
Mitigating Psychological Problems Associated with the 2023 Wildfires in Alberta and Nova Scotia: Six-Week Outcomes from the Text4Hope Program
 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Institutional Review Board Approval
2.3. Study Intervention
“No matter what setbacks you’ve faced or challenges that lie ahead, you can succeed if you have inner strength and stay focused. Have faith in yourself and success will be yours no matter what problems the wildfire throws at you.”
“There are two days in the week we should not worry about, yesterday and tomorrow. That leaves today, live for today. Thinking of the past or the future can be overwhelming for anyone facing a challenging situation or crisis.”
2.4. Data Collection
2.5. Outcome Measures
2.6. Hypotheses
2.7. Sample Size Considerations
2.8. Statistical Analysis
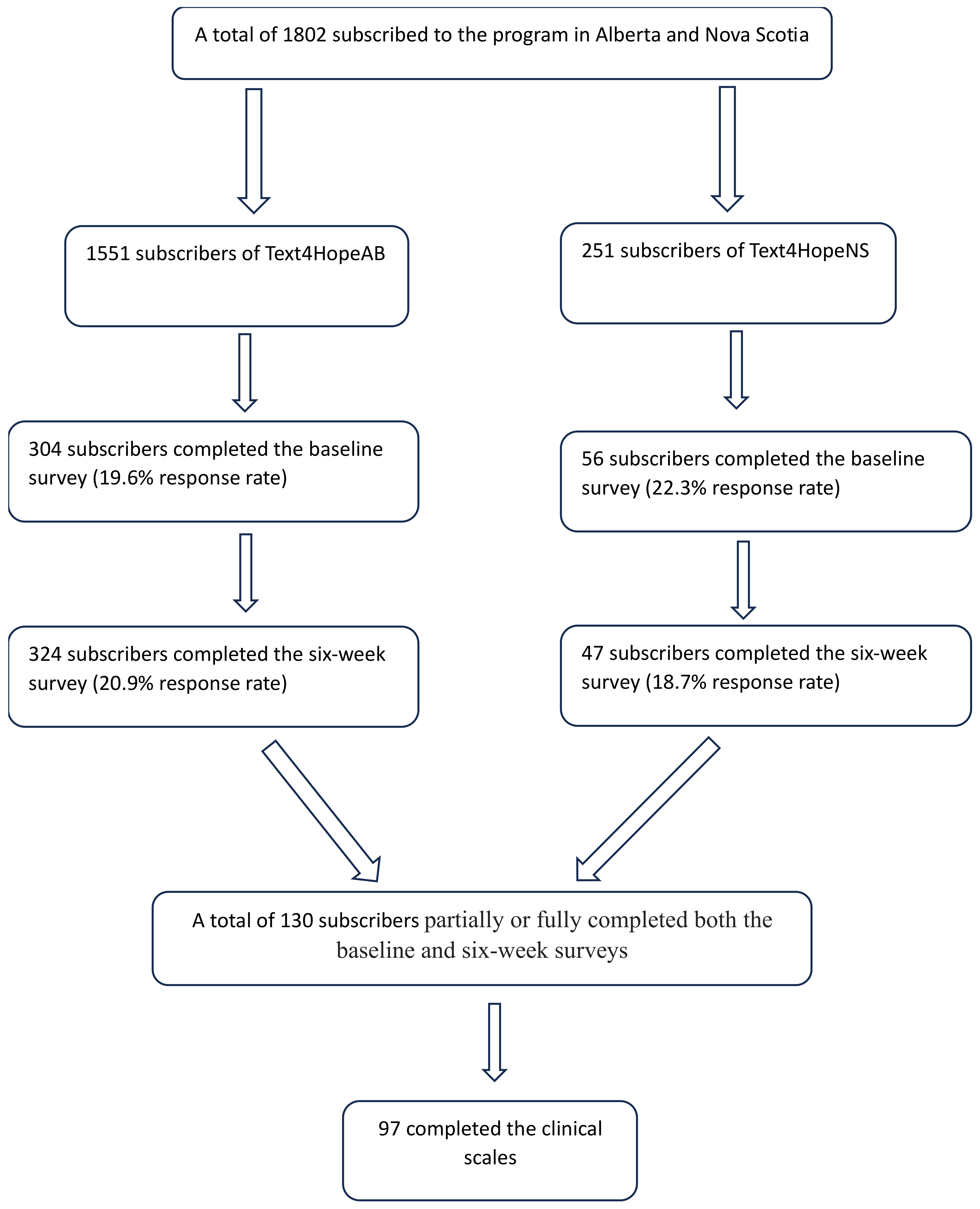
3. Results
3.1. Longitudinal Study Results
3.2. Naturalistic Controlled Study Results
4. Discussion
5. Limitations
6. Conclusions and Implications for Policy and Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Distribution of Demographic Characteristics of Study Participants
| Variable | Province | Total n = 424 | |
| Alberta n (%) n = 358 | Nova Scotia n (%) n = 66 | ||
| Age (years) | |||
| ≤30 | 46 (12.8) | 7 (10.6) | 53 (12.5) |
| 31–50 | 137 (38.3) | 31 (47) | 168 (39.6) |
| 51–65 | 133 (37.2) | 22 (33.3) | 155 (36.6) |
| >65 | 42 (11.7) | 6 (9.1) | 48 (11.3) |
| Gender | |||
| Male | 47 (13.1) | 12 (18.2) | 59 (13.9) |
| Female | 304 (84.9) | 52 (78.8) | 356 (84.0) |
| Other | 7 (2.0) | 2 (3.0) | 9 (2.1) |
| Ethnicity | |||
| Caucasian | 299 (83.5) | 57 (86.4) | 356 (84.0) |
| Indigenous | 21 (5.9) | 0 (0.0) | 21 (5.0) |
| Asian | 20 (5.6) | 0 (0.0) | 20 (4.7) |
| Black/Hispanic | 8 (2.2) | 5 (7.6) | 13 (3.1) |
| Other | 10 (2.8) | 4 (6.1) | 14 (3.3) |
| Education | |||
| Elementary school | 5 (1.4) | 2 (3.0) | 7 (1.7) |
| High school | 60 (16.8) | 7 (10.6) | 67 (15.8) |
| Post-secondary (college, trade school, university, or postgraduate study) | 293 (81.8) | 57 (86.4) | 350 (82.5) |
| Relationship status | |||
| Married/Partnered/Common-Law/Cohabiting | 186 (52.1) | 42 (63.6) | 228 (53.9) |
| Single | 94 (26.3) | 17 (25.8) | 111 (26.2) |
| Separated or divorced | 56 (15.7) | 3 (4.5) | 59 (13.9) |
| Widowed | 14 (3.9) | 2 (3.0) | 16 (3.8) |
| Other | 7 (2.0) | 2 (3.0) | 9 (2.1) |
| Employment status | |||
| Student | 12 (3.4) | 5 (7.6) | 17 (4.0) |
| Employed | 224 (62.6) | 43 (65.2) | 267 (63.0) |
| Unemployed | 59 (16.5) | 9 (13.6) | 68 (16.0) |
| Retired | 63 (17.6) | 9 (13.6) | 72 (17.0) |
| Housing status | |||
| Own home | 230 (64.2) | 44 (66.7) | 274 (64.6) |
| Renting accommodation | 85 (23.7) | 17 (25.8) | 102 (24.1) |
| Live with family and friends | 43 (12.0) | 5 (7.6) | 48 (11.3) |
| Other—categories are not included in the survey options. | |||
References
- To, P.; Eboreime, E.; Agyapong, V.I.O. The Impact of Wildfires on Mental Health: A Scoping Review. Behav. Sci. 2021, 11, 126. [Google Scholar] [CrossRef]
- Ibrahim, D. Canadians’ Experiences with Emergencies and Disasters. 2014. Available online: https://www150.statcan.gc.ca/n1/pub/85-002-x/2016001/article/14469-eng.htm (accessed on 2 January 2024).
- Parisien, M.A.; Barber, Q.E.; Flannigan, M.D.; Jain, P. Broadleaf tree phenology and springtime wildfire occurrence in boreal Canada. Glob. Chang. Biol. 2023, 29, 6106–6119. [Google Scholar] [CrossRef]
- Meilleur, D. Alberta Declares State of Emergency as Wildfires Rage. Available online: https://globalnews.ca/news/9679627/alberta-premier-adresses-wildfire-state-of-emergency/ (accessed on 11 August 2023).
