
Outcome Prediction of Speech Perception in Quiet and in Noise for Cochlear Implant Candidates Based on Pre-Operative Measures


Abstract
1. Introduction
2. Materials and Methods
3. Results
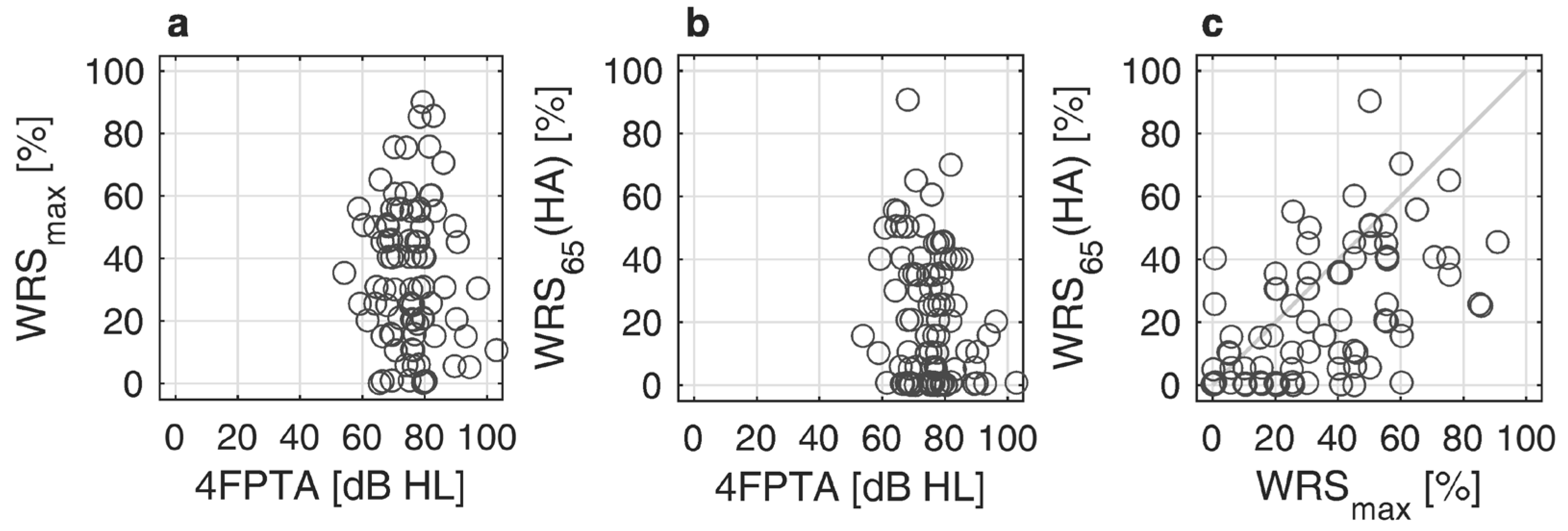
3.1. Preoperative Pure Tone and Speech Audiometry
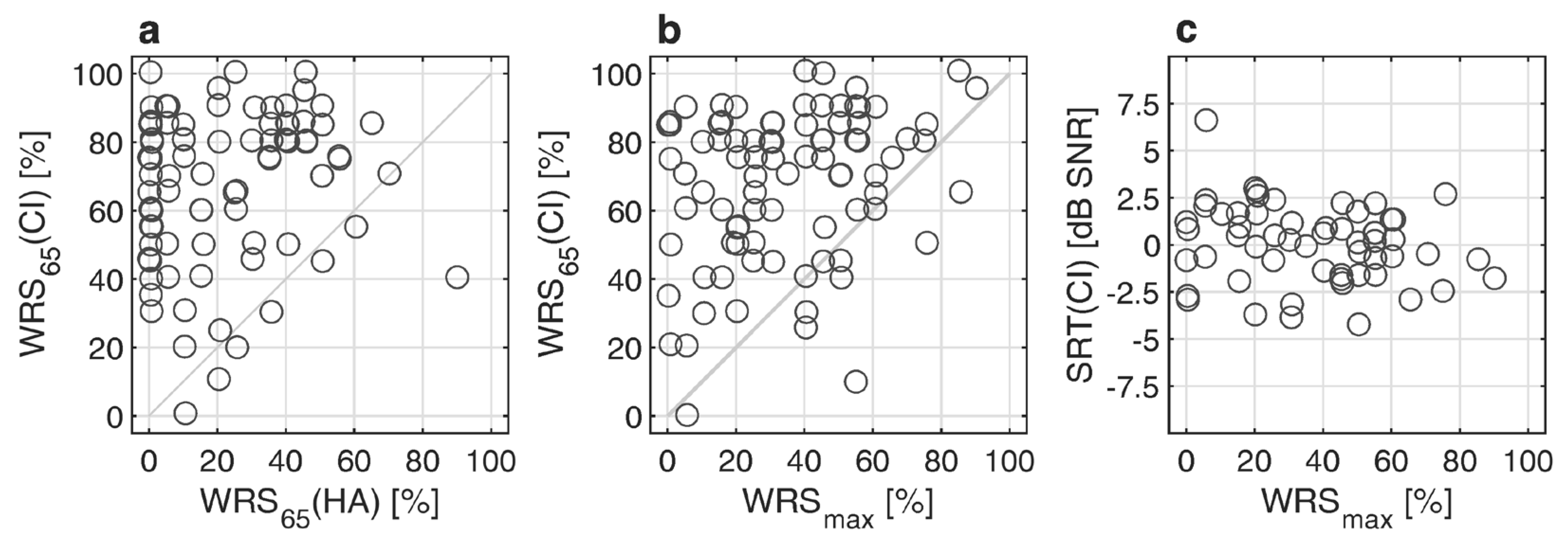
3.2. Postoperative Speech Audiometry
3.3. Prediction for Word Recognition in Quiet
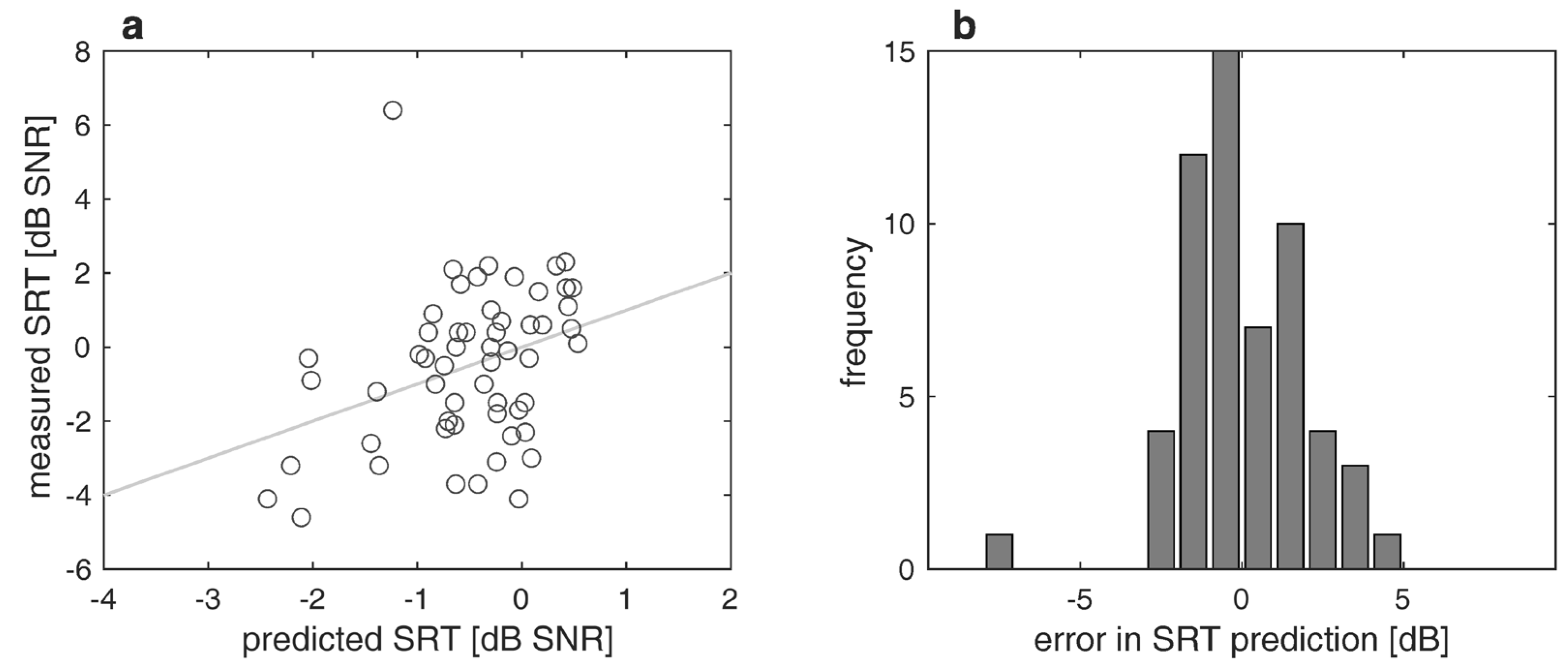
3.4. Prediction for Speech Recognition in Noise
4. Discussion
4.1. Speech Recognition Scores in Quiet
4.2. Prediction Model for Speech Perception Threshold in Noise
4.3. Limitations of this Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buchman, C.A.; Gifford, R.H.; Haynes, D.S.; Lenarz, T.; O’Donoghue, G.; Adunka, O.; Biever, A.; Briggs, R.J.; Carlson, M.L.; Dai, P.; et al. Unilateral Cochlear Implants for Severe, Profound, or Moderate Sloping to Profound Bilateral Sensorineural Hearing Loss: A Systematic Review and Consensus Statements. JAMA Otolaryngol. Head. Neck Surg. 2020, 146, 942–953. [Google Scholar] [CrossRef]
- AWMF. Leitlinien: Cochlea-Implantat Versorgung und Zentral-Auditorische Implantate [Guidelines: Cochlear Implant Care and Central Auditory Implants]. 2020. Available online: https://www.awmf.org/uploads/tx_szleitlinien/017-071l_S2k_Cochlea-Implantat-Versorgung-zentral-auditorische-Implantate_2020-12.pdf (accessed on 1 December 2023).
- Gifford, R.H.; Dorman, M.F.; Shallop, J.K.; Sydlowski, S.A. Evidence for the expansion of adult cochlear implant candidacy. Ear Hear. 2010, 31, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Van der Straaten, T.F.K.; Briaire, J.J.; Vickers, D.; Boermans, P.; Frijns, J.H.M. Selection Criteria for Cochlear Implantation in the United Kingdom and Flanders: Toward a Less Restrictive Standard. Ear Hear. 2020, 42, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Helbig, S.; Adel, Y.; Rader, T.; Stover, T.; Baumann, U. Long-term Hearing Preservation Outcomes After Cochlear Implantation for Electric-Acoustic Stimulation. Otol. Neurotol. 2016, 37, e353–e359. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, U.; Hocke, T.; Hast, A.; Iro, H. Maximum preimplantation monosyllabic score as predictor of cochlear implant outcome. HNO 2019, 67, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Thangavelu, K.; Nitzge, M.; Weiß, R.M.; Mueller-Mazzotta, J.; Stuck, B.A.; Reimann, K. Role of cochlear reserve in adults with cochlear implants following post-lingual hearing loss. Eur. Arch. Otorhinolaryngol. 2022, 280, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Rieck, J.H.; Beyer, A.; Mewes, A.; Caliebe, A.; Hey, M. Extended Preoperative Audiometry for Outcome Prediction and Risk Analysis in Patients Receiving Cochlear Implants. J. Clin. Med. 2023, 12, 3262. [Google Scholar] [CrossRef] [PubMed]
- Halpin, C.; Rauch, S. Clinical implications of a damaged cochlea: Pure tone thresholds vs. information-carrying capacity. Otolaryngol.-Head Neck Surg. 2009, 140, 473–476. [Google Scholar] [CrossRef]
- Hoppe, U.; Hast, A.; Hocke, T. Sprachverstehen mit Hörgeraten in Abhängigkeit vom Tongehör [Speech recognition with hearing aids depending on pure-tone hearing]. HNO 2014, 62, 443–448. [Google Scholar] [CrossRef]
- McRackan, T.R.; Ahlstrom, J.B.; Clinkscales, W.B.; Meyer, T.A.; Dubno, J.R. Clinical Implications of Word Recognition Differences in Earphone and Aided Conditions. Otol. Neurotol. 2016, 37, 1475–1481. [Google Scholar] [CrossRef]
- McRackan, T.R.; Fabie, J.E.; Burton, J.A.; Munawar, S.; Holcomb, M.A.; Dubno, J.R. Earphone and Aided Word Recognition Differences in Cochlear Implant Candidates. Otol. Neurotol. 2018, 39, e543–e549. [Google Scholar] [CrossRef] [PubMed]
- Kronlachner, M.; Baumann, U.; Stover, T.; Weissgerber, T. Investigation of the quality of hearing aid provision in seniors considering cognitive functions. Laryngorhinootologie 2018, 97, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Franks, Z.G.; Jacob, A. The speech perception gap in cochlear implant patients. Cochlear Implant. Int. 2019, 20, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Dörfler, C.; Hocke, T.; Hast, A.; Hoppe, U. Speech recognition with hearing aids for 10 standard audiograms: English version. HNO 2020, 68, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Beyer, A.; Rieck, J.H.; Mewes, A.; Dambon, J.A.; Hey, M. Extended preoperative speech audiometric diagnostics for cochlear implant treatment. HNO 2023, 71, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, U.; Hocke, T.; Hast, A.; Iro, H. Cochlear Implantation in Candidates With Moderate-to-Severe Hearing Loss and Poor Speech Perception. Laryngoscope 2021, 131, e940–e945. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, U.; Hast, A.; Hocke, T. Validation of a predictive model for speech discrimination after cochlear impIant provision. HNO 2023, 71, 53–59. [Google Scholar] [CrossRef]
- Dziemba, O.C.; Merz, S.; Hocke, T. Evaluative audiometry after cochlear implant provision. HNO 2023, 72, 56–62. [Google Scholar] [CrossRef]
- Rader, T.; Doms, P.; Adel, Y.; Weissgerber, T.; Strieth, S.; Baumann, U. A method for determining precise electrical hearing thresholds in cochlear implant users. Int. J. Audiol. 2018, 57, 502–509. [Google Scholar] [CrossRef]
- Busch, T.; Vanpoucke, F.; Van Wieringen, A. Auditory Environment Across the Life Span of Cochlear Implant Users: Insights From Data Logging. J. Speech Lang. Hear. Res. 2017, 60, 1362–1377. [Google Scholar] [CrossRef]
- Oberhoffner, T.; Hoppe, U.; Hey, M.; Hecker, D.; Bagus, H.; Voigt, P.; Schicktanz, S.; Braun, A.; Hocke, T. Multicentric analysis of the use behavior of cochlear implant users. Laryngorhinootologie 2018, 97, 313–320. [Google Scholar] [CrossRef]
- Glaubitz, C.; Liebscher, T.; Hoppe, U. Children with cochlear implant and additional disabilities benefit from consistent device use. Int. J. Pediatr. Otorhinolaryngol. 2022, 162, 111301. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Cochlear Implants for Children and Adults with Severe to Profound Deafness. 2019. Available online: https://www.nice.org.uk/guidance/ta566 (accessed on 1 December 2023).
- Hahlbrock, K.H. Sprachaudiometrie—Grundlagen und praktische Anwendung Einer Sprachaudiometrie für das Deutsche Sprachgebiet [Speech Audiometry—Basics and Practical Application of Speech Audiometry for the German Language Area]; Georg Thieme Verlag: Stuttgart, Germany, 1957. [Google Scholar]
- Wagener, K.C.; Kühnel, V.; Kollmeier, B. Entwicklung und Evaluation eines Satztests für die deutsche Sprache I: Design des Oldenburger Satztests [Development and evaluation of a sentence test for the German language I: Design of the Oldenburg sentence test]. Z. Für Audiol. 1999, 1, 4–15. [Google Scholar]
