
Age- and Sex-Specific Reference Values for Renal Volume and Association with Risk Factors for Chronic Kidney Disease in a General Population—An MRI-Based Study

Abstract
1. Introduction
2. Materials and Methods
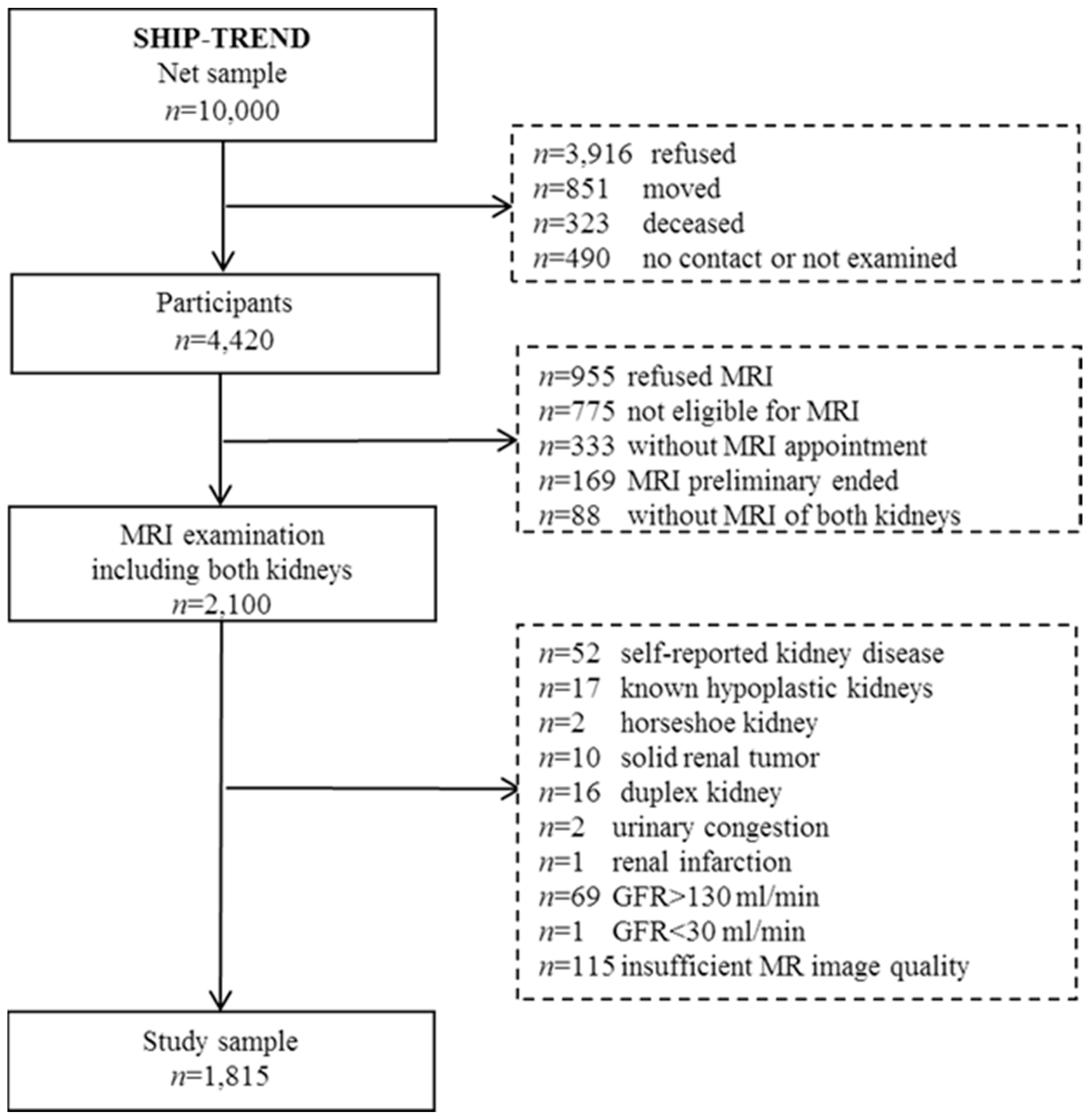
2.1. Study Sample
2.2. MR Imaging and Renal Volumetry
2.3. Clinical and Laboratory Measurements
2.4. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
| Women | Men | ||
|---|---|---|---|
| Parameter | n = 930 | n = 885 | p-Value * |
| Age (years) | 52 (41; 62) | 51 (41; 62) | 0.718 |
| Smoking status | <0.001 | ||
| Never-smoker | 437 (47.0%) | 270 (30.6%) | |
| Ex-smoker | 280 (30.1%) | 398 (45.1%) | |
| Current smoker | 212 (22.8%) | 214 (24.3%) | |
| Body mass index (kg/m2) | 26.5 (23.3; 30.5) | 27.8 (25.5; 30.5) | <0.001 |
| Body surface area (m2) | 1.78 (1.68; 1.89) | 2.05 (1.94; 2.15) | <0.001 |
| Systolic BP (mmHg) | 119 (109; 130) | 132 (123; 142) | <0.001 |
| Diastolic BP (mmHg) | 74 (69; 80) | 80 (73; 86) | <0.001 |
| Hypertension | 345 (37.1%) | 439 (49.9%) | <0.001 |
| Diabetes mellitus (Typ-2) | 58 (6.2%) | 73 (8.3%) | 0.994 |
