
Neurodevelopmental Outcome after Culture-Proven or So-Called Culture-Negative Sepsis in Preterm Infants
 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
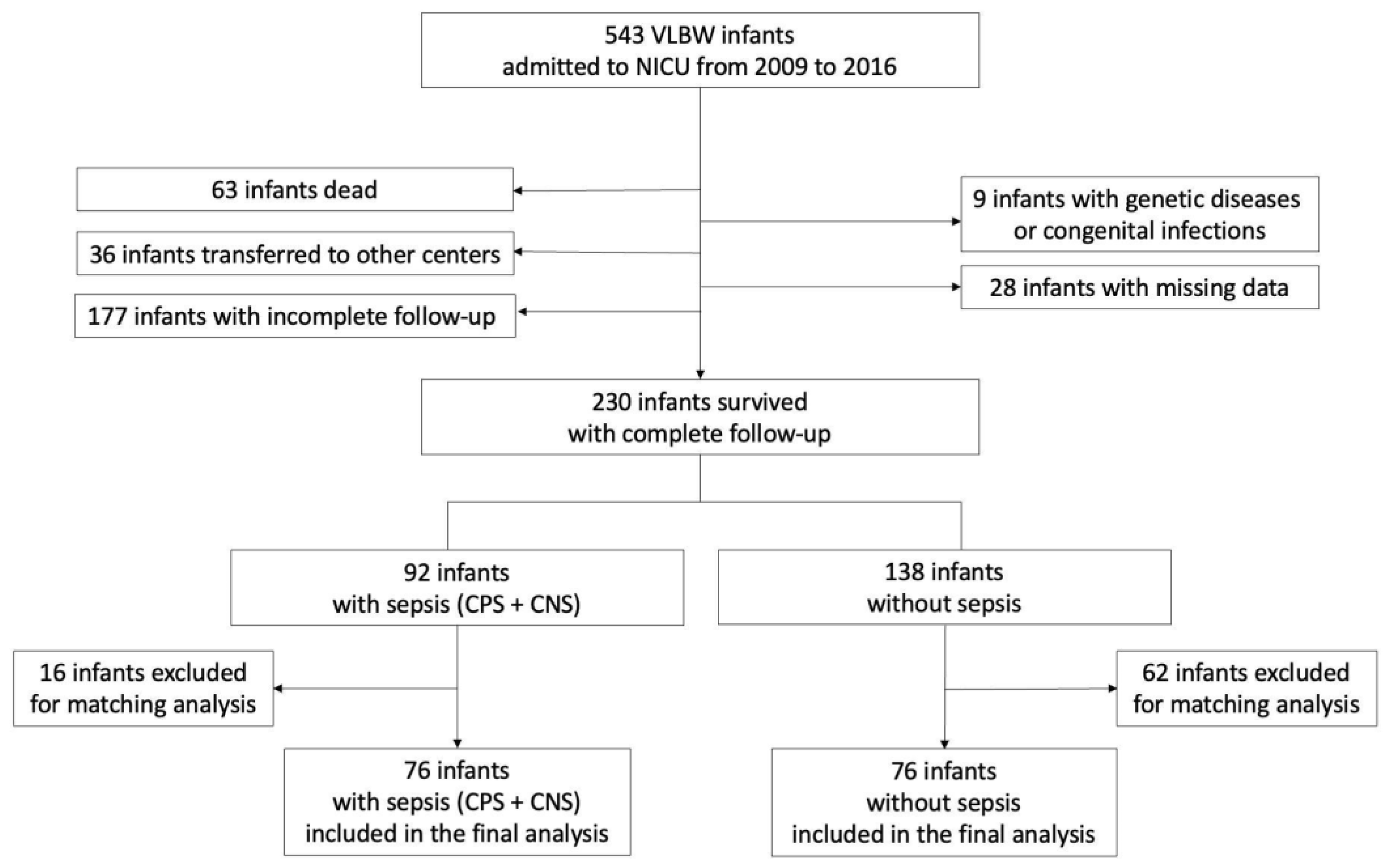
2.1. Study Design
2.2. Definitions
2.3. Data Collection
2.4. Neurodevelopmental Assessment at 24 Months of Age
2.5. Brain MRI Evaluations
- Germinal matrix hemorrhage–intraventricular hemorrhage: The germinal matrix is a structure that is normally visible on imaging and undergoes involution as the fetus ages, leaving only remnants in the caudothalamic notch and roof of the temporal horns after 32 weeks of gestation. An irregular contour in a subependymal area with a low T2 signal or accompanying intraventricular hemorrhage is categorized as germinal matrix hemorrhage–intraventricular hemorrhage [30].