- Wagener, K.C.; Kühnel, V.; Kollmeier, B. Entwicklung und Evaluation eines Satztests für die deutsche Sprache II: Optimierung des Oldenburger Satztests [Development and evaluation of a sentence test for the German language II: Optimization of the Oldenburg sentence test]. Z. Für Audiol. 1999, 2, 44–56. [Google Scholar]
- Wagener, K.C.; Kühnel, V.; Kollmeier, B. Entwicklung und Evaluation eines Satztests für die deutsche Sprache III: Evaluation des Oldenburger Satztests [Development and evaluation of a sentence test for the German language III: Evaluation of the Oldenburg sentence test]. Z. Für Audiol. 1999, 3, 86–95. [Google Scholar]
- Hoppe, U.; Hast, A.; Hornung, J.; Hocke, T. Evolving a Model for Cochlear Implant Outcome. J. Clin. Med. 2023, 12, 6215. [Google Scholar] [CrossRef] [PubMed]
- Kießling, J.; Kollmeier, B.; Baumann, U. Versorgung mit Hörgeräten und Hörimplantaten [Provision of Hearing Aids and Hearing Implants], 3rd ed.; Georg Thieme Verlag: Stuttgart, Germany, 2018. [Google Scholar]
- Dryden, A.; Allen, H.A.; Henshaw, H.; Heinrich, A. The Association Between Cognitive Performance and Speech-in-Noise Perception for Adult Listeners: A Systematic Literature Review and Meta-Analysis. Trends Hear. 2017, 21, 2331216517744675. [Google Scholar] [CrossRef] [PubMed]
- Gundogdu, O.; Serbetcioglu, M.B.; Kara, E.; Eser, B.N. Effects of Cognitive Functions on Speech Recognition in Noise in Cochlear Implant Recipients. ORL J. Otorhinolaryngol. Relat. Spec. 2023, 85, 208–214. [Google Scholar] [CrossRef]
- Füllgrabe, C.; Moore, B.C.; Stone, M.A. Age-group differences in speech identification despite matched audiometrically normal hearing: Contributions from auditory temporal processing and cognition. Front. Aging Neurosci. 2014, 6, 347. [Google Scholar] [CrossRef]
- Weissgerber, T.; Müller, C.; Stöver, T.; Baumann, U. Age Differences in Speech Perception in Noise and Sound Localization in Individuals With Subjective Normal Hearing. Front. Psychol. 2022, 13, 845285. [Google Scholar] [CrossRef]
- Holden, L.K.; Finley, C.C.; Firszt, J.B.; Holden, T.A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; Mispagel, K.; Heydebrand, G.; et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear Hear. 2013, 34, 342–360. [Google Scholar] [CrossRef]
