3.5. Question 5—Does Atrial-Fibrillation-Related Rhythm Irregularity Have a Negative Impact on the Measurement of Vascular Age?
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2020, 16, 217–221. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Wu, J.; Nadarajah, R.; Nakao, Y.M.; Nakao, K.; Wilkinson, C.; Mamas, M.A.; Camm, A.J.; Gale, C.P. Temporal trends and patterns in atrial fibrillation incidence: A population-based study of 3·4 million individuals. Lancet Reg. Health Eur. 2022, 17, 100386. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, J.-A.; Dilaveris, P.E.; et al. The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Martinez, C.; Katholing, A.; Freedman, S.B.; Martinez, C.; Katholing, A.; Freedman, S.B. Adverse prognosis of incidentally detected ambulatory atrial fibrillation. Thromb. Haemost. 2014, 112, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B.; Potpara, T.S.; Lip, G.Y.H. Stroke prevention in atrial fibrillation. Lancet 2016, 388, 806–817. [Google Scholar] [CrossRef] [PubMed]
- Freedman, B. Screening for Atrial Fibrillation Using a Smartphone: Is There an App for That? J. Am. Heart Assoc. 2016, 5, e004000. [Google Scholar] [CrossRef] [PubMed]
- Climie, R.E.; Alastruey, J.; Mayer, C.C.; Schwarz, A.; Laucyte-Cibulskiene, A.; Voicehovska, J.; Bianchini, E.; Bruno, R.-M.; Charlton, P.H.; Grillo, A.; et al. Vascular ageing: Moving from bench towards bedside. Eur. J. Prev. Cardiol. 2023, 30, 1101–1117. [Google Scholar] [CrossRef] [PubMed]
- Gkaliagkousi, E.; Lazaridis, A.; Dogan, S.; Fraenkel, E.; Tuna, B.G.; Mozos, I.; Vukicevic, M.; Yalcin, O.; Gopcevic, K. Theories and Molecular Basis of Vascular Aging: A Review of the Literature from VascAgeNet Group on Pathophysiological Mechanisms of Vascular Aging. Int. J. Mol. Sci. 2022, 23, 8672. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; May, M.; Anderson, S.; Benjamin, E.; Boutouyrie, P.; Cameron, J.; Chen, C.-H.; Cruickshank, J.K.; et al. Aortic Pulse Wave Velocity Improves Cardiovascular Event Prediction. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Bruno, R.M.; Nilsson, P.M.; Engström, G.; Wadström, B.N.; Empana, J.-P.; Boutouyrie, P.; Laurent, S. Early and Supernormal Vascular Aging: Clinical Characteristics and Association with Incident Cardiovascular Events. Hypertension 2020, 76, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.; Li, M.; Wang, T.; Chen, Y.; Dai, M.; Zhang, D.; Xu, Y.; Xu, M.; Lu, J.; Wang, W.; et al. Association of Early and Supernormal Vascular Aging categories with cardiovascular disease in the Chinese population. Front. Cardiovasc. Med. 2022, 9, 895792. [Google Scholar] [CrossRef] [PubMed]
- Lip, G. Does atrial fibrillation confer a hypercoagulable state? Lancet 1995, 346, 1313–1314. [Google Scholar] [CrossRef]
- Cai, H.; Li, Z.; Goette, A.; Mera, F.; Honeycutt, C.; Feterik, K.; Wilcox, J.N.; Dudley, S.C.; Harrison, D.G.; Langberg, J.J.; et al. Downregulation of endocardial nitric oxide synthase expression and nitric oxide production in atrial fibrillation: Potential mechanisms for atrial thrombosis and stroke. Circulation 2002, 106, 2854–2858. [Google Scholar] [CrossRef]
- Khan, A.A.; Thomas, G.N.; Lip, G.Y.H.; Shantsila, A. Endothelial function in patients with atrial fibrillation. Ann. Med. 2020, 52, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Thijssen, D.H.J.; Bruno, R.M.; Van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Xu, Y.; Arora, R.C.; Hiebert, B.M.; Lerner, B.; Szwajcer, A.; McDonald, K.; Rigatto, C.; Komenda, P.; Sood, M.M.; Tangri, N. Non-invasive endothelial function testing and the risk of adverse outcomes: A systematic review and meta-analysis. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 736–746. [Google Scholar] [CrossRef]
- Climie, R.E.; Mayer, C.C.; Bruno, R.M.; Hametner, B. Addressing the Unmet Needs of Measuring Vascular Ageing in Clinical Practice—European COoperation in Science and Technology Action VascAgeNet. Artery Res. 2020, 26, 71–75. [Google Scholar] [CrossRef]
