
Morbidity among Adolescent Hypnotic Drug Users in Norway: An Observational Population-Based Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.1.1. The Norwegian Prescription Database (NorPD)—Information about Prescribed Hypnotic Drugs
2.1.2. The Norwegian Patient Registry (NPR)—Information on Diagnosis from Secondary Health Care
2.1.3. Norway Control and Payment of Health Reimbursements (KUHR) Database—Information on Diagnosis from Primary Care
2.2. Study Population
2.3. Analytical Approach
2.3.1. Annual Prevalence of Hypnotic Drug Use
2.3.2. Annual Prevalence of Sleep Disorder Diagnosis in Primary and Secondary Health Care
2.3.3. Incident Hypnotic Drug Users
- (a)
- Incidence rate
- (b)
- Type of the first hypnotic drug use and amount dispensed to incident hypnotic drug users
- (c)
- Contact with secondary health care
- (d)
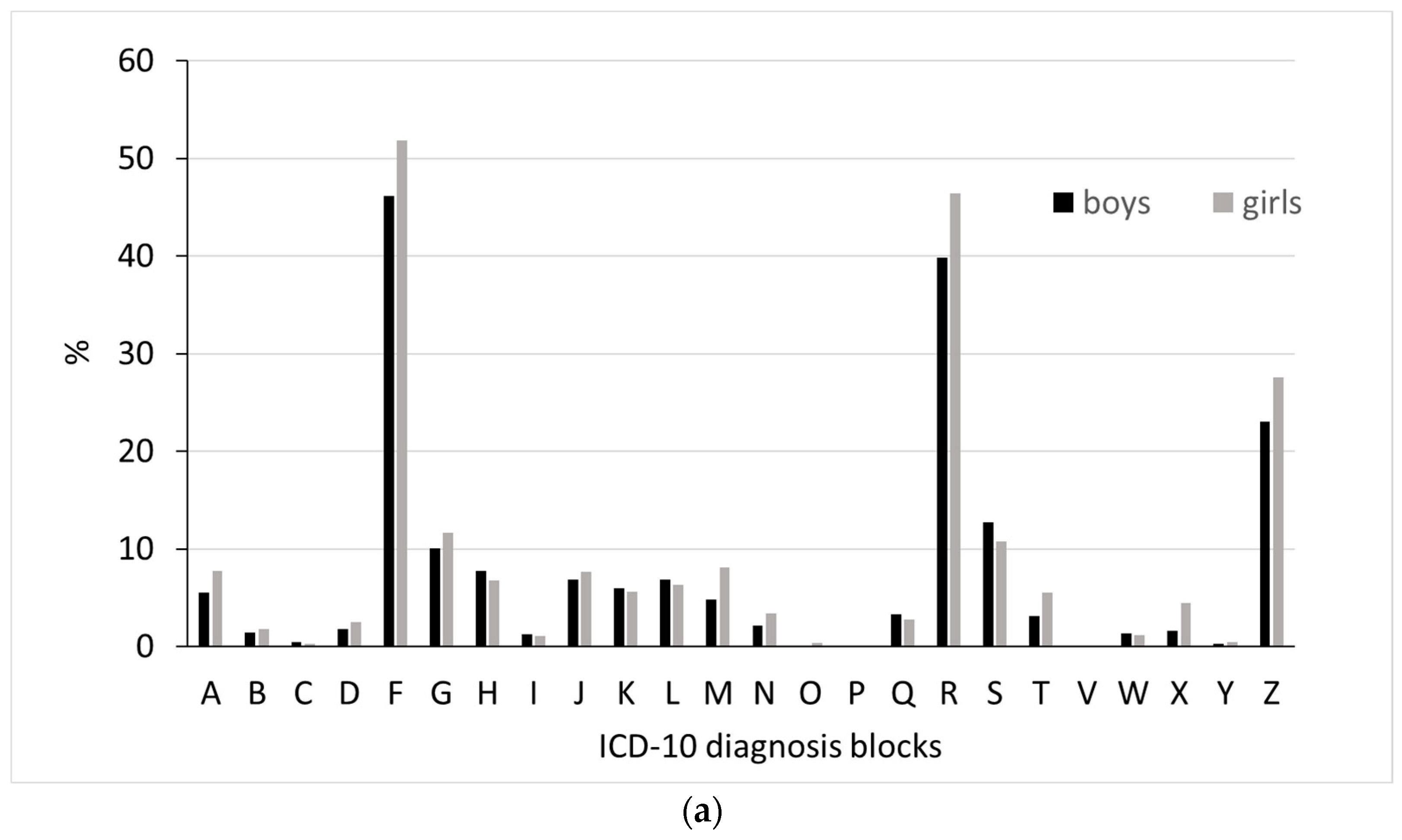
- Diagnoses from secondary health care
- (e)
- Diagnoses from secondary health care during childhood
2.4. Ethical Considerations
3. Results
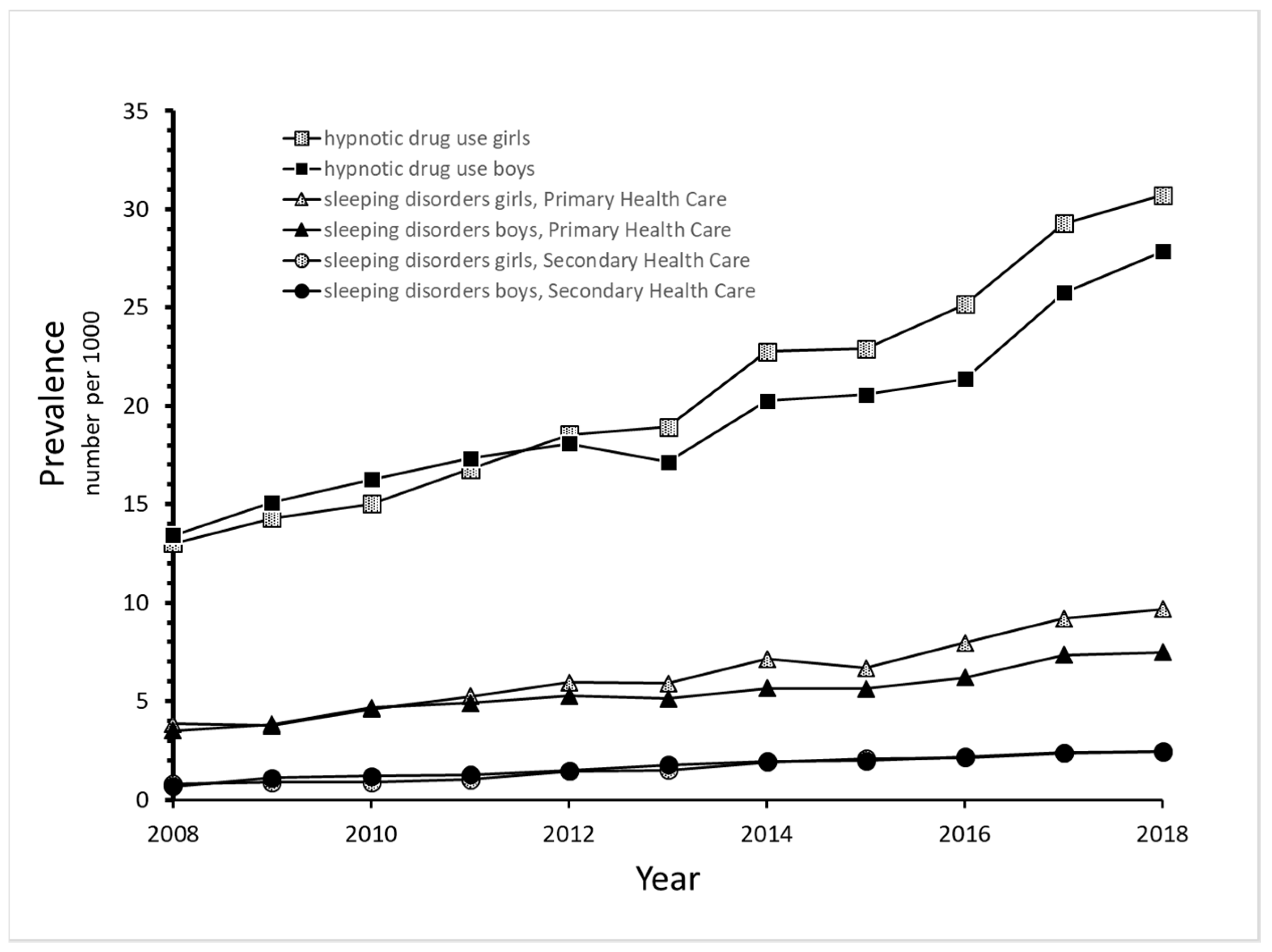
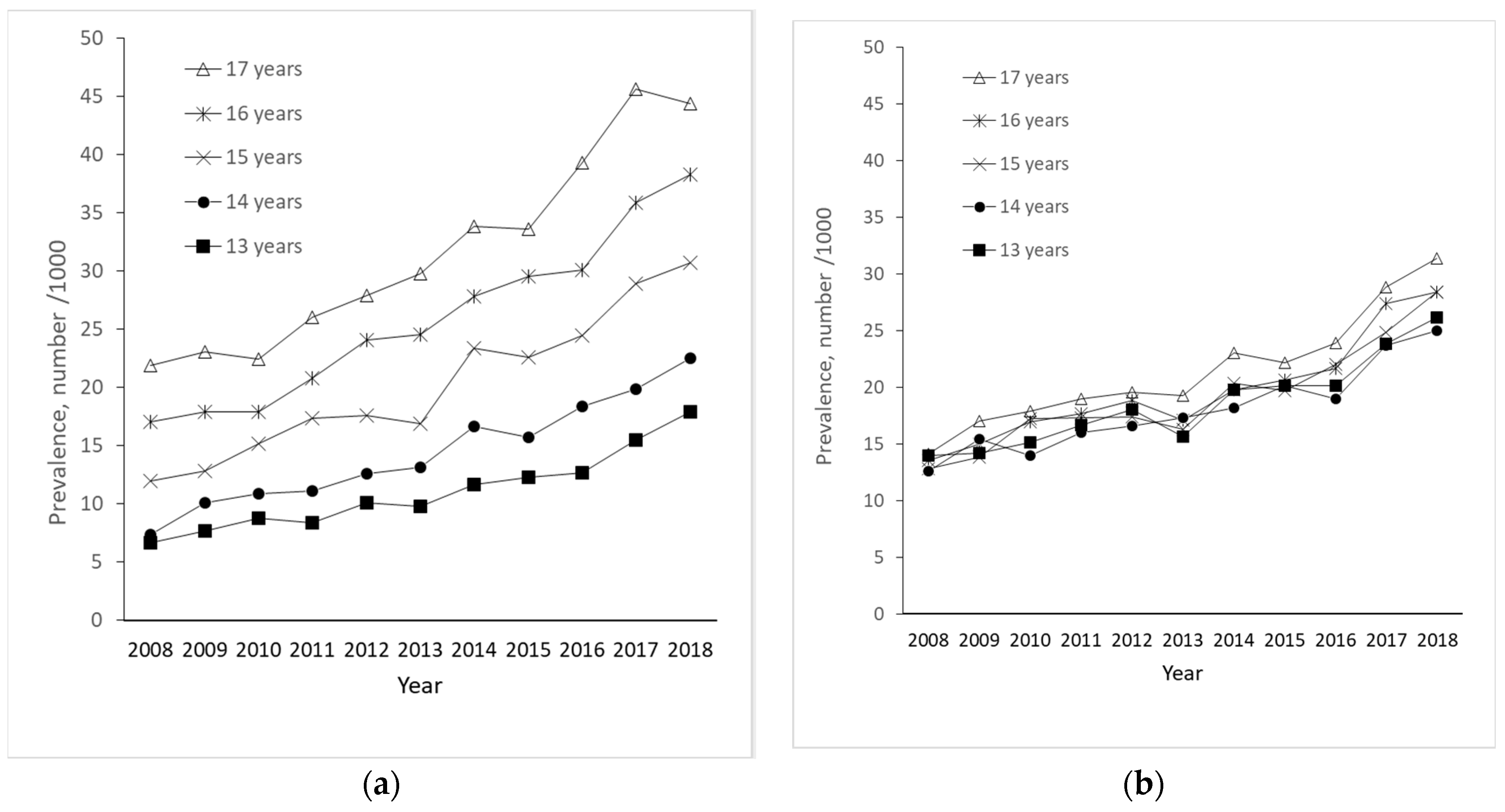
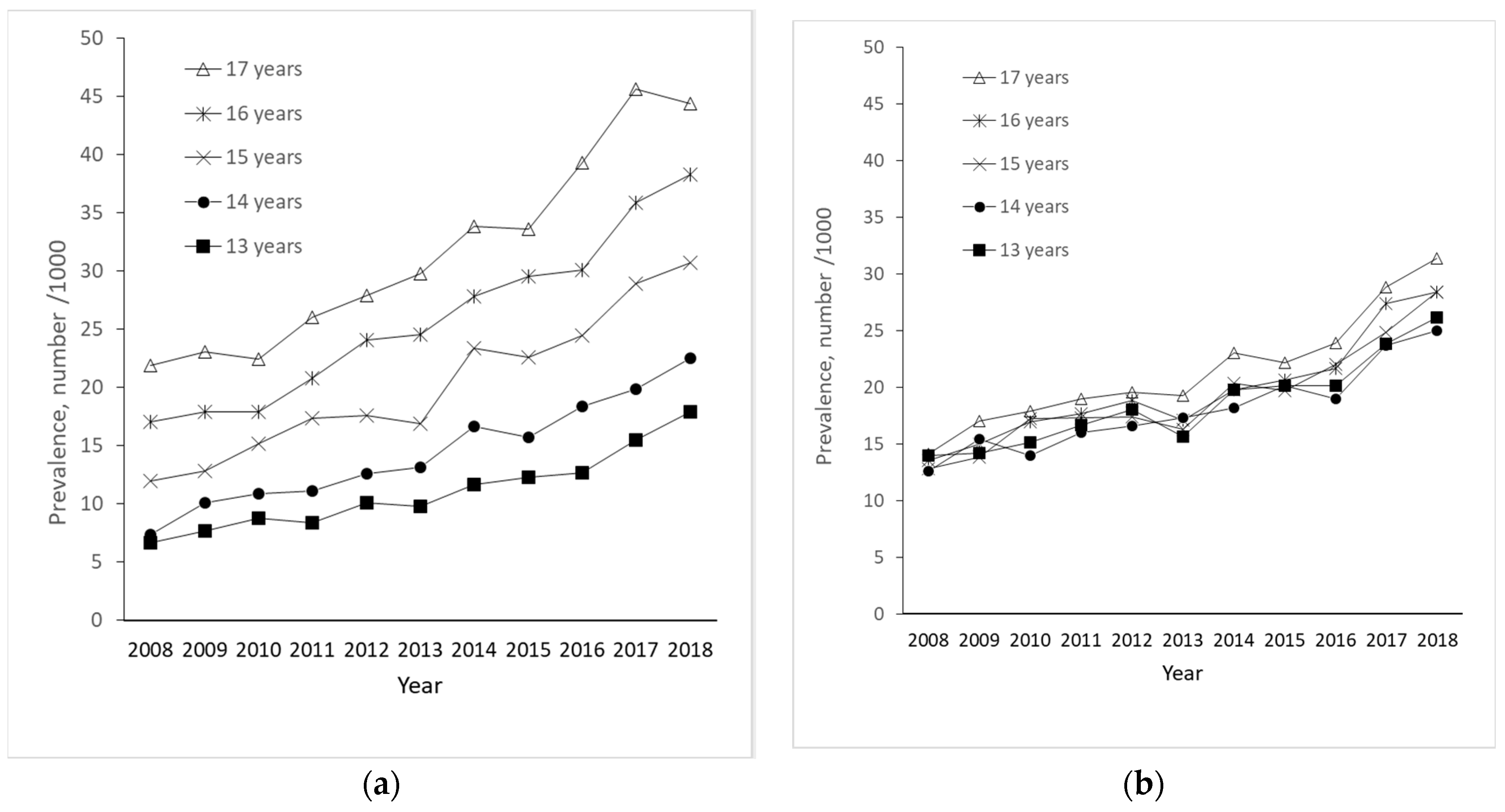
3.1. Annual Prevalence of Hypnotic Drug Use
3.2. Annual Prevalence of Sleep Disorder Diagnosis in Primary and Secondary Health Care
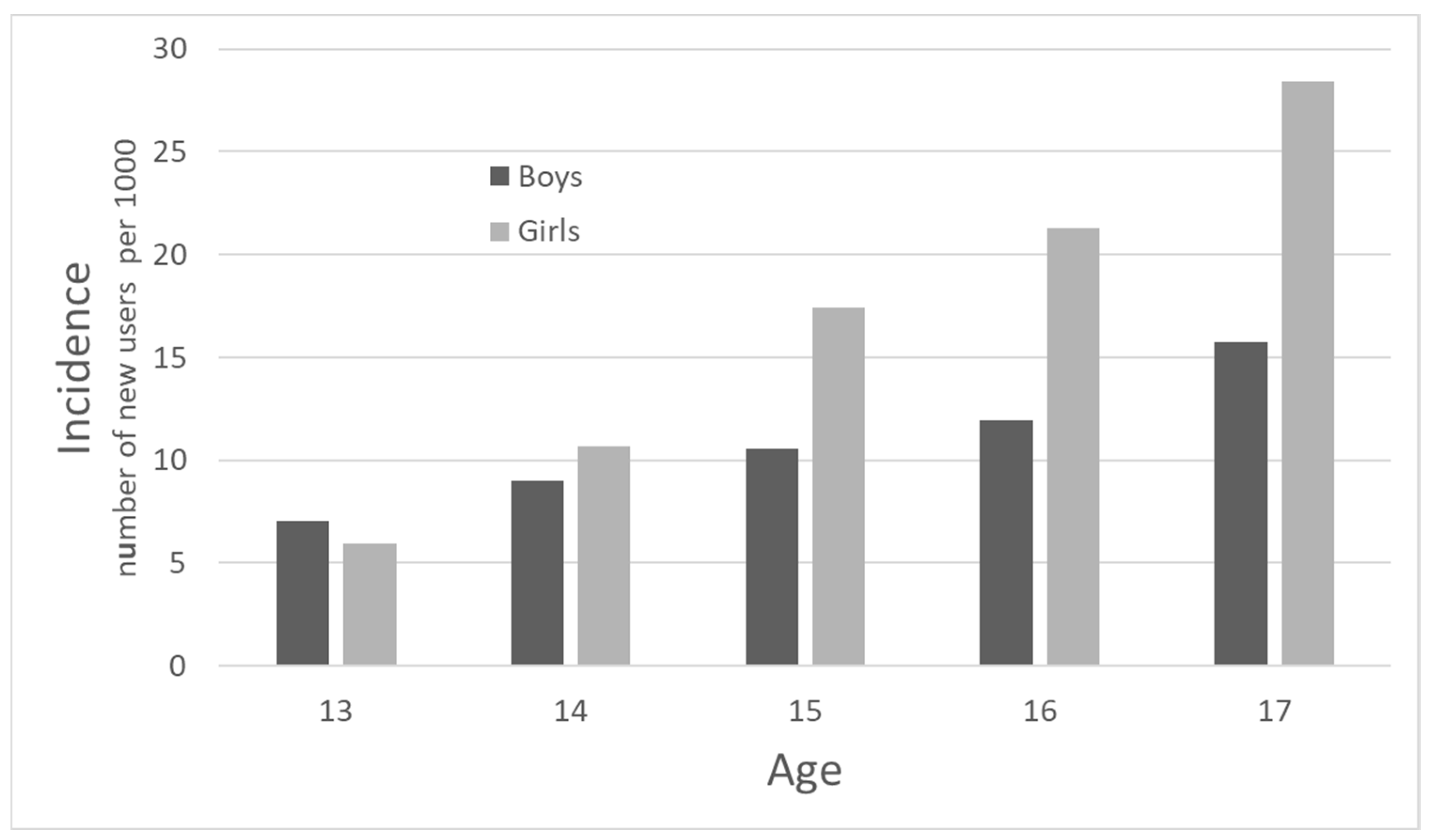
3.3. Incident Hypnotic Drug Users