- Hemorrhagic parenchymal infarction: When fully developed, hemorrhagic parenchymal infarction is characterized by a focal bulging or outpouching of the ventricular contour, usually unilateral. This is often accompanied by a low T2 signal component, indicating a previous hemorrhage [30].
- Periventricular leukomalacia: Periventricular leukomalacia typically manifests as multiple bilateral periventricular cysts in a symmetric distribution, initially appearing to be separate from the ventricle. Solitary or unilateral cysts are more likely to be venous infarcts or conatal cysts. Criteria to diagnose periventricular leukomalacia are as follows: residual bilateral periventricular cysts, dilated/angulated posterior aspects of the lateral ventricles, and associated white matter volume loss [30].
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. All Sepsis (CPS + CNS) vs. No Sepsis
3.2. Culture-Proven Sepsis vs. No Sepsis
3.3. Culture-Negative Sepsis vs. No Sepsis
3.4. Sepsis and Severe Functional Disability: Logistic Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Serenius, F.; Källén, K.; Blennow, M.; Ewald, U.; Fellman, V.; Holmström, G.; Lindberg, E.; Lundqvist, P.; Maršál, K.; Norman, M.; et al. Neurodevelopmental outcome in extremely preterm infants at 2.5 years after active perinatal care in Sweden. JAMA 2013, 309, 1810–1820. [Google Scholar] [CrossRef]
- Younge, N.; Goldstein, R.F.; Bann, C.M.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Survival and neurodevelopmental outcomes among Periviable infants. N. Engl. J. Med. 2017, 376, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Marlow, N.; Wolke, D.; Bracewell, M.A.; Samara, M. EPICure Study Group: Neurologic and developmental disability at six years of age after extremely preterm birth. N. Engl. J. Med. 2005, 352, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Lugli, L.; Bedetti, L.; Guidotti, I.; Pugliese, M.; Picciolini, O.; Roversi, M.F.; Muttini, E.D.; Lucaccioni, L.; Bertoncelli, N.; Ancora, G.; et al. Neuroprem 2: An Italian Study of Neurodevelopmental Outcomes of Very Low Birth Weight Infants. Front. Pediatr. 2021, 9, 697100. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Sánchez, P.J.; Faix, R.G.; Poindexter, B.B.; Van Meurs, K.P.; Bizzarro, M.J.; Goldberg, R.N.; Frantz, I.D., III.; Hale, E.C.; et al. Early onset neonatal sepsis: The burden of group B Streptococcal and E. coli disease continues. Pediatrics 2011, 127, 817–826. [Google Scholar] [CrossRef]
- Stoll, B.J.; Puopolo, K.M.; Hansen, N.I.; Sánchez, P.J.; Bell, E.F.; Carlo, W.A.; Cotten, C.M.; D’angio, C.T.; Kazzi, S.N.J.; Poindexter, B.B.; et al. Early-Onset Neonatal Sepsis 2015 to 2017, the Rise of Escherichia coli, and the Need for Novel Prevention Strategies. JAMA Pediatr. 2020, 174, e200593. [Google Scholar] [CrossRef] [PubMed]
- Berardi, A.; Sforza, F.; Baroni, L.; Spada, C.; Ambretti, S.; Biasucci, G.; Bolognesi, S.; Capretti, M.; Carretto, E.; Ciccia, M.; et al. Epidemiology and complications of late-onset sepsis: An Italian area-based study. PLoS ONE 2019, 14, e0225407. [Google Scholar] [CrossRef]
- Strunk, T.; Inder, T.; Wang, X.; Burgner, D.; Mallard, C.; Levy, O. Infection-induced inflammation and cerebral injury in preterm infants. Lancet Infect. Dis. 2014, 14, 751–762. [Google Scholar] [CrossRef]