| HbA1c (%) | 5.2 (4.8; 5.6) | 5.3 (4.9; 5.6) | <0.001 |
| HDL-C (mmol/L) | 1.58 (1.35; 1.85) | 1.25 (1.07; 1.47) | <0.001 |
| LDL-C (mmol/L) | 3.33 (2.76; 4) | 3.43 (2.77; 4) | 0.697 |
| eGFR (mL/min per 1.73 m2) | 84.9 (73.4; 98.75) | 88.6 (77.8; 100.4) | <0.001 |
| Uric acid (mmol/L) | 238 (198; 278) | 319 (278; 364) | <0.001 |
| Albumin i.U. (mg/L) # | 7.9 (5.6; 13.2) | 9 (6.1; 15.2) | 0.003 |
| Urinary albumin/creatinin ratio (uACR, g/g) ## | 8.9 (5.81; 16.35) | 5.87 (4.21; 11.08) | <0.001 |
| Left parenchyma volume (mL) | 144 (125; 165) | 180 (160; 203) | <0.001 |
| Women | Men | ||||
|---|---|---|---|---|---|
| Age (Years) | Median (25th, 75th) | Reference Value (5th Percentile) | Median (25th, 75th) | Reference Value (5th Percentile) | |
| Right kidney volume | 138 (121; 156) | 99 | 174 (154; 197) | 126 | |
| 22–39 | 141 (126; 160) | 106 | 172 (153; 192) | 123 | |
| 40–59 | 142 (126; 161) | 102 | 180 (162; 206) | 134 | |
| 60–81 | 129 (111; 143) | 92 | 164 (149; 184) | 123 | |
| p-value | <0.001 | <0.001 | |||
| Left kidney volume | 144 (125; 165) | 102 | 180 (160; 203) | 132 | |