- (a)
- Incidence rate
- (b)
- Type of first hypnotic drug use and amount dispensed to incident hypnotic drug users
- (c)
- Contact with secondary health care among incident hypnotic drug users
- (d)
- Diagnoses from secondary health care among incident hypnotic drug users
- (e)
- Diagnoses during Childhood among incident hypnotic drug users
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piovani, D.; Clavenna, A.; Bonati, M. Prescription prevalence of psychotropic drugs in children and adolescents: An analysis of international data. Eur. J. Clin. Pharmacol. 2019, 75, 1333–1346. [Google Scholar] [CrossRef]
- Wesselhoeft, R.; Rasmussen, L.; Jensen, P.B.; Jennum, P.J.; Skurtveit, S.; Hartz, I.; Reutfors, J.; Damkier, P.; Bliddal, M.; Pottegård, A. Use of hypnotic drugs among children, adolescents, and young adults in Scandinavia. Acta Psychiatr. Scand. 2021, 144, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Abbas, S.; Ihle, P.; Adler, J.B.; Engel, S.; Gunster, C.; Linder, R.; Lehmkuhl, G.; Schubert, I. Psychopharmacological Prescriptions in Children and Adolescents in Germany. Dtsch. Arztebl. Int. 2016, 113, 396–403. [Google Scholar] [CrossRef]
- Zoega, H.; Baldursson, G.; Hrafnkelsson, B.; Almarsdottir, A.B.; Valdimarsdottir, U.; Halldorsson, M. Psychotropic drug use among Icelandic children: A nationwide population-based study. J. Child. Adolesc. Psychopharmacol. 2009, 19, 757–764. [Google Scholar] [CrossRef]
