
Management and Outcome of Women with Placenta Accreta Spectrum and Treatment with Uterine Artery Embolization

 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Data
2.2. Management of Women Diagnosed with PAS
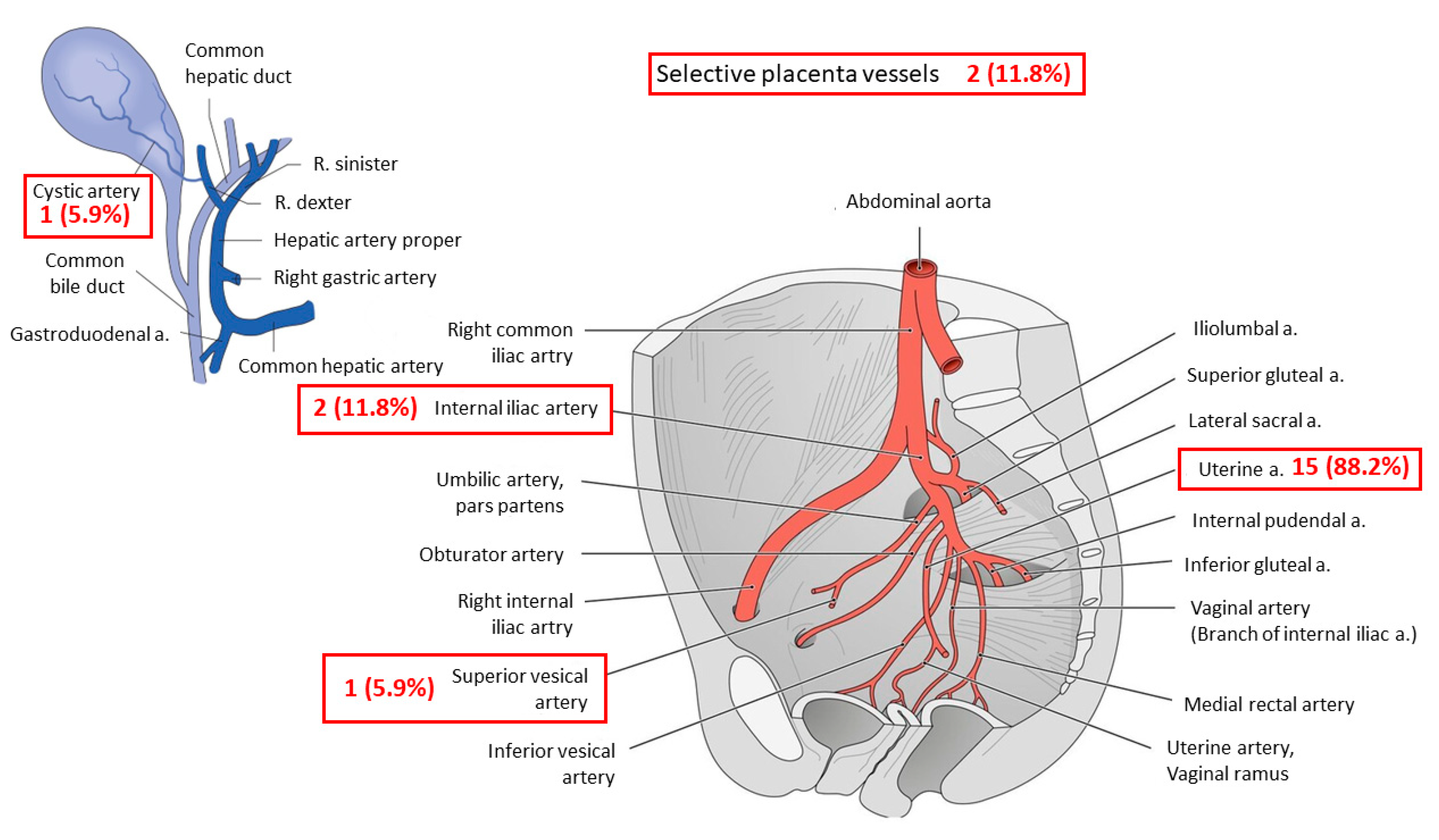
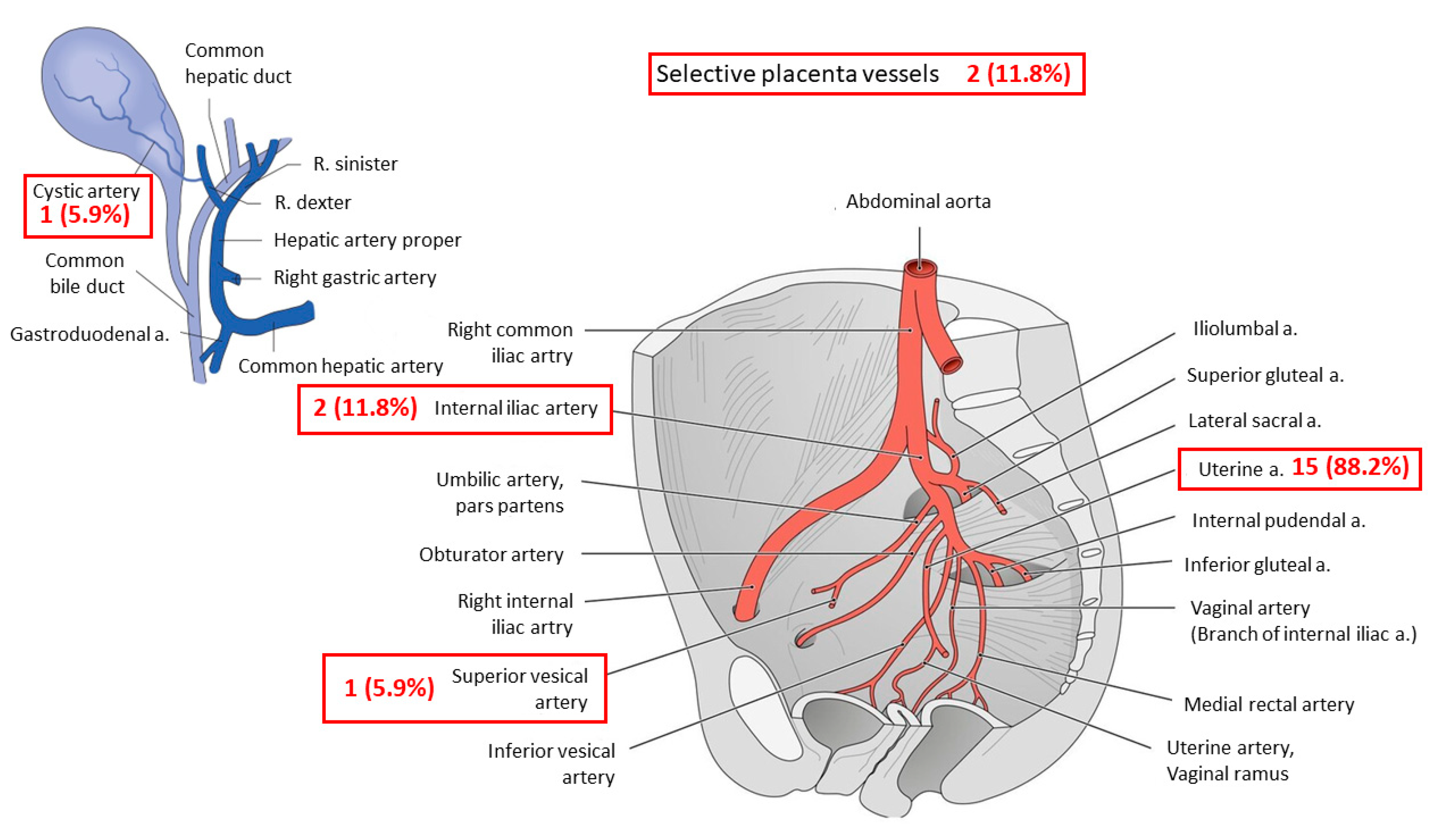
2.3. Embolization
2.4. Definition of Anemia, PPH and RBC Transfusion
2.5. Statistical Analysis
3. Results
3.1. Patient’s Characteristics
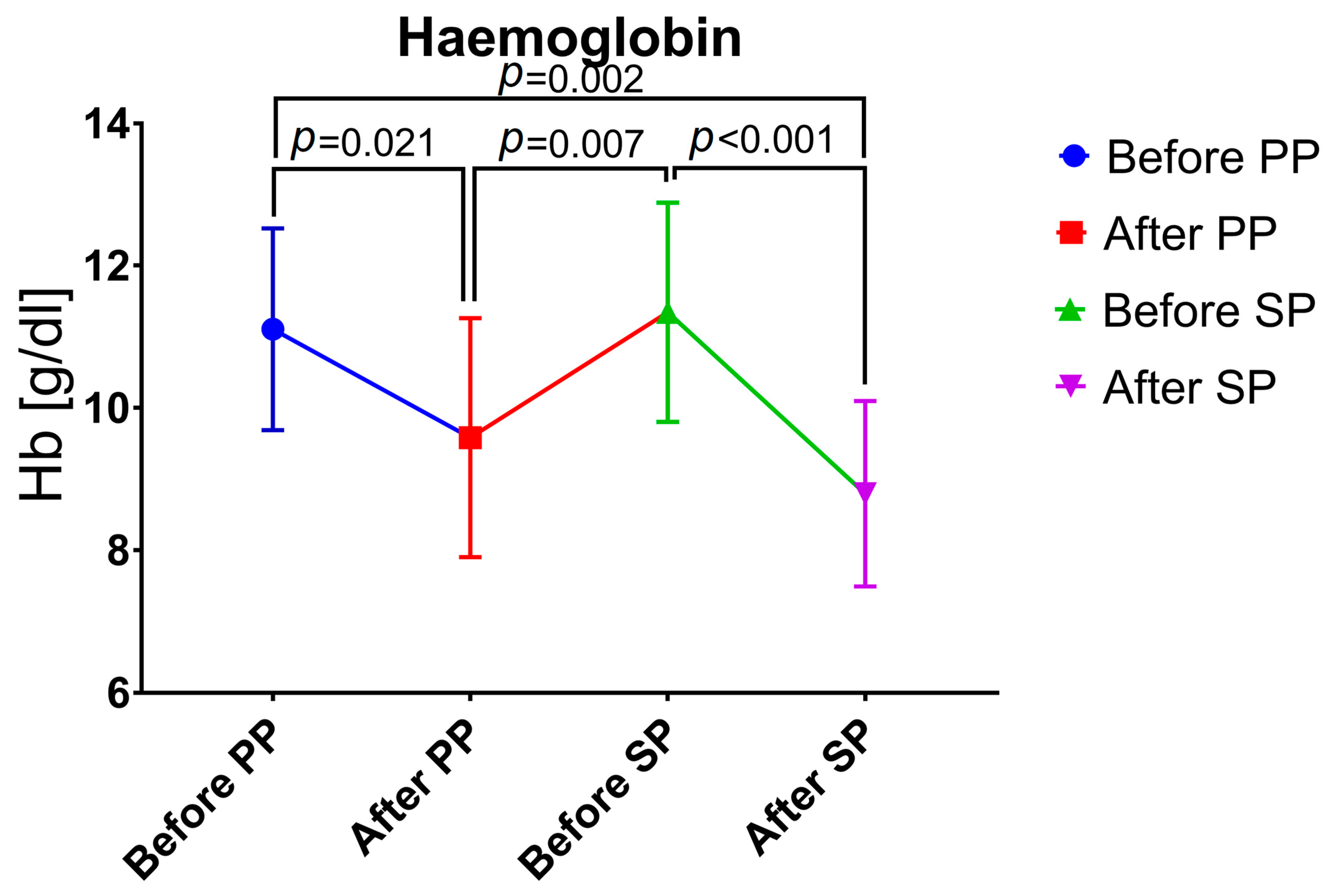
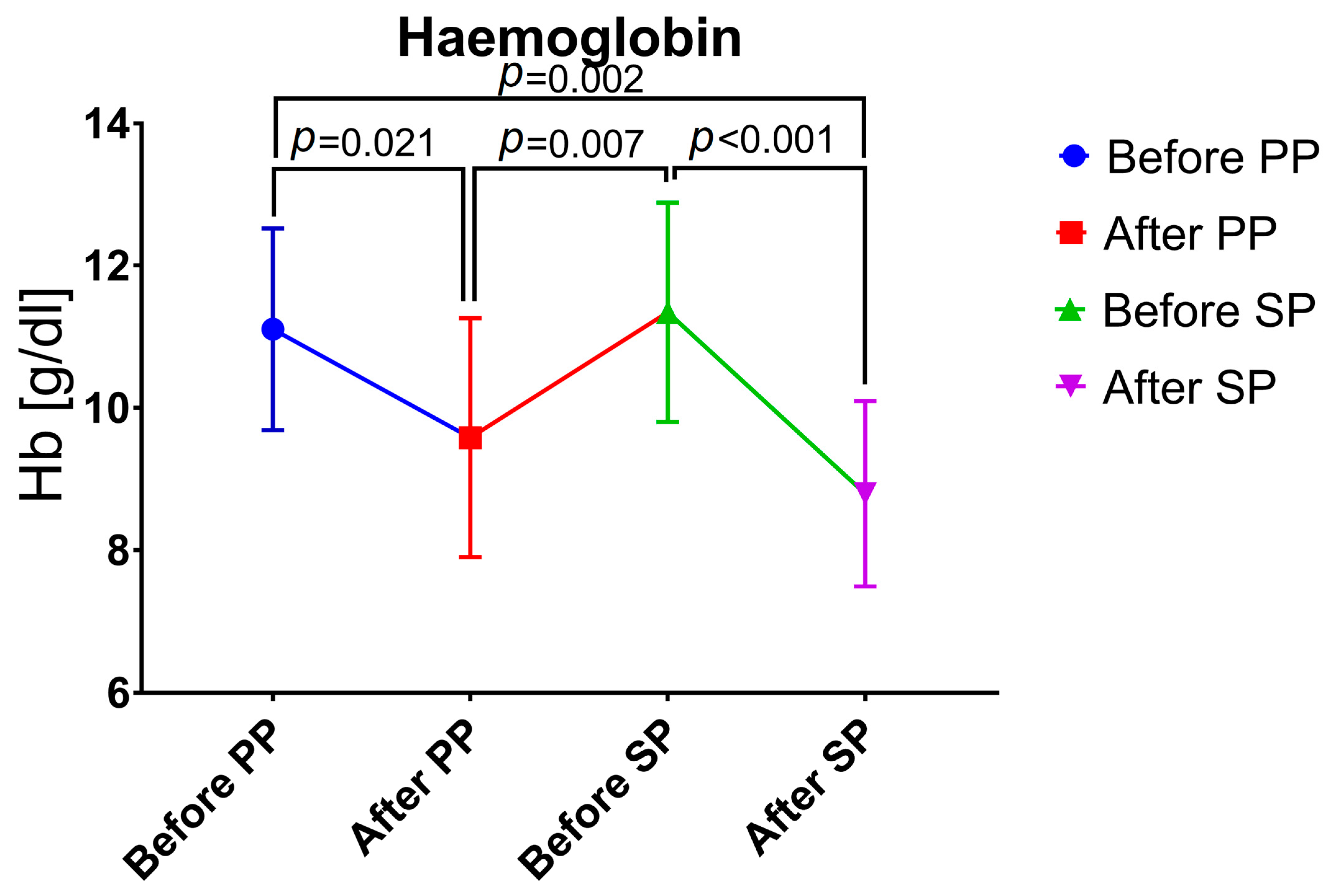
3.2. Administration of Blood Products, Hb Values and the Anemia Rate
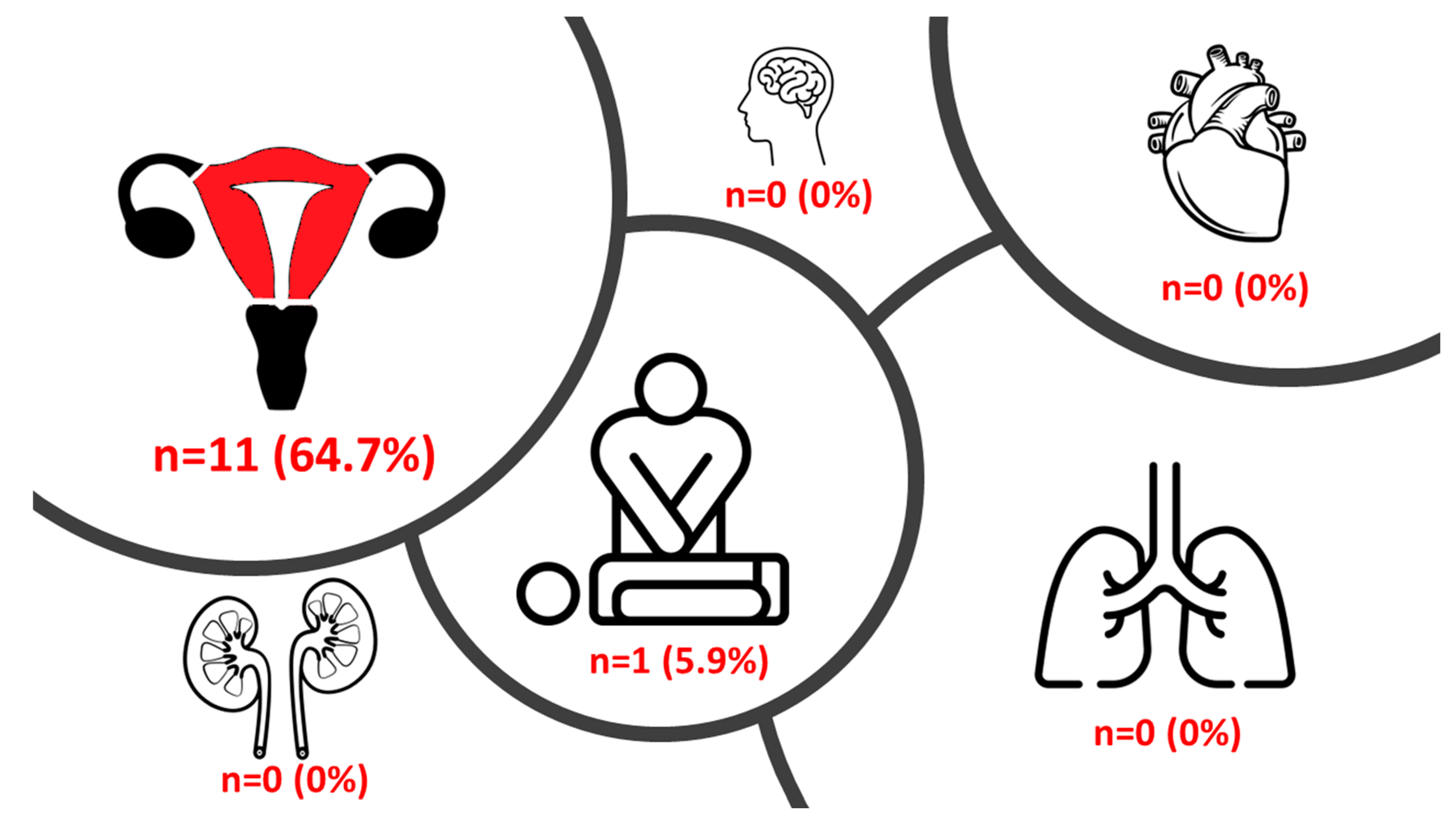
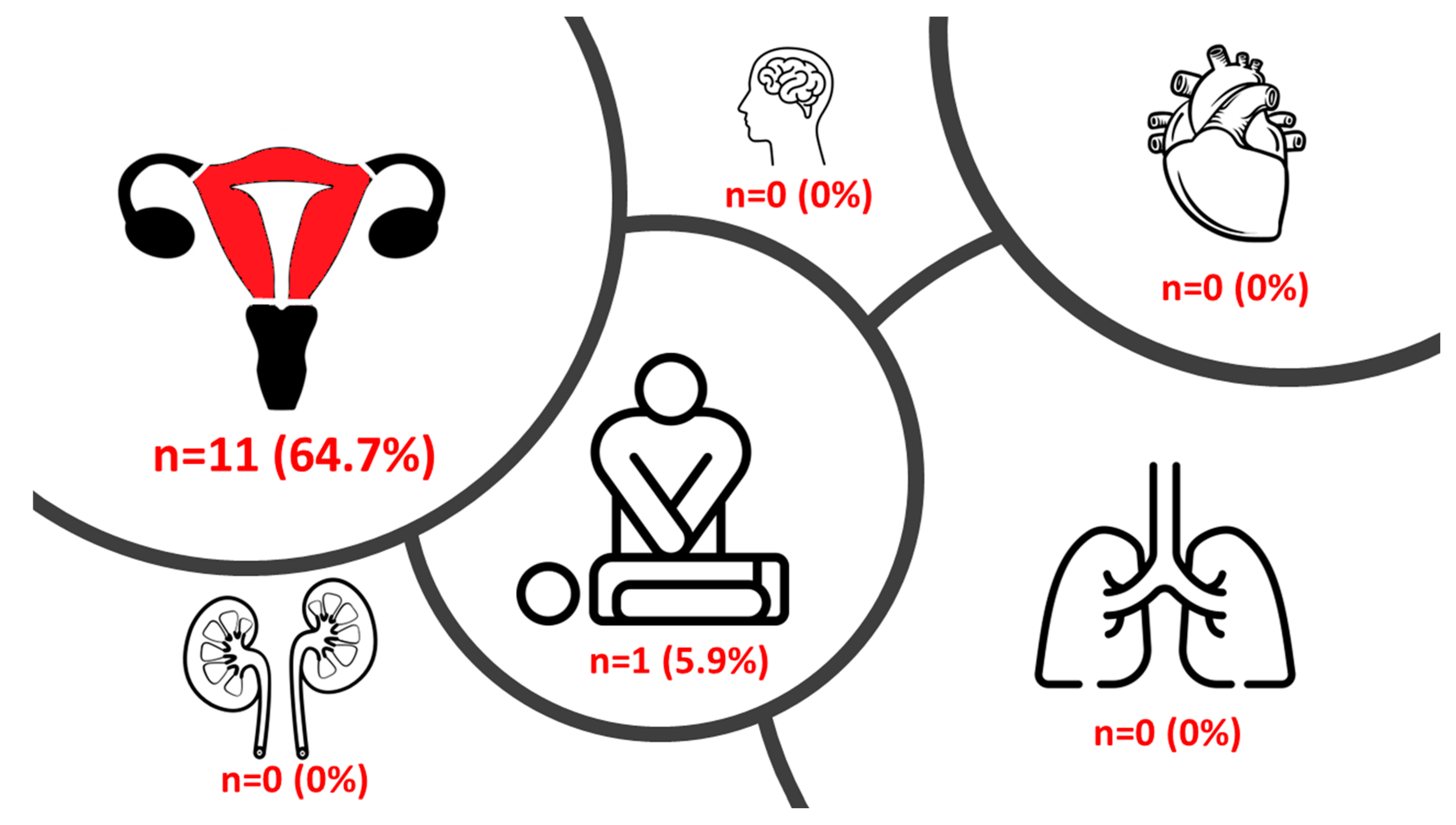
3.3. Outcome of Study Population
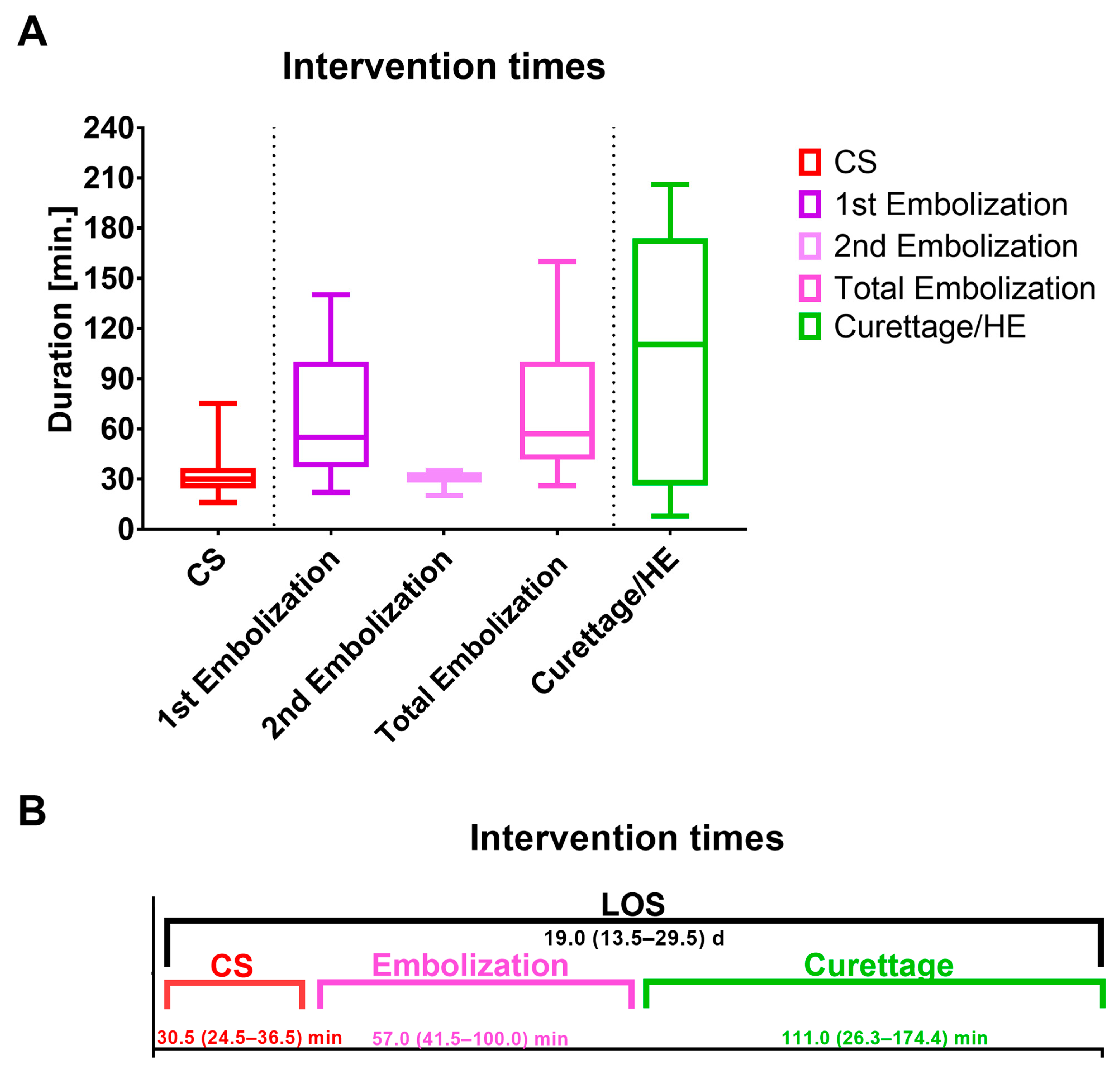
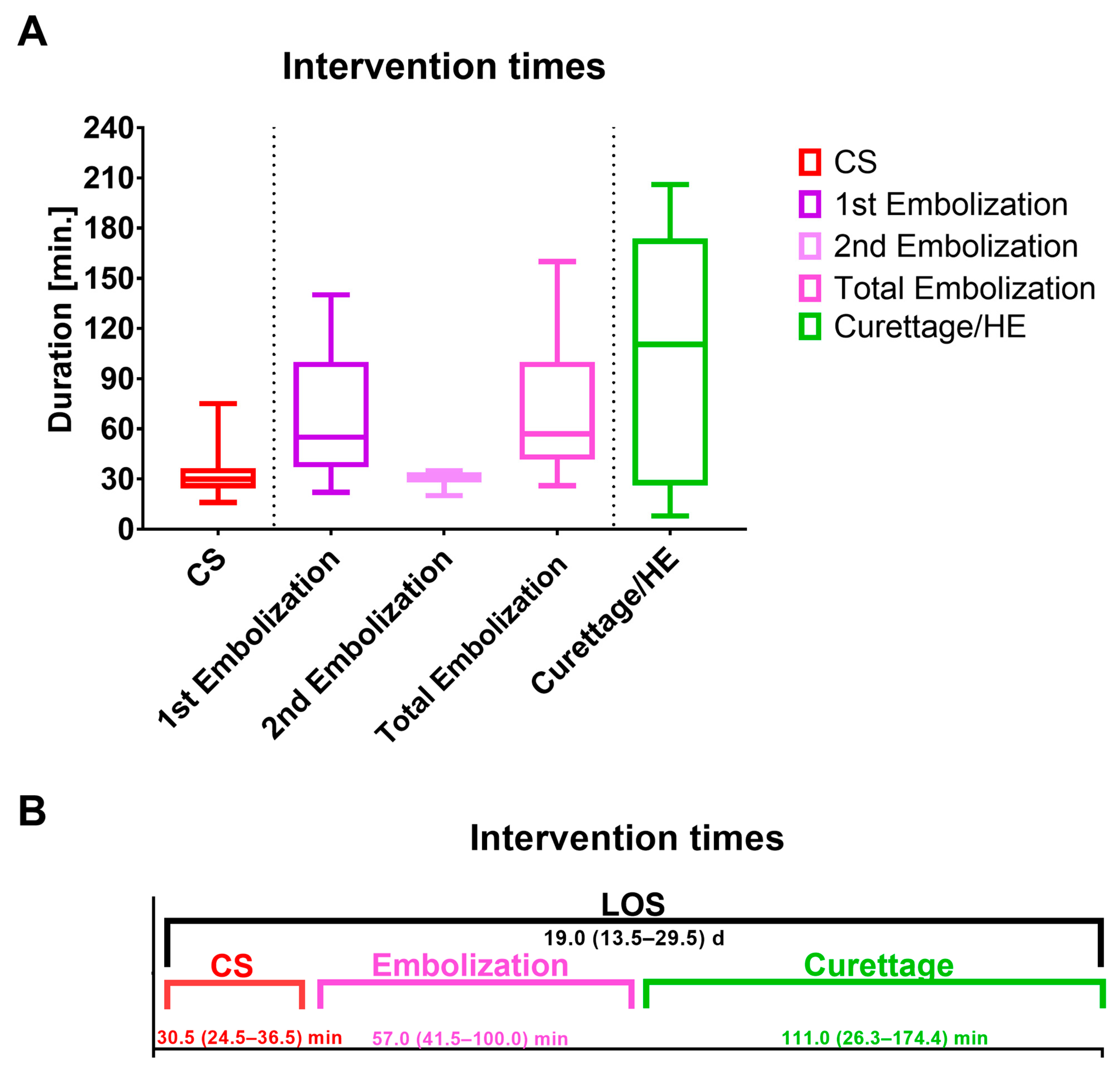
3.4. Anesthesiological and Surgical Management
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silver, R.M.; Branch, D.W. Placenta Accreta Spectrum. N. Engl. J. Med. 2018, 378, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Kocherginsky, M.; Hibbard, J.U. Abnormal placentation: Twenty-year analysis. Am. J. Obstet. Gynecol. 2005, 192, 1458–1461. [Google Scholar] [CrossRef] [PubMed]