- Caluwé, R.; De Vriese, A.S.; Van Vlem, B.; Verbeke, F. Measurement of pulse wave velocity, augmentation index, and central pulse pressure in atrial fibrillation: A proof of concept study. J. Am. Soc. Hypertens. 2018, 12, 627–632. [Google Scholar] [CrossRef]
- Skalidis, E.I.; Zacharis, E.A.; Tsetis, D.K.; Pagonidis, K.; Chlouverakis, G.; Yarmenitis, S.; Hamilos, M.; Manios, E.G.; Vardas, P.E. Endothelial cell function during atrial fibrillation and after restoration of sinus rhythm. Am. J. Cardiol. 2007, 99, 1258–1262. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-C.; Lee, W.-H.; Hsu, P.-C.; Lin, M.-Y.; Lee, C.-S.; Lin, T.-H.; Voon, W.-C.; Lai, W.-T.; Sheu, S.-H.; Su, H.-M. Association of Brachial–Ankle Pulse Wave Velocity with Cardiovascular Events in Atrial Fibrillation. Am. J. Hypertens. 2015, 29, 348–356. [Google Scholar] [CrossRef]
- Shchetynska-Marinova, T.; Liebe, V.; Papavassiliu, T.; Fernandez, A.d.F.; Hetjens, S.; Sieburg, T.; Doesch, C.; Sigl, M.; Akin, I.; Borggrefe, M.; et al. Determinants of arterial stiffness in patients with atrial fibrillation. Arch. Cardiovasc. Dis. 2021, 114, 550–560. [Google Scholar] [CrossRef]
- Chen, L.Y.; Tai, B.C.; Foo, D.C.; Wong, R.C.; Adabag, A.S.; Benditt, D.G.; Ling, L.H. Carotid-femoral pulse wave velocity is associated with N-terminal pro-B-type natriuretic peptide level in patients with atrial fibrillation. Heart Asia 2011, 3, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Perri, L.; Pastori, D.; Pignatelli, P.; Violi, F.; Loffredo, L. Flow-mediated dilation is associated with cardiovascular events in non-valvular atrial fibrillation patients. Int. J. Cardiol. 2015, 179, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Tan, Q.; Lina, W.; Zhaoqian, Z. Endothelial dysfunction predicted cardiovascular events in patients with paroxysmal atrial fibrillation. SciVee 2022, 43, 708–714. [Google Scholar] [CrossRef]
- Chen, L.Y.; Leening, M.J.G.; Norby, F.L.; Roetker, N.S.; Hofman, A.; Franco, O.H.; Pan, W.; Polak, J.F.; Witteman, J.C.; Kronmal, R.A.; et al. Carotid Intima-Media Thickness and Arterial Stiffness and the Risk of Atrial Fibrillation: The Atherosclerosis Risk in Communities (ARIC) Study, Multi-Ethnic Study of Atherosclerosis (MESA), and the Rotterdam Study. J. Am. Heart Assoc. 2016, 5, e002907. [Google Scholar] [CrossRef]
- Almuwaqqat, Z.; Claxton, J.S.; Norby, F.L.; Lutsey, P.L.; Wei, J.; Soliman, E.Z.; Chen, L.Y.; Matsushita, K.; Heiss, G.; Alonso, A. Association of arterial stiffness with incident atrial fibrillation: A cohort study. BMC Cardiovasc. Disord. 2021, 21, 247. [Google Scholar] [CrossRef]
- Shaikh, A.Y.; Wang, N.; Yin, X.; Larson, M.G.; Vasan, R.S.; Hamburg, N.M.; Magnani, J.W.; Ellinor, P.T.; Lubitz, S.A.; Mitchell, G.F.; et al. Relations of Arterial Stiffness and Brachial Flow–Mediated Dilation with New-Onset Atrial Fibrillation: The Framingham Heart Study. Hypertension 2016, 68, 590–596. [Google Scholar] [CrossRef]
- Nagayama, D.; Fujishiro, K.; Nakamura, K.; Watanabe, Y.; Yamaguchi, T.; Suzuki, K.; Shimizu, K.; Saiki, A.; Shirai, K. Cardio-Ankle Vascular Index is Associated with Prevalence and New-Appearance of Atrial Fibrillation in Japanese Urban Residents: A Retrospective Cross-Sectional and Cohort Study. Vasc. Health Risk Manag. 2022, 18, 5–15. [Google Scholar] [CrossRef]
- Roetker, N.S.; Chen, L.Y.; Heckbert, S.R.; Nazarian, S.; Soliman, E.Z.; Bluemke, D.A.; Lima, J.A.; Alonso, A. Relation of Systolic, Diastolic, and Pulse Pressures and Aortic Distensibility with Atrial Fibrillation (from the Multi-Ethnic Study of Atherosclerosis). Am. J. Cardiol. 2014, 114, 587–592. [Google Scholar] [CrossRef]
- Valbusa, F.; Bonapace, S.; Bertolini, L.; Zenari, L.; Arcaro, G.; Targher, G. Increased Pulse Pressure Independently Predicts Incident Atrial Fibrillation in Patients with Type 2 Diabetes. Diabetes Care 2012, 35, 2337–2339. [Google Scholar] [CrossRef][Green Version]