- Hartz, I.; Skurtveit, S.; Steffenak, A.K.; Karlstad, O.; Handal, M. Psychotropic drug use among 0–17 year olds during 2004–2014: A nationwide prescription database study. BMC Psychiatry 2016, 16, 12. [Google Scholar] [CrossRef] [PubMed]
- Hartz, I.; Furu, K.; Bratlid, T.; Handal, M.; Skurtveit, S. Hypnotic drug use among 0–17 year olds during 2004–2011: A nationwide prescription database study. Scand. J. Public Health 2012, 40, 704–711. [Google Scholar] [CrossRef]
- Hartz, I.; Handal, M.; Tverdal, A.; Skurtveit, S. Paediatric Off-Label Use of Melatonin—A Register Linkage Study between the Norwegian Prescription Database and Patient Register. Basic. Clin. Pharmacol. Toxicol. 2015, 117, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, E.S.; Rasmussen, L.; Hellfritzsch, M.; Thomsen, P.H.; Norgaard, M.; Laursen, T. Trends in Off-Label Prescribing of Sedatives, Hypnotics and Antidepressants among Children and Adolescents—A Danish, Nationwide Register-Based Study. Basic. Clin. Pharmacol. Toxicol. 2017, 120, 360–367. [Google Scholar] [CrossRef]
- Swedish Medical Products Agency. Kartläggning av Melatoninanvändning hos Barn och Ungdomar. Available online: https://www.lakemedelsverket.se/sv/om-lakemedelsverket/rapporter-och-publikationer/barn-och-ungdomar/kartlaggning-av-melatoninanvandning-hos-barn-och-ungdomar (accessed on 12 February 2024).
