
Recent Treatment Strategies for Acute Pancreatitis

Abstract
1. Introduction
2. Initial Management during the First 72 h
2.1. Assessment of Disease Severity
2.2. Fluid Resuscitation
2.2.1. Goal-Directed Therapy (GDT)
2.2.2. Fluid Type
2.2.3. Fluid Rate and Volume
2.2.4. Fluid Therapy Duration
2.3. Pain Control
2.3.1. Opioids
2.3.2. NSAIDs and Acetaminophen
2.3.3. Epidural Analgesia
2.4. Nutritional Support
2.4.1. When to Start Oral Feeding
2.4.2. Route of Tube Feeding
2.5. Prophylactic Antibiotic Use
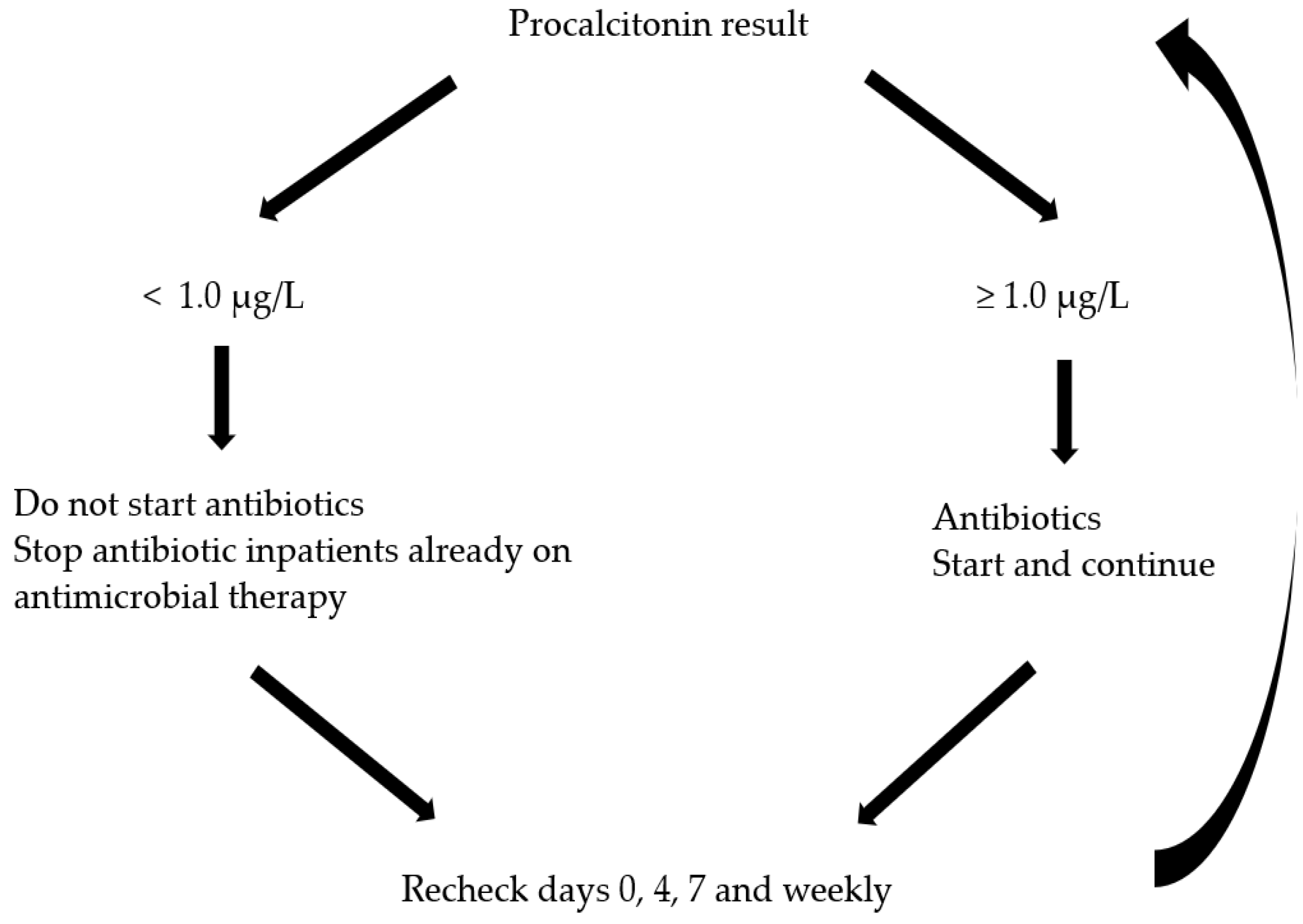
Procalcitonin-Guided Antibiotic Use
2.6. Timing and Role of ERCP and Endoscopic Ultrasonography (EUS) in Gallstone Pancreatitis
2.7. Other Therapeutic Interventions
2.7.1. Insulin and Plasmapheresis for Hypertriglyceridemia Induced AP (HTG-AP)
2.7.2. Low-Molecular-Weight Heparin (LMWH)
2.7.3. Protease Inhibitors
3. Management of Local Complications
3.1. Local Complications in Interstitial Edematous Pancreatitis
3.1.1. Indication of Intervention for Pancreatic Pseudocysts
3.1.2. Method of Intervention for Pancreatic Pseudocysts
3.2. Necrotizing Pancreatitis
3.2.1. Infected Necrosis
- Diagnosis of infected necrosis
3.2.2. Treatment Strategies for Necrotizing Pancreatitis
- Indications of intervention
- Timing of intervention
- Anatomical considerations for intervention
3.2.3. Selection of Interventional Techniques
- Percutaneous drainage
- Endoscopic drainage
- Endoscopic necrosectomy
- Surgical debridement
- Comparison of endoscopic and minimally invasive surgical step-up approach
4. Convalescent Treatment
4.1. Cholecystectomy in Gallstone AP
Timing of Cholecystectomy
4.2. Lipid-Lowering Medications for HTG-AP
4.3. Alcohol Intervention in Alcoholic AP
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mederos, M.A.; Reber, H.A.; Girgis, M.D. Acute pancreatitis: A review. JAMA 2021, 325, 382–390. [Google Scholar] [CrossRef]
- Krishna, S.G.; Kamboj, A.K.; Hart, P.A.; Hinton, A.; Conwell, D.L. The changing epidemiology of acute pancreatitis hospitalizations: A decade of trends and the impact of chronic pancreatitis. Pancreas 2017, 46, 482–488. [Google Scholar] [CrossRef]
- de-Madaria, E.; Buxbaum, J.L. Advances in the management of acute pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 691–692. [Google Scholar] [CrossRef]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S.; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis—2012: Revision of the atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S.; Shanbhag, S.; Chakraborty, M.; Phillips, A.R.; Windsor, J.A. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology 2010, 139, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.U.; Bakker, O.J.; Papachristou, G.I.; Besselink, M.G.; Repas, K.; van Santvoort, H.C.; Muddana, V.; Singh, V.K.; Whitcomb, D.C.; Gooszen, H.G.; et al. Blood urea nitrogen in the early assessment of acute pancreatitis: An international validation study. Arch. Intern. Med. 2011, 171, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Orav, J.; Banks, P.A. Hemoconcentration is an early marker for organ failure and necrotizing pancreatitis. Pancreas 2000, 20, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Koutroumpakis, E.; Wu, B.U.; Bakker, O.J.; Dudekula, A.; Singh, V.K.; Besselink, M.G.; Yadav, D.; Mounzer, R.; van Santvoort, H.C.; Whitcomb, D.C.; et al. Admission hematocrit and rise in blood urea nitrogen at 24 h outperform other laboratory markers in predicting persistent organ failure and pancreatic necrosis in acute pancreatitis: A post hoc analysis of three large prospective databases. Am. J. Gastroenterol. 2015, 110, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- Sathyanarayan, G.; Garg, P.K.; Prasad, H.; Tandon, R.K. Elevated level of interleukin-6 predicts organ failure and severe disease in patients with acute pancreatitis. J. Gastroenterol. Hepatol. 2007, 22, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.H.; Hu, C.; Cai, W.H.; Chen, W.W.; Zhang, X.X.; Shi, N.; Huang, W.; Ma, Y.; Jin, T.; Lin, Z.Q.; et al. Plasma cytokines can help to identify the development of severe acute pancreatitis on admission. Medicine 2017, 96, e7312. [Google Scholar] [CrossRef]
- Papachristou, G.I. Prediction of severe acute pancreatitis: Current knowledge and novel insights. World J. Gastroenterol. 2008, 14, 6273–6275. [Google Scholar] [CrossRef] [PubMed]
- Mentula, P.; Kylanpaa, M.L.; Kemppainen, E.; Jansson, S.E.; Sarna, S.; Puolakkainen, P.; Haapiainen, R.; Repo, H. Early prediction of organ failure by combined markers in patients with acute pancreatitis. Br. J. Surg. 2005, 92, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Di, M.Y.; Liu, H.; Yang, Z.Y.; Bonis, P.A.; Tang, J.L.; Lau, J. Prediction models of mortality in acute pancreatitis in adults: A systematic review. Ann. Intern. Med. 2016, 165, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.U.; Johannes, R.S.; Sun, X.; Tabak, Y.; Conwell, D.L.; Banks, P.A. The early prediction of mortality in acute pancreatitis: A large population-based study. Gut 2008, 57, 1698–1703. [Google Scholar] [CrossRef] [PubMed]
