
Time-Dependent Prediction Models for Individual Prognosis of Chronic Postsurgical Pain following Knee Replacement Based on an Extensive Multivariable Data Set
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Methods
3. Results
3.1. Study Subjects
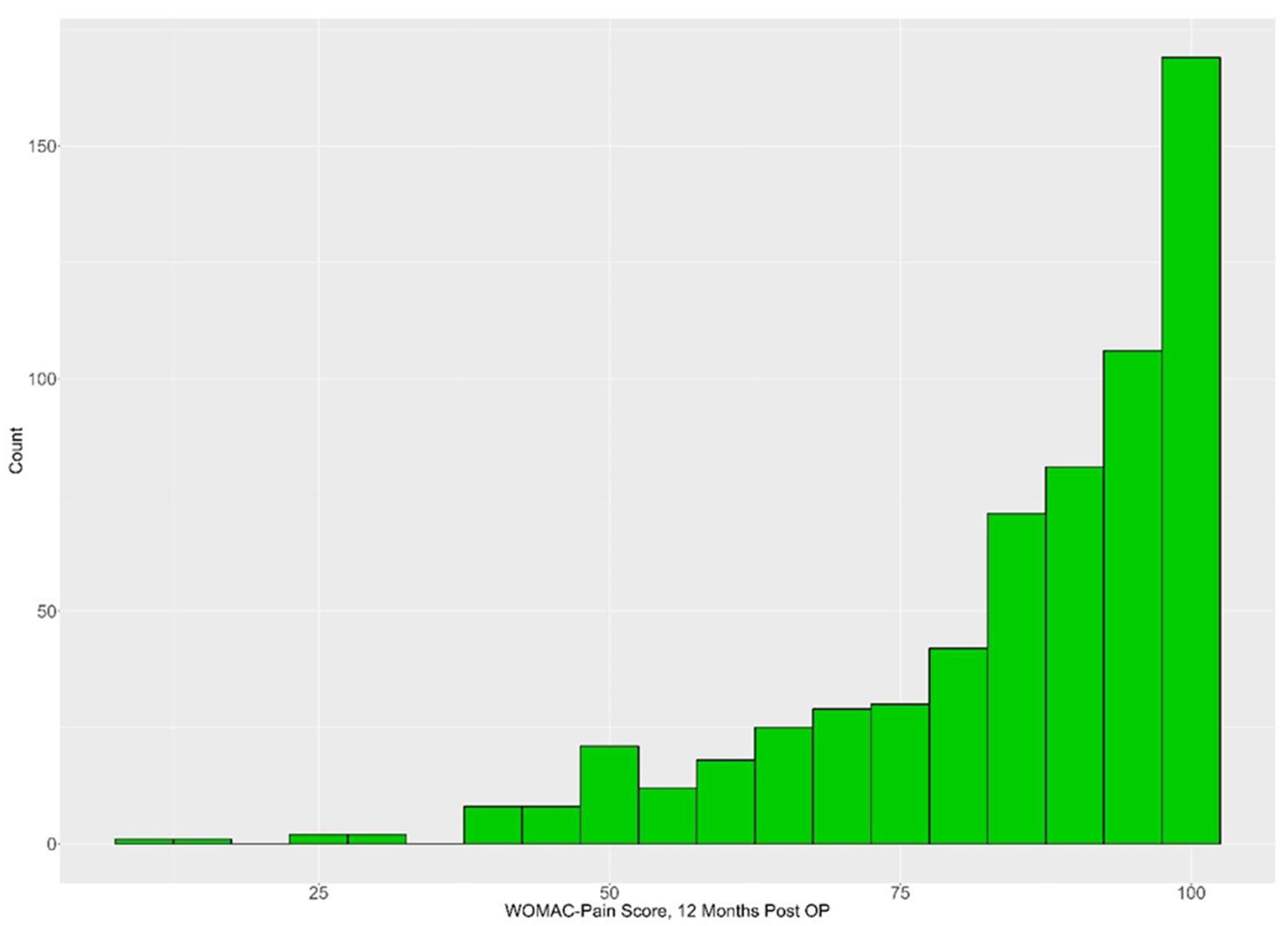
3.2. Pain Profile during the Process
3.3. Data Distributions between Subgroups with/without CPSP
3.4. Univariate Correlations
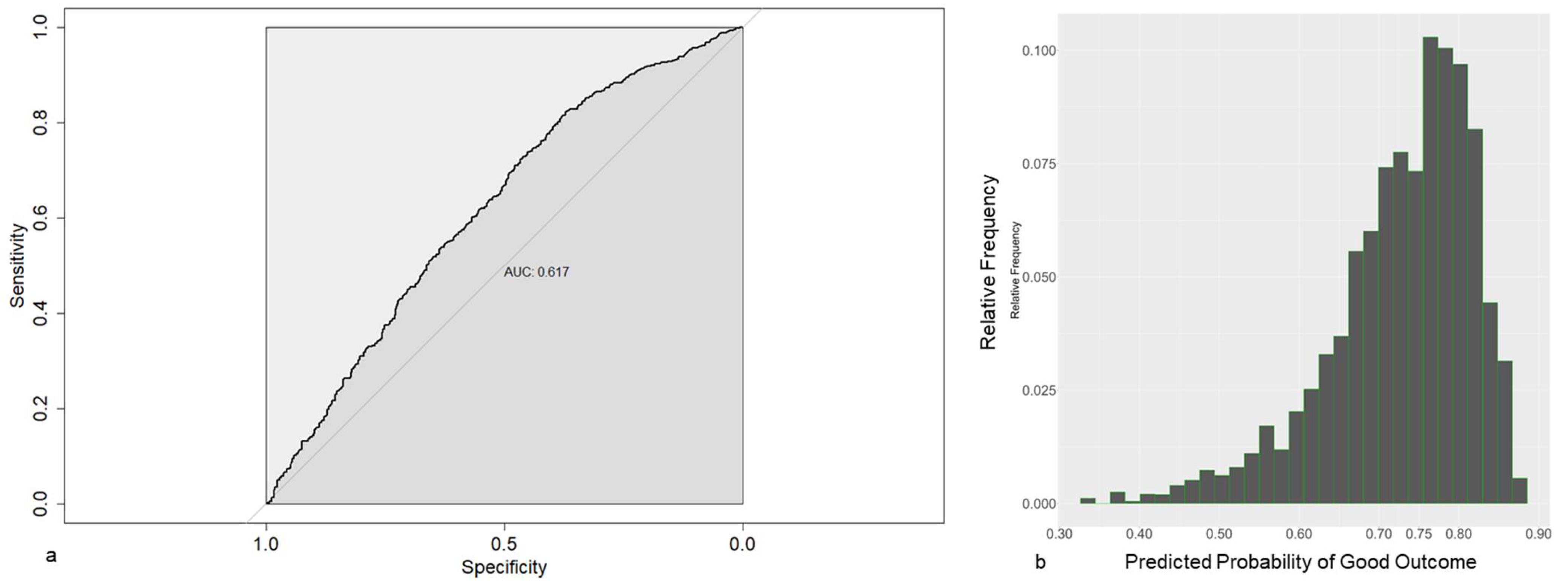
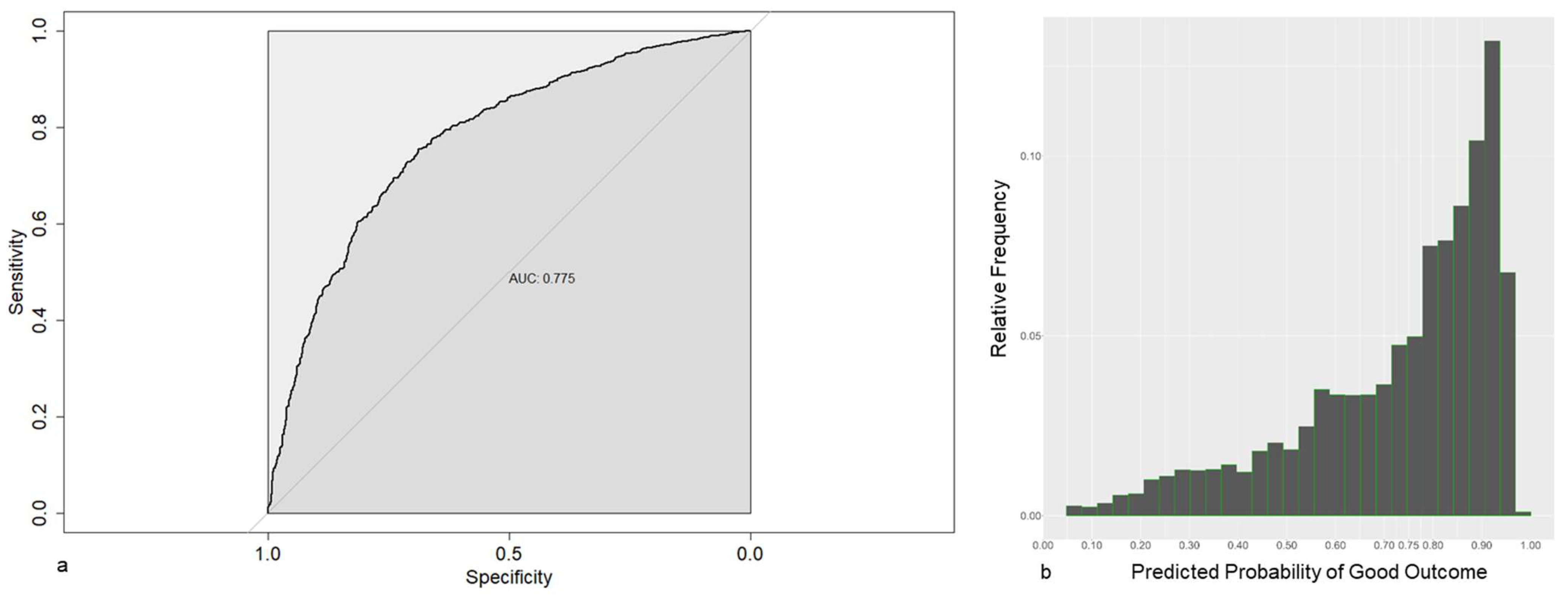
3.5. Prediction Models
4. Discussion
5. Summary
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rodríguez-Merchán, E.C. Outpatient total knee arthroplasty: Is it worth considering? EFORT Open Rev. 2020, 5, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Bundesamt, S. Die 20 Häufigsten Operationen Insgesamt. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Krankenhaeuser/Tabellen/drg-operationen-insgesamt.html (accessed on 12 October 2023).
- (DGOU) Deutsche Gesellschaft für Orthopädie und Unfallchirurgie. S2k-Leitlinie Indikation Knieendoprothese. 2023. Available online: https://register.awmf.org/assets/guidelines/187-004k_S3_Indikation_Knieendoprothese_2023-06.pdf (accessed on 12 October 2023).