| 22–39 | 150 (134; 169) | 114 | 179 (161; 200) | 129 | |
| 40–59 | 149 (128; 170) | 109 | 190 (168; 215) | 142 | |
| 60–81 | 131 (115; 148) | 93 | 168 (150; 186) | 128 | |
| p-value | <0.001 | <0.001 | |||
| Right kidney volume/BSA | 77.4 (68.8; 86.4) | 57.3 | 84.6 (77.0; 93.9) | 65.4 | |
| 22–39 | 79.6 (72.0; 88.9) | 60.0 | 84.0 (76.3; 89.9) | 64.5 | |
| 40–59 | 79.7 (71.6; 88.0) | 60.2 | 89.2 (79.3; 98.4) | 67.6 | |
| 60–81 | 71.1 (63.9; 80.1) | 53.7 | 80.4 (74.7; 88.8) | 63.8 | |
| p-value | <0.001 | <0.001 | |||
| Left kidney volume/BSA | 80.2 (71.6; 90.3) | 59.6 | 87.7 (78.9; 97.6) | 67.7 | |
| 22–39 | 84.0 (77.3; 92.6) | 63.7 | 87.2 (78.9; 95.9) | 68.4 | |
| 40–59 | 83.1 (74.2; 93.2) | 63.0 | 92.0 (82.3; 101.8) | 70.8 | |
| 60–81 | 73.3 (65.0; 81.8) | 55.2 | 82.0 (75.4; 89.8) | 64.4 | |
| p-value | <0.001 | <0.001 | |||
4. Discussion
Summary of the Main Results
- (1)
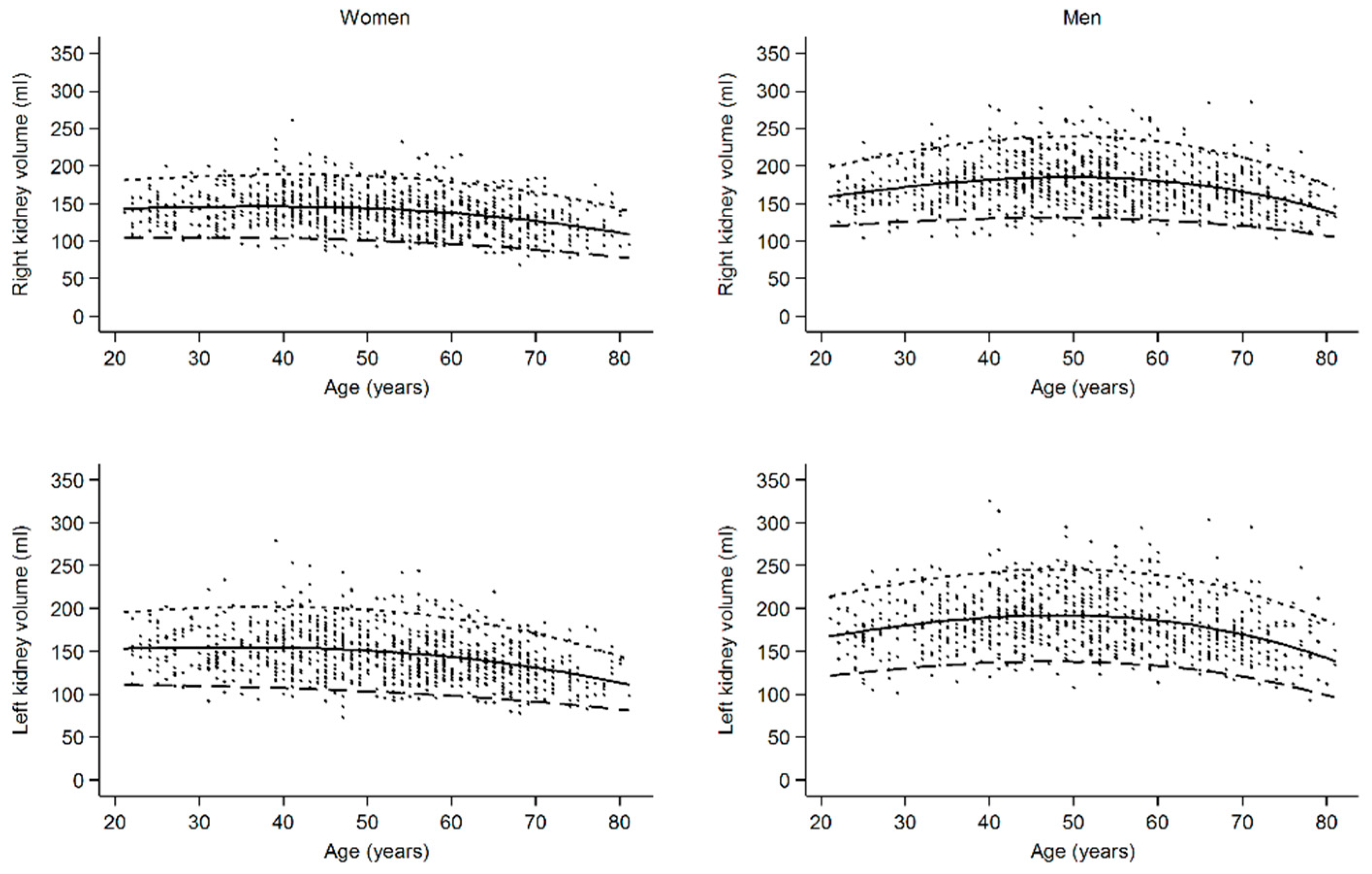
- Reference values for renal volumes are different for age groups and sex.
- (2)
- For any given age and even when indexed to BSA, female kidneys are smaller than male kidneys.