- Thomas, R.; Bijlsma, M.W.; Gonçalves, B.P.; Nakwa, F.L.; Velaphi, S.; Heath, P.T. Long-term impact of serious neonatal bacterial infections on neurodevelopment. Clin. Microbiol. Infect. 2024, 30, 28–37. [Google Scholar] [CrossRef]
- Graham, E.M.; Holcroft, C.J.; Rai, K.K.; Donohue, P.K.; Allen, M.C. Neonatal cerebral white matter injury in preterm infants is associated with culture positive infections and only rarely with metabolic acidosis. Am. J. Obstet. Gynecol. 2004, 191, 1305–1310. [Google Scholar] [CrossRef]
- Inder, T.E.; Volpe, J.J.; Anderson, P.J. Defining the Neurologic Consequences of Preterm Birth. N. Engl. J. Med. 2023, 389, 441–453. [Google Scholar] [CrossRef]
- Mitha, A.; Foix-L’hélias, L.; Arnaud, C.; Marret, S.; Vieux, R.; Aujard, Y.; Thiriez, G.; Larroque, B.; Cambonie, G.; Burguet, A.; et al. Neonatal infection and 5-year neurodevelopmental outcome of very preterm infants. Pediatrics 2013, 132, e372–e380. [Google Scholar] [CrossRef]
- Schlapbach, L.J.; Aebischer, M.; Adams, M.; Natalucci, G.; Bonhoeffer, J.; Latzin, P.; Nelle, M.; Bucher, H.U.; Latal, B.; Swiss Neonatal Network and Follow-Up Group. Impact of sepsis on neurodevelopmental outcome in a Swiss National Cohort of extremely premature infants. Pediatrics 2011, 128, e348–e357. [Google Scholar] [CrossRef]
- Alshaikh, B.; Yusuf, K.; Sauve, R. Neurodevelopmental outcomes of very low birth weight infants with neonatal sepsis: Systematic review and meta-analysis. J. Perinatol. 2013, 33, 558–564. [Google Scholar] [CrossRef]
- Cantey, J.B.; Prusakov, P. A Proposed Framework for the Clinical Management of Neonatal “Culture-Negative” Sepsis. J. Pediatr. 2022, 244, 203–211. [Google Scholar] [CrossRef] [PubMed]
- EFCNI–European Standards of Care for Newborn Health. Follow-up and Continuing Care. Available online: htps://newborn-health-standards.org/standards/standards-english/follow-up-continuing-care (accessed on 15 March 2023).
- Spittle, A.; Orton, J.; Anderson, P.J.; Boyd, R.; Doyle, L.W. Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants. Cochrane Database Syst. Rev. 2015, 2015, CD005495. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Haque, K.N. Definitions of bloodstream infection in the newborn. Pediatr. Crit. Care Med. 2005, 6 (Suppl. 3), S45–S49. [Google Scholar] [CrossRef] [PubMed]
- Leistner, R.; Piening, B.; Gastmeier, P.; Geffers, C.; Schwab, F. Nosocomial Infections in Very Low Birthweight Infants in Germany: Current Data from the National Surveillance System NEO-KISS. Klin. Padiatr. 2013, 225, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Baczynski, M.; Kharrat, A.; Ye, X.Y.; Weisz, D.; Jain, A. Blood pressure, organ dysfunction, and mortality in preterm neonates with late-onset sepsis. Pediatr. Res. 2022, 92, 498–504. [Google Scholar] [CrossRef]
- Vermont-Oxford Network Database. Manual of Operations, Data Definitions; release 22.0; Vermont Oxford Network: Burlington, VT, USA, 2017. [Google Scholar]
- Stoll, B.J.; Hansen, N.I.; Adams-Chapman, I.; Fanaroff, A.A.; Hintz, S.R.; Vohr, B.; Higgins, R.D.; National Institute of Child Health and Human Development Neonatal Research Network. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 2004, 292, 2357–2365. [Google Scholar] [CrossRef]