- Press, A. Nova Scotia Wildfires Grow, Prompt Air Quality Warnings as Far South as Virginia. Available online: https://apnews.com/article/canada-wildfires-halifax-firefighters-us-south-africa-20f340036282d892aaa5528f1e48e618 (accessed on 11 August 2023).
- Eisenman, D.P.; Galway, L.P. The mental health and well-being effects of wildfire smoke: A scoping review. BMC Public Health 2022, 22, 2274. [Google Scholar] [CrossRef]
- Brown, M.R.G.; Pazderka, H.; Agyapong, V.I.O.; Greenshaw, A.J.; Cribben, I.; Brett-MacLean, P.; Drolet, J.; McDonald-Harker, C.B.; Omeje, J.; Lee, B.; et al. Mental Health Symptoms Unexpectedly Increased in Students Aged 11–19 Years During the 3.5 Years After the 2016 Fort McMurray Wildfire: Findings from 9376 Survey Responses. Front. Psychiatry 2021, 12, 676256. [Google Scholar] [CrossRef]
- Brown, M.R.G.; Agyapong, V.; Greenshaw, A.J.; Cribben, I.; Brett-MacLean, P.; Drolet, J.; McDonald-Harker, C.; Omeje, J.; Mankowsi, M.; Noble, S.; et al. Significant PTSD and Other Mental Health Effects Present 18 Months After the Fort Mcmurray Wildfire: Findings from 3,070 Grades 7–12 Students. Front. Psychiatry 2019, 10, 623. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Ritchie, A.; Brown, M.R.G.; Noble, S.; Mankowsi, M.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; et al. Long-Term Mental Health Effects of a Devastating Wildfire Are Amplified by Socio-Demographic and Clinical Antecedents in Elementary and High School Staff. Front. Psychiatry 2020, 11, 448. [Google Scholar] [CrossRef]
- Bryant, R.A.; Gibbs, L.; Gallagher, H.C.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; Sinnott, V.; Ireton, G.; et al. Longitudinal study of changing psychological outcomes following the Victorian Black Saturday bushfires. Aust. N. Z. J. Psychiatry 2018, 52, 542–551. [Google Scholar] [CrossRef]
- Agyapong, B.; Eboreime, E.; Shalaby, R.; Pazderka, H.; Obuobi-Donkor, G.; Adu, M.K.; Mao, W.; Oluwasina, F.; Owusu, E.; Greenshaw, A.J.; et al. Mental Health Impacts of Wildfire, Flooding and COVID-19 on Fort McMurray School Board Staff and Other Employees: A Comparative Study. Int. J. Environ. Res. Public Health 2021, 19, 435. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Hrabok, M.; Juhas, M.; Omeje, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Moosavi, S.; Brown, M.; et al. Prevalence Rates and Predictors of Generalized Anxiety Disorder Symptoms in Residents of Fort McMurray Six Months After a Wildfire. Front. Psychiatry 2018, 9, 345. [Google Scholar] [CrossRef]
- North, C.S.; Pfefferbaum, B. Mental health response to community disasters: A systematic review. JAMA 2013, 310, 507–518. [Google Scholar] [CrossRef]
- Obuobi-Donkor, G.; Shalaby, R.; Vuong, W.; Agyapong, B.; Hrabok, M.; Gusnowski, A.; Surood, S.; Greenshaw, A.J.; Agyapong, V.I. Effects of Text4Hope-Addiction Support Program on Cravings and Mental Health Symptoms: Results of a Longitudinal Cross-sectional Study. JMIR Form. Res. 2023, 7, e40440. [Google Scholar] [CrossRef]
- Obuobi-Donkor, G.; Shalaby, R.; Eboreime, E.; Agyapong, B.; Phung, N.; Eyben, S.; Wells, K.; Hilario, C.; Dias, R.D.L.; Jones, C.; et al. Text4PTSI: A Promising Supportive Text Messaging Program to Mitigate Psychological Symptoms in Public Safety Personnel. Int. J. Environ. Res. Public Health 2023, 20, 4215. [Google Scholar] [CrossRef]
- Obuobi-Donkor, G.; Eboreime, E.; Shalaby, R.; Agyapong, B.; Phung, N.; Eyben, S.; Wells, K.; Dias, R.D.L.; Hilario, C.; Jones, C.; et al. User Satisfaction with a Daily Supportive Text Message Program (Text4PTSI) for Public Safety Personnel: Longitudinal Cross-Sectional Study. JMIR Form. Res. 2023, 7, e46431. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Hrabok, M.; Vuong, W.; Shalaby, R.; Noble, J.M.; Gusnowski, A.; Mrklas, K.J.; Li, D.; Urichuk, L.; Snaterse, M.; et al. Changes in Stress, Anxiety, and Depression Levels of Subscribers to a Daily Supportive Text Message Program (Text4Hope) During the COVID-19 Pandemic: Cross-Sectional Survey Study. JMIR Ment. Health 2020, 7, e22423. [Google Scholar] [CrossRef]