- Mounzer, R.; Langmead, C.J.; Wu, B.U.; Evans, A.C.; Bishehsari, F.; Muddana, V.; Singh, V.K.; Slivka, A.; Whitcomb, D.C.; Yadav, D.; et al. Comparison of existing clinical scoring systems to predict persistent organ failure in patients with acute pancreatitis. Gastroenterology 2012, 142, 1476–1482. [Google Scholar] [CrossRef] [PubMed]
- Forsmark, C.E.; Yadav, D. Predicting the prognosis of acute pancreatitis. Ann. Intern. Med. 2016, 165, 523–524. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.J.; Papachristou, G.I. New insights into acute pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 479–496. [Google Scholar] [CrossRef] [PubMed]
- Mofidi, R.; Duff, M.D.; Wigmore, S.J.; Madhavan, K.K.; Garden, O.J.; Parks, R.W. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. Br. J. Surg. 2006, 93, 738–744. [Google Scholar] [CrossRef]
- Singh, V.K.; Wu, B.U.; Bollen, T.L.; Repas, K.; Maurer, R.; Mortele, K.J.; Banks, P.A. Early systemic inflammatory response syndrome is associated with severe acute pancreatitis. Clin. Gastroenterol. Hepatol. 2009, 7, 1247–1251. [Google Scholar] [CrossRef]
- Kui, B.; Pinter, J.; Molontay, R.; Nagy, M.; Farkas, N.; Gede, N.; Vincze, A.; Bajor, J.; Godi, S.; Czimmer, J.; et al. Easy-app: An artificial intelligence model and application for early and easy prediction of severity in acute pancreatitis. Clin. Transl. Med. 2022, 12, e842. [Google Scholar] [CrossRef]
- Lee, A.; Ko, C.; Buitrago, C.; Hiramoto, B.; Hilson, L.; Buxbaum, J.; Group, N.-L.S. Lactated ringers vs normal saline resuscitation for mild acute pancreatitis: A randomized trial. Gastroenterology 2021, 160, 955–957.e954. [Google Scholar] [CrossRef]
- Myburgh, J.A.; Finfer, S.; Bellomo, R.; Billot, L.; Cass, A.; Gattas, D.; Glass, P.; Lipman, J.; Liu, B.; McArthur, C.; et al. Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N. Engl. J. Med. 2012, 367, 1901–1911. [Google Scholar] [CrossRef]
- de-Madaria, E.; Buxbaum, J.L.; Maisonneuve, P.; Garcia Garcia de Paredes, A.; Zapater, P.; Guilabert, L.; Vaillo-Rocamora, A.; Rodriguez-Gandia, M.A.; Donate-Ortega, J.; Lozada-Hernandez, E.E.; et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N. Engl. J. Med. 2022, 387, 989–1000. [Google Scholar] [CrossRef]
- Buxbaum, J.L.; Quezada, M.; Da, B.; Jani, N.; Lane, C.; Mwengela, D.; Kelly, T.; Jhun, P.; Dhanireddy, K.; Laine, L. Early aggressive hydration hastens clinical improvement in mild acute pancreatitis. Am. J. Gastroenterol. 2017, 112, 797–803. [Google Scholar] [CrossRef]
- de-Madaria, E.; Soler-Sala, G.; Sanchez-Paya, J.; Lopez-Font, I.; Martinez, J.; Gomez-Escolar, L.; Sempere, L.; Sanchez-Fortun, C.; Perez-Mateo, M. Influence of fluid therapy on the prognosis of acute pancreatitis: A prospective cohort study. Am. J. Gastroenterol. 2011, 106, 1843–1850. [Google Scholar] [CrossRef]
- De Waele, J.J.; Leppaniemi, A.K. Intra-abdominal hypertension in acute pancreatitis. World J. Surg. 2009, 33, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Wilms, H.; Mittal, A.; Haydock, M.D.; van den Heever, M.; Devaud, M.; Windsor, J.A. A systematic review of goal directed fluid therapy: Rating of evidence for goals and monitoring methods. J. Crit. Care 2014, 29, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Crockett, S.D.; Wani, S.; Gardner, T.B.; Falck-Ytter, Y.; Barkun, A.N.; American Gastroenterological Association Institute Clinical Guidelines Committee. American gastroenterological association institute guideline on initial management of acute pancreatitis. Gastroenterology 2018, 154, 1096–1101. [Google Scholar] [CrossRef]
- Lee, S.H.; Choe, J.W.; Cheon, Y.K.; Choi, M.; Jung, M.K.; Jang, D.K.; Jo, J.H.; Lee, J.M.; Kim, E.J.; Han, S.Y.; et al. Revised clinical practice guidelines of the korean pancreatobiliary association for acute pancreatitis. Gut Liver. 2023, 17, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Yokoe, M.; Takada, T.; Mayumi, T.; Yoshida, M.; Isaji, S.; Wada, K.; Itoi, T.; Sata, N.; Gabata, T.; Igarashi, H.; et al. Japanese guidelines for the management of acute pancreatitis: Japanese guidelines 2015. J. Hepatobiliary Pancreat. Sci. 2015, 22, 405–432. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.U.; Johannes, R.S.; Sun, X.; Conwell, D.L.; Banks, P.A. Early changes in blood urea nitrogen predict mortality in acute pancreatitis. Gastroenterology 2009, 137, 129–135. [Google Scholar] [CrossRef]
- Brown, A.; Baillargeon, J.D.; Hughes, M.D.; Banks, P.A. Can fluid resuscitation prevent pancreatic necrosis in severe acute pancreatitis? Pancreatology 2002, 2, 104–107. [Google Scholar] [CrossRef]
- Jin, T.; Li, L.; Deng, L.; Wen, S.; Zhang, R.; Shi, N.; Zhu, P.; Lan, L.; Lin, Z.; Jiang, K.; et al. Hemoconcentration is associated with early faster fluid rate and increased risk of persistent organ failure in acute pancreatitis patients. JGH Open 2020, 4, 684–691. [Google Scholar] [CrossRef]
- Crosignani, A.; Spina, S.; Marrazzo, F.; Cimbanassi, S.; Malbrain, M.; Van Regenmortel, N.; Fumagalli, R.; Langer, T. Intravenous fluid therapy in patients with severe acute pancreatitis admitted to the intensive care unit: A narrative review. Ann. Intensive Care 2022, 12, 98. [Google Scholar] [CrossRef]