- Ohlsson, A.; Walia, R.; Shah, S.S. Ibuprofen for the treatment of patent ductus arteriosus in preterm or low birth weight (or both) infants. Cochrane Database Syst. Rev. 2018, 9, CD003481. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Chiang, M.F.; Quinn, G.E.; Fielder, A.R.; Ostmo, S.R.; Chan, R.P.; Berrocal, A.; Binenbaum, G.; Blair, M.; Campbell, J.P.; Capone, A.; et al. International Classification of Retinopathy of Prematurity, Third Edition. Ophthalmology 2021, 128, e51–e68. [Google Scholar] [CrossRef] [PubMed]
- Amiel-Tison, C.; Grenier, L. La Valutazione Neurologica del Neonato e del Lattante; Masson: Padova, Italy, 1981. [Google Scholar]
- Griffiths, R. Griffiths Mental Developmental Scale-Revised: Birth to 2 Years (GMDS-R); Hogrefe: Firenze, Italy, 1996. [Google Scholar]
- Arulkumaran, S.; Tusor, N.; Chew, A.; Falconer, S.; Kennea, N.; Nongena, P.; Hajnal, J.V.; Counsell, S.J.; Rutherford, M.A.; Edwards, A.D. MRI Findings at Term-Corrected Age and Neurodevelopmental Outcomes in a Large Cohort of Very Preterm Infants. Am. J. Neuroradiol. 2020, 41, 1509–1516. [Google Scholar] [CrossRef]
- Nizet, V.; Klein, J.O. Bacterial Sepsis and Meningitis. In Infectious Diseases of the Fetus and Newborn Infant; Elsevier: Amsterdam, The Netherlands, 2010; pp. 222–275. [Google Scholar]
- Miselli, F.; Crestani, S.; Maugeri, M.; Passini, E.; Spaggiari, V.; Deonette, E.; Ćosić, B.; Rossi, K.; Roversi, M.F.; Bedetti, L.; et al. Late-Onset Sepsis Mortality among Preterm Infants: Beyond Time to First Antibiotics. Microorganisms 2023, 11, 396. [Google Scholar] [CrossRef] [PubMed]
- Berardi, A.; Lugli, L.; Rossi, C.; China, M.C.; Vellani, G.; Contiero, R.; Calanca, F.; Camerlo, F.; Casula, F.; Di Carlo, C.; et al. Neonatal bacterial meningitis. Minerva Pediatr. 2010, 62 (3 Suppl. 1), 51–54. [Google Scholar]
- Rand, K.M.; Austin, N.C.; Inder, T.E.; Bora, S.; Woodward, L.J. Neonatal Infection and Later Neurodevelopmental Risk in the Very Preterm Infant. J. Pediatr. 2016, 170, 97–104. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.; Puopolo, K.M.; Hansen, N.I.; Lorch, S.A.; DeMauro, S.B.; Greenberg, R.G.; Cotten, C.M.; Sanchez, P.J.; Bell, E.F.; Eichenwald, E.C.; et al. NICHD Neonatal Research Network. Neurodevelopmental outcomes following neonatal late-onset sepsis and blood culture-negative conditions. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 467–473. [Google Scholar] [CrossRef]
- Cantey, J.B.; Baird, S.D. Ending the Culture of Culture-Negative Sepsis in the Neonatal ICU. Pediatrics 2017, 140, e20170044. [Google Scholar] [CrossRef]
- Zonnenberg, I.A.; van Dijk-Lokkart, E.M.; van den Dungen, F.A.M.; Vermeulen, R.J.; van Weissenbruch, M.M. Neurodevelopmental outcome at 2 years of age in preterm infants with late-onset sepsis. Eur. J. Pediatr. 2019, 178, 673–680. [Google Scholar] [CrossRef]
- Davis, J.W.; Odd, D.; Jary, S.; Luyt, K. The impact of a sepsis quality improvement project on neurodisability rates in very low birthweight infants. Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, F562–F564. [Google Scholar] [CrossRef]