- The Norwegian Medicines Agency. Klassifisering av Melatonin. Available online: https://legemiddelverket.no/godkjenning/klassifisering/produktspesifikke-veiledere-om-klassifisering/klassifisering-av-melatonin (accessed on 12 February 2024).
- Bliddal, M.; Kildegaard, H.; Rasmussen, L.; Ernst, M.; Jennum, P.J.; Mogensen, S.H.; Pottegård, A.; Wesselhoeft, R. Melatonin use among children, adolescents, and young adults: A Danish nationwide drug utilization study. Eur. Child Adolesc. Psychiatry 2023, 32, 2021–2029. [Google Scholar] [CrossRef]
- Hysing, M.; Pallesen, S.; Stormark, K.M.; Lundervold, A.J.; Sivertsen, B. Sleep patterns and insomnia among adolescents: A population-based study. J. Sleep Res. 2013, 22, 549–556. [Google Scholar] [CrossRef]
- Pallesen, S.; Hetland, J.; Sivertsen, B.; Samdal, O.; Torsheim, T.; Nordhus, I.H. Time trends in sleep-onset difficulties among Norwegian adolescents: 1983–2005. Scand. J. Public Health 2008, 36, 889–895. [Google Scholar] [CrossRef]
- Bakken, A. Ungdata. National results. NOVA 2018, 8/18. Available online: https://oda.oslomet.no/oda-xmlui/bitstream/handle/20.500.12199/5128/Ungdata-2018.%20Nasjonale%20resultater.pdf?sequence=1&isAllowed=y (accessed on 12 February 2024).