- Owusu, E.; Shalaby, R.; Eboreime, E.; Nkire, N.; Lawal, M.A.; Agyapong, B.; Pazderka, H.; Obuobi-Donkor, G.; Adu, M.K.; Mao, W.; et al. Prevalence and Determinants of Generalized Anxiety Disorder Symptoms in Residents of Fort McMurray 12 Months Following the 2020 Flooding. Front. Psychiatry 2022, 13, 844907. [Google Scholar] [CrossRef]
- Cox, K.L.; Allida, S.M.; Hackett, M.L. Text messages to reduce depressive symptoms: Do they work and what makes them effective? A systematic review. Health Educ. J. 2021, 80, 253–271. [Google Scholar] [CrossRef]
- Agyapong, V.I.O. Coronavirus Disease 2019 Pandemic: Health System and Community Response to a Text Message (Text4Hope) Program Supporting Mental Health in Alberta. Disaster Med. Public Health Prep. 2020, 14, e5–e6. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Hrabok, M.; Shalaby, R.; Mrklas, K.; Vuong, W.; Gusnowski, A.; Surood, S.; Greenshaw, A.J.; Nkire, N. Closing the COVID-19 Psychological Treatment Gap for Cancer Patients in Alberta: Protocol for the Implementation and Evaluation of Text4Hope-Cancer Care. JMIR Res. Protoc. 2020, 9, e20240. [Google Scholar] [CrossRef]
- Hong, J.S.; Hyun, S.Y.; Lee, J.H.; Sim, M. Mental health effects of the Gangwon wildfires. BMC Public Health 2022, 22, 1183. [Google Scholar] [CrossRef]
- Raeside, R.; Spielman, K.; Maguire, S.; Mihrshahi, S.; Steinbeck, K.; Kang, M.; Laranjo, L.; Hyun, K.; Redfern, J.; Partridge, S.R. A healthy lifestyle text message intervention for adolescents: Protocol for the Health4Me randomized controlled trial. BMC Public Health 2022, 22, 1805. [Google Scholar] [CrossRef]
- Agyapong, B.; Shalaby, R.; Vuong, W.; Gusnowski, A.; Surood, S.; Greenshaw, A.J.; Wei, Y.; Agyapong, V.I.O. Text4Hope Effectiveness in Reducing Psychological Symptoms among Young Adults in Canada: Longitudinal and Naturalistic Controlled Program Evaluation. J. Clin. Med. 2023, 12, 1942. [Google Scholar] [CrossRef]
- Mbao, M.; Collins-Pisano, C.; Fortuna, K. Older Adult Peer Support Specialists’ Age-Related Contributions to an Integrated Medical and Psychiatric Self-Management Intervention: Qualitative Study of Text Message Exchanges. JMIR Form. Res. 2021, 5, e22950. [Google Scholar] [CrossRef]
- Agyapong, V.I.; Ahern, S.; McLoughlin, D.M.; Farren, C.K. Supportive text messaging for depression and comorbid alcohol use disorder: Single-blind randomised trial. J. Affect. Disord. 2012, 141, 168–176. [Google Scholar] [CrossRef]
- Celano, C.M.; Massey, C.; Long, J.; Kim, S.; Velasquez, O.; Healy, B.C.; Wexler, D.J.; Madva, E.N.; Huffman, J.C. An Adaptive, Algorithm-based Text Message Intervention to Promote Health Behavior Adherence in Type 2 Diabetes: Treatment Development and Proof-of-Concept Trial. J. Diabetes Sci. Technol. 2023, 17, 364–373. [Google Scholar] [CrossRef]
- Craig Rushing, S.; Kelley, A.; Bull, S.; Stephens, D.; Wrobel, J.; Silvasstar, J.; Peterson, R.; Begay, C.; Ghost Dog, T.; McCray, C.; et al. Efficacy of an mHealth Intervention (BRAVE) to Promote Mental Wellness for American Indian and Alaska Native Teenagers and Young Adults: Randomized Controlled Trial. JMIR Ment. Health 2021, 8, e26158. [Google Scholar] [CrossRef]
- Statistics Canada. Population and Dwelling Counts: Canada, Provinces and Territories; Statistics Canada: Ottawa, ON, Canada, 2022. [Google Scholar]
- Authority, N.S.H. HopeNS. Available online: https://mha.nshealth.ca/en/services/hopens (accessed on 16 November 2023).