- Keller, K.; Hobohm, L.; Barco, S.; Schmidtmann, I.; Münzel, T.; Engelhardt, M.; Drees, P. Venous thromboembolism in patients hospitalized for knee joint replacement surgery. Sci. Rep. 2020, 10, 22440. [Google Scholar] [CrossRef]
- Henderson, R.A.; Austin, M.S. Management of Periprosthetic Joint Infection: The More We Learn, the Less We Know. J. Arthroplast. 2017, 32, 2056–2059. [Google Scholar] [CrossRef] [PubMed]
- Beswick, A.D.; Wylde, V.; Gooberman-Hill, R.; Blom, A.; Dieppe, P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open 2012, 2, 435. [Google Scholar] [CrossRef]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Wang, S.J. A classification of chronic pain for ICD-11. PAIN 2015, 156, 1003–1007. [Google Scholar] [CrossRef]
- Schug, S.A.; Lavand’homme, P.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.D. The IASP classification of chronic pain for ICD-11, chronic postsurgical or posttraumatic pain. PAIN 2019, 160, 45–52. [Google Scholar] [CrossRef]
- World Health Organization. ICD-11 for Mortality and Morbidity Statistics: MG30.21 Chronic Postsurgical Pain; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Korwisi, B.; Hay, G.; Attal, N.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Barke, A. Classification algorithm for the International Classification of Diseases-11 chronic pain classification: Development and results from a preliminary pilot evaluation. PAIN 2021, 162, 2087–2096. [Google Scholar] [CrossRef]
- Dualé, C.; Ouchchane, L.; Schoeffler, P.; Soule-Sonneville, S.; Decoene, C.; Baylot, D.; Dubray, C. Neuropathic Aspects of Persistent Postsurgical Pain: A French Multicenter Survey With a 6-Month Prospective Follow-Up. J. Pain 2014, 15, 24.e1. [Google Scholar] [CrossRef]
- Wylde, V.; Hewlett, S.; Learmonth, I.D.; Dieppe, P. Persistent pain after joint replacement: Prevalence, sensory qualities, and postoperative determinants. PAIN 2011, 152, 566–572. [Google Scholar] [CrossRef]
- Fletcher, D.; Stamer, U.M.; Pogatzki-Zahn, E.; Zaslansky, R.; Tanase, N.V.; Perruchoud, C.; Meissner, W. Chronic postsurgical pain in Europe: An observational study. Eur. J. Anaesthesiol. EJA 2015, 32, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P. Transition from acute to chronic pain after surgery. Pain 2017, 158 (Suppl. S1), S50–S54. [Google Scholar] [CrossRef]
- Lewis, G.N.; Rice, D.A.; McNair, P.J.; Kluger, M. Predictors of persistent pain after total knee arthroplasty: A systematic review and meta-analysis. Br. J. Anaesth. 2015, 114, 551–561. [Google Scholar] [CrossRef]
- Núñez-Cortés, R.; Chamorro, C.; Ortega-Palavecinos, M.; Mattar, G.; Paredes, O.; Besoaín-Saldaña, Á.; Cruz-Montecinos, C. Social determinants associated to chronic pain after total knee arthroplasty. Int. Orthop. 2019, 43, 2767–2771. [Google Scholar] [CrossRef]
- Bonnin, M.P.; Basiglini, L.; Archbold, H.A. What are the factors of residual pain after uncomplicated TKA? Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Gabriel, S.; Lewallen, D. The impact of gender, age, and preoperative pain severity on pain after TKA. Clin. Orthop. Relat. Res. 2008, 466, 2717–2723. [Google Scholar] [CrossRef] [PubMed]
- Hafkamp, F.J.; de Vries, J.; Gosens, T.; den Oudsten, B.L. The Relationship Between Psychological Aspects and Trajectories of Symptoms in Total Knee Arthroplasty and Total Hip Arthroplasty. J. Arthroplast. 2021, 36, 78–87. [Google Scholar] [CrossRef]
- Chen, F.; Gao, W.; Hu, J.; Yang, X.; Chai, X.; Wang, D. Preoperative angiotensin II type 2 receptor is a predictor for developing chronic post-surgical pain after total knee arthroplasty surgery. Life Sci. 2021, 278, 119654. [Google Scholar] [CrossRef]
- Tian, M.; Li, Z.; Chen, X.; Wu, Q.; Shi, H.; Zhu, Y.; Shi, Y. Prevalence and Predictors of Chronic Pain with Two-Year Follow-Up After Knee Arthroplasty. J. Pain Res. 2022, 15, 1091–1105. [Google Scholar] [CrossRef] [PubMed]
- Sakellariou, V.I.; Poultsides, L.A.; Ma, Y.; Bae, J.; Liu, S.; Sculco, T.P. Risk Assessment for Chronic Pain and Patient Satisfaction After Total Knee Arthroplasty. Orthopedics 2016, 39, 55–62. [Google Scholar] [CrossRef]
- Sciberras, S.C.; Vella, A.P.; Vella, B.; Spiteri, J.; Mizzi, C.; Borg-Xuereb, K.; LaFerla, G.; Grech, G.; Sammut, F. A randomized, controlled trial on the effect of anesthesia on chronic pain after total knee arthroplasty. Pain Manag. 2022, 12, 711–723. [Google Scholar] [CrossRef]
- Aso, K.; Ikeuchi, M.; Takaya, S.; Sugimura, N.; Izumi, M.; Wada, H.; Okanoue, Y.; Dan, J. Chronic postsurgical pain after total knee arthroplasty: A prospective cohort study in Japanese population. Mod. Rheumatol. 2021, 31, 1038–1044. [Google Scholar] [CrossRef]