- (3)
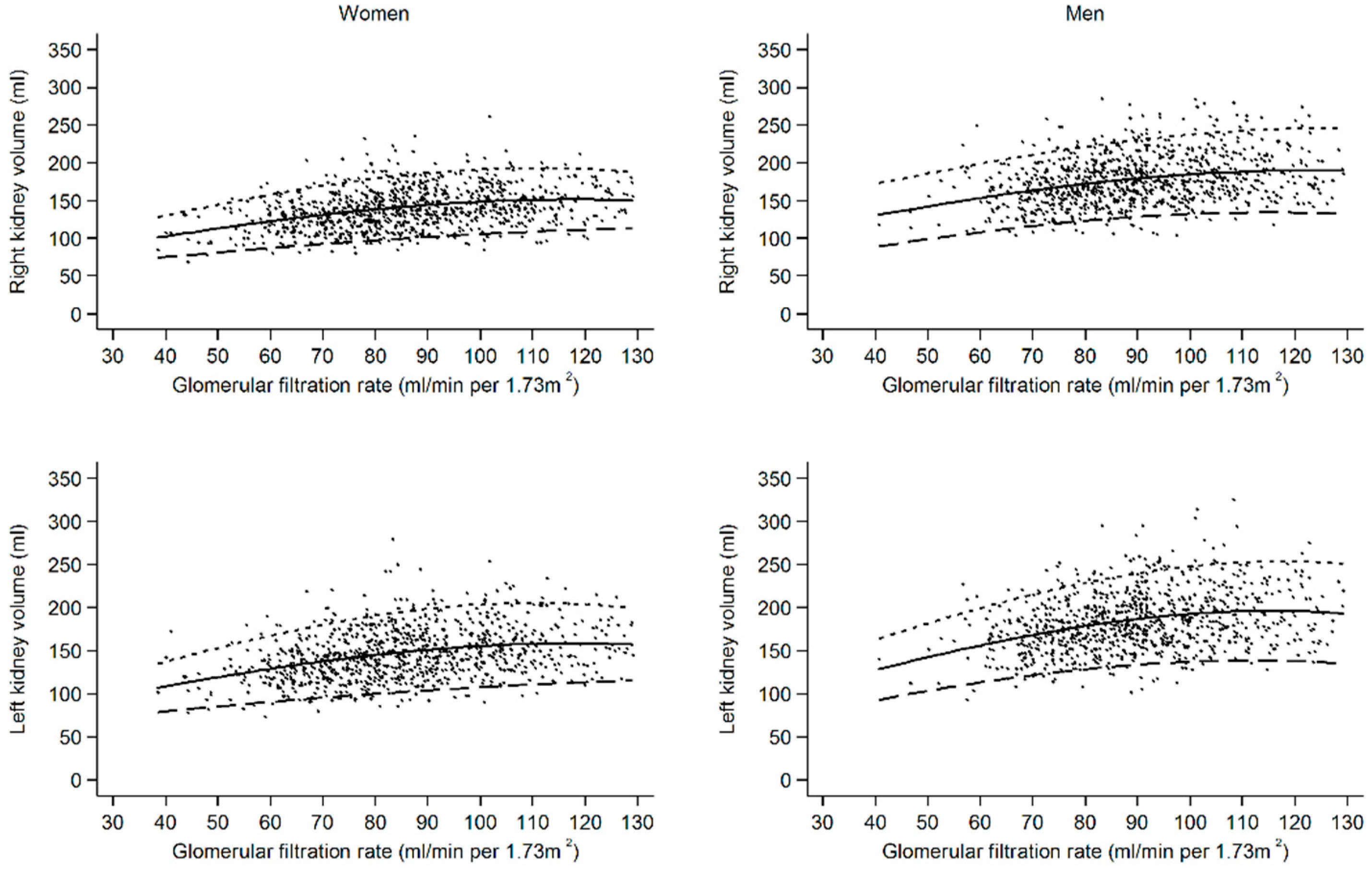
- Renal volume is associated positively with eGFR, but for any chosen eGFR, renal volume in females is lower compared to males.
- (4)
- Left kidneys are larger than right kidneys in both males and females.
- (5)
- Hypertension, diabetes, and smoking were associated with larger renal volumes.