- Larstorp, A.C.K.; Ariansen, I.; Gjesdal, K.; Olsen, M.H.; Ibsen, H.; Devereux, R.B.; Okin, P.M.; Dahlöf, B.; Kjeldsen, S.E.; Wachtell, K. Association of pulse pressure with new-onset atrial fibrillation in patients with hypertension and left ventricular hypertrophy: The Losartan Intervention For Endpoint (LIFE) reduction in hypertension study. Hypertension 2012, 60, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Vasan, R.S.; Keyes, M.J.; Parise, H.; Wang, T.J.; Larson, M.G.; D’agostino, R.B.; Kannel, W.B.; Levy, D.; Benjamin, E.J. Pulse pressure and risk of new-onset atrial fibrillation. JAMA 2007, 297, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Jin, Z.; Homma, S.; Elkind, M.S.; Schwartz, J.E.; Rundek, T.; Mannina, C.; Ito, K.; Sacco, R.L.; Di Tullio, M.R. Office, central and ambulatory blood pressure for predicting incident atrial fibrillation in older adults. J. Hypertens. 2020, 39, 46–52. [Google Scholar] [CrossRef]
- Shchetynska-Marinova, T.; Kranert, M.; Baumann, S.; Liebe, V.; Grafen, A.; Gerhards, S.; Rosenkaimer, S.; Akin, I.; Borggrefe, M.; Hohneck, A.L. Recurrence of atrial fibrillation after pulmonary vein isolation in dependence of arterial stiffness. Neth. Heart J. 2021, 30, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.H.; Middeldorp, M.E.; Brooks, A.G.; Ganesan, A.N.; Roberts-Thomson, K.C.; Stiles, M.K.; Leong, D.P.; Abed, H.S.; Lim, H.S.; Wong, C.X.; et al. Aortic Stiffness in Lone Atrial Fibrillation: A Novel Risk Factor for Arrhythmia Recurrence. PLoS ONE 2013, 8, e76776. [Google Scholar] [CrossRef]
- Fumagalli, S.; Giannini, I.; Pupo, S.; Agostini, F.; Boni, S.; Roberts, A.T.; Gabbai, D.; Di Serio, C.; Gabbani, L.; Tarantini, F.; et al. Atrial fibrillation after electrical cardioversion in elderly patients: A role for arterial stiffness? Results from a preliminary study. Aging Clin. Exp. Res. 2016, 28, 1273–1277. [Google Scholar] [CrossRef]
- Kizilirmak, F.; Guler, G.B.; Guler, E.; Gunes, H.M.; Demir, G.G.; Omaygenc, M.O.; Cakal, B.; Olgun, F.E.; Koklu, E.; Kilicaslan, F. Impact of aortic stiff ness on the frequency of paroxysmal atrial fi brillation recurrences. Acta Cardiol. 2015, 70, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Zekavat, S.M.; Roselli, C.; Hindy, G.; Lubitz, S.A.; Ellinor, P.T.; Zhao, H.; Natarajan, P. Genetic Link Between Arterial Stiffness and Atrial Fibrillation. Circ. Genom. Precis. Med. 2019, 12, e002453. [Google Scholar] [CrossRef]
- Drager, L.F.; Bortolotto, L.A.; Pedrosa, R.P.; Krieger, E.M.; Lorenzi-Filho, G. Left atrial diameter is independently associated with arterial stiffness in patients with obstructive sleep apnea: Potential implications for atrial fibrillation. Int. J. Cardiol. 2010, 144, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Lantelme, P.; Laurent, S.; Besnard, C.; Bricca, G.; Vincent, M.; Legedz, L.; Milon, H. Arterial stiffness is associated with left atrial size in hypertensive patients. Arch. Cardiovasc. Dis. 2008, 101, 35–40. [Google Scholar] [CrossRef]
- Garg, P.K.; Bartz, T.M.; Burke, G.; Gottdiener, J.S.; Herrington, D.; Heckbert, S.R.; Kizer, J.R.; Sotoodehnia, N.; Mukamal, K.J. Brachial Flow-Mediated Dilation and Risk of Atrial Fibrillation in Older Adults: The Cardiovascular Health Study. Vasc. Health Risk Manag. 2021, 17, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Pauklin, P.; Eha, J.; Tootsi, K.; Kolk, R.; Paju, R.; Kals, M.; Kampus, P. Atrial fibrillation is associated with increased central blood pressure and arterial stiffness. J. Clin. Hypertens. 2021, 23, 1581–1587. [Google Scholar] [CrossRef]
- Cui, R.; Yamagishi, K.; Muraki, I.; Hayama-Terada, M.; Umesawa, M.; Imano, H.; Li, Y.; Eshak, E.S.; Ohira, T.; Kiyama, M.; et al. Association between markers of arterial stiffness and atrial fibrillation in the Circulatory Risk in Communities Study (CIRCS). Atherosclerosis 2017, 263, 244–248. [Google Scholar] [CrossRef]
- Doi, M.; Miyoshi, T.; Hirohata, S.; Iwabu, A.; Tominaga, Y.; Kaji, Y.; Kamikawa, S.; Sakane, K.; Kitawaki, T.; Kusano, K.F.; et al. Increased Augmentation Index of the Radial Pressure Waveform in Patients with Paroxysmal Atrial Fibrillation. Cardiology 2009, 113, 138–145. [Google Scholar] [CrossRef]