- Bierlaire, S.; Danhaive, O.; Carkeek, K.; Piersigilli, F. How to minimize central line-associated bloodstream infections in a neonatal intensive care unit: A quality improvement intervention based on a retrospective analysis and the adoption of an evidence-based bundle. Eur. J. Pediatr. 2021, 180, 449–460. [Google Scholar] [CrossRef]
- Mobley, R.E.; Bizzarro, M.J. Central line-associated bloodstream infections in the NICU: Successes and controversies in the quest for zero. Semin. Perinatol. 2017, 41, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.; Simms, A.; Wood, M.; Taylor, K.; Ferrari, S.; Rhein, M.; Margallo, D.; Bain, L.C.; Valencia, A.K.; Bargmann-Losche, J.; et al. Reduction of Central Line-associated Bloodstream Infection Through Focus on the Mesosystem: Standardization, Data, and Accountability. Pediatr. Qual. Saf. 2020, 5, e272. [Google Scholar] [CrossRef] [PubMed]
- Schulman, J.; Benitz, W.E.; Profit, J.; Lee, H.C.; Dueñas, G.; Bennett, M.V.; Jocson, M.A.L.; Schutzengel, R.; Gould, J.B. Newborn Antibiotic Exposures and Association with Proven Bloodstream Infection. Pediatrics 2019, 144, e20191105. [Google Scholar] [CrossRef]
- Kuppala, V.S.; Meinzen-Derr, J.; Morrow, A.L.; Schibler, K.R. Prolonged initial empirical antibiotic treatment is associated with adverse outcomes in premature infants. J. Pediatr. 2011, 159, 720–725. [Google Scholar] [CrossRef] [PubMed]
- Ting, J.Y.; Roberts, A.; Sherlock, R.; Ojah, C.; Cieslak, Z.; Dunn, M.; Barrington, K.; Yoon, E.W.; Shah, P.S.; Canadian Neonatal Network Investigators. Duration of Initial Empirical Antibiotic Therapy and Outcomes in Very Low Birth Weight Infants. Pediatrics 2019, 143, e20182286. [Google Scholar] [CrossRef]
- Berardi, A.; Zinani, I.; Rossi, C.; Spaggiari, E.; D’Amico, V.; Toni, G.; Bedetti, L.; Lucaccioni, L.; Iughetti, L.; Lugli, L. Antibiotic Use in Very Low Birth Weight Neonates After an Antimicrobial Stewardship Program. Antibiotics 2021, 10, 411. [Google Scholar] [CrossRef]
- Yu, W.; Zhang, L.; Li, S.; Yan, W.; Bai, R.; Yang, Z.; Shi, J.; Yuan, J.; Yang, C.; Cai, W.; et al. Reduction of Infection in Neonatal Intensive Care Units Using the Evidence-based Practice for Improving Quality (REIN-EPIQ) Study Group. Early Antibiotic Use and Neonatal Outcomes Among Preterm Infants Without Infections. Pediatrics 2023, 151, e2022059427. [Google Scholar] [CrossRef]
- Weiss, S.L.M.; Peters, M.J.M.; Alhazzani, W.M.; Agus, M.S.D.M.; Flori, H.R.M.; Inwald, D.P.M.; Nadel, S.M.; Schlapbach, L.J.F.; Tasker, R.C.M.B.; Argent, A.C.M.B.; et al. Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children. Pediatr. Crit. Care Med. 2020, 21, e52–e106. [Google Scholar] [CrossRef] [PubMed]
- Sepsis: Recognition, diagnosis and early management: © NICE (2017). BJU Int. 2018, 121, 497–514. [CrossRef]
- Spaggiari, V.; Passini, E.; Crestani, S.; Roversi, M.F.; Bedetti, L.; Rossi, K.; Lucaccioni, L.; Baraldi, C.; Muttini, E.D.C.; Lugli, L.; et al. Neonatal septic shock, a focus on first line interventions. Acta Biomed. 2022, 93, e2022141. [Google Scholar] [CrossRef]