- Rangul, V.; Kvaløy, K. Self-Perceived Health, Body Mass and Risk Behavior among Adolescents in Nord-Trøndelag County 2017–2019. Available online: https://www.ntnu.no/documents/10304/4902807/Delrapport1_Ung_HUNT4+_Mars2020.pdf/e7f7a922-906f-aa1c-9aed-4fa2d7bf14b9?t=1584711026088 (accessed on 12 February 2024).
- Baglioni, C.; Nanovska, S.; Regen, W.; Spiegelhalder, K.; Feige, B.; Nissen, C.; Reynolds, C.F.; Riemann, D. Sleep and mental disorders: A meta-analysis of polysomnographic research. Psychol. Bull. 2016, 142, 969–990. [Google Scholar] [CrossRef] [PubMed]
- Ford, D.E.; Kamerow, D.B. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA 1989, 262, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Norwegian Prescription Database (NorPD). Available online: https://www.fhi.no/en/hn/health-registries/norpd/ (accessed on 12 February 2024).
- WHO Collaborating Centre for Drug Statistics Methodology. ATC Classification Index with DDDs. WHO Collaborating Centre for Drug Statistics Methodology, Oslo. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 12 February 2024).
- The Norwegian Patient Register. Available online: https://www.helsedirektoratet.no/tema/statistikk-registre-og-rapporter/helsedata-og-helseregistre/norsk-pasientregister-npr (accessed on 12 February 2024).
- WHO. ICD-10 Version:2019. Available online: https://icd.who.int/browse10/2019/en#/I (accessed on 12 February 2024).
- Norwegian Directorate of Health. Norway Control and Payment of Health Reimbursements (KHUR) Database. Available online: https://www.helsedirektoratet.no/tema/statistikk-registre-og-rapporter/helsedata-og-helseregistre/kuhr (accessed on 12 February 2024).
- Sivertsen, B.; Harvey, A.G.; Pallesen, S.; Hysing, M. Trajectories of sleep problems from childhood to adolescence: A population-based longitudinal study from Norway. J. Sleep Res. 2017, 26, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, I. Stress og Press Blant Ungdom. In Erfaringer, Årsaker og Utbredelse av Psykiske Helseplager; NOVA: Osaka, Japan, 2017. [Google Scholar]
- Collishaw, S. Annual research review: Secular trends in child and adolescent mental health. J. Child. Psychol. Psychiatry 2015, 56, 370–393. [Google Scholar] [CrossRef] [PubMed]
- Lien, L.; Bonsaksen, T.; Holte Stea, T.; Kleppang, A.L.; Steigen, A.M.; Leonhardt, M. Time trends in self-reported depressive symptoms, prescription of antidepressants, sedatives and hypnotics and the emergence of social media among Norwegian adolescents. PLoS ONE 2023, 18, e0295384. [Google Scholar] [CrossRef] [PubMed]