- Jin, T.; Li, L.; Zhu, P.; Deng, L.; Zhang, X.; Hu, C.; Shi, N.; Zhang, R.; Tan, Q.; Chen, C.; et al. Optimising fluid requirements after initial resuscitation: A pilot study evaluating mini-fluid challenge and passive leg raising test in patients with predicted severe acute pancreatitis. Pancreatology 2022, 22, 894–901. [Google Scholar] [CrossRef]
- Zhou, S.; Buitrago, C.; Foong, A.; Lee, V.; Dawit, L.; Hiramoto, B.; Chang, P.; Schilperoort, H.; Lee, A.; de-Madaria, E.; et al. Comprehensive meta-analysis of randomized controlled trials of lactated ringer’s versus normal saline for acute pancreatitis. Pancreatology 2021, 21, 1405–1410. [Google Scholar] [CrossRef] [PubMed]
- Semler, M.W.; Self, W.H.; Wanderer, J.P.; Ehrenfeld, J.M.; Wang, L.; Byrne, D.W.; Stollings, J.L.; Kumar, A.B.; Hughes, C.G.; Hernandez, A.; et al. Balanced crystalloids versus saline in critically ill adults. N. Engl. J. Med. 2018, 378, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Semler, M.W.; Wanderer, J.P.; Wang, L.; Byrne, D.W.; Collins, S.P.; Slovis, C.M.; Lindsell, C.J.; Ehrenfeld, J.M.; Siew, E.D.; et al. Balanced crystalloids versus saline in noncritically ill adults. N. Engl. J. Med. 2018, 378, 819–828. [Google Scholar] [CrossRef] [PubMed]
- de-Madaria, E.; Herrera-Marante, I.; Gonzalez-Camacho, V.; Bonjoch, L.; Quesada-Vazquez, N.; Almenta-Saavedra, I.; Miralles-Macia, C.; Acevedo-Piedra, N.G.; Roger-Ibanez, M.; Sanchez-Marin, C.; et al. Fluid resuscitation with lactated ringer’s solution vs normal saline in acute pancreatitis: A triple-blind, randomized, controlled trial. United Eur. Gastroenterol. J. 2018, 6, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Zhang, J.G.; Wu, H.S.; Tao, J.; Qin, Q.; Deng, S.C.; Liu, Y.; Liu, L.; Wang, B.; Tian, K.; et al. Effects of different resuscitation fluid on severe acute pancreatitis. World J. Gastroenterol. 2013, 19, 2044–2052. [Google Scholar] [CrossRef] [PubMed]
- Du, X.J.; Hu, W.M.; Xia, Q.; Huang, Z.W.; Chen, G.Y.; Jin, X.D.; Xue, P.; Lu, H.M.; Ke, N.W.; Zhang, Z.D.; et al. Hydroxyethyl starch resuscitation reduces the risk of intra-abdominal hypertension in severe acute pancreatitis. Pancreas 2011, 40, 1220–1225. [Google Scholar] [CrossRef]
- Ma, Y.; Yan, T.; Xu, F.; Ding, J.; Yang, B.; Ma, Q.; Wu, Z.; Lyu, J.; Wang, Z. Infusion of human albumin on acute pancreatitis therapy: New tricks for old dog? Front. Pharmacol. 2022, 13, 842108. [Google Scholar] [CrossRef]
- Working Group IAP/APA Acute Pancreatitis Guidelines. Iap/apa evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013, 13, e1–e15. [Google Scholar] [CrossRef] [PubMed]
- Mao, E.Q.; Tang, Y.Q.; Fei, J.; Qin, S.; Wu, J.; Li, L.; Min, D.; Zhang, S.D. Fluid therapy for severe acute pancreatitis in acute response stage. Chin. Med. J. 2009, 122, 169–173. [Google Scholar] [CrossRef]
- Mao, E.Q.; Fei, J.; Peng, Y.B.; Huang, J.; Tang, Y.Q.; Zhang, S.D. Rapid hemodilution is associated with increased sepsis and mortality among patients with severe acute pancreatitis. Chin. Med. J. 2010, 123, 1639–1644. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.U.; Hwang, J.Q.; Gardner, T.H.; Repas, K.; Delee, R.; Yu, S.; Smith, B.; Banks, P.A.; Conwell, D.L. Lactated ringer’s solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin. Gastroenterol. Hepatol. 2011, 9, 710–717.e711. [Google Scholar] [CrossRef] [PubMed]
- Cuellar-Monterrubio, J.E.; Monreal-Robles, R.; Gonzalez-Moreno, E.I.; Borjas-Almaguer, O.D.; Herrera-Elizondo, J.L.; Garcia-Compean, D.; Maldonado-Garza, H.J.; Gonzalez-Gonzalez, J.A. Nonaggressive versus aggressive intravenous fluid therapy in acute pancreatitis with more than 24 hours from disease onset: A randomized controlled trial. Pancreas 2020, 49, 579–583. [Google Scholar] [CrossRef]
- Yaowmaneerat, T.; Sirinawasatien, A. Update on the strategy for intravenous fluid treatment in acute pancreatitis. World J. Gastrointest. Pharmacol. Ther. 2023, 14, 22–32. [Google Scholar] [CrossRef]
- Gulen, B.; Dur, A.; Serinken, M.; Karcioglu, O.; Sonmez, E. Pain treatment in patients with acute pancreatitis: A randomized controlled trial. Turk. J. Gastroenterol. 2016, 27, 192–196. [Google Scholar] [CrossRef]
- Basurto Ona, X.; Rigau Comas, D.; Urrutia, G. Opioids for acute pancreatitis pain. Cochrane Database Syst. Rev. 2013, 26, CD009179. [Google Scholar] [CrossRef]
- Saini, M.; Samanta, J.; Kumar, A.; Choudhury, A.; Dhar, J.; Jafra, A.; Chauhan, R.; Muktesh, G.; Gupta, P.; Gupta, V.; et al. Buprenorphine versus diclofenac for pain relief in acute pancreatitis: A double-blinded randomized controlled trial. Clin. Gastroenterol. Hepatol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Jabaudon, M.; Genevrier, A.; Jaber, S.; Windisch, O.; Bulyez, S.; Laterre, P.F.; Escudier, E.; Sossou, A.; Guerci, P.; Bertrand, P.M.; et al. Thoracic epidural analgesia in intensive care unit patients with acute pancreatitis: The epipan multicenter randomized controlled trial. Crit. Care 2023, 27, 213. [Google Scholar] [CrossRef] [PubMed]
- Louie, B.E.; Noseworthy, T.; Hailey, D.; Gramlich, L.M.; Jacobs, P.; Warnock, G.L. 2004 maclean-mueller prize enteral or parenteral nutrition for severe pancreatitis: A randomized controlled trial and health technology assessment. Can. J. Surg. 2005, 48, 298–306. [Google Scholar] [PubMed]