- Hoppe, U.; Hocke, T.; Digeser, F. Bimodal benefit for cochlear implant listeners with different grades of hearing loss in the opposite ear. Acta Otolaryngol. 2018, 138, 713–721. [Google Scholar] [CrossRef]
- Hochmair-Desoyer, I.; Schulz, E.; Moser, L.; Schmidt, M. The HSM sentence test as a tool for evaluating the speech understanding in noise of cochlear implant users. Am. J. Otol. 1997, 18, S83. [Google Scholar]
- Smits, C.; Theo Goverts, S.; Festen, J.M. The digits-in-noise test: Assessing auditory speech recognition abilities in noise. J. Acoust. Soc. Am. 2013, 133, 1693–1706. [Google Scholar] [CrossRef]
- Czurda, R.; Wesarg, T.; Aschendorff, A.; Beck, R.L.; Hocke, T.; Ketterer, M.C.; Arndt, S. Investigation of Maximum Monosyllabic Word Recognition as a Predictor of Speech Understanding with Cochlear Implant. J. Clin. Med. 2024, 13, 646. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Estimate | Standard Error | T Statistics | p | |
|---|---|---|---|---|
| Constant, η0 | −0.7434 | 2.6145 | −0.2843 | 0.7772 |
| WRSmax | −0.0030 | 0.0141 | −0.2180 | 0.8282 |
| WRS65(HA) | −0.0102 | 0.0147 | −0.6911 | 0.4925 |
| age, η1 | 0.0408 | 0.0177 | 2.2976 | 0.0256 |
| 4FPTA | −0.0213 | 0.0311 | −0.6857 | 0.4959 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weissgerber, T.; Löschner, M.; Stöver, T.; Baumann, U. Outcome Prediction of Speech Perception in Quiet and in Noise for Cochlear Implant Candidates Based on Pre-Operative Measures. J. Clin. Med. 2024, 13, 994. https://doi.org/10.3390/jcm13040994
Weissgerber T, Löschner M, Stöver T, Baumann U. Outcome Prediction of Speech Perception in Quiet and in Noise for Cochlear Implant Candidates Based on Pre-Operative Measures. Journal of Clinical Medicine. 2024; 13(4):994. https://doi.org/10.3390/jcm13040994
Chicago/Turabian StyleWeissgerber, Tobias, Marcel Löschner, Timo Stöver, and Uwe Baumann. 2024. "Outcome Prediction of Speech Perception in Quiet and in Noise for Cochlear Implant Candidates Based on Pre-Operative Measures" Journal of Clinical Medicine 13, no. 4: 994. https://doi.org/10.3390/jcm13040994
APA StyleWeissgerber, T., Löschner, M., Stöver, T., & Baumann, U. (2024). Outcome Prediction of Speech Perception in Quiet and in Noise for Cochlear Implant Candidates Based on Pre-Operative Measures. Journal of Clinical Medicine, 13(4), 994. https://doi.org/10.3390/jcm13040994