- Imai, R.; Nishigami, T.; Kubo, T.; Ishigaki, T.; Yonemoto, Y.; Mibu, A.; Morioka, S.; Fujii, T. Using a postoperative pain trajectory to predict pain at 1 year after total knee arthroplasty. Knee 2021, 32, 194–200. [Google Scholar] [CrossRef]
- Buvanendran, A.; Della Valle, C.J.; Kroin, J.S.; Shah, M.; Moric, M.; Tuman, K.J.; McCarthy, R.J. Acute postoperative pain is an independent predictor of chronic postsurgical pain following total knee arthroplasty at 6 months: A prospective cohort study. Reg. Anesth. Pain. Med. 2019, 44, e100036. [Google Scholar] [CrossRef]
- Palanne, R.; Rantasalo, M.; Vakkuri, A.; Olkkola, K.T.; Vahlberg, T.; Skants, N. Testing of a predictive risk index for persistent postsurgical pain on patients undergoing total knee arthroplasty: A prospective cohort study. Eur. J. Pain 2023, 27, 961–972. [Google Scholar] [CrossRef]
- Betz, U.; Langanki, L.; Heid, F.; Spielberger, J.; Schollenberger, L.; Kronfeld, K.; Büttner, M.; Büchler, B.; Goldhofer, M.; Eckhard, L.; et al. The PROMISE study protocol: A multicenter prospective study of process optimization with interdisciplinary and cross-sectoral care for German patients receiving hip and knee endoprostheses. Acta Orthop. 2021, 92, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Betz, U.; Langanki, L.; Heid, F.; Schollenberger, L.; Kronfeld, K.; Büttner, M.; Büchler, B.; Eckhard, L.; Klonschinski, T.; Drees, P. Feasibility of a Complex Optimized Process for the Treatment of Patients Receiving Hip and Knee Endoprostheses in Most Different Settings in Germany—Results from the PROMISE Trial. Processes 2022, 10, 824. [Google Scholar] [CrossRef]
- Wainwright, T.W.; Gill, M.; McDonald, D.A.; Middleton, R.G.; Reed, M.; Sahota, O.; Yates, P.; Ljungqvist, O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop. 2020, 91, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W.; Gill, M.; McDonald, D.A.; Middleton, R.G.; Reed, M.; Sahota, O.; Yates, P.; Ljungqvist, O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Acta Orthop. 2020, 91, 3–19, Erratum in Acta Orthop. 2020, 91, 363. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Lange, T.; Günther, K.P.; Kopkow, C.; Rataj, E.; Apfelbacher, C.; Aringer, M.; Böhle, E.; Bork, H.; Dreinhöfer, K.; et al. Indication Criteria for Total Knee Arthroplasty in Patients with Osteoarthritis—A Multi-perspective Consensus Study. Z. Orthop. Unfall 2017, 155, 539–548. [Google Scholar] [CrossRef]
- Wylde, V.; Beswick, A.; Bruce, J.; Blom, A.; Howells, N.; Gooberman-Hill, R. Chronic pain after total knee arthroplasty. EFORT Open Rev. 2018, 3, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Knee Injury an Osteoarthritis Outcome Score. KOOS Scoring 2012. 2012. Available online: https://www.koos.nu/KOOSscoring2012.pdf (accessed on 10 October 2018).
- Du, J.; Han, P.; Beesley, L.J.; Goutman, S.A.; Batterman, S.; Feldman, E.L.; Mukherjee, B. Variable selection with multiply-imputed datasets: Choosing between stacked and grouped methods. arXiv 2020. [Google Scholar] [CrossRef]
- Clement, N.D.; Bardgett, M.; Weir, D.; Holland, J.; Gerrand, C.; Deehan, D.J. What is the Minimum Clinically Important Difference for the WOMAC Index After TKA? Clin. Orthop. Relat. Res. 2018, 476, 2005–2014. [Google Scholar] [CrossRef]
- Schug, S.A.; Bruce, J. Risk stratification for the development of chronic postsurgical pain. PAIN Rep. 2017, 2, e627. [Google Scholar] [CrossRef]
- Rosenberger, D.C.; Pogatzki-Zahn, E.M. Chronic post-surgical pain—Update on incidence, risk factors and preventive treatment options. BJA Educ. 2022, 22, 190–196. [Google Scholar] [CrossRef]
- Pinedo-Villanueva, R.; Khalid, S.; Wylde, V.; Gooberman-Hill, R.; Soni, A.; Judge, A. Identifying individuals with chronic pain after knee replacement: A population-cohort, cluster-analysis of Oxford knee scores in 128,145 patients from the English National Health Service. BMC Musculoskelet. Disord. 2018, 19, 354. [Google Scholar] [CrossRef] [PubMed]
- Wunderlich, F.; Eckhard, L.; Büttner, M.; Lange, T.; Konradi, J.; Betz, U.; Drees, P.; Lützner, J. The INDICATE Knee expectations survey detects general patient treatment goals for total knee arthroplasty and the influence of demographic factors on patients expectations. Knee Surg. Sports Traumatol. Arthrosc. 2022, 31, 892–904. [Google Scholar] [CrossRef] [PubMed]
- Ayers, D.C.; Yousef, M.; Zheng, H.; Yang, W.; Franklin, P.D. The Prevalence and Predictors of Patient Dissatisfaction 5-years Following Primary Total Knee Arthroplasty. J. Arthroplast. 2022, 37, S121–S128. [Google Scholar] [CrossRef]