- Alberta, G.O. Wildfire Evacuee Information: Mental Health and Addiction Support; Ministry of Mental Health and Addiction: Edmonton, AB, Canada, 2023.
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. (1960) 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. In Annual Convention of the International Society for Traumatic Stress Studies; San Antonio, TX, USA; 1993; Available online: https://www.researchgate.net/profile/Frank-Weathers/publication/291448760_The_PTSD_Checklist_PCL_Reliability_validity_and_diagnostic_utility/links/57c7121208ae9d64047e9569/The-PTSD-Checklist-PCL-Reliability-validity-and-diagnostic-utility (accessed on 27 December 2023).
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- World Health Organization. Wellbeing Measures in Primary Health Care/The DepCare Project: Report on a WHO Meeting: Stockholm, Sweden, 12–13 February 1998; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 1998. [Google Scholar]
- Dhira, T.A.; Rahman, M.A.; Sarker, A.R.; Mehareen, J. Validity and reliability of the Generalized Anxiety Disorder-7 (GAD-7) among university students of Bangladesh. PLoS ONE 2021, 16, e0261590. [Google Scholar] [CrossRef]
- Bovin, M.J.; Marx, B.P.; Weathers, F.W.; Gallagher, M.W.; Rodriguez, P.; Schnurr, P.P.; Keane, T.M. Psychometric properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (PCL-5) in veterans. Psychol. Assess. 2016, 28, 1379–1391. [Google Scholar] [CrossRef]
- Smith, B.W.; Epstein, E.M.; Ortiz, J.A.; Christopher, P.J.; Tooley, E.M. The foundations of resilience: What are the critical resources for bouncing back from stress? In Resilience in Children, Adolescents, and Adults; Springer: Berlin/Heidelberg, Germany, 2013; pp. 167–187. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Juhás, M.; Ohinmaa, A.; Omeje, J.; Mrklas, K.; Suen, V.Y.M.; Dursun, S.M.; Greenshaw, A.J. Randomized controlled pilot trial of supportive text messages for patients with depression. BMC Psychiatry 2017, 17, 286. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Juhás, M.; Mrklas, K.; Hrabok, M.; Omeje, J.; Gladue, I.; Kozak, J.; Leslie, M.; Chue, P.; Greenshaw, A.J. Randomized controlled pilot trial of supportive text messaging for alcohol use disorder patients. J. Subst. Abuse Treat. 2018, 94, 74–80. [Google Scholar] [CrossRef]
- Dias, R.D.L.; Shalaby, R.; Agyapong, B.; Vuong, W.; Gusnowski, A.; Surood, S.; Greenshaw, A.J.; Agyapong, V.I. The effectiveness of CBT-based daily supportive text messages in improving female mental health during COVID-19 pandemic: Results from the Text4Hope program. Front. Glob. Women’s Health 2023, 4, 1182267. [Google Scholar] [CrossRef]
- Shalaby, R.; Agyapong, B.; Vuong, W.; Hrabok, M.; Gusnowski, A.; Surood, S.; Greenshaw, A.J.; Agyapong, V.I.O. Naturalistic randomized controlled trial demonstrating effectiveness of Text4Hope in supporting male population mental health during the COVID-19 pandemic. Front. Public Health 2022, 10, 1002288. [Google Scholar] [CrossRef]
- Dhand, N.; Khatkar, M. Sample Size Calculator for Comparing Paired Differences. 2023. Available online: https://statulator.com/SampleSize/ss2PM.html (accessed on 21 November 2023).
- Dhand, N.; Khatkar, M. Sample Size Calculator for Comparing Two Independent Means. 2023. Available online: https://statulator.com/SampleSize/ss2M.html (accessed on 21 November 2023).
- IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. In Google Search; IBM Corp: Armonk, NY, USA, 2021. [Google Scholar]
- Colizzi, M.; Lasalvia, A.; Ruggeri, M. Prevention and early intervention in youth mental health: Is it time for a multidisciplinary and trans-diagnostic model for care? Int. J. Ment. Health Syst. 2020, 14, 23. [Google Scholar] [CrossRef]
- Dennis, M.; Scott, C.K. Managing addiction as a chronic condition. Addict. Sci. Clin. Pract. 2007, 4, 45–55. [Google Scholar] [CrossRef]
- Sugg, M.M.; Runkle, J.D.; Hajnos, S.N.; Green, S.; Michael, K.D. Understanding the concurrent risk of mental health and dangerous wildfire events in the COVID-19 pandemic. Sci. Total Environ. 2022, 806 Pt 1, 150391. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Mrklas, K.; Juhás, M.; Omeje, J.; Ohinmaa, A.; Dursun, S.M.; Greenshaw, A.J. Cross-sectional survey evaluating Text4Mood: Mobile health program to reduce psychological treatment gap in mental healthcare in Alberta through daily supportive text messages. BMC Psychiatry 2016, 16, 378. [Google Scholar] [CrossRef]
- Shalaby, R.; Vuong, W.; Hrabok, M.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; Cao, B.; Li, X.M.; et al. Gender Differences in Satisfaction with a Text Messaging Program (Text4Hope) and Anticipated Receptivity to Technology-Based Health Support During the COVID-19 Pandemic: Cross-sectional Survey Study. JMIR Mhealth Uhealth 2021, 9, e24184. [Google Scholar] [CrossRef]
- Agyapong, V.; Mrklas, K.; Juhas, M.; Omeje, J.; Ohinmaa, A.; Dursun, S.; Greenshaw, A. Mobile health program to reduce psychological treatment gap in mental healthcare in Alberta through daily supportive text messages–Cross-sectional survey evaluating Text4Mood. Eur. Psychiatry 2017, 41, S139. [Google Scholar] [CrossRef]
- Abroms, L.C.; Ahuja, M.; Kodl, Y.; Thaweethai, L.; Sims, J.; Winickoff, J.P.; Windsor, R.A. Text2Quit: Results from a pilot test of a personalized, interactive mobile health smoking cessation program. J. Health Commun. 2012, 17 (Suppl. S1), 44–53. [Google Scholar] [CrossRef]
- Van Wyk, J.; Gibson, K. An Analysis of Young Clients’ Communications About Their Suicidality on a Text Message Helpline: “I’m Scared of What I Might Do to Myself”. Front. Psychiatry 2022, 13, 925830. [Google Scholar] [CrossRef]
- Kreuze, E.; Jenkins, C.; Gregoski, M.; York, J.; Mueller, M.; Lamis, D.A.; Ruggiero, K.J. Technology-enhanced suicide prevention interventions: A systematic review. J. Telemed. Telecare 2017, 23, 605–617. [Google Scholar] [CrossRef]
- Rizvi, S.L.; Fitzpatrick, S. Changes in suicide and non-suicidal self-injury ideation and the moderating role of specific emotions over the course of dialectical behavior therapy. Suicide Life Threat. Behav. 2021, 51, 429–445. [Google Scholar] [CrossRef]
- Czyz, E.K.; Arango, A.; Healy, N.; King, C.A.; Walton, M. Augmenting Safety Planning with Text Messaging Support for Adolescents at Elevated Suicide Risk: Development and Acceptability Study. JMIR Ment. Health 2020, 7, e17345. [Google Scholar] [CrossRef]
- Comtois, K.A.; Kerbrat, A.H.; DeCou, C.R.; Atkins, D.C.; Majeres, J.J.; Baker, J.C.; Ries, R.K. Effect of Augmenting Standard Care for Military Personnel with Brief Caring Text Messages for Suicide Prevention: A Randomized Clinical Trial. JAMA Psychiatry 2019, 76, 474–483. [Google Scholar] [CrossRef]
- Berrouiguet, S.; Larsen, M.E.; Mesmeur, C.; Gravey, M.; Billot, R.; Walter, M.; Lemey, C.; Lenca, P. Toward mHealth Brief Contact Interventions in Suicide Prevention: Case Series from the Suicide Intervention Assisted by Messages (SIAM) Randomized Controlled Trial. JMIR Mhealth Uhealth 2018, 6, e8. [Google Scholar] [CrossRef]
- McCall, W.V.; Ribbens, L.T.; Looney, S.W. Relationships among insomnia, executive function, and suicidal ideation in depressed outpatients: A mediation analysis. Scand. J. Psychol. 2023, 64, 105–112. [Google Scholar] [CrossRef]