- Zahn-Waxler, C.; Shirtcliff, E.A.; Marceau, K. Disorders of childhood and adolescence: Gender and psychopathology. Annu. Rev. Clin. Psychol. 2008, 4, 275–303. [Google Scholar] [CrossRef]
- Paus, T.; Keshavan, M.; Giedd, J.N. Why do many psychiatric disorders emerge during adolescence? Nat. Rev. Neurosci. 2008, 9, 947–957. [Google Scholar] [CrossRef]
- Bangasser, D.A.; Valentino, R.J. Sex differences in stress-related psychiatric disorders: Neurobiological perspectives. Front. Neuroendocrinol. 2014, 35, 303–319. [Google Scholar] [CrossRef]
- Hammerslag, L.R.; Gulley, J.M. Sex differences in behavior and neural development and their role in adolescent vulnerability to substance use. Behav. Brain Res. 2016, 298, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Ullebo, A.K.; Posserud, M.B.; Heiervang, E.; Obel, C.; Gillberg, C. Prevalence of the ADHD phenotype in 7- to 9-year-old children: Effects of informant, gender and non-participation. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Abdelgadir, I.S.; Gordon, M.A.; Akobeng, A.K. Melatonin for the management of sleep problems in children with neurodevelopmental disorders: A systematic review and meta-analysis. Arch. Dis. Child. 2018, 103, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.; Beresford, B.; Dawson, V.; Elphick, H.; Fairhurst, C.; Hewitt, C.; Scantlebury, A.; Spiers, G.; Thomas, M.; Wright, K.; et al. Oral melatonin for non-respiratory sleep disturbance in children with neurodisabilities: Systematic review and meta-analyses. Dev. Med. Child. Neurol. 2019, 61, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Smits, M.G.; Tang, X.; Kuang, L.; Meng, H.; Ni, S.; Xiao, M.; Zhou, X. Efficacy and safety of melatonin for sleep onset insomnia in children and adolescents: A meta-analysis of randomized controlled trials. Sleep Med. 2020, 68, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.P.; Gogenur, I.; Rosenberg, J.; Reiter, R.J. The Safety of Melatonin in Humans. Clin. Drug Investig. 2016, 36, 169–175. [Google Scholar] [CrossRef]
- Slordal, L.; Bramness, J.G. Is alimemazine a suitable sleeping agent for children? Tidsskr. Nor. Laegeforen. 2008, 128, 2194–2196. [Google Scholar]
- De Bruyne, P.; Christiaens, T.; Boussery, K.; Mehuys, E.; Van Winckel, M. Are antihistamines effective in children? A review of the evidence. Arch. Dis. Child. 2017, 102, 56–60. [Google Scholar] [CrossRef]
- Dewald-Kaufmann, J.; de Bruin, E.; Michael, G. Cognitive Behavioral Therapy for Insomnia in School-Aged Children and Adolescents. Sleep Med. Clin. 2022, 17, 355–365. [Google Scholar] [CrossRef]