- Al-Omran, M.; Albalawi, Z.H.; Tashkandi, M.F.; Al-Ansary, L.A. Enteral versus parenteral nutrition for acute pancreatitis. Cochrane Database Syst. Rev. 2010, 2010, CD002837. [Google Scholar] [CrossRef] [PubMed]
- Petrov, M.S.; Pylypchuk, R.D.; Uchugina, A.F. A systematic review on the timing of artificial nutrition in acute pancreatitis. Br. J. Nutr. 2009, 101, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Windsor, A.C.; Kanwar, S.; Li, A.G.; Barnes, E.; Guthrie, J.A.; Spark, J.I.; Welsh, F.; Guillou, P.J.; Reynolds, J.V. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. Gut 1998, 42, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Bakker, O.J.; van Brunschot, S.; van Santvoort, H.C.; Besselink, M.G.; Bollen, T.L.; Boermeester, M.A.; Dejong, C.H.; van Goor, H.; Bosscha, K.; Ahmed Ali, U.; et al. Early versus on-demand nasoenteric tube feeding in acute pancreatitis. N. Engl. J. Med. 2014, 371, 1983–1993. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Maldonado, E.; Lopez Gordo, S.; Pueyo, E.M.; Sanchez-Garcia, A.; Mayol, S.; Gonzalez, S.; Elvira, J.; Memba, R.; Fondevila, C.; Jorba, R. Immediate oral refeeding in patients with mild and moderate acute pancreatitis: A multicenter, randomized controlled trial (padi trial). Ann. Surg. 2021, 274, 255–263. [Google Scholar] [CrossRef]
- Vege, S.S.; DiMagno, M.J.; Forsmark, C.E.; Martel, M.; Barkun, A.N. Initial medical treatment of acute pancreatitis: American gastroenterological association institute technical review. Gastroenterology 2018, 154, 1103–1139. [Google Scholar] [CrossRef]
- Werge, M.; Novovic, S.; Schmidt, P.N.; Gluud, L.L. Infection increases mortality in necrotizing pancreatitis: A systematic review and meta-analysis. Pancreatology 2016, 16, 698–707. [Google Scholar] [CrossRef]
- Wittau, M.; Mayer, B.; Scheele, J.; Henne-Bruns, D.; Dellinger, E.P.; Isenmann, R. Systematic review and meta-analysis of antibiotic prophylaxis in severe acute pancreatitis. Scand. J. Gastroenterol. 2011, 46, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Baltatzis, M.; Mason, J.M.; Chandrabalan, V.; Stathakis, P.; McIntyre, B.; Jegatheeswaran, S.; Jamdar, S.; O’Reilly, D.A.; Siriwardena, A.K. Antibiotic use in acute pancreatitis: An audit of current practice in a tertiary centre. Pancreatology 2016, 16, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Parniczky, A.; Lantos, T.; Toth, E.M.; Szakacs, Z.; Godi, S.; Hagendorn, R.; Illes, D.; Koncz, B.; Marta, K.; Miko, A.; et al. Antibiotic therapy in acute pancreatitis: From global overuse to evidence based recommendations. Pancreatology 2019, 19, 488–499. [Google Scholar] [CrossRef]
- Siriwardena, A.K.; Jegatheeswaran, S.; Mason, J.M.; PROCAP investigators. A procalcitonin-based algorithm to guide antibiotic use in patients with acute pancreatitis (procap): A single-centre, patient-blinded, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2022, 7, 913–921. [Google Scholar] [CrossRef]
- Yadav, D.; Lowenfels, A.B. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013, 144, 1252–1261. [Google Scholar] [CrossRef] [PubMed]
- Lerch, M.M.; Saluja, A.K.; Runzi, M.; Dawra, R.; Saluja, M.; Steer, M.L. Pancreatic duct obstruction triggers acute necrotizing pancreatitis in the opossum. Gastroenterology 1993, 104, 853–861. [Google Scholar] [CrossRef]
- Fan, S.T.; Lai, E.C.; Mok, F.P.; Lo, C.M.; Zheng, S.S.; Wong, J. Early treatment of acute biliary pancreatitis by endoscopic papillotomy. N. Engl. J. Med. 1993, 328, 228–232. [Google Scholar] [CrossRef]
- van Santvoort, H.C.; Besselink, M.G.; de Vries, A.C.; Boermeester, M.A.; Fischer, K.; Bollen, T.L.; Cirkel, G.A.; Schaapherder, A.F.; Nieuwenhuijs, V.B.; van Goor, H.; et al. Early endoscopic retrograde cholangiopancreatography in predicted severe acute biliary pancreatitis: A prospective multicenter study. Ann. Surg. 2009, 250, 68–75. [Google Scholar] [CrossRef]
- Hallensleben, N.D.; Stassen, P.M.C.; Schepers, N.J.; Besselink, M.G.; Anten, M.G.F.; Bakker, O.J.; Bollen, T.L.; da Costa, D.W.; van Dijk, S.M.; van Dullemen, H.M.; et al. Patient selection for urgent endoscopic retrograde cholangio-pancreatography by endoscopic ultrasound in predicted severe acute biliary pancreatitis (apec-2): A multicentre prospective study. Gut 2023, 72, 1534–1542. [Google Scholar] [CrossRef]
- Schepers, N.J.; Hallensleben, N.D.L.; Besselink, M.G.; Anten, M.G.F.; Bollen, T.L.; da Costa, D.W.; van Delft, F.; van Dijk, S.M.; van Dullemen, H.M.; Dijkgraaf, M.G.W.; et al. Urgent endoscopic retrograde cholangiopancreatography with sphincterotomy versus conservative treatment in predicted severe acute gallstone pancreatitis (apec): A multicentre randomised controlled trial. Lancet 2020, 396, 167–176. [Google Scholar] [CrossRef]
- Yan, L.H.; Hu, X.H.; Chen, R.X.; Pan, M.M.; Han, Y.C.; Gao, M.; Liu, H. Plasmapheresis compared with conventional treatment for hypertriglyceridemia-induced acute pancreatitis: A systematic review and meta-analysis. J. Clin. Apher. 2023, 38, 4–15. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, J.; Wu, L.; Lin, J.; Liang, Y. Blood purification for hypertriglyceridemia-induced acute pancreatitis: A meta-analysis. Pancreas 2022, 51, 531–539. [Google Scholar] [CrossRef]