- Petrou, S.; Yiu, H.H.; Kwon, J. Economic consequences of preterm birth: A systematic review of the recent literature (2009–2017). Arch. Dis. Child. 2019, 104, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, M.C.; Gugiatti, A.; Fattore, G.; Gerzeli, S.; Barbieri, D.; Zanini, R.; Neonatal Adequate Care for Quality of Life (NEO-ACQUA) Study Group. Cost of care and social consequences of very low birth weight infants without premature- related morbidities in Italy. Ital. J. Pediatr. 2015, 41, 59. [Google Scholar] [CrossRef]
- Newnham, J.P.; Schilling, C.; Petrou, S.; Morris, J.M.; Wallace, E.M.; Brown, K.; Edwards, L.; Skubisz, M.M.; White, S.W.; Rynne, B.; et al. The health and educational costs of preterm birth to 18 years of age in Australia. Aust. N. Z. J. Obstet. Gynaecol. 2022, 62, 55–61. [Google Scholar] [CrossRef]
- de Abreu, M.F.C.W.; Ogata, J.F.M.; Fonseca, M.C.M.; Sansone, D.; Guinsburg, R. The financial impact of neonatal sepsis on the Brazilian Unified Health System. Clinics 2023, 78, 100277. [Google Scholar] [CrossRef]


{kind=link}
| Variables | All Sepsis (CPS + CNS) | p † | CPS | p § | CNS | p ¥ | Infants without Sepsis |
|---|---|---|---|---|---|---|---|
| n = 76 | n = 33 | n = 43 | n = 76 | ||||
| Sex, male | 38 (50) | 0.871 | 17 (51.2) | 0.985 | 21 (48.8) | 0.795 | 39 (51.3) |
| Gestational age | 27.7 (26.8; 29.6) | 0.139 | 27.1 (26.3; 28.6) | 0.016 | 28 (27; 29.9) | 0.842 | 29 (26.6; 30) |
| Birth weight | 959 (805; 1200) | 0.575 | 960 (773; 1210) | 0.557 | 970 (829; 1146) | 0.727 | 955 (820; 1146) |
| SGA | 11 (14.5) | 0.656 | 4 (12.1) | 0.510 | 7 (16.3) | 0.908 | 13 (17.1) |
| Twinning | 28 (36.9) | 0.610 | 15 (45.5) | 0.211 | 13 (30.2) | 0.765 | 25 (32.3) |
| Cesarean section | 55 (72.4) | 0.047 | 21 (63.6) | 0.010 | 34 (79.1) | 0.366 | 65 (83.5) |
| Prenatal steroids ¶ | 10 (14.1) | 0.758 | 7 (23.3) | 0.381 | 3 (7.3) | 0.189 | 11 (15.9) |
| 5th minute Apgar score | 8 (7–9) | 0.105 | 8 (7–8) | 0.044 | 8 (7–9) | 0.454 | 8 (7–9) |
| Chorioamnionitis | 23 (31.6) | 0.594 | 11 (33.3) | 0.548 | 13 (30.2) | 0.763 | 21 (27.6) |
| Variables | All Sepsis (CPS + CNS) | p † | CPS | p § | CNS | p ¥ | Infants without Sepsis |
|---|---|---|---|---|---|---|---|
| n = 76 | n = 33 | n = 43 | n = 76 | ||||
| Days of central line | 29 (14; 39) | <0.001 | 33 (22–44) | <0.001 | 26 (12–36) | 0.001 | 15 (6; 22) |
| Surfactant | 59 (73.6) | 0.105 | 26 (78.8) | 0.175 | 33 (76.7) | 0.211 | 50 (65.8) |
| Post-natal steroids | 15 (19.7) | 0.008 | 8 (24.2) | 0.004 | 7 (16.3) | 0.049 | 4 (5.3) |
| MV | 61 (80.3) | <0.001 | 30 (90.9) | <0.001 | 31 (72.1) | 0.001 | 36 (47.4) |
| MV, days | 5 (1; 15) | <0.001 | 7 (2–10) | <0.001 | 4 (0–17) | <0.001 | 0 (0–3) |
| BPD | <0.001 | <0.001 | 0.003 | ||||
| 22 (29.0) | 13 (39.4) | 9 (20.9) | 22 (29.0) | |||
| 13 (17.1) | 5 (15.2) | 8 (18.6) | 6 (7.9) | |||
| 15 (19.8) | 8 (24.2) | 7 (16.3) | 1 (1.3) | |||
| PDA | 0.007 | 0.021 | 0.031 | ||||
| 34 (44.7) | 14 (42.4) | 20 (46.5) | 20 (26.3) | |||
| 5 (6.6) | 3 (9.1) | 2 (4.7) | 1 (1.3) | |||
| NEC ‖ | 4 (5.3) | 0.043 | 1 (3) | 0.127 | 3 (7.0) | 0.020 | 0 |
| ROP ≥ grade 3 | 5 (6.7) | 0.246 | 4 (12.1) | 0.046 | 1 (2.3) | 0.919 | 2 (2.6) |
| IVH | 18 (24.7) | 0.085 | 9 (29.0) | 0.059 | 9 (21.4) | 0.259 | 9 (13.2) |
| HPI | 6 (8.2) | 0.065 | 3 (9.7) | 0.054 | 3 (7.1) | 0.123 | 1 (1.5) |
| PVL | 11 (15.1) | 0.034 | 4 (12.9) | 0.126 | 7 (16.7) | 0.030 | 3 (4.4) |
| Hospital stay, days | 75 (55; 93) | <0.001 | 88 (58–100) | <0.001 | 66 (55–84) | 0.013 | 60 (45; 72) |