- Conturie, C.L.; Lyell, D.J. Prenatal diagnosis of placenta accreta spectrum. Curr. Opin. Obstet. Gynecol. 2022, 34, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Shamshirsaz, A.A.; Fox, K.A.; Salmanian, B.; Diaz-Arrastia, C.R.; Lee, W.; Baker, B.W.; Ballas, J.; Chen, Q.; Van Veen, T.R.; Javadian, P.; et al. Maternal morbidity in patients with morbidly adherent placenta treated with and without a standardized multidisciplinary approach. Am. J. Obstet. Gynecol. 2015, 212, 218.e1–218.e9. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Jaraquemada, J.M. Diagnosis and management of placenta accreta. Best Pract. Res. Clin. Obstet. Gynaecol. 2008, 22, 1133–1148. [Google Scholar] [CrossRef] [PubMed]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet. Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef]
- Wright, J.D.; Pri-Paz, S.; Herzog, T.J.; Shah, M.; Bonanno, C.; Lewin, S.N.; Simpson, L.L.; Gaddipati, S.; Sun, X.; D’Alton, M.E.; et al. Predictors of massive blood loss in women with placenta accreta. Am. J. Obstet. Gynecol. 2011, 205, 38.e1–38.e6. [Google Scholar] [CrossRef]
- Miller, S.E.; Leonard, S.A.; Meza, P.K.; Ku, S.; Ren, L.Y.; Lyell, D.J.; Sultan, P.; Butwick, A. Red Blood Cell Transfusion in Patients With Placenta Accreta Spectrum: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2023, 141, 49–58. [Google Scholar] [CrossRef]
- Gatta, L.A.; Weber, J.M.; Gilner, J.B.; Lee, P.S.; Grotegut, C.A.; Herbert, K.A.; Bashir, M.; Pieper, C.F.; Ronald, J.; Pabon-Ramos, W.; et al. Transfusion Requirements with Hybrid Management of Placenta Accreta Spectrum Incorporating Targeted Embolization and a Selective Use of Delayed Hysterectomy. Am. J. Perinatol. 2022, 29, 1503–1513. [Google Scholar] [CrossRef]
- Sentilhes, L.; Goffinet, F.; Kayem, G. Management of placenta accreta. Acta Obstet. Et Gynecol. Scand. 2013, 92, 1125–1134. [Google Scholar] [CrossRef]