- Ashoorion, V.; Sadeghirad, B.; Wang, L.; Noori, A.; Abdar, M.; Kim, Y.; Chang, Y.; Rehman, N.; Lopes, L.C.; Couban, R.J.; et al. Predictors of Persistent Post-Surgical Pain Following Total Knee Arthroplasty: A Systematic Review and Meta-Analysis of Observational Studies. Pain Med. 2022, 24, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Balogun, S.; Scott, D.; Cicuttini, F.; Jones, G.; Aitken, D. Longitudinal study of the relationship between physical activity and knee pain and functional limitation in community-dwelling older adults. Arch. Gerontol. Geriatr. 2020, 90, 104101. [Google Scholar] [CrossRef]
- Braunwalder, C.; Müller, R.; Glisic, M.; Fekete, C. Are Positive Psychology Interventions Efficacious in Chronic Pain Treatment? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Med. 2022, 23, 122–136. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B. Individual differences in pain: Understanding the mosaic that makes pain personal. PAIN 2017, 158 (Suppl. S1), S11–S18. [Google Scholar] [CrossRef] [PubMed]
- Wunderlich, F.; Ghaemi Kerahrodi, J.; Kuchen, R.; Klonschinski, T.; Afghanyar, Y.; Wegner, E.; Drees, P.; Eckhard, L. Optimism and pessimism are antithetically associated with post-operative knee function in patients’ undergoing total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 3971–3980. [Google Scholar] [CrossRef]
- Schnabel, A.; Yahiaoui-Doktor, M.; Meissner, W.; Zahn, P.K.; Pogatzki-Zahn, E.M. Predicting poor postoperative acute pain outcome in adults: An international, multicentre database analysis of risk factors in 50,005 patients. PAIN Rep. 2020, 5, e831. [Google Scholar] [CrossRef]
- Shiri, R.; Karppinen, J.; Leino-Arjas, P.; Solovieva, S.; Viikari-Juntura, E. The association between smoking and low back pain: A meta-analysis. Am. J. Med. 2010, 123, 87.e7–87.e35. [Google Scholar] [CrossRef] [PubMed]
- Muertizha, M.; Cai, X.; Ji, B.; Aimaiti, A.; Cao, L. Factors contributing to 1-year dissatisfaction after total knee arthroplasty: A nomogram prediction model. J. Orthop. Surg. Res. 2022, 17, 367. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Short Form * | Category | Values | Time Point | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ind | pre | surg | post | rehab | 3 mo | 6 mo | 1 y | ||||
| Knee Injury and Osteoarthritis Outcome Score (KOOS)—subscore sport Questionnaire to assess short- and long-term patient-relevant outcomes following knee injury. Five subscores: pain, symptoms, Activities of Daily Living, sport and recreation function and knee-related Quality of Life; self-administered | KOOS sport | Activity | Score range 0–100 | X | X | X | X | ||||
| Knee Injury and Osteoarthritis Outcome Score (KOOS)—subscore ADL | KOOS ADL | ADL | Score range 0–100 | X | X | X | X | ||||
| Somatic Symptom Disorder (SSD) Q2: During the last 7 days, my bodily symptoms interfered with daily life activities Two-item screening questionnaire to assess somatic symptom disorder. | SSD Q2 | ADL | Score range 0–10 | X | X | X | X | X | X | X | |
| Height of the patient | Height | Body characterization | Centimeters | X | |||||||
| Weight at day of surgery | Weight | Body characterization | Kilograms | X | |||||||
| Length of hospital stay | LOS | Function | Days | X | |||||||
| Possible walking distance | Walking dist | Function | Score range 1–5 | X | |||||||
| Timed “Up and Go” Test | TUG | Function | Seconds | X | X | X | |||||
| Alcohol consumption on a regular basis | Alcohol | Health | Yes/no | X | |||||||
| American Society of Anesthesiologists (ASA) classification Grading system for a person’s state of health before a surgical procedure. | ASA | Health | Score range 1–6 | X | |||||||
| Identification of Seniors at Risk (ISAR) Questionnaire to identify seniors with increased risk of adverse functional outcomes. | ISAR | Health | Score range 0–6 | X | |||||||
| Smoker | Smoker | Health | Yes/no | X | |||||||
| Did the patient participate in the preoperative patient school? | Patients School | Process | Yes/no | X | |||||||
| Duration of rehabilitation | Rehab duration | Process | Days | X | |||||||
| Duration of pre-treatment | Pre-treatment | Process | Days | X | |||||||
| Life Orientation Tests (LOT-R) on optimism Questionnaire to assess the dispositional level of optimism/pessimism. | LOT-R opt | Psychometric | Score range 0–12 | X | |||||||
| Life Orientation Tests (LOT-R) on pessimism Questionnaire to assess the dispositional level of optimism/pessimism. | LOT-R pess | Psychometric | Score range 0–12 | X | |||||||
| Oslo Social Support Scale (OSSS) Three-item screening questionnaire to assess perceived social support. | OSSS | Psychometric | Score range 3–14 | X | |||||||