- Shi, D.; Meng, Q.; Zhou, X.; Li, L.; Liu, K.; He, S.; Wang, S.; Chen, X. Factors influencing the relationship between atrial fibrillation and artery stiffness in elderly Chinese patients with hypertension. Aging Clin. Exp. Res. 2016, 28, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Choi, S.; Jung, J.-H.; Lee, N. Effects of Atrial Fibrillation on Arterial Stiffness in Patients with Hypertension. Angiology 2008, 59, 459–463. [Google Scholar] [CrossRef]
- Miyoshi, T.; Doi, M.; Noda, Y.; Ohno, Y.; Sakane, K.; Kamikawa, S.; Noguchi, Y.; Ito, H. Arterial stiffness determined according to the cardio-ankle vascular index is associated with paroxysmal atrial fibrillation: A cross-sectional study. Heart Asia 2014, 6, 59–63. [Google Scholar] [CrossRef]
- Fumagalli, S.; Gabbai, D.; Nreu, B.; Roberts, A.T.; Boni, S.; Ceccofiglio, A.; Fracchia, S.; Baldasseroni, S.; Tarantini, F.; Marchionni, N. Age, left atrial dimension and arterial stiffness after external cardioversion of atrial fibrillation. A vascular component in arrhythmia maintenance? Results from a preliminary study. Aging Clin. Exp. Res. 2014, 26, 327–330. [Google Scholar] [CrossRef][Green Version]
- Chung, G.E.; Park, H.E.; Lee, H.; Choi, S.-Y. Clinical significance of increased arterial stiffness associated with atrial fibrillation, according to Framingham risk score. Sci. Rep. 2021, 11, 4955. [Google Scholar] [CrossRef]
- Heshmat-Ghahdarijani, K.; Jangjoo, S.; Amirpoor, A.; Najafian, J.; Khosravi, A.; Heidarpour, M.; Hekmat, M.; Shafie, D. Endothelial dysfunction in patients with lone atrial fibrillation. ARYA Atheroscler. 2020, 16, 278–283. [Google Scholar] [CrossRef]
- Guazzi, M.; Belletti, S.; Tumminello, G.; Fiorentini, C.; Guazzi, M.D. Exercise hyperventilation, dyspnea sensation, and ergoreflex activation in lone atrial fibrillation. Am. J. Physiol. Circ. Physiol. 2004, 287, H2899–H2905. [Google Scholar] [CrossRef] [PubMed]
- Börschel, C.S.; Rübsamen, N.; Ojeda, F.M.; Wild, P.S.; Hoffmann, B.A.; Prochaska, J.H.; Gori, T.; Lackner, K.J.; Blankenberg, S.; Zeller, T.; et al. Noninvasive peripheral vascular function and atrial fibrillation in the general population. J. Hypertens. 2019, 37, 928–934. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Junejo, R.T.; Alsharari, R.; Thomas, G.N.; Fisher, J.P.; Lip, G.Y.H. A greater burden of atrial fibrillation is associated with worse endothelial dysfunction in hypertension. J. Hum. Hypertens. 2021, 35, 667–677. [Google Scholar] [CrossRef]
- Polovina, M.; Potpara, T.; Giga, V.; Stepanovic, J.; Ostojic, M. Impaired endothelial function in lone atrial fibrillation. Vojnosanit. Pregl. 2013, 70, 908–914. [Google Scholar] [CrossRef]
- Spronck, B.; Heusinkveld, M.H.; Vanmolkot, F.H.; Roodt, J.O.; Hermeling, E.; Delhaas, T.; Kroon, A.A.; Reesink, K.D. Pressure-dependence of arterial stiffness: Potential clinical implications. J. Hypertens. 2015, 33, 330–338. [Google Scholar] [CrossRef]
- Franklin, S.S.; Gustin, W.; Wong, N.D.; Larson, M.G.; Weber, M.A.; Kannel, W.B.; Levy, D. Hemodynamic patterns of age-related changes in blood pressure: The Framingham Heart Study. Circulation 1997, 96, 308–315. [Google Scholar] [CrossRef]
- Yu, S.; McEniery, C.M. Central Versus Peripheral Artery Stiffening and Cardiovascular Risk. Arter. Thromb. Vasc. Biol. 2020, 40, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Charlton, P.H.; Paliakaitė, B.; Pilt, K.; Bachler, M.; Zanelli, S.; Kulin, D.; Allen, J.; Hallab, M.; Bianchini, E.; Mayer, C.C.; et al. Assessing hemodynamics from the photoplethysmogram to gain insights into vascular age: A review from VascAgeNet. Am. J. Physiol. Heart Circ. Physiol. 2022, 322, H493–H522. [Google Scholar] [CrossRef]
- Chan, P.; Wong, C.; Poh, Y.C.; Pun, L.; Leung, W.W.; Wong, Y.; Wong, M.M.; Poh, M.; Chu, D.W.; Siu, C.; et al. Diagnostic Performance of a Smartphone-Based Photoplethysmographic Application for Atrial Fibrillation Screening in a Primary Care Setting. J. Am. Heart Assoc. 2016, 5, e003428. [Google Scholar] [CrossRef]