- Kiosses, D.N.; Gross, J.J.; Banerjee, S.; Duberstein, P.R.; Putrino, D.; Alexopoulos, G.S. Negative Emotions and Suicidal Ideation during Psychosocial Treatments in Older Adults with Major Depression and Cognitive Impairment. Am. J. Geriatr. Psychiatry 2017, 25, 620–629. [Google Scholar] [CrossRef]
- Surgenor, P.W. Promoting recovery from suicidal ideation through the development of protective factors. Couns. Psychother. Res. 2015, 15, 207–216. [Google Scholar] [CrossRef]
- Pisani, A.R.; Gould, M.S.; Gallo, C.; Ertefaie, A.; Kelberman, C.; Harrington, D.; Weller, D.; Green, S. Individuals who text crisis text line: Key characteristics and opportunities for suicide prevention. Suicide Life Threat. Behav. 2022, 52, 567–582. [Google Scholar] [CrossRef]
- Abdullah, H.; Lynch, S.; Aftab, S.; Shahar, S.; Klepacz, L.; Cristofano, P.; Rahmat, S.; Save-Mundra, J.; Dornbush, R.; Lerman, A.; et al. Characteristics of Calls to a COVID-19 Mental Health Hotline in the First Wave of the Pandemic in New York. Community Ment. Health J. 2021, 57, 1252–1254. [Google Scholar] [CrossRef]
- Isaac, F.; Toukhsati, S.R.; Di Benedetto, M.; Kennedy, G.A. A Systematic Review of the Impact of Wildfires on Sleep Disturbances. Int. J. Environ. Res. Public Health 2021, 18, 10152. [Google Scholar] [CrossRef]
- Moosavi, S.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Chue, P.; Greenshaw, A.J.; Silverstone, P.H.; Li, X.M.; Agyapong, V.I.O. Mental Health Effects in Primary Care Patients 18 Months After a Major Wildfire in Fort McMurray: Risk Increased by Social Demographic Issues, Clinical Antecedents, and Degree of Fire Exposure. Front. Psychiatry 2019, 10, 683. [Google Scholar] [CrossRef]
- Agyapong, V.I.O.; Hrabok, M.; Shalaby, R.; Vuong, W.; Noble, J.M.; Gusnowski, A.; Mrklas, K.; Li, D.; Urichuck, L.; Snaterse, M.; et al. Text4Hope: Receiving Daily Supportive Text Messages for 3 Months During the COVID-19 Pandemic Reduces Stress, Anxiety, and Depression. Disaster Med. Public Health Prep. 2021, 16, 1326–1330. [Google Scholar] [CrossRef]
- Bidargaddi, N.; Schrader, G.; Klasnja, P.; Licinio, J.; Murphy, S. Designing m-Health interventions for precision mental health support. Transl. Psychiatry 2020, 10, 222. [Google Scholar] [CrossRef]
- Braithwaite, S.R.; Fincham, F.D. A randomized clinical trial of a computer based preventive intervention: Replication and extension of ePREP. J. Fam. Psychol. 2009, 23, 32–38. [Google Scholar] [CrossRef]
- Brown, M.R.G.; Agyapong, V.; Greenshaw, A.J.; Cribben, I.; Brett-MacLean, P.; Drolet, J.; McDonald-Harker, C.; Omeje, J.; Mankowsi, M.; Noble, S.; et al. After the Fort McMurray wildfire there are significant increases in mental health symptoms in grade 7-12 students compared to controls. BMC Psychiatry 2019, 19, 18. [Google Scholar] [CrossRef]
- Dudas, R.; Malouf, R.; McCleery, J.; Dening, T. Antidepressants for treating depression in dementia. Cochrane Database Syst. Rev. 2018, 8, Cd003944. [Google Scholar] [CrossRef]
- Duffy, L.; Lewis, G.; Ades, A.; Araya, R.; Bone, J.; Brabyn, S.; Button, K.; Churchill, R.; Croudace, T.; Derrick, C.; et al. Programme Grants for Applied Research. In Antidepressant Treatment with Sertraline for Adults with Depressive Symptoms in Primary Care: The PANDA Research Programme Including RCT; NIHR Journals Library; National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park: Southampton, UK, 2019. [Google Scholar] [CrossRef]
- Watanabe, N.; Omori, I.M.; Nakagawa, A.; Cipriani, A.; Barbui, C.; Churchill, R.; Furukawa, T.A. Mirtazapine versus other antidepressive agents for depression. Cochrane Database Syst. Rev. 2011, 12, Cd006528. [Google Scholar] [CrossRef]
- Heinz, A.J.; Wiltsey-Stirman, S.; Jaworski, B.K.; Sharin, T.; Rhodes, L.; Steinmetz, S.; Taylor, K.; Gorman, B.; Mason, D.; Marikos, S.; et al. Feasibility and preliminary efficacy of a public mobile app to reduce symptoms of postdisaster distress in adolescent wildfire survivors: Sonoma rises. Psychol. Serv. 2021, 19, 67. [Google Scholar] [CrossRef]