- Dhindsa, S.; Sharma, A.; Al-Khazaali, A.; Sitaula, S.; Nadella, S.; McKee, A.; Albert, S.; Bourey, R.; Dandona, P. Intravenous insulin versus conservative management in hypertriglyceridemia-associated acute pancreatitis. J. Endocr. Soc. 2020, 4, bvz019. [Google Scholar] [CrossRef]
- Berberich, A.J.; Ziada, A.; Zou, G.Y.; Hegele, R.A. Conservative management in hypertriglyceridemia-associated pancreatitis. J. Intern. Med. 2019, 286, 644–650. [Google Scholar] [CrossRef]
- Zádori, N.; Gede, N.; Antal, J.; Szentesi, A.; Alizadeh, H.; Vincze, Á.; Izbéki, F.; Papp, M.; Czakó, L.; Varga, M.; et al. Early elimination of fatty acids in hypertriglyceridemia-induced acute pancreatitis (elefant trial): Protocol of an open-label, multicenter, adaptive randomized clinical trial. Pancreatol. Off. J. Int. Assoc. Pancreatol. (IAP) 2020, 20, 369–376. [Google Scholar] [CrossRef]
- Patil, B.; Meena, L.N.; Sharma, D.C.; Agarwal, G.; Dadhich, Y.; Gupta, G. Impact of low-molecular-weight heparin in the treatment of moderately severe and severe acute pancreatitis; a randomized, single blind, phase 3 control trial. Int. J. Surg. 2022, 101, 106621. [Google Scholar] [CrossRef] [PubMed]
- Seta, T.; Noguchi, Y.; Shikata, S.; Nakayama, T. Treatment of acute pancreatitis with protease inhibitors administered through intravenous infusion: An updated systematic review and meta-analysis. BMC Gastroenterol. 2014, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Liu, Y.; Zhou, S.F.; Qiu, P.; Xu, L.; Wen, P.; Wen, J.; Xiao, X. Effect of somatostatin, ulinastatin and gabexate on the treatment of severe acute pancreatitis. Am. J. Med. Sci. 2016, 351, 506–512. [Google Scholar] [CrossRef] [PubMed]
- van Grinsven, J.; van Brunschot, S.; van Baal, M.C.; Besselink, M.G.; Fockens, P.; van Goor, H.; van Santvoort, H.C.; Bollen, T.L.; Dutch Pancreatitis Study, G. Natural history of gas configurations and encapsulation in necrotic collections during necrotizing pancreatitis. J. Gastrointest. Surg. 2018, 22, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Lenhart, D.K.; Balthazar, E.J. Mdct of acute mild (nonnecrotizing) pancreatitis: Abdominal complications and fate of fluid collections. AJR Am. J. Roentgenol. 2008, 190, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.L.; Kim, K.H.; Kim, H.G.; Han, J.; Kim, H.; Cho, K.B.; Jung, M.K.; Cho, C.M.; Kim, T.N. Incidence, risk factors and clinical course of pancreatic fluid collections in acute pancreatitis. Dig. Dis. Sci. 2014, 59, 1055–1062. [Google Scholar] [CrossRef]
- Fabbri, C.; Luigiano, C.; Lisotti, A.; Cennamo, V.; Virgilio, C.; Caletti, G.; Fusaroli, P. Endoscopic ultrasound-guided treatments: Are we getting evidence based—A systematic review. World J. Gastroenterol. 2014, 20, 8424–8448. [Google Scholar] [CrossRef]
- Keane, M.G.; Sze, S.F.; Cieplik, N.; Murray, S.; Johnson, G.J.; Webster, G.J.; Thorburn, D.; Pereira, S.P. Endoscopic versus percutaneous drainage of symptomatic pancreatic fluid collections: A 14-year experience from a tertiary hepatobiliary centre. Surg. Endosc. 2016, 30, 3730–3740. [Google Scholar] [CrossRef] [PubMed]
- Varadarajulu, S.; Bang, J.Y.; Sutton, B.S.; Trevino, J.M.; Christein, J.D.; Wilcox, C.M. Equal efficacy of endoscopic and surgical cystogastrostomy for pancreatic pseudocyst drainage in a randomized trial. Gastroenterology 2013, 145, 583–590.e581. [Google Scholar] [CrossRef] [PubMed]
- Catalano, M.F.; Geenen, J.E.; Schmalz, M.J.; Johnson, G.K.; Dean, R.S.; Hogan, W.J. Treatment of pancreatic pseudocysts with ductal communication by transpapillary pancreatic duct endoprosthesis. Gastrointest. Endosc. 1995, 42, 214–218. [Google Scholar] [CrossRef]
- Tenner, S.; Baillie, J.; DeWitt, J.; Vege, S.S.; American College of Gastroenterology. American college of gastroenterology guideline: Management of acute pancreatitis. Am. J. Gastroenterol. 2013, 108, 1400–1415. [Google Scholar] [CrossRef]
- Banks, P.A.; Freeman, M.L.; Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am. J. Gastroenterol. 2006, 101, 2379–2400. [Google Scholar] [CrossRef]
- van Baal, M.C.; Bollen, T.L.; Bakker, O.J.; van Goor, H.; Boermeester, M.A.; Dejong, C.H.; Gooszen, H.G.; van der Harst, E.; van Eijck, C.H.; van Santvoort, H.C.; et al. The role of routine fine-needle aspiration in the diagnosis of infected necrotizing pancreatitis. Surgery 2014, 155, 442–448. [Google Scholar] [CrossRef]
- Banks, P.A.; Gerzof, S.G.; Langevin, R.E.; Silverman, S.G.; Sica, G.T.; Hughes, M.D. Ct-guided aspiration of suspected pancreatic infection: Bacteriology and clinical outcome. Int. J. Pancreatol. 1995, 18, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Baron, T.H.; DiMaio, C.J.; Wang, A.Y.; Morgan, K.A. American gastroenterological association clinical practice update: Management of pancreatic necrosis. Gastroenterology 2020, 158, 67–75.e61. [Google Scholar] [CrossRef]
- van Santvoort, H.C.; Bakker, O.J.; Bollen, T.L.; Besselink, M.G.; Ahmed Ali, U.; Schrijver, A.M.; Boermeester, M.A.; van Goor, H.; Dejong, C.H.; van Eijck, C.H.; et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011, 141, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Boxhoorn, L.; van Dijk, S.M.; van Grinsven, J.; Verdonk, R.C.; Boermeester, M.A.; Bollen, T.L.; Bouwense, S.A.W.; Bruno, M.J.; Cappendijk, V.C.; Dejong, C.H.C.; et al. Immediate versus postponed intervention for infected necrotizing pancreatitis. N. Engl. J. Med. 2021, 385, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.R.; Razo, A.O.; Targarona, J.; Thayer, S.P.; Rattner, D.W.; Warshaw, A.L.; Fernandez-del Castillo, C. Debridement and closed packing for sterile or infected necrotizing pancreatitis: Insights into indications and outcomes in 167 patients. Ann. Surg. 2008, 247, 294–299. [Google Scholar] [CrossRef]