| Patient Health Questionnaire-4 (PHQ-4) Four-item screening questionnaire to assess mental distress (anxiety/depression). | PHQ-4 | Psychometric | Score range 0–12 | X | X | X | X | X | X | X | |
| European Quality of Life 5 Dimensions 5 Level Version (EQ-5D-5L) Questionnaire for measuring patient-reported outcomes to assess the Quality of Life of patients regardless of their illness. | EQ-5D-5L | QoL | Score range < 0–1 | X | X | X | X | X | X | ||
| Knee Injury and Osteoarthritis Outcome Score (KOOS)—subscore QoL | KOOS QoL | QoL | Score range 0–100 | X | X | X | X | ||||
| Age at day of surgery | Age | Sociodemographic | Years | X | |||||||
| Higher school degree | Higher school | Sociodemographic | Yes/no | X | |||||||
| Marital status—married or single with partner | Marital with | Sociodemographic | Yes/no | X | |||||||
| Number of children | Number children | Sociodemographic | Number | X | |||||||
| Female Sex | Female sex | Sociodemographic | Yes/male | X | |||||||
| What is the total monthly net income of your household in euros? | Income | Sociodemographic | Score range 1–8 | X | |||||||
| Employment situation—full or part-time (15–34 h/week) employed | Employed | Sociodemographic | Yes/others | X | |||||||
| Cortisone application preoperatively | Cortisone | Surgery | Yes/no | X | |||||||
| Duration of the surgery | Surg duration | Surgery | Minutes | X | |||||||
| Tranexamic acid application intraoperatively | Surg tranex | Surgery | Yes/no | X | |||||||
| Intubation anesthesia | Intub anesthesia | Surgery | Yes/spinal anesthesia | x | |||||||
| Use of local infiltration analgesia (LIA) | Surg LIA | Surgery | Yes/no | x | |||||||
| Use of pneumatic tourniquet | Surg tourn | Surgery | Yes/no | x | |||||||
| Use of drains | Surg drain | Surgery | Yes/no | x | |||||||
| Knee Injury and Osteoarthritis Outcome Score (KOOS)—subscore pain | KOOS pain | Symptoms | Score range 0–100 | X | X | X | X | ||||
| Knee Injury and Osteoarthritis Outcome Score (KOOS)—subscore symptoms | KOOS symp | Symptoms | Score range 0–100 | X | X | X | X | ||||
| SSD Q1 During the last 7 days, the overall intensity of my bodily symptoms was Two-item screening questionnaire to assess somatic symptom disorder. | SSD Q1 | Symptoms | Score range 0–10 | X | X | X | X | X | X | X | |
| Visual analog scale (VAS)/Numeric Rating scale (NRS) at rest | Pain rest | Symptoms | Score range 0–10 | X | X | X | |||||
| Visual analog scale (VAS)/Numeric Rating scale (NRS) with load | Pain load | Symptoms | Score range 0–10 | X | X | X | |||||
| Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)—subscore pain Questionnaire to evaluate the condition of patients with osteoarthritis of the knee and hip, including pain, stiffness and physical functioning of the joints. | WOMAC pain | Symptoms | Score range 0–20 | X | X | X | X | ||||
| Staffelstein Score Questionnaire to assess rehabilitation success after hip and knee arthroplasty, including pain, activities of daily living and physical functioning of the joints. | Staffelstein | Symptoms/ADL/Function | Score range 0–120 | X | X | X | |||||
| TKA (n = 933) | ||
|---|---|---|
| Missing | n (%) | |
| Sex | ||
| male | 416 (44.6) | |
| female | 517 (55.4) | |
| Joint | ||
| knee left | 490 (49.3) | |
| knee right | 504 (50.7) | |
| Comorbidities | ||
| at least one comorbidity | 744 (79.7%) | |
| mean (SD) | ||
| number of comorbidities | 1.7 (1.4) | |
| ASA | 77 | 2.3 (0.6) |
| Age | 52 | 67.1 (9.6) |
| BMI | 73 | 30.2 (5.8) |
| Visit | n | Minimum | 1st Quartile | Median | Mean | 3rd Quartile | Maximum |
|---|---|---|---|---|---|---|---|
| ind | 908 | 0 | 40 | 50 | 50.84 | 65 | 100 |
| 3 mo | 747 | 0 | 60 | 75 | 74.20 | 90 | 100 |
| 6 mo | 726 | 20 | 70 | 85 | 79.73 | 95 | 100 |
| 1 y | 626 | 10 | 76.25 | 90 | 84.93 | 100 | 100 |
| Parameter Short Form | Time Point | WOMAC Pain ≤75 (n = 157) | WOMAC Pain >75 (n = 469) | Total (n = 626) | p Value |
|---|---|---|---|---|---|
| Age | ind | 0.002 | |||
| 65.06 (9.79) | 67.62 (8.74) | 66.97 (9.08) | |||
| SSD Q1 | ind | 0.013 | |||
| 6.20 (1.73) | 5.74 (1.94) | 5.86 (1.90) | |||
| Income | ind | 0.032 | |||
| 5.15 (2.00) | 5.60 (1.94) | 5.49 (1.97) | |||
| EQ-5D-5L | ind | 0.011 | |||
| 0.63 (0.19) | 0.67 (0.18) | 0.66 (0.18) | |||
| OSSS | ind | <0.001 | |||
| 10.51 (2.21) | 11.17 (1.96) | 11.00 (2.04) | |||
| PHQ-4 | ind | <0.001 | |||
| 3.49 (2.96) | 2.14 (2.28) | 2.48 (2.53) | |||
| LOT-R opt | ind | <0.001 | |||
| 9.45 (2.42) | 10.46 (2.18) | 10.21 (2.28) | |||
| LOT-R pess | ind | <0.001 | |||
| 8.23 (3.06) | 9.70 (2.59) | 9.33 (2.79) | |||
| KOOS pain | ind | <0.001 | |||