- Nsagha, D.S.; Siysi, V.V.; Ekobo, S.; Egbe, T.O.; Kibu, O.D. One-Way and Two-Way Mobile Phone Text Messages for Treatment Adherence Among Patients with HIV: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e16127. [Google Scholar] [CrossRef]
- Spek, V.; Cuijpers, P.; Nyklícek, I.; Riper, H.; Keyzer, J.; Pop, V. Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: A meta-analysis. Psychol. Med. 2007, 37, 319–328. [Google Scholar] [CrossRef]
- Howell, A.N.; Rheingold, A.A.; Uhde, T.W.; Guille, C. Web-based CBT for the prevention of anxiety symptoms among medical and health science graduate students. Cogn. Behav. Ther. 2019, 48, 385–405. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Survey Completed | Chi2/Fisher’s Exact a/t-Test (df) | p-Value | |
|---|---|---|---|---|
| Both Baseline and Six-Week Surveys n (%) n = 97 * | Baseline Survey Only n (%) n = 263 | |||
| Province | ||||
| Alberta | 80 (82.5) | 224 (85.2) | 0.4 | 0.6 |
| Nova Scotia | 17 (17.5) | 39 (14.8) | ||
| Age (years) | ||||
| ≤30 | 7 (7.2) | 39 (14.9) | 23.7 | <0.001 |
| 31–50 | 24 (24.7) | 120 (45.8) | ||
| 51–65 | 50 (51.5) | 81 (30.9) | ||
| >65 | 16 (16.5) | 22 (8.4) | ||
| Gender | ||||
| Male | 14 (14.4) | 35 (13.4) | 0.6 | 0.8 |
| Female | 82 (84.5) | 221 (84.4) | ||
| Other | 1 (1.0) | 6 (2.3) | ||
| Ethnicity | ||||
| Caucasian | 86 (88.7) | 215 (82.1) | 2.3 a | 0.7 |
| Indigenous | 4 (4.1) | 16 (6.1) | ||
| Asian | 4 (4.1) | 12 (4.6) | ||
| Black/Hispanic | 1 (1) | 8 (3.1) | ||
| Other | 2 (2.1) | 11 (4.2) | ||
| Education | ||||
| Elementary school | 1 (1.0) | 6 (2.3) | 0.8 | 0.7 |
| High school | 14 (14.4) | 43 (16.4) | ||
| Post-secondary (college, trade school, university, or postgraduate study) | 82 (84.5) | 213 (81.3) | ||
| Relationship status | ||||
| Married/Partnered/Common-Law/Cohabiting | 47 (48.5) | 148 (56.7) | 6.4 a | 0.2 |
| Single | 24 (24.7) | 72 (27.6) | ||
| Separated or divorced | 17 (17.5) | 29 (11.1) | ||
| Widowed | 6 (6.2) | 7 (2.7) | ||
| Other | 3 (3.1) | 5 (1.9) | ||
| Employment status | ||||
| Student | 3 (3.1) | 12 (4.6) | 3.9 | 0.3 |
| Employed | 57 (58.8) | 168 (64.1) | ||
| Unemployed | 15 (15.5) | 45 (17.2) | ||
| Retired | 22 (22.7) | 37 (14.1) | ||
| Housing status | ||||
| Own home | 167 (63.7) | 1.2 | 0.6 | |
| Renting accommodation | 65 (24.8) | |||
| Live with family and friends | 30 (11.5) | |||
| BRS | Mean Score (SD) | |||
| n = 97 | n = 216 | |||
| 2.7 (0.9) | 2.8 (0.8) | −0.4 (311) | 0.7 | |
| WHO-5 Wellbeing Index | Mean Score (SD) | |||
| n = 97 | n = 213 | |||
| 9.6 (5.1) | 10.3 (5.2) | −1.1 (308) | 0.3 | |
| PHQ-9 | Mean Score (SD) | |||
| n = 96 | n = 203 | |||
| 11.3 (6.4) | 11.4 (6.6) | 0.2 (304) | 0.8 | |
| GAD-7 scale | Mean Score (SD) | |||
| n = 96 | n = 207 | |||
| 9.5 (5.5) | 9.6 (5.8) | −0.04 (301) | 0.9 | |
| PTSD PCL-C | Mean Score (SD) | |||
| n = 96 | n = 203 | |||
| 43.2 (16.2) | 41.3 (16.3) | 0.7 (297) | 0.4 | |
| Measure | n * | Mean Scores | Mean Difference (95% CI) | % Change from Baseline | p-Value | t-Test | Effect Size (Hedges’ g) | |
|---|---|---|---|---|---|---|---|---|
| Baseline Mean (SD) | 6-Week Mean (SD) | |||||||
| BRS total score | 97 | 2.7 (0.9) | 2.8 (0.8) | −0.85 (−0.20–0.03) | +3.7 | 0.158 | −1.42 | 0.12 |
| WHO-5 total score | 94 | 9.5 (5.1) | 11.6 (5.2) | −2.09 (−3.01 to −1.18) | +22.1 | 0.000 | −454 | 0.41 |
| PHQ-9 total score | 93 | 11.7 (6.5) | 10.3 (6.2) | 1.44 (0.48–2.4) | −12 | 0.004 | 2.97 | 0.22 |
| GAD-7 total score | 92 | 9.6 (5.4) | 8.2 (5.3) | 1.42 (0.53–2.32) | −14.6 | 0.002 | 3.15 | 0.26 |
| PCL-C total score | 90 | 43.6 (16.4) | 41.1 (16.3) | 2.52 (0.53–4.5) | −5.7 | 0.014 | 2.51 | 0.15 |
| Suicidal ideation or thoughts of self-harm | 93 | 0.29 (0.6) | 0.26 (0.5) | −0.03 (−0.75–0.14) | −10.3 | 0.55 | 0.59 | 0.05 |
| Variable | Control Group n = 52 | Intervention Group n = 174 | Total n = 226 | Chi2/Fisher’s Exact b | p-Value |
|---|---|---|---|---|---|
| Age (years) | |||||
| ≤30 | 10 (19.2) | 16 (9.2) | 26 (11.5) | 7.1 | 0.07 |