- Kivilaakso, E.; Lempinen, M.; Makelainen, A.; Nikki, P.; Schroder, T. Pancreatic resection versus peritoneal lavation for acute fulminant pancreatitis. A randomized prospective study. Ann. Surg. 1984, 199, 426–431. [Google Scholar] [CrossRef] [PubMed]
- van Santvoort, H.C.; Besselink, M.G.; Bakker, O.J.; Hofker, H.S.; Boermeester, M.A.; Dejong, C.H.; van Goor, H.; Schaapherder, A.F.; van Eijck, C.H.; Bollen, T.L.; et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N. Engl. J. Med. 2010, 362, 1491–1502. [Google Scholar] [CrossRef]
- Elmunzer, B.J. Endoscopic drainage of pancreatic fluid collections. Clin. Gastroenterol. Hepatol. 2018, 16, 1851–1863.e1853. [Google Scholar] [CrossRef]
- Li, A.Y.; Bergquist, J.R.; Visser, B.C. Necrosectomy in the management of necrotizing pancreatitis. Adv. Surg. 2021, 55, 231–250. [Google Scholar] [CrossRef]
- van Brunschot, S.; van Grinsven, J.; van Santvoort, H.C.; Bakker, O.J.; Besselink, M.G.; Boermeester, M.A.; Bollen, T.L.; Bosscha, K.; Bouwense, S.A.; Bruno, M.J.; et al. Endoscopic or surgical step-up approach for infected necrotising pancreatitis: A multicentre randomised trial. Lancet 2018, 391, 51–58. [Google Scholar] [CrossRef]
- van Baal, M.C.; van Santvoort, H.C.; Bollen, T.L.; Bakker, O.J.; Besselink, M.G.; Gooszen, H.G.; Grp, D.P.S. Systematic review of percutaneous catheter drainage as primary treatment for necrotizing pancreatitis. Brit. J. Surg. 2011, 98, 18–27. [Google Scholar] [CrossRef]
- Varadarajulu, S.; Christein, J.D.; Tamhane, A.; Drelichman, E.R.; Wilcox, C.M. Prospective randomized trial comparing eus and egd for transmural drainage of pancreatic pseudocysts (with videos). Gastrointest. Endosc. 2008, 68, 1102–1111. [Google Scholar] [CrossRef]
- Park, D.H.; Lee, S.S.; Moon, S.H.; Choi, S.Y.; Jung, S.W.; Seo, D.W.; Lee, S.K.; Kim, M.H. Endoscopic ultrasound-guided versus conventional transmural drainage for pancreatic pseudocysts: A prospective randomized trial. Endoscopy 2009, 41, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Calderón, E.; Chacaltana, A.; Díaz, R.; Li, B.; Martinez-Moreno, B.; Aparicio, J.R. Head-to-head comparison between endoscopic ultrasound guided lumen apposing metal stent and plastic stents for the treatment of pancreatic fluid collections: A systematic review and meta-analysis. J. Hepato.-Bil.-Pan. Sci. 2022, 29, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Navaneethan, U.; Hasan, M.K.; Sutton, B.; Hawes, R.; Varadarajulu, S. Non-superiority of lumen-apposing metal stents over plastic stents for drainage of walled-off necrosis in a randomised trial. Gut 2019, 68, 1200–1209. [Google Scholar] [CrossRef] [PubMed]
- Karstensen, J.G.; Novovic, S.; Hansen, E.F.; Jensen, A.B.; Jorgensen, H.L.; Lauritsen, M.L.; Werge, M.P.; Schmidt, P.N. Eus-guided drainage of large walled-off pancreatic necroses using plastic versus lumen-apposing metal stents: A single-centre randomised controlled trial. Gut 2023, 72, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Boxhoorn, L.; Verdonk, R.C.; Besselink, M.G.; Boermeester, M.; Bollen, T.L.; Bouwense, S.A.; Cappendijk, V.C.; Curvers, W.L.; Dejong, C.H.; van Dijk, S.M.; et al. Comparison of lumen-apposing metal stents versus double-pigtail plastic stents for infected necrotising pancreatitis. Gut 2023, 72, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Vanek, P.; Falt, P.; Vitek, P.; Zoundjiekpon, V.; Horinkova, M.; Zapletalova, J.; Lovecek, M.; Urban, O. Eus-guided transluminal drainage using lumen-apposing metal stents with or without coaxial plastic stents for treatment of walled-off necrotizing pancreatitis: A prospective bicentric randomized controlled trial. Gastrointest. Endosc. 2023, 97, 1070–1080. [Google Scholar] [CrossRef]
- Gardner, T.B.; Coelho-Prabhu, N.; Gordon, S.R.; Gelrud, A.; Maple, J.T.; Papachristou, G.I.; Freeman, M.L.; Topazian, M.D.; Attam, R.; Mackenzie, T.A.; et al. Direct endoscopic necrosectomy for the treatment of walled-off pancreatic necrosis: Results from a multicenter U.S. Series. Gastrointest. Endosc. 2011, 73, 718–726. [Google Scholar] [CrossRef]
- van Brunschot, S.; Fockens, P.; Bakker, O.J.; Besselink, M.G.; Voermans, R.P.; Poley, J.W.; Gooszen, H.G.; Bruno, M.; van Santvoort, H.C. Endoscopic transluminal necrosectomy in necrotising pancreatitis: A systematic review. Surg. Endosc. 2014, 28, 1425–1438. [Google Scholar] [CrossRef]
- Garg, R.; Gupta, S.; Singh, A.; Simonson, M.T.; Rustagi, T.; Chahal, P. Hydrogen peroxide assisted endoscopic necrosectomy for walled-off pancreatic necrosis: A systematic review and meta-analysis. Pancreatology 2021, 21, 1540–1547. [Google Scholar] [CrossRef]