- (6)
- Overt cardiovascular risk factor accumulation in middle-aged males serves as a potential explanation for hyperfiltration and renal hypertrophy in this group.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Michaely, H.J.; Herrmann, K.A.; Nael, K.; Oesingmann, N.; Reiser, M.F.; Schoenberg, S.O. Functional renal imaging: Nonvascular renal disease. Abdom. Imaging 2007, 32, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lanzman, R.S.; Notohamiprodjo, M.; Wittsack, H.J. Funktionelle Magnetresonanztomographie der Nieren (Functional magnetic resonance imaging of the kidneys). Radiologe 2015, 55, 1077–1087. [Google Scholar] [CrossRef] [PubMed]
- Binkert, C.A.; Hoffman, U.; Leung, D.A.; Matter, H.G.; Schmidt, M.; Debatin, J.F. Characterization of renal artery stenoses based on magnetic resonance renal flow and volume measurements. Kidney Int. 1999, 56, 1846–1854. [Google Scholar] [CrossRef]
- Michaely, H.J.; Schoenberg, S.O.; Ittrich, C.; Dikow, R.; Bock, M.; Guenther, M. Renal Disease: Value of Functional Magnetic Resonance Imaging with Flow and Perfusion Measurements. Investig. Radiol. 2004, 39, 698–705. [Google Scholar] [CrossRef]
- Van den Dool, S.W.; Wasser, M.N.; de Fijter, J.W.; van der Geest, R.J. Functional renal volume: Quantitative analysis at gadolinium-enhanced MR angiography—Feasibility study in healthy potential kidney donors. Radiology 2005, 236, 189–195. [Google Scholar] [CrossRef]
- Bakker, J.; Olree, M.; Kaatee, R.; de Lange, E.E.; Moons, K.G.; Beutler, J.J.; Beek, F.J. Renal volume measurements: Accuracy and repeatability of US compared with that of MR imaging. Radiology 1999, 211, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Di Leo, G.; Di Terlizzi, F.; Flor, N.; Morganti, A.; Sardanelli, F. Measurement of renal volume using respiratory-gated MRI in subjects without known kidney disease: Intraobserver, interobserver, and interstudy reproducibility. Eur. J. Radiol. 2001, 80, e212-6. [Google Scholar] [CrossRef]
- Cohen, E.I.; Kelly, S.A.; Edye, M.; Mitty, H.A.; Bromberg, J.S. MRI estimation of total renal volume demonstrates significant association with healthy donor weight. Eur. J. Radiol. 2009, 71, 283–287. [Google Scholar] [CrossRef]
- Cheong, B.; Muthupillai, R.; Rubin, M.F.; Flamm, S.D. Normal values for renal length and volume as measured by magnetic resonance imaging. Clin. J. Am. Soc. Nephrol. 2007, 2, 38–45. [Google Scholar] [CrossRef]
- Roseman, D.A.; Hwang, S.-J.; Oyama-Manabe, N.; Chuang, M.L.; O’Donnell, C.J.; Manning, W.J.; Fox, C.S. Clinical associations of total kidney volume: The Framingham Heart Study. Nephrol. Dial. Transplant. 2017, 32, 1344–1350. [Google Scholar] [CrossRef]
- A&B One. Kommunikationsagentur GmbH Ihre Nieren Liegen Uns am Herzen: Infobroschüre der Deutschen Gesellschaft für Nephrologie. Available online: https://www.a-b-one.de/referenzen/nephrologen (accessed on 31 October 2023).