- Schlembach, D.; Helmer, H.; Henrich, W.; von Heymann, C.; Kainer, F.; Korte, W.; Kühnert, M.; Lier, H.; Maul, H.; Rath, W.; et al. Peripartum Haemorrhage, Diagnosis and Therapy. Guideline of the DGGG, OEGGG and SGGG (S2k Level, AWMF Registry No. 015/063, March 2016). Geburtshilfe Frauenheilkd 2018, 78, 382–399. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists; Society for Maternal-Fetal Medicine. Obstetric Care Consensus No. 7: Placenta Accreta Spectrum. Obstet. Gynecol. 2018, 132, e259–e275. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Alfirevic, Z.; Bhide, A.G.; Belfort, M.A.; Burton, G.J.; Collins, S.L.; Dornan, S.; Jurkovic, D.; Kayem, G.; Kingdom, J.; et al. Placenta Praevia and Placenta Accreta: Diagnosis and Management: Green-top Guideline No. 27a. BJOG Int. J. Obstet. Gynaecol. 2019, 126, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.M.; Barbour, K.D. Placenta accreta spectrum: Accreta, increta, and percreta. Obstet. Gynecol. Clin. North Am. 2015, 42, 381–402. [Google Scholar] [CrossRef] [PubMed]
- Eller, A.G.; Bennett, M.A.; Sharshiner, M.; Masheter, C.; Soisson, A.P.; Dodson, M.; Silver, R.M. Maternal morbidity in cases of placenta accreta managed by a multidisciplinary care team compared with standard obstetric care. Obstet. Gynecol. 2011, 117, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Shamshirsaz, A.A.; Fox, K.A.; Erfani, H.; Clark, S.L.; Salmanian, B.; Baker, B.W.; Coburn, M.; Shamshirsaz, A.A.; Bateni, Z.H.; Espinoza, J.; et al. Multidisciplinary team learning in the management of the morbidly adherent placenta: Outcome improvements over time. Am. J. Obstet. Gynecol. 2017, 216, 612.e1–612.e5. [Google Scholar] [CrossRef] [PubMed]
- Fratto, V.M.; Conturie, C.L.; Ballas, J.; Pettit, K.E.; Stephenson, M.L.; Truong, Y.N.; Henry, D.; Afshar, Y.; Murphy, A.; Kim, L.; et al. Assessing the multidisciplinary team approaches to placenta accreta spectrum across five institutions within the University of California fetal Consortium (UCfC). J. Matern.-Fetal Neonatal Med. 2021, 34, 2971–2976. [Google Scholar] [CrossRef] [PubMed]