- Messallam, A.A.; Adler, D.G.; Shah, R.J.; Nieto, J.M.; Moran, R.; Elmunzer, B.J.; Cosgrove, N.; Mullady, D.; Singh, H.; Cote, G.; et al. Direct endoscopic necrosectomy with and without hydrogen peroxide for walled-off pancreatic necrosis: A multicenter comparative study. Am. J. Gastroenterol. 2021, 116, 700–709. [Google Scholar] [CrossRef]
- Raraty, M.G.; Halloran, C.M.; Dodd, S.; Ghaneh, P.; Connor, S.; Evans, J.; Sutton, R.; Neoptolemos, J.P. Minimal access retroperitoneal pancreatic necrosectomy: Improvement in morbidity and mortality with a less invasive approach. Ann. Surg. 2010, 251, 787–793. [Google Scholar] [CrossRef]
- Bradley, E.L., 3rd; Howard, T.J.; van Sonnenberg, E.; Fotoohi, M. Intervention in necrotizing pancreatitis: An evidence-based review of surgical and percutaneous alternatives. J. Gastrointest. Surg. 2008, 12, 634–639. [Google Scholar] [CrossRef]
- Bakker, O.J.; van Santvoort, H.C.; van Brunschot, S.; Geskus, R.B.; Besselink, M.G.; Bollen, T.L.; van Eijck, C.H.; Fockens, P.; Hazebroek, E.J.; Nijmeijer, R.M.; et al. Endoscopic transgastric vs surgical necrosectomy for infected necrotizing pancreatitis: A randomized trial. JAMA 2012, 307, 1053–1061. [Google Scholar] [CrossRef]
- Bang, J.Y.; Arnoletti, J.P.; Holt, B.A.; Sutton, B.; Hasan, M.K.; Navaneethan, U.; Feranec, N.; Wilcox, C.M.; Tharian, B.; Hawes, R.H.; et al. An endoscopic transluminal approach, compared with minimally invasive surgery, reduces complications and costs for patients with necrotizing pancreatitis. Gastroenterology 2019, 156, 1027–1040.e1023. [Google Scholar] [CrossRef]
- Wysocki, A.P.; McKay, C.J.; Carter, C.R. Infected pancreatic necrosis: Minimizing the cut. ANZ J. Surg. 2010, 80, 58–70. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.K.; Zyromski, N.J.; Freeman, M.L. Infected necrotizing pancreatitis: Evolving interventional strategies from minimally invasive surgery to endoscopic therapy-evidence mounts, but one size does not fit all. Gastroenterology 2019, 156, 867–871. [Google Scholar] [CrossRef] [PubMed]
- Trikudanathan, G.; Tawfik, P.; Amateau, S.K.; Munigala, S.; Arain, M.; Attam, R.; Beilman, G.; Flanagan, S.; Freeman, M.L.; Mallery, S. Early (<4 weeks) versus standard (>/= 4 weeks) endoscopically centered step-up interventions for necrotizing pancreatitis. Am. J. Gastroenterol. 2018, 113, 1550–1558. [Google Scholar] [PubMed]
- Onnekink, A.M.; Boxhoorn, L.; Timmerhuis, H.C.; Bac, S.T.; Besselink, M.G.; Boermeester, M.A.; Bollen, T.L.; Bosscha, K.; Bouwense, S.A.W.; Bruno, M.J.; et al. Endoscopic versus surgical step-up approach for infected necrotizing pancreatitis (extension): Long-term follow-up of a randomized trial. Gastroenterology 2022, 163, 712–722.e714. [Google Scholar] [CrossRef] [PubMed]
- Boerma, D.; Rauws, E.A.; Keulemans, Y.C.; Janssen, I.M.; Bolwerk, C.J.; Timmer, R.; Boerma, E.J.; Obertop, H.; Huibregtse, K.; Gouma, D.J. Wait-and-see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile-duct stones: A randomised trial. Lancet 2002, 360, 761–765. [Google Scholar] [CrossRef] [PubMed]
- da Costa, D.W.; Bouwense, S.A.; Schepers, N.J.; Besselink, M.G.; van Santvoort, H.C.; van Brunschot, S.; Bakker, O.J.; Bollen, T.L.; Dejong, C.H.; van Goor, H.; et al. Same-admission versus interval cholecystectomy for mild gallstone pancreatitis (poncho): A multicentre randomised controlled trial. Lancet 2015, 386, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- da Costa, D.W.; Dijksman, L.M.; Bouwense, S.A.; Schepers, N.J.; Besselink, M.G.; van Santvoort, H.C.; Boerma, D.; Gooszen, H.G.; Dijkgraaf, M.G.; Dutch Pancreatitis Study, G. Cost-effectiveness of same-admission versus interval cholecystectomy after mild gallstone pancreatitis in the poncho trial. Br. J. Surg. 2016, 103, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Hallensleben, N.D.; Timmerhuis, H.C.; Hollemans, R.A.; Pocornie, S.; van Grinsven, J.; van Brunschot, S.; Bakker, O.J.; van der Sluijs, R.; Schwartz, M.P.; van Duijvendijk, P.; et al. Optimal timing of cholecystectomy after necrotising biliary pancreatitis. Gut 2022, 71, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Florentin, M.; Kostapanos, M.S.; Anagnostis, P.; Liamis, G. Recent developments in pharmacotherapy for hypertriglyceridemia: What’s the current state of the art? Expert Opin. Pharmacother. 2020, 21, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, D.; Gipe, D.A.; Pordy, R.; Ahmad, Z.; Cuchel, M.; Shah, P.K.; Chyu, K.Y.; Sasiela, W.J.; Chan, K.C.; Brisson, D.; et al. Angptl3 inhibition in homozygous familial hypercholesterolemia. N. Engl. J. Med. 2017, 377, 296–297. [Google Scholar] [CrossRef]
- Rosenson, R.S.; Gaudet, D.; Ballantyne, C.M.; Baum, S.J.; Bergeron, J.; Kershaw, E.E.; Moriarty, P.M.; Rubba, P.; Whitcomb, D.C.; Banerjee, P.; et al. Evinacumab in severe hypertriglyceridemia with or without lipoprotein lipase pathway mutations: A phase 2 randomized trial. Nat. Med. 2023, 29, 729–737. [Google Scholar] [CrossRef]
- Pelli, H.; Lappalainen-Lehto, R.; Piironen, A.; Sand, J.; Nordback, I. Risk factors for recurrent acute alcohol-associated pancreatitis: A prospective analysis. Scand. J. Gastroenterol. 2008, 43, 614–621. [Google Scholar] [CrossRef]
- Nordback, I.; Pelli, H.; Lappalainen-Lehto, R.; Jarvinen, S.; Raty, S.; Sand, J. The recurrence of acute alcohol-associated pancreatitis can be reduced: A randomized controlled trial. Gastroenterology 2009, 136, 848–855. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters and Target | Significance in GDT |