- Girndt, M.; Trocchi, P.; Scheidt-Nave, C.; Markau, S.; Stang, A. The Prevalence of Renal Failure. Results from the German Health Interview and Examination Survey for Adults, 2008–2011 (DEGS1). Dtsch. Arztebl. Int. 2016, 113, 85–91. [Google Scholar] [CrossRef]
- Stevens, P.E.; Lein, A. Evaluation and management of chronic kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef]
- Paleologo, G.; Abdelkawy, H.; Barsotti, M.; Basha, A.; Bernabini, G.; Bianchi, A.; Caprio, F.; Emad, A.; Grassi, G.; Nerucci, B.; et al. Kidney dimensions at sonography are correlated with glomerular filtration rate in renal transplant recipients and in kidney donors. Transplant. Proc. 2007, 39, 1779–1781. [Google Scholar] [CrossRef]
- Johnson, S.; Rishi, R.; Andone, A.; Khawandi, W.; Al-Said, J.; Gletsu-Miller, N.; Lin, L.; Baumgarten, D.A.; O’Neill, W.C. Determinants and functional significance of renal parenchymal volume in adults. Clin. J. Am. Soc. Nephrol. 2011, 6, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Vrtiska, T.J.; Avula, R.T.; Walters, L.R.; Chakkere, H.A.; Kremers, W.K.; Lerman, L.O.; Rule, A.D. Age, kidney function, and risk factors associate differently with cortical and medullary volumes of the kidney. Kidney Int. 2014, 85, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Donadio, C.; Abdelkawy, H.; Grassi, G. Echographic renal dimensions can predict glomerular filtration rate of potential living kidney donors. Transpl. Proc. 2010, 42, 1035–1039. [Google Scholar] [CrossRef]
- Völzke, H.; Schössow, J.; Schmidt, C.O.; Jürgens, C.; Richter, A.; Werner, A.; Werner, N.; Radke, D.; Teumer, A.; Ittermann, T.; et al. Cohort Profile Update: The Study of Health in Pomerania (SHIP). Int. J. Epidemiol. 2022, 51, e372–e383. [Google Scholar] [CrossRef]
- Schmidt, C.O.; Sierocinski, E.; Hegenscheid, K.; Baumeister, E.; Grabe, H.J.; Völzke, H. Impact of whole-body MRI in a general population study. Eur. J. Epidemiol. 2016, 31, 31–39. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Caps, M.T.; Zierler, R.E.; Polissar, N.L.; Bergelin, R.O.; Beach, K.W.; Cantwell-Gab, K.; Casadei, A.; Davidson, R.C.; Strandness, D.E., Jr. Risk of Atrophy in Kidneys with Atherosclerotic Renal Artery Stenosis. Kidney Int. 1998, 160, 952–953. [Google Scholar] [CrossRef]
- Buturović-Ponikvar, J.; Višnar-Perovič, A. Ultrasonography in chronic renal failure. Eur. J. Radiol. 2003, 46, 115–122. [Google Scholar] [CrossRef]
- Luyckx, V.A.; Rule, A.D.; Tuttle, K.R.; Delanaye, P.; Liapis, H.; Gandjour, A.; Romagnani, P.; Anders, H.-J. Nephron overload as a therapeutic target to maximize kidney lifespan. Nat. Rev. Nephrol. 2021, 18, 171–183. [Google Scholar] [CrossRef]
- Van der Sande, N.G.C.; Visseren, F.L.J.; van der Graaf, Y.; Nathoe, H.M.; de Borst, G.J.; Leiner, T.; Blankestijn, P.J.; SMART Study Group. Relation between Kidney Length and Cardiovascular and Renal Risk in High-Risk Patients. Clin. J. Am. Soc. Nephrol. 2017, 12, 921–928. [Google Scholar] [CrossRef][Green Version]
- Woodard, T.; Sigurdsson, S.; Gotal, J.D.; Torjesen, A.A.; Inker, L.A.; Aspelund, T.; Eiriksdottir, G.; Gudnason, V.; Harris, T.B.; Launer, L.J.; et al. Segmental kidney volumes measured by dynamic contrast-enhanced magnetic resonance imaging and their association with CKD in older people. Am. J. Kidney Dis. 2014, 65, 41–48. [Google Scholar] [CrossRef]