- Park, S.-H.; June, K.J.; Choi, Y.-K. Predictive validity of automated oscillometric blood pressure monitors for screening atrial fibrillation: A systematic review and meta-analysis. Expert Rev. Med. Devices 2019, 16, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Najjar, S.S.; Scuteri, A.; Shetty, V.; Wright, J.G.; Muller, D.C.; Fleg, J.L.; Spurgeon, H.P.; Ferrucci, L.; Lakatta, E.G. Pulse Wave Velocity Is an Independent Predictor of the Longitudinal Increase in Systolic Blood Pressure and of Incident Hypertension in the Baltimore Longitudinal Study of Aging. J. Am. Coll. Cardiol. 2008, 51, 1377–1383. [Google Scholar] [CrossRef] [PubMed]
- Parati, G.; Bilo, G.; Kollias, A.; Pengo, M.; Ochoa, J.E.; Castiglioni, P.; Stergiou, G.S.; Mancia, G.; Asayama, K.; Asmar, R.; et al. Blood pressure variability: Methodological aspects, clinical relevance and practical indications for management-a European Society of Hypertension position paper. J. Hypertens. 2023, 41, 527–544. [Google Scholar] [CrossRef] [PubMed]
- Kaze, A.D.; Yuyun, M.F.; Fonarow, G.C.; Echouffo-Tcheugui, J.B. Blood Pressure Variability and Risk of Atrial Fibrillation in Adults with Type 2 Diabetes. JACC Adv. 2023, 2, e100382. [Google Scholar] [CrossRef]
- Proietti, M.; Romiti, G.F.; Olshansky, B.; Lip, G.Y. Systolic Blood Pressure Visit-to-Visit Variability and Major Adverse Outcomes in Atrial Fibrillation: The AFFIRM Study (Atrial Fibrillation Follow-Up Investigation of Rhythm Management). Hypertension 2017, 70, 949–958. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Vascular Aging Biomarker | Method of Measurement |
|---|---|
| Carotid–femoral pulse wave velocity (cfPWV) | Ratio of traveled distance between the carotid and femoral pulse site and transit time between common carotid and common femoral artery; based on tonometers, piezoelectronic sensors, cuffs or Doppler ultrasound, either simultaneously or sequentially, using ECG for gating. |
| Heart–femoral pulse wave velocity (hfPWV) | Ratio of traveled distance between the heart and femoral pulse sites and transit time starting from second heart sound; based on tonometers, ECG and microphones. |
| Brachial–ankle pulse wave velocity (baPWV) | Ratio between traveled distance and transit time calculated with occlusive cuffs placed at brachial artery and ankle; cardio-ankle vascular index is a variation using a phonocardiogram and occlusive cuffs. |
| Arterial stiffness index (ASI) | Marker of arterial stiffness calculated by dividing height by the timing of reflected waves from finger photoplethysmography |
| Cardio-ankle vascular index (CAVI) | Marker of arterial stiffness based on the stiffness parameter β, reflecting arterial properties from origin of the ascending aorta to the ankle. |
| Brachial pulse pressure (PP) | Measured using validated sphygmomanometers; brachial pulse pressure defined as systolic minus diastolic BP. |
| Central pulse pressure (cPP) | Central pulse pressure based on waveforms recorded at the radial, brachial or carotid artery, mainly using tonometers or cuffs; waveforms are calibrated with measured brachial BP leading to central systolic BP and pulse pressure. |
| Augmentation index (AIx) | The ratio between central augmented pressure and pulse pressure, as a surrogate indicator of wave reflections and left ventricular loading. |
| Pulse pressure amplification (PPA) | Central to peripheral pulse pressure amplification (peripheral PP/central PP) is due to both cardiac and arterial factors: ventricular ejection, arterial stiffness, amplitude and timing of wave reflection. VA reduces PPA values. |
| Brachial artery flow-mediated dilation (FMD) | Flow-mediated dilation induces the release of nitric oxide, resulting in vasodilation that can be measured by ultrasound imaging of the diameter of the brachial artery after an ischemia induced by arterial occlusion using a cuff, which is released after 5 min, leading to reactive hyperemia. |