- Melber, D.J.; Berman, Z.T.; Jacobs, M.B.; Picel, A.C.; Conturie, C.L.; Zhang-Rutledge, K.; Binder, P.S.; Eskander, R.N.; Roberts, A.C.; McHale, M.T.; et al. Placenta Accreta Spectrum Treatment With Intraoperative Multivessel Embolization: The PASTIME protocol. Am. J. Obstet. Gynecol. 2021, 225, 442.e1–442.e10. [Google Scholar] [CrossRef]
- Sebastian, B.; Rajesh, U.; Scott, P.M.; Sayeed, S.; Robinson, G.J.; Ettles, D.F.; Shrivastava, V.; Lakshminarayan, R. Prophylactic Uterine Artery Embolization in Placenta Accreta Spectrum-An Active Intervention to Reduce Morbidity and Promote Uterine Preservation. J. Vasc. Interv. Radiol. JVIR 2023, 34, 1922–1928. [Google Scholar] [CrossRef]
- Yang, C.C.; Chou, Y.C.; Kuo, T.N.; Liou, J.Y.; Cheng, H.M.; Kuo, Y.T. Prophylactic Intraoperative Uterine Artery Embolization During Cesarean Section or Cesarean Hysterectomy in Patients with Abnormal Placentation: A Systematic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2022, 45, 488–501. [Google Scholar] [CrossRef]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Anaemia. 2023. Available online: https://www.who.int/data/nutrition/nlis/info/anaemia (accessed on 8 February 2024).