- Vedaa, O.; Kallestad, H.; Scott, J.; Smith, O.R.F.; Pallesen, S.; Morken, G.; Langsrud, K.; Gehrman, P.; Thorndike, F.P.; Ritterband, L.M.; et al. Effects of digital cognitive behavioural therapy for insomnia on insomnia severity: A large-scale randomised controlled trial. Lancet Digit. Health 2020, 2, e397–e406. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.J.; Yang, A.C.; Zhu, J.D.; Hsu, Y.Y.; Hsu, T.F.; Tsai, S.J. Effectiveness of Digital Cognitive Behavioral Therapy for Insomnia in Young People: Preliminary Findings from Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 481. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hypnotic Drug | Boys | Girls | ||
|---|---|---|---|---|
| n | % | n | % | |
| melatonin | 1168 | 68.0 | 1738.0 | 69.0 |
| alimemazine | 465 | 27.1 | 675 | 26.8 |
| zopiclone | 58 | 3.4 | 71 | 2.8 |
| zolpidem | 16 | 0.9 | 22 | 0.9 |
| nitrazepam | <11 | - | <13 | - |
| flunitrazepam | <5 | - | <5 | - |
| Age (Years) | DDD/365 Days | Number of Prescriptions Filled/365 Days | ||
|---|---|---|---|---|
| Median (IQR) | Median (IQR) | |||
| Girls | Boys | Girls | Boys | |
| 13 | 150 (56–360) | 180 (90–450) | 2.5 (1–5) | 3 (1–5) |
| 14 | 120 (59–360) | 120 (78–360) | 2 (1–4) | 2 (1–4) |
| 15 | 90 (30–270) | 98 (30–270) | 2 (1–4) | 2 (1–4) |
| 16 | 90 (30–194) | 90 (30–227) | 2 (1–3) | 2 (1–4) |
| 17 | 90 (30–180) | 69 (30–150) | 2 (1–3) | 1 (1–3) |
| ICD-10 Diagnosis Blocks | Boys | Girls | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| General Population | Hypnotic Users | General Population | Hypnotic Users | |||||||
| n = 189,900 | n = 1718 | p | n = 179,270 | n = 2519 | p | |||||
| n | % | n | % | n | % | n | % | |||
| A | 2914 | 1.6 | 132 | 7.7 | <0.001 | 2465 | 1.4 | 190 | 7.5 | <0.001 |
| B | 4747 | 2.6 | 62 | 3.6 | <0.001 | 5278 | 2.9 | 97 | 3.9 | <0.001 |
| C | 391 | 0.2 | 8 | 0.5 | 0.019 | 302 | 0.2 | 7 | 0.3 | 0.186 |
| D | 4922 | 2.7 | 48 | 2.8 | 0.600 | 4952 | 2.8 | 77 | 3.1 | 0.371 |
| E | 5891 | 3.3 | 0 | 0.0 | <0.001 | 6568 | 3.7 | 0 | 0.0 | 0.001 |
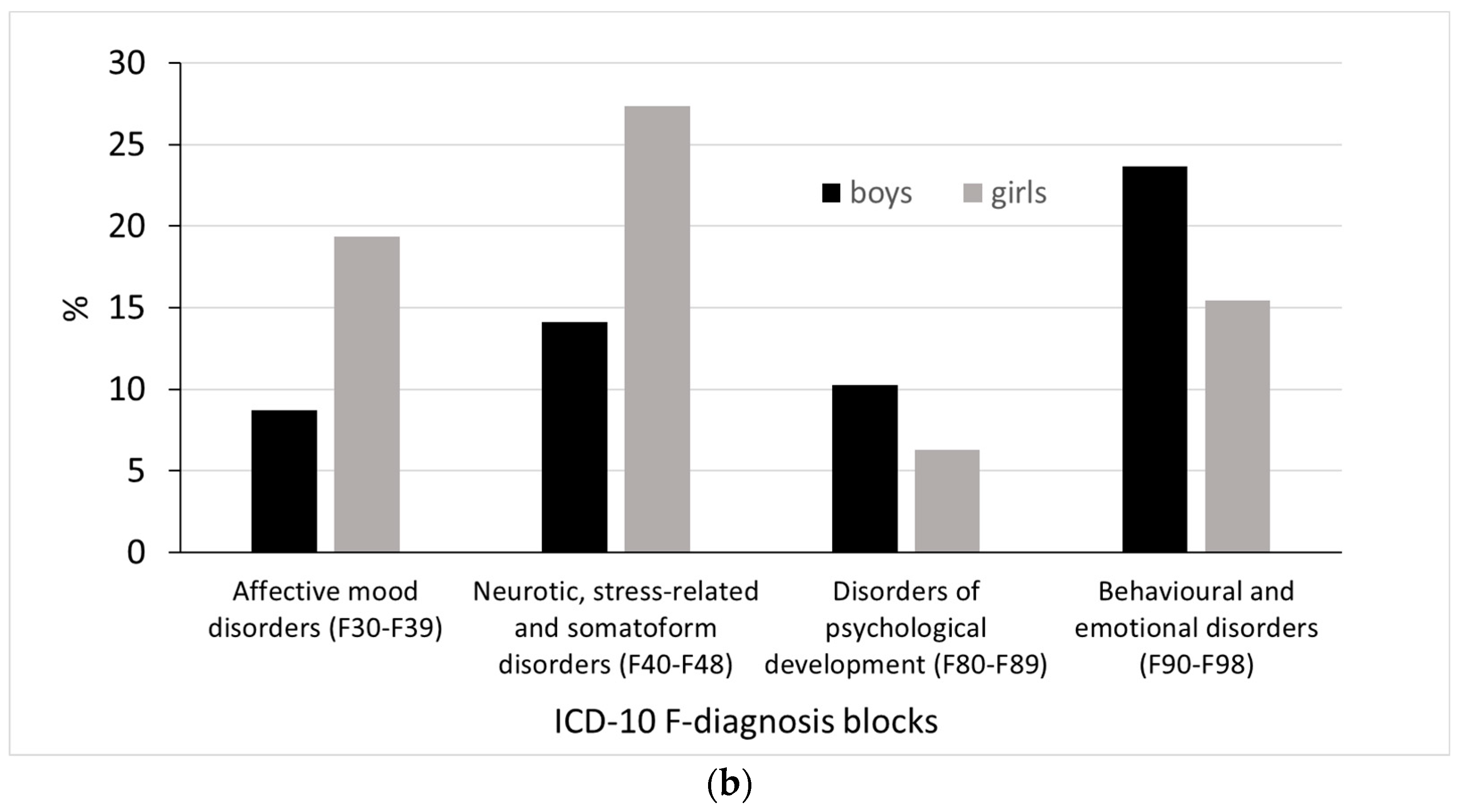
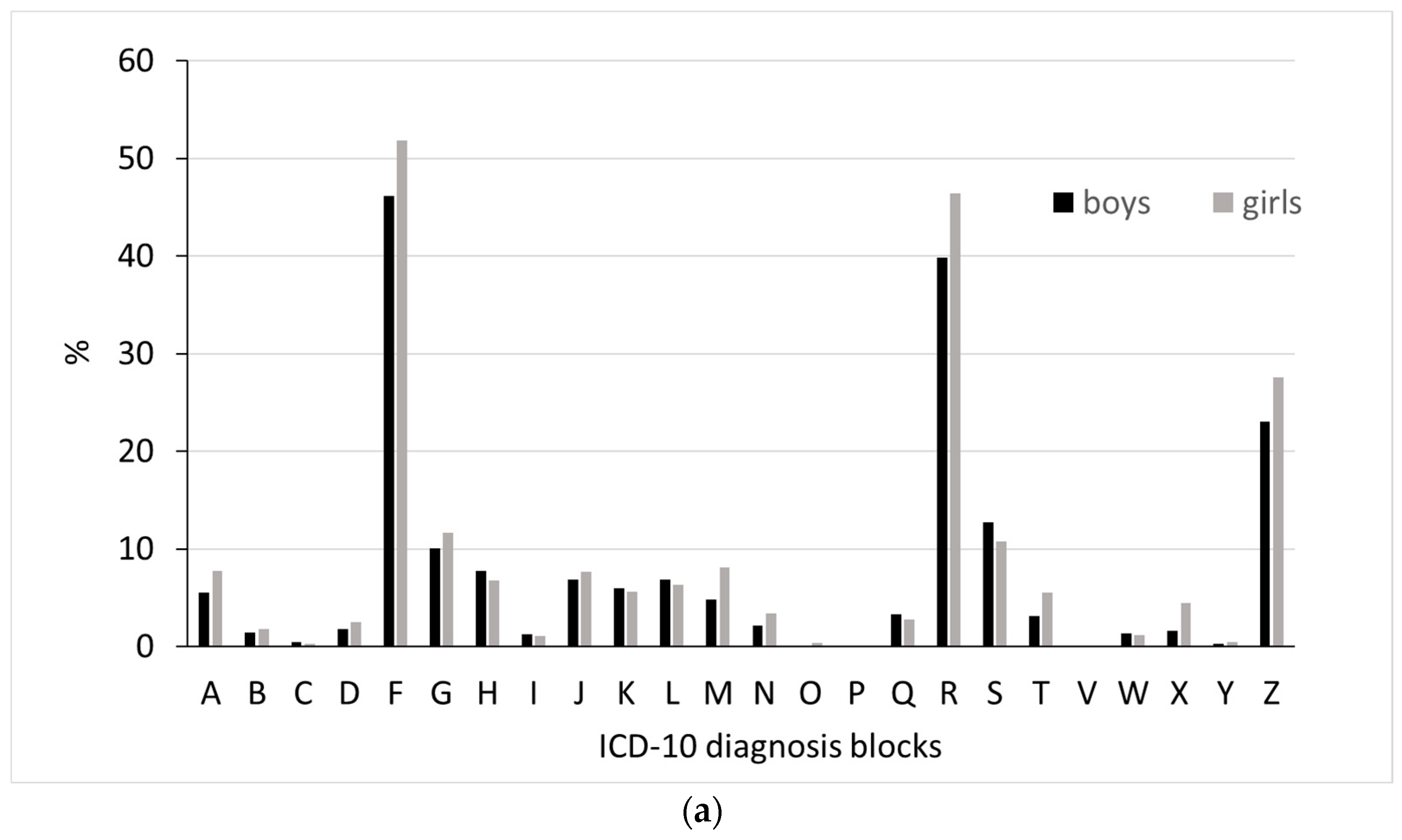
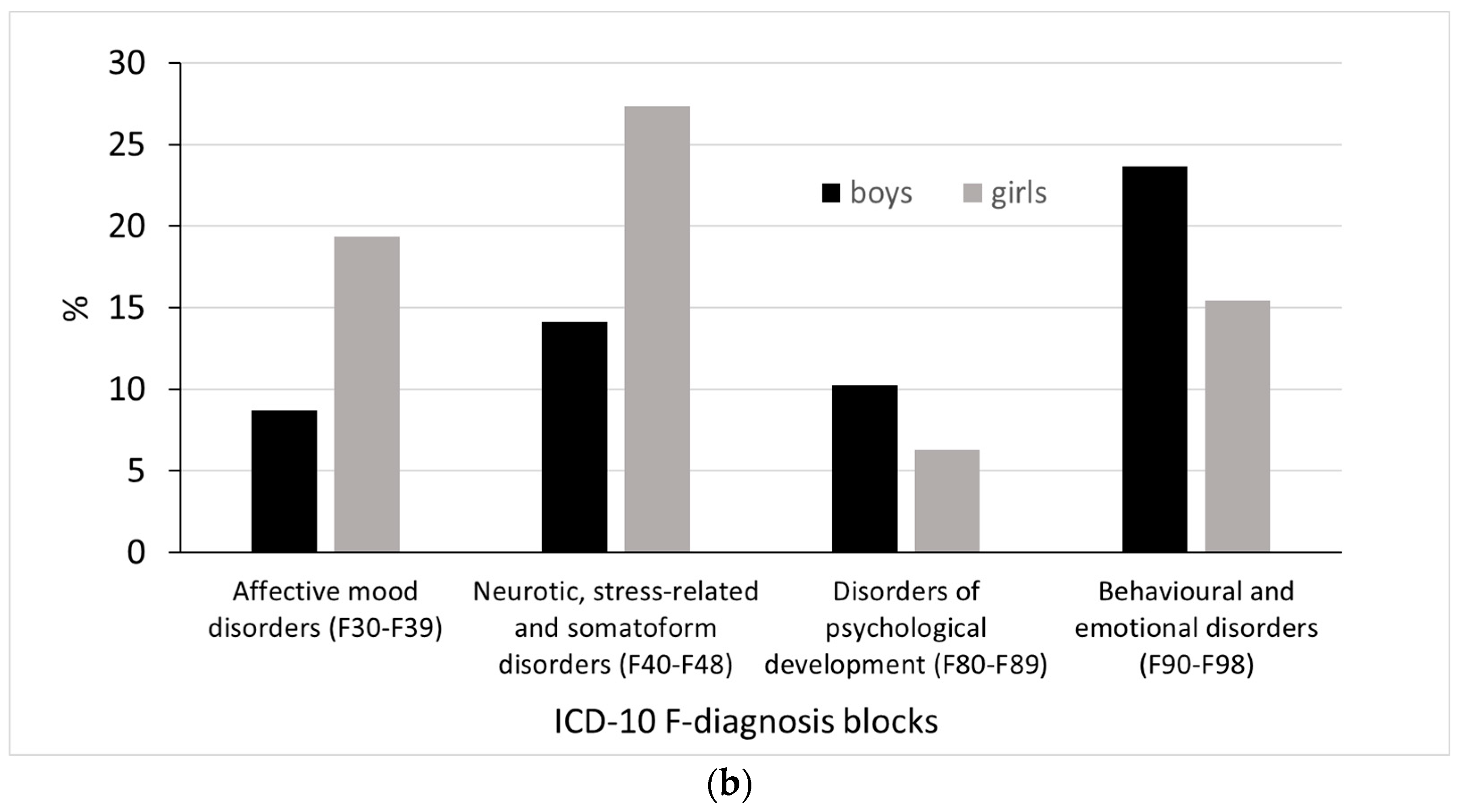
| F | 22,960 | 12.8 | 622 | 36.2 | <0.001 | 12,417 | 6.9 | 492 | 19.5 | <0.001 |
| G | 7349 | 4.1 | 161 | 9.4 | <0.001 | 5670 | 3.2 | 161 | 6.4 | <0.001 |
| H | 30,726 | 17.1 | 362 | 21.1 | <0.001 | 28,916 | 16.1 | 552 | 21.9 | <0.001 |
| I | 2109 | 1.2 | 31 | 1.8 | 0.006 | 1789 | 1.0 | 34 | 1.3 | 0.078 |