| Aortic distensibility | Measure of aortic elasticity estimated by the relative change in diameter, area or volume divided by the pulse pressure generating this change; may be measured by echocardiography or by MRI. |
| Carotid artery distensibility | Measure of carotid artery elasticity estimated by the ratio between relative change in diameter or volume and the pulse pressure generating this change; usually measured by carotid ultrasound. |
| Year, Author, Country | Method (Biomarker) | Population | Study Design | Main Results | Questions | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||||
| 2018, Caluwé R et al., Belgium [20] | SphygmoCor (cfPWV, AIx, central pulse pressure) | 34 patients with AF | Experimental study: before and after cardioversion for AF | Good agreement before and after cardioversion for cfPWV and cPP, moderate agreement for AIx. | |||||
| 2007, Skalidis EI et al., Greece [21] | Brachial artery FMD and NMD (FMD, NMD) | 46 patients with AF and 25 controls | Experimental study, before and after electrical cardioversion | FMD improved after successful cardioversion, while NMD was not significantly altered. High agreement in Bland–Altmann analysis. | |||||
| 2016, Chen SC et al., Taiwan [22] | Omron VP-1000 (baPWV) | 167 patients with AF | Longitudinal observational study | In patients with AF, a high baPWV was independently associated with increased CV events. | |||||
| 2021, Shchetynska-Marinova T et al., Germany [23] | Echocardiography (aortic distensibility) | 151 patients with AF and 54 controls | Longitudinal observational study | AF was associated with reduced aortic distensibility, left atrial size and pulse pressure. The incidence of AF recurrences increased with loss of aortic distensibility. | |||||
| 2011, Chen LY et al., USA [24] | SphygmoCor (cfPWV) | 118 patients with AF, 274 controls | Observational. case-control study | CfPWV was associated with NT-proBNP level in AF. | |||||
| 2015, Perri L et al., Italy [25] | Brachial artery FMD (FMD) | 514 non-valvular AF patients | Experimental prospective study | In patients with AF, low FMD (<4.6%) independently predicted CV events. | |||||
| 2022, Zhang J et al., China [26] | Brachial artery FMD (FMD) | 291 with paroxysmal AF | Longitudinal observational study | FMD was a predictor of CV events in patients with PAF. | |||||
| 2016, Chen LY et al., USA [27] | IMT, carotid distensibility (Echodoppler), aortic PWV (Complior) | 13,907 ARIC, 6640 MESA, 5220 Rotterdam Study | Longitudinal observational study | Higher IMT and greater arterial stiffness were associated with higher AF incidence, with modest improvement in AF risk prediction. | |||||
| 2021, Almuwaqqat Z et al., USA [28] | Omron VP-1000 (cfPWV) | 3882 elderly participants of ARIC | Longitudinal observational study | Low (first quartile) and high (third and fourth quartiles) cfPWV were associated with higher AF risk. | |||||
| 2016, Shaikh AY et al., USA [29] | Arterial tonometry (cfPWV, CPP, AIx). Doppler ultrasound (FMD) | 5797 Framingham tonometry sample; 3921 ED sample | Retrospective observational study | Higher AIx and central pressure, lower FMD were associated with increased risk of incident AF. | |||||
| 2022, Nagayama D et al., Japan [30] | VaSera cardio-ankle vascular index (CAVI) | 47,687 cross-sectional study; 5418 cohort study | Cross-sectional and longitudinal study | CAVI was independently associated with AF. CAVI ≥8.0 was an independent predictor for AF incidence. | |||||
| 2014, Roetker NS et al., USA [31] | Brachial oscillometry, MRI (pulse pressure, aortic distensibility) | 6630 participants from the MESA | Longitudinal observational study | Higher levels of systolic and pulse pressure were associated with increased risk of AF. Aortic distensibility was not consistently associated with the risk of AF. | |||||
| 2012, Valbusa F et al., Italy [32] | Brachial oscillometry (pulse pressure) | 350 patients with type 2 diabetes mellitus | Longitudinal observational study | Increased pulse pressure independently predicted incident AF in 10-year follow-up. | |||||