- Bundesärztekammer. Querschnitts-Leitlinien zur Therapie mit Blutkomponenten und Plasmaderivaten. 2020. Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/_old-files/downloads/pdf-Ordner/MuE/Querschnitts-Leitlinien_BAEK_zur_Therapie_mit_Blutkomponenten_und_Plasmaderivaten-Gesamtnovelle_2020.pdf (accessed on 8 February 2024).
- Allen, L.; Jauniaux, E.; Hobson, S.; Papillon-Smith, J.; Belfort, M.A. FIGO consensus guidelines on placenta accreta spectrum disorders: Nonconservative surgical management. Int. J. Gynecol. Obstet. 2018, 140, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Sivan, E.; Spira, M.; Achiron, R.; Rimon, U.; Golan, G.; Mazaki-Tovi, S.; Schiff, E. Prophylactic pelvic artery catheterization and embolization in women with placenta accreta: Can it prevent cesarean hysterectomy? Am. J. Perinatol. 2010, 27, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Hayes, E.; Ayida, G.; Crocker, A. The morbidly adherent placenta: Diagnosis and management options. Curr. Opin. Obstet. Gynecol. 2011, 23, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Munoz, J.L.; Blankenship, L.M.; Ramsey, P.S.; McCann, G.A. Implementation and outcomes of a uterine artery embolization and tranexamic acid protocol for placenta accreta spectrum. Am. J. Obstet. Gynecol. 2023, 229, 61.e1–61.e7. [Google Scholar] [CrossRef] [PubMed]
- Mohr-Sasson, A.; Hochman, R.; Anteby, M.; Spira, M.; Castel, E.; Hendler, I.; Mazaki-Tovi, S.; Sivan, E. Cesarean delivery with and without uterine artery embolization for the management of placenta accreta spectrum disorder-A comparative study. Acta Obstet. Gynecol. Scand. 2020, 99, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Diop, A.N.; Bros, S.; Chabrot, P.; Gallot, D.; Boyer, L. Placenta percreta: Urologic complication after successful conservative management by uterine arterial embolization: A case report. Am. J. Obstet. Gynecol. 2009, 201, e7–e8. [Google Scholar] [CrossRef] [PubMed]
- Alanis, M.; Hurst, B.S.; Marshburn, P.B.; Matthews, M.L. Conservative management of placenta increta with selective arterial embolization preserves future fertility and results in a favorable outcome in subsequent pregnancies. Fertil. Steril. 2006, 86, 1514.e3–1514.e7. [Google Scholar] [CrossRef]
- Kloka, J.A.; Friedrichson, B.; Jasny, T.; Old, O.; Piekarski, F.; Zacharowski, K.; Neef, V. Anemia, red blood cell transfusion and administration of blood products in obstetrics: A nationwide analysis of more than 6 million cases from 2011–2020. Blood Transfus. 2023, 22, 37–45. [Google Scholar]
- Wiesenack, C.; Meybohm, P.; Neef, V.; Kranke, P. Current concepts in preoperative anemia management in obstetrics. Curr. Opin. Anaesthesiol. 2023, 36, 255–262. [Google Scholar] [CrossRef]
- Milman, N. Postpartum anemia I: Definition, prevalence, causes, and consequences. Ann. Hematol. 2011, 90, 1247–1253. [Google Scholar] [CrossRef]
- Muñoz, M.; Peña-Rosas, J.P.; Robinson, S.; Milman, N.; Holzgreve, W.; Breymann, C.; Goffinet, F.; Nizard, J.; Christory, F.; Samama, C.M.; et al. Patient blood management in obstetrics: Management of anaemia and haematinic deficiencies in pregnancy and in the post-partum period: NATA consensus statement. Transfus. Med. 2018, 28, 22–39. [Google Scholar] [CrossRef]
- NICE. Antenatal Care. 2021. Available online: https://www.nice.org.uk/guidance/ng201/resources/antenatal-care-pdf-66143709695941 (accessed on 8 February 2024).