- Saran, A.M.; Hsu, F.-C.; Lohman, K.K.; Carr, J.J.; Bowden, D.W.; Wagenknecht, L.E.; Freedman, B.I. Kidney volume associations with subclinical renal and cardiovascular disease: The Diabetes Heart Study. Am. J. Nephrol. 2008, 28, 366–371. [Google Scholar] [CrossRef]
- Gourtsoyiannis, N.; Prassopoulos, P.; Cavouras, D.; Pantelidis, N. The thickness of the renal parenchyma decreases with age: A CT study of 360 patients. Am. J. Roentgenol. 1990, 155, 541–544. [Google Scholar] [CrossRef]
- Cheung, C.M.; Shurrab, A.E.; Buckley, D.L.; Hegarty, J.; Middleton, R.J.; Mamtora, H.; Kalra, P.A. MR-derived renal morphology and renal function in patients with atherosclerotic renovascular disease. Kidney Int. 2006, 69, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Neuhauser, H.; Diederichs, C.; Boeing, H.; Felix, S.B.; Jünger, C.; Lorbeer, R.; Meisinger, C.; Peters, A.; Völzke, H.; Weikert, C.; et al. Hypertension in Germany. Dtsch. Arztebl. Int. 2016, 113, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Päivänsalo, M.J.; Merikanto, J.; Savolainen, M.J.; Lilja, M.; Rantala, A.O.; Kauma, H.; Reunanen, A.; Kesäniemi, Y.A.; Suramo, I. Effect of hypertension, diabetes and other cardiovascular risk factors on kidney size in middle-aged adults. Clin. Nephrol. 1998, 50, 161–168. [Google Scholar] [PubMed]
- Maeda, I.; Hayashi, T.; Sato, K.K.; Koh, H.; Harita, N.; Nakamura, Y.; Endo, G.; Kambe, H.; Fukuda, K. Cigarette smoking and the association with glomerular hyperfiltration and proteinuria in healthy middle-aged men. Clin. J. Am. Soc. Nephrol. 2011, 6, 2462–2469. [Google Scholar] [CrossRef] [PubMed]
- Noborisaka, Y.; Ishizaki, M.; Yamada, Y.; Honda, R.; Yokoyama, H.; Miyao, M.; Tabata, M. The effects of continuing and discontinuing smoking on the development of chronic kidney disease (CKD) in the healthy middle-aged working population in Japan. Environ. Health Prev. Med. 2013, 18, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Fassett, R.G.; Venuthurupalli, S.K.; Gobe, G.C.; Coombes, J.S.; Cooper, M.A.; Hoy, W.E. Biomarkers in chronic kidney disease: A review. Kidney Int. 2011, 80, 806–821. [Google Scholar] [CrossRef] [PubMed]
- Siu, Y.-P.; Leung, K.-T.; Tong, M.K.-H.; Kwan, T.-H. Use of allopurinol in slowing the progression of renal disease through its ability to lower serum uric acid level. Am. J. Kidney Dis. 2006, 47, 51–59. [Google Scholar] [CrossRef] [PubMed]



| Right Kidney Volume | Left Kidney Volume | |||
|---|---|---|---|---|
| Risk Factor | β (95% CI) | p-Value | β (95% CI) | p-Value |
| Men | 8.97 (5.91; 12.03) | <0.001 | 9.43 (6.1; 12.75) | <0.001 |
| Age | 0.10 (0.00; 0.19) | 0.049 | 0.00 (−0.11; 0.10) | 0.948 |
| Smoking status | ||||
| Never smoker | Ref | Ref | ||
| Ex-smoker | 2.31 (−0.12; 4.75) | 0.063 | 1.93 (−0.72; 4.59) | 0.153 |
| Current smoker | 14.96 (12.12; 17.79) | <0.001 | 16.03 (12.94; 19.11) | <0.001 |
| Body surface area | 97.66 (90.4; 104.93) | <0.001 | 100.55 (92.64; 108.47) | <0.001 |
| Systolic BP | 0.00 (−0.10; 0.10) | 0.996 | −0.02 (−0.13; 0.08) | 0.648 |
| Diastolic BP | 0.17 (0.01; 0.32) | 0.032 | 0.22 (0.05; 0.39) | 0.011 |
| Diabetes mellitus (Typ-2) | 5.60 (1.31; 9.90) | 0.011 | 3.99 (−0.69; 8.67) | 0.095 |
| HDL-C | −4.55 (−7.88; −1.23) | 0.007 | −3.22 (−6.84; 0.40) | 0.081 |