| 2012, Larstorp AC et al., Norway [33] | Oscillometry (pulse pressure) | 8810 hypertensive patients | Longitudinal observational study | Pulse pressure was the strongest single BP predictor of new-onset AF. | |||||
| 2007, Mitchell G et al., USA [34] | Brachial oscillometry (pulse pressure) | 5331 Framingham Heart Study participants initially free from AF | Longitudinal observational study | Pulse pressure was associated with increased risk for AF (adjusted hazard ratio, 1.26 per 20 mm Hg increment; p = 0.001). | |||||
| 2021, Matsumoto K et al., USA [35] | ABPM, SphygmoCor (central BP, ambulatory BP) | 769 participants in sinus rhythm | Longitudinal observational study | ABPM was a better independent predictor of incident AF than central BP. | |||||
| 2022, Shchetynska-Marinova T et al., Germany [36] | Echocardiography (aortic distensibility) | 151 patients with AF who underwent pulmonary vein isolation | Longitudinal observational study | Reduced aortic distensibility and increased atrial size were associated with AF recurrence. | |||||
| 2013, Lau DH et al., Australia [37] | SphygmoCor (Central BP, AIx) | 68 patients with lone AF undergoing successful catheter ablation | Longitudinal observational study | Central pulse pressure ≥ 45 mmHg and augmentation pressure ≥ 12 mmHg were both associated with lower survival free from AF. | |||||
| 2016, Fumagalli S et al., Italy [38] | VaSera Cardio-ankle vascular index (CAVI) | 31 patients with AF | Longitudinal observational study | After cardioversion, AF persistence at follow-up was associated with higher CAVI. | |||||
| 2015, Kizilirmak F et al., Turkey [39] | Mobil-O-Graph (central pulse pressure, PWV, AIx) | 103 patients with PAF, 103 controls | Longitudinal observational study | Increased arterial stiffness markers were associated with AF occurrence but not predicted recurrence after catheter ablation. | |||||
| 2019, Zekavat SM et al., USA [40] | Finger photoplethysmography (ASI) | 225,636 UK Biobank participants | Genome-wide association study. Mendelian randomization | Genetic predisposition to higher ASI was significantly associated with increased risk of incident and prevalent AF | |||||
| 2010, Drager LF et al., Portugal [41] | SphygmoCor, echocardiography (cf-PWV, left atrial diameter) | 73 middle-aged patients | Observational study | Left atrial diameter is associated with pulse wave velocity independently of common determinants. | |||||
| 2008, Lantelme P et al., France [42] | Complior, ABPM, echocardiography (cfPWV, 24 h PP, left atrial diameter) | 310 hypertensive patients | Observational study | Left atrial diameter is associated with cfPWV and 24 h PP independently from classical determinants (e.g., age, BMI, LV dimensions and geometry). | |||||
| 2021, Garg PK et al., USA [43] | Brachial artery FMD (FMD) | 2027 elderly patients | Longitudinal observational study | The risk of incident AF was not dependent on baseline FMD when analysis was adjusted for confounders. | |||||
| 2021, Pauklin P et al., Estonia [44] | Oscillometry, SphygmoCor (cfPWV, central BP, pressure amplification) | 76 patients with AF | Observational study | Patients with AF had significantly higher cSBP, cPP, PWV compared to healthy controls. Positive correlation of left atrial diameter and volume with PWV. | |||||
| 2017, Cui R et al., Japan [45] | Omron HEM9000AI (AIx) | 4264 participants | Longitudinal observational study | AIx values, but not brachial or central pulse pressures, were positively and independently associated with the prevalence of AF. | |||||
| 2009, Doi M et al., Japan [46] | Omron HEM9000AI (radial Aix) | 122 patients with PAF (in sinus rhythm), 122 controls | Observational Case–control study | AIx was significantly higher in patients with PAF than in subjects without PAF. | |||||
| 2005, Shi D et al., China [47] | Omron VP-1000 (brachial–ankle PWV) | 132 patients with hypertension and AF (78 paroxysmal, 84 persistent) and 136 with only hypertension | Observational study | Patients with AF and hypertension presented higher baPWV values than hypertension alone. Persistent AF was associated with higher baPWV than PAF. | |||||