| PCE at discharge | 38.6 (36.9; 41) | <0.001 | 39 (37–41.6) | 0.002 | 38.4 (36.8–40) | 0.005 | 37.2 (35.8; 38.1) |
| Variables | All Sepsis (CPS + CNS) | p † | CPS | p § | CNS | p ¥ | Infants without Sepsis |
|---|---|---|---|---|---|---|---|
| n = 76 | n = 33 | n = 33 | n = 76 | ||||
| Neurodevelopmental outcome | 0.008 | 0.004 | 0.063 | ||||
| 47 (61.8) | 18 (54.6) | 29 (67.5) | 59 (77.6) | |||
| 10 (13.2) | 5 (15.2) | 5 (11.6) | 12 (15.8) | |||
| 19 (25.0) | 10 (30.3) ‡ | 9 (20.9) ¶ | 5 (6.6) * | |||
| Motor outcome | 0.003 | 0.007 | 0.137 | ||||
| 50 (65.8) | 18 (55.6) | 32 (74.4) | 62 (81.6) | |||
| 14 (18.4) | 9 (27.3) | 5 (11.6) | 11 (14.5) | |||
| 12 (15.8) | 6 (18.2) | 6 (14.0) | 3 (3.9) | |||
| GMDS-R ‖ | |||||||
| A | 98 (98–107) | 0.322 | 98 (98–107) | 0.387 | 98 (98–107) | 0.458 | 98 (98–107) |
| B | 106 (99–115) | 0.038 | 106 (92–106) | 0.006 | 109 (99–119) | 0.416 | 112 (100–119) |
| C | 101 (88–105) | 0.621 | 98 (84–102) | 0.179 | 102 (91–107) | 0.719 | 102 (88–105) |
| D | 107(102–112) | 0.762 | 107 (102–112) | 0.259 | 107 (102–118) | 0.644 | 107 (102–118) |
| E | 101 (99–106) | 0.286 | 100 (99–106) | 0.497 | 102 (100–106) | 0.319 | 106 (100–106) |
| GQ | 103 (96–109) | 0.264 | 100 (95–106) | 0.033 | 105 (97–111) | 0.931 | 105 (98–111) |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | CI | p | OR | CI | p | |
| All sepsis (CPS + CNS) | 4.73 | 1.6–13.4 | 0.004 | 3.68 | 1.2–11.1 | 0.021 |
| BPD | 1.40 | 0.9–2.1 | 0.102 | |||
| IVH | 5.8 | 2.2–15.4 | <0.001 | 4.7 | 1.7–13.1 | 0.002 |
| Gestational age | 0.74 | 0.5–0.9 | 0.014 | 0.83 | 0.6–1.0 | 0.159 |
| Birth weight | 0.99 | 0.9–1.0 | 0.071 | |||
| Mechanical ventilation | 2.43 | 0.8–6.9 | 0.096 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bedetti, L.; Corso, L.; Miselli, F.; Guidotti, I.; Toffoli, C.; Miglio, R.; Roversi, M.F.; Muttini, E.d.C.; Pugliese, M.; Bertoncelli, N.; et al. Neurodevelopmental Outcome after Culture-Proven or So-Called Culture-Negative Sepsis in Preterm Infants. J. Clin. Med. 2024, 13, 1140. https://doi.org/10.3390/jcm13041140
Bedetti L, Corso L, Miselli F, Guidotti I, Toffoli C, Miglio R, Roversi MF, Muttini EdC, Pugliese M, Bertoncelli N, et al. Neurodevelopmental Outcome after Culture-Proven or So-Called Culture-Negative Sepsis in Preterm Infants. Journal of Clinical Medicine. 2024; 13(4):1140. https://doi.org/10.3390/jcm13041140
Chicago/Turabian StyleBedetti, Luca, Lucia Corso, Francesca Miselli, Isotta Guidotti, Carlotta Toffoli, Rossella Miglio, Maria Federica Roversi, Elisa della Casa Muttini, Marisa Pugliese, Natascia Bertoncelli, and et al. 2024. "Neurodevelopmental Outcome after Culture-Proven or So-Called Culture-Negative Sepsis in Preterm Infants" Journal of Clinical Medicine 13, no. 4: 1140. https://doi.org/10.3390/jcm13041140
APA StyleBedetti, L., Corso, L., Miselli, F., Guidotti, I., Toffoli, C., Miglio, R., Roversi, M. F., Muttini, E. d. C., Pugliese, M., Bertoncelli, N., Zini, T., Mazzotti, S., Lugli, L., Lucaccioni, L., & Berardi, A. (2024). Neurodevelopmental Outcome after Culture-Proven or So-Called Culture-Negative Sepsis in Preterm Infants. Journal of Clinical Medicine, 13(4), 1140. https://doi.org/10.3390/jcm13041140