| 41.90 (15.72) | 48.13 (17.28) | 46.56 (17.10) | |||
| KOOS symp | ind | <0.001 | |||
| 47.33 (17.55) | 55.73 (19.38) | 53.62 (19.28) | |||
| KOOS ADL | ind | <0.001 | |||
| 50.54 (19.24) | 57.06 (17.93) | 55.42 (18.47) | |||
| Staffelstein | ind | 0.010 | |||
| 78.33 (12.43) | 81.55 (12.37) | 80.77 (12.45) | |||
| WOMAC pain | ind | <0.001 | |||
| 45.80 (17.12) | 53.99 (18.29) | 51.93 (18.33) | |||
| Pain rest | pre | <0.001 | |||
| 3.48 (2.44) | 2.43 (2.37) | 2.68 (2.43) | |||
| Pain load | pre | 0.016 | |||
| 5.25 (2.30) | 4.64 (2.63) | 4.79 (2.56) | |||
| ISAR | pre | 0.005 | |||
| 0.58 (0.84) | 0.35 (0.72) | 0.41 (0.76) | |||
| PHQ-4 | pre | <0.001 | |||
| 3.81 (3.17) | 2.03 (2.13) | 2.43 (2.52) | |||
| Weight | surg | 0.027 | |||
| 90.55 (18.46) | 86.90 (17.76) | 87.81 (18.00) | |||
| TUG | post | 0.023 | |||
| 18.22 (8.26) | 16.70 (5.91) | 17.09 (6.62) | |||
| Pain rest | post | <0.001 | |||
| 2.62 (1.90) | 1.92 (1.72) | 2.10 (1.79) | |||
| Pain load | post | 0.002 | |||
| 3.89 (1.95) | 3.32 (1.80) | 3.46 (1.85) | |||
| EQ-5D-5L | post | 0.022 | |||
| 0.76 (0.17) | 0.80 (0.15) | 0.79 (0.15) | |||
| PHQ-4 | post | <0.001 | |||
| 2.71 (2.79) | 1.71 (2.10) | 1.96 (2.33) | |||
| EQ-5D-5L | rehab | <0.001 | |||
| 0.77 (0.14) | 0.84 (0.11) | 0.82 (0.12) | |||
| Pain rest | rehab | 0.001 | |||
| 2.28 (1.85) | 1.50 (1.51) | 1.72 (1.65) | |||
| Pain load | rehab | 0.002 | |||
| 3.68 (1.94) | 2.86 (1.71) | 3.09 (1.81) | |||
| PHQ-4 | rehab | <0.001 | |||
| 2.49 (2.12) | 1.04 (1.73) | 1.42 (1.95) | |||
| Staffelstein | rehab | <0.001 | |||
| 85.04 (12.36) | 92.43 (13.21) | 90.73 (13.37) | |||
| SSD Q1 | 3 mo | <0.001 | |||
| 4.21 (1.88) | 2.72 (1.97) | 3.10 (2.05) | |||
| EQ-5D-5L | 3 mo | <0.001 | |||
| 0.74 (0.18) | 0.87 (0.11) | 0.84 (0.14) | |||
| KOOS pain | 3 mo | <0.001 | |||
| 55.16 (17.13) | 75.76 (15.37) | 70.61 (18.16) | |||
| KOOS symp | 3 mo | <0.001 | |||
| 54.06 (17.52) | 72.40 (15.05) | 67.83 (17.58) | |||
| KOOS ADL | 3 mo | <0.001 | |||
| 60.62 (16.21) | 79.64 (13.60) | 74.88 (16.49) | |||
| KOOS sport | 3 mo | <0.001 | |||
| 29.41 (21.90) | 49.59 (25.18) | 44.46 (25.91) | |||
| KOOS QoL | 3 mo | <0.001 | |||
| 36.53 (19.02) | 56.66 (20.86) | 51.56 (22.19) | |||
| WOMAC pain | 3 mo | <0.001 | |||
| 59.90 (17.48) | 79.86 (14.38) | 74.87 (17.49) | |||
| PHQ-4 | 3 mo | <0.001 | |||
| 2.97 (2.86) | 1.09 (1.90) | 1.57 (2.33) | |||
| SSD Q1 | 6 mo | <0.001 | |||
| 4.16 (1.95) | 2.24 (1.85) | 2.71 (2.05) | |||
| SSD Q2 | 6 mo | <0.001 | |||
| 4.13 (2.14) | 2.08 (1.93) | 2.59 (2.17) | |||
| EQ-5D-5L | 6 mo | <0.001 | |||
| 0.75 (0.18) | 0.90 (0.11) | 0.86 (0.14) | |||
| PHQ-4 | 6 mo | <0.001 | |||
| 2.88 (2.66) | 0.93 (1.64) | 1.40 (2.11) | |||
| KOOS pain | 6 mo | <0.001 | |||
| 58.34 (16.85) | 82.80 (13.86) | 76.96 (17.95) | |||
| KOOS symp | 6 mo | <0.001 | |||
| 58.21 (14.42) | 78.81 (14.61) | 73.91 (17.00) | |||
| KOOS ADL | 6 mo | <0.001 | |||
| 62.72 (15.65) | 84.16 (12.55) | 79.11 (16.15) | |||
| KOOS sport | 6 mo | <0.001 | |||
| 32.29 (21.60) | 58.92 (23.32) | 52.53 (25.57) | |||
| KOOS QoL | 6 mo | <0.001 | |||
| 40.65 (19.52) | 65.57 (20.48) | 59.59 (22.87) | |||
| WOMAC pain | 6 mo | <0.001 | |||
| 63.05 (17.17) | 86.01 (12.99) | 80.53 (17.16) | |||
| SSD Q1 | 1 y | <0.001 | |||
| 3.95 (2.07) | 1.84 (1.81) | 2.36 (2.09) | |||
| SSD Q2 | 1 y | <0.001 | |||
| 4.03 (2.28) | 1.64 (1.80) | 2.24 (2.19) | |||
| EQ-5D-5L | 1 y | <0.001 | |||
| 0.75 (0.18) | 0.93 (0.10) | 0.89 (0.14) | |||
| PHQ-4 | 1 y | <0.001 | |||
| 2.74 (2.99) | 0.80 (1.49) | 1.29 (2.15) | |||
| KOOS symp | 1 y | <0.001 | |||
| 61.51 (15.61) | 84.79 (12.11) | 79.01 (16.48) | |||
| KOOS ADL | 1 y | <0.001 | |||
| 62.81 (16.35) | 90.22 (9.15) | 83.32 (16.47) | |||
| KOOS sport | 1 y | <0.001 | |||
| 35.57 (24.58) | 67.68 (21.08) | 59.42 (26.11) | |||
| KOOS QoL | 1 y | <0.001 | |||
| 42.31 (18.54) | 72.95 (18.71) | 65.26 (22.90) |
| Parameter—Short Form | Time Point | r | p |
|---|---|---|---|
| KOOS pain | 6 mo | 0.555 | <0.0001 |
| WOMAC pain | 6 mo | 0.554 | <0.0001 |
| KOOS ADL | 6 mo | 0.550 | <0.0001 |
| KOOS ADL | 3 mo | 0.510 | <0.0001 |
| WOMAC pain | 3 mo | 0.483 | <0.0001 |
| KOOS pain | 3 mo | 0.480 | <0.0001 |
| KOOS symp | 6 mo | 0.474 | <0.0001 |
| KOOS QoL | 6 mo | 0.467 | <0.0001 |
| KOOS sport | 6 mo | 0.466 | <0.0001 |
| EQ-5D-5L | 6 mo | 0.445 | <0.0001 |
| KOOS symp | 3 mo | 0.427 | <0.0001 |
| SSD Q1 | 6 mo | −0.419 | <0.0001 |
| EQ-5D-5L | 3 mo | 0.418 | <0.0001 |
| SSD Q2 | 6 mo | −0.416 | <0.0001 |
| SSD Q2 | 3 mo | −0.407 | <0.0001 |
| KOOS QoL | 3 mo | 0.407 | <0.0001 |
| KOOS sport | 3 mo | 0.385 | <0.0001 |
| PHQ-4 | 6 mo | −0.383 | <0.0001 |
| SSD Q1 | 3 mo | −0.369 | <0.0001 |