| 2008, Lee SH et al., Republic of Korea [48] | VP-2000 (heart–femoral PWV) | 35 subjects with sinus rhythm, 33 subjects with AF | Observational case–control study | Patients with AF had higher hfPWV than those in sinus rhythm. AF was an independent predictor of increased hfPWV together with age and systolic BP. | |||||
| 2014, Miyoshi T et al., Japan [49] | VaSera cardio-ankle vascular index (CAVI) | 91 patients with PAF compared with 90 matched controls | Case–control study | CAVI was significantly higher in patients with PAF than in controls. | |||||
| 2014, Fumagalli S et al., Italy [50] | VaSera cardio-ankle vascular index (CAVI) | 33 patients with AF | Observational study | CAVI obtained immediately after cardioversion was associated with short AF duration and left atrial diameter. | |||||
| 2021, Chung GE et al., Korea [51] | VaSera cardio-ankle vascular index (CAVI) | 8048 subjects | Longitudinal observational study | High CAVI was associated with AF in those with intermediate or high CV risk. | |||||
| 2020, Heshmat-Ghahdarijani K et al., Iran [52] | Brachial artery FMD (FMD) | 43 patients with AF and 51 controls | Case–control study | FMD of patients with AF was significantly lower than controls. | |||||
| 2004, Guazzi M et al., Italy [53] | Brachial artery FMD | 35 patients with lone AF undergoing external cardioversion | Longitudinal observational study | Brachial FMD improved after cardioversion and returned to basal values in subjects with AF recurrency. | |||||
| 2019, Börschel CS et al., Germany [54] | Brachial artery FMD and peripheral arterial tonometry (PAT ratio) | 15,010 subjects (466 AF) | Observational study | FMD and PAT were compromised in individuals with AF, but associations were mediated by age and classical risk factors. | |||||
| 2021, Khan AA et al., United Kingdom [55] | Brachial artery FMD | 30 patients with permanent AF vs. 31 patients with PAF | Case–control study | Duration and frequency of AF lead to worsening endothelial function. | |||||
| 2013, Polovina M et al., Serbia [56] | Brachial artery FMD and NMD | 38 patients with persistent AF and 28 controls | Observational case–control study | FMD of AF patients was significantly lower than FMD of healthy controls. No differences in median NMD values. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pucci, G.; Grillo, A.; Dalakleidi, K.V.; Fraenkel, E.; Gkaliagkousi, E.; Golemati, S.; Guala, A.; Hametner, B.; Lazaridis, A.; Mayer, C.C.; et al. Atrial Fibrillation and Early Vascular Aging: Clinical Implications, Methodology Issues and Open Questions—A Review from the VascAgeNet COST Action. J. Clin. Med. 2024, 13, 1207. https://doi.org/10.3390/jcm13051207
Pucci G, Grillo A, Dalakleidi KV, Fraenkel E, Gkaliagkousi E, Golemati S, Guala A, Hametner B, Lazaridis A, Mayer CC, et al. Atrial Fibrillation and Early Vascular Aging: Clinical Implications, Methodology Issues and Open Questions—A Review from the VascAgeNet COST Action. Journal of Clinical Medicine. 2024; 13(5):1207. https://doi.org/10.3390/jcm13051207
Chicago/Turabian StylePucci, Giacomo, Andrea Grillo, Kalliopi V. Dalakleidi, Emil Fraenkel, Eugenia Gkaliagkousi, Spyretta Golemati, Andrea Guala, Bernhard Hametner, Antonios Lazaridis, Christopher C. Mayer, and et al. 2024. "Atrial Fibrillation and Early Vascular Aging: Clinical Implications, Methodology Issues and Open Questions—A Review from the VascAgeNet COST Action" Journal of Clinical Medicine 13, no. 5: 1207. https://doi.org/10.3390/jcm13051207
APA StylePucci, G., Grillo, A., Dalakleidi, K. V., Fraenkel, E., Gkaliagkousi, E., Golemati, S., Guala, A., Hametner, B., Lazaridis, A., Mayer, C. C., Mozos, I., Pereira, T., Veerasingam, D., Terentes-Printzios, D., & Agnoletti, D. (2024). Atrial Fibrillation and Early Vascular Aging: Clinical Implications, Methodology Issues and Open Questions—A Review from the VascAgeNet COST Action. Journal of Clinical Medicine, 13(5), 1207. https://doi.org/10.3390/jcm13051207