| LDL-C | 0.35 (−0.82; 1.51) | 0.559 | 0.31 (−0.95; 1.58) | 0.629 |
| Glomerular filtration rate | 0.57 (0.5; 0.65) | <0.001 | 0.54 (0.46; 0.62) | <0.001 |
| Uric acid | −0.03 (−0.05; −0.01) | 0.001 | −0.04 (−0.06; −0.02) | <0.001 |
| Age Groups (Years) | ||||
|---|---|---|---|---|
| 22–39 | 40–59 | 60–81 | ||
| Parameter | n = 384 | n = 888 | n = 543 | p-Value * |
| Men | 199 (51.8%) | 420 (47.3%) | 266 (49%) | 0.331 |
| Smoking status | <0.001 | |||
| Never-smoker | 140 (36.7%) | 312 (35.2%) | 255 (47.1%) | |
| Ex-smoker | 101 (26.4%) | 333 (37.5%) | 244 (45%) | |
| Current smoker | 141 (36.9%) | 242 (27.3%) | 43 (7.9%) | |
| Body mass index (kg/m2) | 24.9 (22.7; 28.1) | 27.3 (24.4; 30.4) | 28.8 (26.3; 31.8) | <0.001 |
| Body surface area (m2) | 1.92 (1.78; 2.06) | 1.92 (1.76; 2.07) | 1.91 (1.76; 2.06) | 0.617 |
| Systolic BP (mmHg) | 119 (109; 131) | 125 (113; 137) | 132 (123; 144) | <0.001 |
| Diastolic BP (mmHg) | 74 (68; 80) | 79 (72; 85) | 77 (71; 83) | <0.001 |
| Hypertension | 53 (13.9%) | 357 (40.3%) | 374 (69%) | <0.001 |
| Diabetes mellitus (Typ-2) | 4 (1%) | 38 (4.3%) | 89 (16.4%) | <0.001 |
| HbA1c (%) | 5.0 (4.7; 5.3) | 5.2 (4.9; 5.5) | 5.5 (5.2; 5.8) | <0.001 |
| HDL-C (mmol/L) | 1.41 (1.17; 1.66) | 1.42 (1.2; 1.7) | 1.40 (1.17; 1.69) | 0.201 |
| LDL-C (mmol/L) | 2.96 (2.38; 3.54) | 3.52 (2.94; 4.07) | 3.45 (2.84; 4.11) | <0.001 |
| eGFR (mL/min per 1.73 m2) | 95.2 (86.45; 107.8) | 88.4 (78.5; 100.5) | 76.3 (67.3; 87) | <0.001 |
| Uric acid (mmol/L) | 263 (216.5; 308) | 275 (222; 328) | 294.5 (247; 352) | <0.001 |
| Albumin i.U. (mg/L) | 8.1 (6; 13) | 8.1 (5.6; 12.7) | 9.8 (6.3; 20.1) | <0.001 |
| Right parenchyma volume (mL) | 156 (138; 179) | 160 (137; 185) | 146 (124; 168) | <0.001 |
| Left parenchyma volume (mL) | 166 (144; 186) | 167 (143; 194) | 148 (128; 172) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dabers, T.; Sass, P.; Fechner, F.; Weyer, J.; Völzke, H.; Mahnken, A.H.; Lorbeer, R.; Mensel, B.; Stracke, S. Age- and Sex-Specific Reference Values for Renal Volume and Association with Risk Factors for Chronic Kidney Disease in a General Population—An MRI-Based Study. J. Clin. Med. 2024, 13, 769. https://doi.org/10.3390/jcm13030769
Dabers T, Sass P, Fechner F, Weyer J, Völzke H, Mahnken AH, Lorbeer R, Mensel B, Stracke S. Age- and Sex-Specific Reference Values for Renal Volume and Association with Risk Factors for Chronic Kidney Disease in a General Population—An MRI-Based Study. Journal of Clinical Medicine. 2024; 13(3):769. https://doi.org/10.3390/jcm13030769
Chicago/Turabian StyleDabers, Thomas, Peter Sass, Fritz Fechner, Julian Weyer, Henry Völzke, Andreas Horst Mahnken, Roberto Lorbeer, Birger Mensel, and Sylvia Stracke. 2024. "Age- and Sex-Specific Reference Values for Renal Volume and Association with Risk Factors for Chronic Kidney Disease in a General Population—An MRI-Based Study" Journal of Clinical Medicine 13, no. 3: 769. https://doi.org/10.3390/jcm13030769
APA StyleDabers, T., Sass, P., Fechner, F., Weyer, J., Völzke, H., Mahnken, A. H., Lorbeer, R., Mensel, B., & Stracke, S. (2024). Age- and Sex-Specific Reference Values for Renal Volume and Association with Risk Factors for Chronic Kidney Disease in a General Population—An MRI-Based Study. Journal of Clinical Medicine, 13(3), 769. https://doi.org/10.3390/jcm13030769