| PHQ-4 | 3 mo | −0.363 | <0.0001 |
| PHQ-4 | rehab | −0.320 | <0.0001 |
| PHQ-4 | pre | −0.294 | <0.0001 |
| EQ-5D-5L | rehab | 0.284 | <0.0001 |
| Staffelstein | rehab | 0.269 | <0.0001 |
| LOT-R pess | ind | 0.251 | <0.0001 |
| PHQ-4 | ind | −0.249 | <0.0001 |
| Pain load | rehab | −0.235 | <0.0001 |
| SSD Q2 | rehab | −0.235 | <0.0001 |
| Pain rest | rehab | −0.225 | 0.0002 |
| KOOS ADL | ind | 0.217 | <0.0001 |
| SSD Q1 | rehab | −0.215 | <0.0001 |
| WOMAC pain | ind | 0.214 | <0.0001 |
| PHQ-4 | post | −0.205 | <0.0001 |
| Pain rest | pre | −0.200 | <0.0001 |
| Pain rest | post | −0.191 | <0.0001 |
| KOOS pain | ind | 0.187 | <0.0001 |
| LOT-R opt | ind | 0.184 | <0.0001 |
| EQ-5D-5L | ind | 0.180 | <0.0001 |
| KOOS symp | ind | 0.171 | <0.0001 |
| Pain load | pre | −0.157 | 0.0001 |
| Pain load | post | −0.156 | 0.0005 |
| ISAR | pre | −0.155 | <0.0001 |
| KOOS sport | ind | 0.151 | <0.0001 |
| OSSS | ind | 0.148 | 0.0001 |
| Staffelstein | ind | 0.142 | 0.0004 |
| EQ-5D-5L | post | 0.136 | 0.0006 |
| SSD Q1 | ind | −0.129 | 0.0009 |
| KOOS QoL | ind | 0.125 | 0.0008 |
| Age | ind | 0.124 | 0.001 |
| SSD Q2 | pre | −0.120 | 0.001 |
| SSD Q1 | pre | −0.111 | 0.005 |
| Staffelstein | post | 0.109 | 0.004 |
| Weight | surg | −0.104 | 0.008 |
| Income | ind | 0.104 | 0.010 |
| TUG | post | −0.103 | 0.022 |
| SSD Q2 | ind | −0.102 | 0.006 |
| TUG | pre | −0.098 | 0.015 |
| TUG | rehab | −0.087 | 0.121 |
| SSD Q2 | post | −0.078 | 0.037 |
| SSD Q1 | post | −0.076 | 0.053 |
| Surg duration | surg | −0.059 | 0.118 |
| Intub anesthesia | surg | −0.056 | 0.185 |
| Number children | ind | 0.049 | 0.194 |
| LOS | post | −0.044 | 0.304 |
| Surg tourn | surg | 0.042 | 0.268 |
| Alcohol | ind | 0.041 | 0.289 |
| Surg LIA | surg | 0.036 | 0.406 |
| Smoker | ind | −0.035 | 0.357 |
| Cortisone | surg | −0.035 | 0.364 |
| Higher school | ind | 0.030 | 0.397 |
| Walking dist | post | 0.029 | 0.595 |
| Patients school | post | 0.025 | 0.505 |
| Rehab duration | rehab | −0.018 | 0.711 |
| Martial with | ind | 0.018 | 0.648 |
| Female sex | ind | −0.016 | 0.673 |
| Employed | ind | −0.016 | 0.684 |
| Time till surg | pre | 0.014 | 0.722 |
| Surg drain | surg | −0.013 | 0.724 |
| Height | surg | 0.010 | 0.796 |
| Surg tranex | surg | 0.005 | 0.899 |
| ASA | pre | −0.004 | 0.915 |
| Using Non-Standardized Data | ||||
|---|---|---|---|---|
| (Intercept) | Age, ind | LOT-R pess, ind | WOMAC pain, ind | TUG, pre |
| −1.1000 | 0.0100 | 0.1100 | 0.0089 | −0.0004 |
| Using Standardized Data | ||||
| (Intercept) | Age, ind | LOT-R pess, ind | WOMAC pain, ind | TUG, pre |
| 1.005 | 0.097 | 0.316 | 0.165 | −0.002 |
| Using Non-Standardized Data | |||
|---|---|---|---|
| (Intercept) | PHQ-4 Score, pre | KOOS pain, 3 mo | WOMAC pain, 3 mo |
| −3.784 | −0.088 | 0.008 | 0.014 |
| KOOS symp, 6 mo | KOOS sport, 6 mo | KOOS QoL, 6 mo | WOMAC pain, 6 mo |
| 0.019 | 0.007 | 0.002 | 0.023 |
| Using Standardized Data | |||
| (Intercept) | PHQ-4 Score, pre | KOOS pain, 3 mo | WOMAC pain, 3 mo |
| 1.207 | −0.224 | 0.144 | 0.253 |
| KOOS symp, 6 mo | KOOS sport, 6 mo | KOOS QoL, 6 mo | WOMAC pain, 6 mo |
| 0.335 | 0.179 | 0.040 | 0.400 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Betz, U.; Clarius, M.; Krieger, M.; Konradi, J.; Kuchen, R.; Schollenberger, L.; Wiltink, J.; Drees, P. Time-Dependent Prediction Models for Individual Prognosis of Chronic Postsurgical Pain following Knee Replacement Based on an Extensive Multivariable Data Set. J. Clin. Med. 2024, 13, 862. https://doi.org/10.3390/jcm13030862
Betz U, Clarius M, Krieger M, Konradi J, Kuchen R, Schollenberger L, Wiltink J, Drees P. Time-Dependent Prediction Models for Individual Prognosis of Chronic Postsurgical Pain following Knee Replacement Based on an Extensive Multivariable Data Set. Journal of Clinical Medicine. 2024; 13(3):862. https://doi.org/10.3390/jcm13030862
Chicago/Turabian StyleBetz, Ulrich, Michael Clarius, Manfred Krieger, Jürgen Konradi, Robert Kuchen, Lukas Schollenberger, Jörg Wiltink, and Philipp Drees. 2024. "Time-Dependent Prediction Models for Individual Prognosis of Chronic Postsurgical Pain following Knee Replacement Based on an Extensive Multivariable Data Set" Journal of Clinical Medicine 13, no. 3: 862. https://doi.org/10.3390/jcm13030862
APA StyleBetz, U., Clarius, M., Krieger, M., Konradi, J., Kuchen, R., Schollenberger, L., Wiltink, J., & Drees, P. (2024). Time-Dependent Prediction Models for Individual Prognosis of Chronic Postsurgical Pain following Knee Replacement Based on an Extensive Multivariable Data Set. Journal of Clinical Medicine, 13(3), 862. https://doi.org/10.3390/jcm13030862