| 31–50 | 20 (38.5) | 52 (29.9) | 72 (31.9) | ||
| 51–65 | 17 (32.7) | 76 (43.7) | 93 (41.2) | ||
| >65 | 5 (9.6) | 30 (17.2) | 35 (15.5) | ||
| Gender | |||||
| Male | 10 (19.2) | 28 (16.1) | 38 (16.8) | 0.6 | 0.8 |
| Female | 41 (78.8) | 143 (82.2) | 184 (81.4) | ||
| Other | 1 (1.9) | 3 (1.7) | 4 (1.8) | ||
| Ethnicity | |||||
| Caucasian | 43 (82.7) | 150 (86.2) | 193 (85.4) | 1.9 b | 0.72 |
| Indigenous | 2 (3.8) | 6 (3.4) | 8 (3.5) | ||
| Asian | 4 (7.7) | 9 (4.0) | 13 (5.8) | ||
| Black/Hispanic | 3 (5.8) | 6 (3.4) | 9 (4.0) | ||
| Other | 0 (0.0) | 3 (1.7) | 3 (1.3) | ||
| Education | |||||
| Elementary school | 1 (1.9) | 1 (0.6) | 2 (0.9) | 2.2 b | 0.28 |
| High school | 11 (21.2) | 28 (16.1) | 39 (17.3) | ||
| Post-secondary (college, trade school, university, or postgraduate study) | 40 (76.9) | 145 (83.3) | 185 (81.9) | ||
| Relationship status | |||||
| Married/Partnered/Common-Law/Cohabiting | 28 (53.8) | 87 (50.0) | 115 (50.9) | 3.6 b | 0.49 |
| Single | 15 (28.8) | 42 (24.1) | 57 (25.2) | ||
| Separated or divorced | 6 (11.5) | 32 (18.4) | 38 (16.8) | ||
| Widowed | 1 (1.9) | 10 (5.7) | 11 (4.9) | ||
| Other | 2 (3.8) | 3 (1.7) | 5 (2.2) | ||
| Employment status | |||||
| Student | 3 (5.8) | 5 (2.9) | 8 (3.5) | 4.3 b | 0.22 |
| Employed | 29 (55.8) | 107 (61.5) | 136 (60.2) | ||
| Unemployed | 11 (21.2) | 21 (12.1) | 32 (14.2) | ||
| Retired | 9 (17.3) | 41 (23.6) | 50 (22.1) | ||
| Housing status | |||||
| Own home | 29 (55.8) | 116 (66.7) | 145 (64.2) | 2.2 | 0.34 |
| Renting accommodation | 16 (30.8) | 38 (21.8) | 54 (23.9) | ||
| Live with family and friends | 7 (13.5) | 20 (11.5) | 27 (11.9) |
| Measure | n | Mean Scores | n | Mean Difference between Groups (95% CI) | % Difference between Groups | p-Value | t-Test | Effect Size (Hedges’ g) | |
|---|---|---|---|---|---|---|---|---|---|
| Intervention Group (SD) | Control Group (SD) | ||||||||
| BRS total score | 327 | 17.3 (4.9) | 16.0 (5.1) | 50 | +1.3 | 0.08 | −1.75 | 0.26 | |
| (−2.7–0.16) | +8.1 | ||||||||
| WHO-5 total score | 315 | 11.9 (4.9) | 9.6 (5.4) | 49 | +2.38 | 0.002 | −3.07 | 0.46 | |
| (−3.9–−0.86) | +24.7 | ||||||||
| PHQ-9 total score | 321 | 9.2 (6.1) | 13.1 | 49 | −3.94 | <0.001 | 4.2 | 0.64 | |
| (6.3) | (2.09–5.78) | −30.1 | |||||||
| GAD-7 total score | 307 | 7.8 (5.5) | 11.1 (5.6) | 48 | −3.26 | <0.001 | 3.76 | 0.6 | |
| (1.55–4.96) | −29.4 | ||||||||
| PCL-C total score | 295 | 38.1 (16.1) | 46.2 (14.7) | 47 | −8.09 | 0.001 | 3.22 | 0.5 | |
| (3.15–13.0) | −17.5 | ||||||||
| Suicidal ideation or thoughts of self-harm | 312 | 0.27 (0.6) | 0.65 (1.0) | 49 | −0.39 | <0.001 | 3.85 | 0.57 | |
| (0.19–0.59) | −60.0 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obuobi-Donkor, G.; Shalaby, R.; Agyapong, B.; Dias, R.d.L.; Agyapong, V.I.O. Mitigating Psychological Problems Associated with the 2023 Wildfires in Alberta and Nova Scotia: Six-Week Outcomes from the Text4Hope Program. J. Clin. Med. 2024, 13, 865. https://doi.org/10.3390/jcm13030865
Obuobi-Donkor G, Shalaby R, Agyapong B, Dias RdL, Agyapong VIO. Mitigating Psychological Problems Associated with the 2023 Wildfires in Alberta and Nova Scotia: Six-Week Outcomes from the Text4Hope Program. Journal of Clinical Medicine. 2024; 13(3):865. https://doi.org/10.3390/jcm13030865
Chicago/Turabian StyleObuobi-Donkor, Gloria, Reham Shalaby, Belinda Agyapong, Raquel da Luz Dias, and Vincent Israel Opoku Agyapong. 2024. "Mitigating Psychological Problems Associated with the 2023 Wildfires in Alberta and Nova Scotia: Six-Week Outcomes from the Text4Hope Program" Journal of Clinical Medicine 13, no. 3: 865. https://doi.org/10.3390/jcm13030865
APA StyleObuobi-Donkor, G., Shalaby, R., Agyapong, B., Dias, R. d. L., & Agyapong, V. I. O. (2024). Mitigating Psychological Problems Associated with the 2023 Wildfires in Alberta and Nova Scotia: Six-Week Outcomes from the Text4Hope Program. Journal of Clinical Medicine, 13(3), 865. https://doi.org/10.3390/jcm13030865