|---|---|
| HR < 120/min | An elevated heart rate can indicate an imbalance between oxygen supply and demand, guiding therapeutic interventions in GDT. Persistent tachycardia might suggest inadequate resuscitation or ongoing inflammation. |
| MAP 65–90 mmHg | A consistent MAP is crucial for ensuring adequate blood flow to vital organs. In GDT, adjustments in fluid volume and vasopressor medications might be considered to maintain or achieve a target MAP, ensuring optimal organ perfusion. |
| CVP 8–12 cmH2O | It indicates the volume and filling status of the right atrium. In GDT, CVP is used to assess the patient’s volume status and right-sided cardiac preload, guiding fluid management. |
| UO ≥ 0.5 mL/kg/h | A decrease in UO is an early and sensitive indicator of reduced kidney perfusion. Maintaining adequate urine output is crucial in GDT as it provides valuable information on general tissue perfusion. |
| ScvO2 ≥ 70% | An indicator in assessing the adequacy of tissue oxygenation. A decrease in ScvO2 can suggest that tissue oxygen demand is exceeding supply. This could be due to decreased oxygen delivery (e.g., due to low cardiac output or hemoglobulin) or increased oxygen consumption (e.g., due to increased metabolic demand). |
| BUN < 25 mg/dL | An elevated BUN has been a useful prognostic biomarker of severe AP, reflecting acute renal injury in AP caused by a decrease in circulatory volume and direct injury mechanisms, which is facilitated by autodigestion and inflammatory cytokines [6,31]. However, a declining or normalized BUN level reflects recovery of renal perfusion and adequate resuscitation. |
| Hematocrit < 44% | Hemoconcentration (high hematocrit values) is linked with high fluid sequestration and increased viscosity, which might contribute to impaired pancreatic microcirculation. Therefore, hematocrit has long been identified as a marker associated with the development of pancreatic necrosis and persistent organ failure [32,33]. Fluid rate adjustment can be guided by the biochemical targets of hematocrit of 35–44% at 12 and 24 h after AP onset. |
| Lactate | Lactate level increases when aerobic cellular respiration is impaired with a switch to anaerobic metabolism. Elevated lactate level has been considered a well-recognized biomarker of tissue hypoxia/hypoperfusion in critically ill patients. |
| Reference | Participants (N) | Aggressive Resuscitation | Non-Aggressive Resuscitation | Effect of Aggressive Resuscitation |
|---|---|---|---|---|
| Mato et al., 2009 [44] | Severe AP lesser than 72 h onset (76) | 10–15 mL/kg/h | 5–10 mL/kg/h | Harmful, more sepsis, mortality, mechanical ventilation, and ACS. |
| Mato et al., 2010 [45] | Severe AP lesser than 24 h onset (115) | Rapid hemodilution with goal hematocrit < 35% at 48 h | Slow hemodilution with goal hematocrit > 35% at 48 h | Harmful, more sepsis, and mortality |
| Wu et al., 2011 [46] | Any severity AP (40) | GDT with 20 mL/kg bolus → 1.5 or 3 mL/kg/h of LR or NS | LR or NS adjusted by physician | Similar in SIRS and CRP at 24 h |
| Buxbaum et al., 2017 [24] | Predicted mild AP (60) | 20 mL/kg bolus over 2 h → 3 mL/kg/h infusion of LR | 10 mL/kg bolus over 2 h → 1.5 mL/kg/h infusion of LR | Beneficial, more clinical improvement, and less persistent SIRS and hemoconcentration |
| At timepoint (12, 24, 36 h) If hematocrit, BUN, or creatinine increased, 20 mL/kg bolus → 3 mL/kg/h infusion If labs were decreased and pain relived, 1.5 mL/kg/h infusion and start diet | ||||
| Cuéllar-Monterrubio et al., 2020 [47] | Any severity AP, more than 24 h onset (88) | 20 mL/kg bolus → 3 mL/kg/h (first 24 h) → 30 mL/h (next 24 h) of HS | 20 mL/kg bolus (only if hypovolemia) → 1.5 mL/kg/h (first 24 h) → 30 mL/h (next 24 h) of HS | No benefit, no difference in persistent SIRS, pancreatic necrosis, respiratory complications, AKI and LOS |
| De-Madaria et al., 2022 [23] | Mild AP, lesser than 24 h onset (249) | 20 mL/kg bolus → 3 mL/kg/h infusion of LR | 10 mL/kg bolus (only if hypovolemia) → 1.5 mL/kg/h infusion of LR | Harmful, more fluid overload |
| At timepoint (3,12, 24, 48, 72 h) If hypovolemia → 20 mL/kg bolus → 3 mL/kg/h If normovolemia → 1.5 mL/kg/h If fluid overload → decrease or stop | At timepoint (3,12, 24, 48, 72 h) If hypovolemia → 10 mL/kg bolus → 1.5 mL/kg/h If normovolemia → 1.5 mL/kg/h If fluid overload → decrease or stop | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.; Lee, S.-H. Recent Treatment Strategies for Acute Pancreatitis. J. Clin. Med. 2024, 13, 978. https://doi.org/10.3390/jcm13040978
Song Y, Lee S-H. Recent Treatment Strategies for Acute Pancreatitis. Journal of Clinical Medicine. 2024; 13(4):978. https://doi.org/10.3390/jcm13040978
Chicago/Turabian StyleSong, Yongcook, and Sang-Hoon Lee. 2024. "Recent Treatment Strategies for Acute Pancreatitis" Journal of Clinical Medicine 13, no. 4: 978. https://doi.org/10.3390/jcm13040978
APA StyleSong, Y., & Lee, S.-H. (2024). Recent Treatment Strategies for Acute Pancreatitis. Journal of Clinical Medicine, 13(4), 978. https://doi.org/10.3390/jcm13040978