| J | 26,860 | 15 | 316 | 18.4 | <0.001 | 20,920 | 11.7 | 396 | 15.7 | <0.001 |
| K | 13,903 | 7.8 | 218 | 12.7 | <0.001 | 12,493 | 7.0 | 315 | 12.5 | <0.001 |
| L | 10,550 | 5.9 | 119 | 6.9 | 0.014 | 10,884 | 6.1 | 206 | 8.2 | <0.001 |
| M | 10,563 | 5.9 | 166 | 9.7 | <0.001 | 10,650 | 5.9 | 244 | 9.7 | <0.001 |
| N | 10,142 | 5.7 | 147 | 8.6 | <0.001 | 4440 | 2.5 | 99 | 3.9 | <0.001 |
| O | <5 | <5 | * | 25 | 0.0 | <5 | * | |||
| P | 269 | 0.2 | <5 | * | 155 | 0.1 | 6 | 0.2 | 0.011 | |
| Q | 11,691 | 6.5 | 145 | 8.4 | <0.001 | 8654 | 4.8 | 160 | 6.4 | <0.001 |
| R | 28,777 | 16.1 | 463 | 26.9 | <0.001 | 24,397 | 13.6 | 616 | 24.5 | <0.001 |
| S | 52,897 | 29.5 | 605 | 35.2 | <0.001 | 46,038 | 25.7 | 968 | 38.4 | <0.001 |
| T | 9842 | 5.5 | 127 | 7.4 | <0.001 | 7668 | 4.3 | 148 | 5.9 | <0.001 |
| U | 9 | 0.0 | 0 | 0.0 | 0.775 | 19 | 0.0 | 0 | 0.0 | 0.605 |
| V | 947 | 0.5 | 5 | 0.3 | 0.223 | 614 | 0.3 | 17 | 0.7 | 0.005 |
| W | 5874 | 3.3 | 82 | 4.8 | <0.001 | 4972 | 2.8 | 108 | 4.3 | <0.001 |
| X | 1147 | 0.6 | 24 | 1.4 | <0.001 | 889 | 0.5 | 22 | 0.9 | 0.008 |
| Y | 235 | 0.1 | <5 | * | 167 | 0.1 | <5 | * | ||
| Z | 58,461 | 32.6 | 887 | 51.6 | <0.001 | 48,874 | 27.3 | 1055 | 41.9 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharikabad, M.N.; Skurtveit, S.; Sommerschild, H.T.; Olsen, K.; Hartz, I.; Wesselhoeft, R.; Hjellvik, V.; Hauge, L.J.; Handal, M. Morbidity among Adolescent Hypnotic Drug Users in Norway: An Observational Population-Based Study. J. Clin. Med. 2024, 13, 1075. https://doi.org/10.3390/jcm13041075
Sharikabad MN, Skurtveit S, Sommerschild HT, Olsen K, Hartz I, Wesselhoeft R, Hjellvik V, Hauge LJ, Handal M. Morbidity among Adolescent Hypnotic Drug Users in Norway: An Observational Population-Based Study. Journal of Clinical Medicine. 2024; 13(4):1075. https://doi.org/10.3390/jcm13041075
Chicago/Turabian StyleSharikabad, Mohammad Nouri, Svetlana Skurtveit, Hilchen Thode Sommerschild, Kristine Olsen, Ingeborg Hartz, Rikke Wesselhoeft, Vidar Hjellvik, Lars Johan Hauge, and Marte Handal. 2024. "Morbidity among Adolescent Hypnotic Drug Users in Norway: An Observational Population-Based Study" Journal of Clinical Medicine 13, no. 4: 1075. https://doi.org/10.3390/jcm13041075
APA StyleSharikabad, M. N., Skurtveit, S., Sommerschild, H. T., Olsen, K., Hartz, I., Wesselhoeft, R., Hjellvik, V., Hauge, L. J., & Handal, M. (2024). Morbidity among Adolescent Hypnotic Drug Users in Norway: An Observational Population-Based Study. Journal of Clinical Medicine, 13(4), 1075. https://doi.org/10.3390/jcm13041075