- Klein, A.A.; Bailey, C.R.; Charlton, A.J.; Evans, E.; Guckian-Fisher, M.; McCrossan, R.; Nimmo, A.F.; Payne, S.; Shreeve, K.; Smith, J.; et al. Association of Anaesthetists guidelines: Cell salvage for peri-operative blood conservation 2018. Anaesthesia 2018, 73, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, M.; Stensballe, J.; Ducloy-Bouthors, A.S.; Bonnet, M.P.; De Robertis, E.; Fornet, I.; Goffinet, F.; Hofer, S.; Holzgreve, W.; Manrique, S.; et al. Patient blood management in obstetrics: Prevention and treatment of postpartum haemorrhage. A NATA consensus statement. Blood Transfus. Trasfus. Sangue 2019, 17, 112–136. [Google Scholar]
- Pacheco, L.D.; Clifton, R.G.; Saade, G.R.; Weiner, S.J.; Parry, S.; Thorp, J.M., Jr.; Longo, M.; Salazar, A.; Dalton, W.; Tita, A.T.N.; et al. Tranexamic Acid to Prevent Obstetrical Hemorrhage after Cesarean Delivery. N. Engl. J. Med. 2023, 388, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Neef, V.; Friedrichson, B.; Jasny, T.; Old, O.; Raimann, F.J.; Choorapoikayil, S.; Steinbicker, A.U.; Meybohm, P.; Zacharowski, K.; Kloka, J.A. Use of cell salvage in obstetrics in Germany: Analysis of national database of 305 610 cases with peripartum haemorrhage. Br. J. Anaesth. 2024; ahead of print. [Google Scholar] [CrossRef]
- Yildiz, K.; Dogru, K.; Dalgic, H.; Serin, I.S.; Sezer, Z.; Madenoglu, H.; Boyaci, A. Inhibitory effects of desflurane and sevoflurane on oxytocin-induced contractions of isolated pregnant human myometrium. Acta Anaesthesiol. Scand. 2005, 49, 1355–1359. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic n (%) | |
|---|---|
| Age (years) | 35 ± 4 # |
| BMI (kg/m2) | 28 ± 7 # |
| ASA score | II: 12 (70.6%) III: 5 (29.4%) |
| Gravity | 2.8 (0–7) * |
| Parity | 2.0 (0–5) * |
| Prior caesarean deliveries | 1.3 (0–3) * |
| Singelton | 17 (100%) |
| Placenta n (%) | |
| Bladder invasion | 9 (52.9%) |
| Prenatal imaging diagnosis Placenta accreta Placenta increta Placenta percreta | 0 (0%) 1 (5.9%) 16 (94.1%) |
| Concomitant placenta previa | 11 (64.7%) |
| Comorbidities n (%) | |
| Pre-eclampsia/Eclampsia | 0 (0%) |
| HELLP | 0 (0%) |
| Gestational diabetes | 3 (17.6%) |
| Gestational hypertension | 0 (0%) |
| Thrombocytopenia | 2 (11.7%) |
| A. Primary Procedure (n = 17) | B. Secondary Procedure (n = 16) | C. Ward (n = 17) | D. Total (n = 17) | p-Value | |
|---|---|---|---|---|---|
| RBC Units * | 0.0 (0.0–0.0) | 2.0 (0.0–5.5) | 0.0 (0.0–3.0) | 4.0 (0.5–7.0) | A. vs. B.: p = 0.038 |
| Transfusion rate n (%) | 2 (11.8%) | 10 (62.5%) | 8 (47.1%) | 13 (76.5%) | A. vs. D.: p = 0.002 |
| FFP Units * | 0.0 (0.0–0.0) | 0.0 (0.0–4.0) | 0.0 (0.0–0.0) | 0.0 (0.0–4.5) | |
| Transfusion rate n (%) | 0 (0%) | 6 (37.5%) | 1 (5.9%) | 6 (35.3%) | |
| Platelets Units * | 0 (0–0) | 0 (0–1.0) | 0 (0–0) | 0 (0–2.5) | |
| Transfusion rate n (%) | 0 (0%) | 5 (31.3%) | 2 (11.8%) | 7 (41.2%) | |
| Fibrinogen (2 g) * | 0.0 (0–0) | 1.0 (0–4.0) | 0 (0–0) | 2 (0–4.0) | A. vs. B.: p = 0.024 |
| Administration n (%) | 1 (5.9%) | 8 (50.0%) | 3 (17.6%) | 10 (58.8%) | A. vs. D.: p = 0.003 |
| PCC (Units) * | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0 (0–0) | |
| Administration n (%) | 0 (0%) | 3 (18.8%) | 0 (0%) | 3 (17.6%) | |
| TXA [mg] * | 0 (0–500.0) | 1000 (0–2000.0) | n.a. | 1000 (0–2000) | A. vs. D.: p = 0.010 |
| Administration n (%) | 4 (23.5%) | 10 (62.5%) | n.a. | 11 (64.7%) | |
| Cell Salvage n(%) | 0 (0%) | 3 (18.8%) | 0 (0%) | 3 (18.8%) | |
| Blood Loss (mL) * | 300 (200–600) | 3600 (450–5500) | n.a. | 1500 (600–4500) | A. vs. B.: p = 0.008 A. vs. D.: p = 0.006 |
| Anesthesiological Procedure | Primary Procedure (n = 17) | Secondary Procedure (n = 16) |
|---|---|---|
| Epidural | 13 (76.5%) | 4 (25.0%) |
| Spinal | 2 (11.8%) | 0 (0%) |
| General anesthesia | 2 (11.8%) | 12 (75.0%) |
| Arterial line | 10 (58.8%) | 10 (62.5%) |
| Central venous line | 2 (11.8%) | 9 (56.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neef, V.; Flinspach, A.N.; Eichler, K.; Woebbecke, T.R.; Noone, S.; Kloka, J.A.; Jennewein, L.; Louwen, F.; Zacharowski, K.; Raimann, F.J. Management and Outcome of Women with Placenta Accreta Spectrum and Treatment with Uterine Artery Embolization. J. Clin. Med. 2024, 13, 1062. https://doi.org/10.3390/jcm13041062
Neef V, Flinspach AN, Eichler K, Woebbecke TR, Noone S, Kloka JA, Jennewein L, Louwen F, Zacharowski K, Raimann FJ. Management and Outcome of Women with Placenta Accreta Spectrum and Treatment with Uterine Artery Embolization. Journal of Clinical Medicine. 2024; 13(4):1062. https://doi.org/10.3390/jcm13041062
Chicago/Turabian StyleNeef, Vanessa, Armin N. Flinspach, Katrin Eichler, Tirza R. Woebbecke, Stephanie Noone, Jan A. Kloka, Lukas Jennewein, Frank Louwen, Kai Zacharowski, and Florian J. Raimann. 2024. "Management and Outcome of Women with Placenta Accreta Spectrum and Treatment with Uterine Artery Embolization" Journal of Clinical Medicine 13, no. 4: 1062. https://doi.org/10.3390/jcm13041062
APA StyleNeef, V., Flinspach, A. N., Eichler, K., Woebbecke, T. R., Noone, S., Kloka, J. A., Jennewein, L., Louwen, F., Zacharowski, K., & Raimann, F. J. (2024). Management and Outcome of Women with Placenta Accreta Spectrum and Treatment with Uterine Artery Embolization. Journal of Clinical Medicine, 13(4), 1062. https://doi.org/10.3390/jcm13041062