
Comparison of Tooth Size Measurements in Orthodontics Using Conventional and 3D Digital Study Models

 and
and
Abstract
1. Introduction
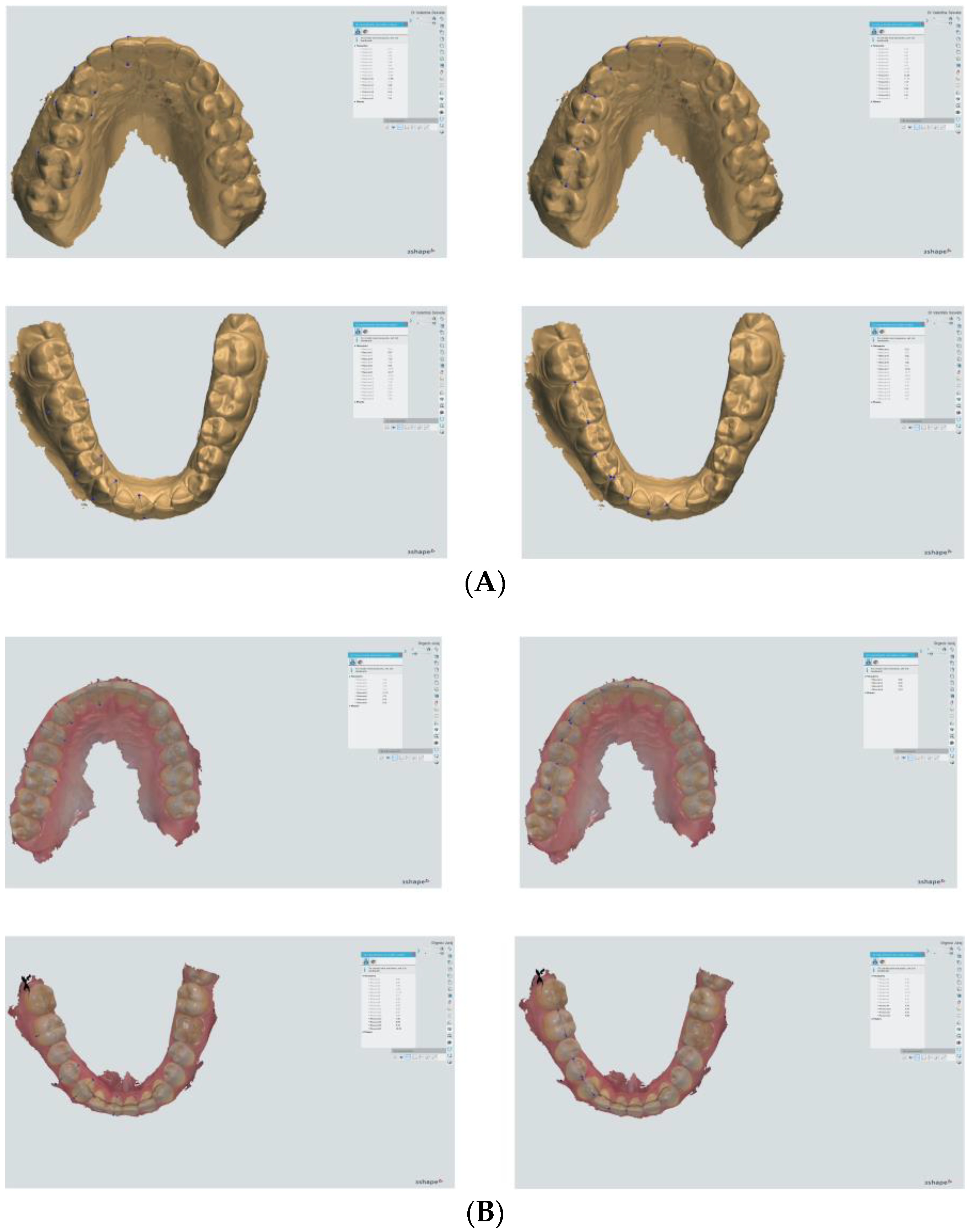
2. Materials and Methods
3. Results
3.1. Reproducibility of Measurements
3.2. Comparison of Methods for Measuring Molar Dimensions
3.2.1. MD Width of Tooth 16
3.2.2. BL Width of Tooth 16
3.2.3. MD Width of Tooth 46
3.2.4. BL Width of Tooth 46
3.3. Comparison of Methods for Measuring Premolar Dimensions
3.3.1. MD Width of Tooth 14
3.3.2. BL Width of Tooth 14
3.3.3. MD Width of Tooth 44
3.3.4. BL Width of Tooth 44
3.4. Comparison of Methods for Measuring Canine Dimensions
3.4.1. MD Width of Tooth 13
3.4.2. BL Width of Tooth 13
3.4.3. MD Width of Tooth 43
3.4.4. BL Width of Tooth 43
3.5. Comparison of Methods for Measuring Incisor Dimensions
3.5.1. MD Width of Tooth 11
3.5.2. BL Width of Tooth 11
3.5.3. MD Width of Tooth 41
3.5.4. BL Width of Tooth 41
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Naidu, D.; Freer, T.J. Validity, reliability, and reproducibility of the iOC intraoral scanner: A comparison of tooth widths and Bolton ratios. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, N.D.; Groth, C.; Jones, P.E.; Graham, J.W.; Redmond, W.R. Intraoral digital scanners. J. Clin. Orthod. 2014, 48, 337–347. [Google Scholar]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C. Diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 161–170. [Google Scholar] [CrossRef]
- Reuschl, R.; Heuer, W.; Stiesch, M.; Wenzel, D.; Dittmer, M. Reliability and validity of measurements on digital study models and plaster models. Eur. J. Orthod. 2016, 38, 22–26. [Google Scholar] [CrossRef]
- Kardach, H.; Szponar-Zurowska, A.; Biedziak, B.A. Comparison of Teeth Measurements on Plaster and Digital Models. J. Clin. Med. 2023, 12, 943. [Google Scholar] [CrossRef] [PubMed]
- Wiranto, M.; Engelbrecht, W.; Nolthenius, H.; van der Meer, W.; Ren, Y. Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Santoro, M.; Galkin, S.; Teredesai, M.; Nicolay, O.; Cangialosi, T. Comparison of measurements made on digital and plaster models. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 101–105. [Google Scholar] [CrossRef]
- Camardella, L.T.; Ongkosuwito, E.M.; Penning, E.W.; Kuijpers-Jagtman, A.M.; Vilella, O.V.; Breuning, K.H. Accuracy and reliability of measurements performed using two different software programs on digital models generated using laser and computed tomography plaster model scanners. Korean J. Orthod. 2020, 50, 13–25. [Google Scholar] [CrossRef]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2020, 64, 109–113. [Google Scholar] [CrossRef]
- Mohammed Alassiry, A. Clinical aspects of digital three-dimensional intraoral scanning in orthodontics—A systematic review. Saudi. Dent. J. 2023, 35, 437–442. [Google Scholar] [CrossRef]
- Fleming, P.; Marinho, V.; Johal, A. Orthodontic measurements on digital study models compared with plaster models: A systematic review. Orthod. Craniofac. Res. 2011, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- De Luca Canto, G.; Pachêco-Pereira, C.; Lagravere, M.O.; Flores-Mir, C.; Major, P.W. Intra-arch dimensional measurement validity of laser-scanned digital dental models compared with the original plaster models: A systematic review. Orthod. Craniofac. Res. 2015, 18, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Aragón, M.L.; Pontes, L.F.; Bichara, L.M.; Flores-Mir, C.; Normando, D. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: A systematic review. Eur. J. Orthod. 2016, 38, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Luu, N.S.; Nikolcheva, L.G.; Retrouvey, J.M.; Flores-Mir, C.; El-Bialy, T.; Carey, J.P.; Major, P.W. Linear measurements using virtual study models. Angle Orthod. 2012, 82, 1098–1106. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.; Ayoub, A.F.; Siebert, P. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J. Orthod. 2003, 30, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Zilberman, O.; Huggare, J.; Parikakis, K. Evaluation of the validity of tooth size and arch width measurements using conventional and three- dimentional virtual orthodontic models. Angle Orthod. 2003, 73, 301–306. [Google Scholar] [PubMed]
- Park, S.H.; Byun, S.H.; Oh, S.H.; Lee, H.L.; Kim, J.W.; Yang, B.E.; Park, I.Y. Evaluation of the Reliability, Reproducibility and Validity of Digital Orthodontic Measurements Based on Various Digital Models among Young Patients. J. Clin. Med. 2020, 9, 2728. [Google Scholar] [CrossRef] [PubMed]
- Mullen, S.; Martin, C.; Ngan, P.; Gladwin, M. Accuracy of space analysis with emodels and plaster models. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 346–352. [Google Scholar] [CrossRef]
- Watanabe-Kanno, G.; Abrao, J.; Miasiro Junior, H.; Sanchez-Ayala, A.; Lagravere, M. Reproducibility, reliability and validity of measurements obtained from Cecile3 digital models. Braz. Oral Res. 2009, 23, 288–295. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef]
- Schmalzl, J.; Róth, I.; Borbély, J.; Hermann, P.; Vecsei, B. The impact of software updates on accuracy of intraoral scanners. BMC Oral Health 2023, 23, 219. [Google Scholar] [CrossRef]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef]
- Leifert, M.F.; Leifert, M.M.; Efstratiadis, S.S.; Cangialosi, T.J. Comparison of space analysis evaluations with digital models and plaster dental casts. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 16.e1–16.e4. [Google Scholar] [CrossRef]
- Joffe, L. OrthoCAD: Digital models for a digital era. J. Orthod. 2004, 31, 344–347. [Google Scholar] [CrossRef]
- Torassian, G.; Kau, C.H.; English, J.D.; Powers, J.; Bussa, H.I.; Marie Salas-Lopez, A.; Corbett, J.A. Digital models vs. plaster models using alginate and alginate substitute materials. Angle Orthod. 2010, 80, 474–481. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, H.L.; Park, I.Y.; On, S.W.; Byun, S.H.; Yang, B.E. Effectiveness of creating digital twins with different digital dentition models and cone-beam computed tomography. Sci. Rep. 2023, 13, 10603. [Google Scholar] [CrossRef]
- Sayed, M.E.; Al-Mansour, H.; Alshehri, A.H.; Al-Sanabani, F.; Al-Makramani, B.M.A.; Mugri, M.H.; Ahmed, W.M.; Alqahtani, N.M.; Bukhary, D.M.; Alsurayyie, F.H.; et al. Accuracy of Master Casts Generated Using Conventional and Digital Impression Modalities: Part 2—The Full Arch Dimension. Appl. Sci. 2022, 12, 2148. [Google Scholar] [CrossRef]
- Alcan, T.; Ceylanoglu, C.; Baysal, B. The relationship between digital model accuracy and time-dependent deformation of alginate impressions. Angle Orthod. 2009, 79, 30–36. [Google Scholar] [CrossRef]
- Mao, Z.; Jia, Y.F.; Zhang, Y.F.; Xu, J.; Wu, Z.N.; Mao, F.; Zhang, Y.; Hu, M. Evaluation of the impact of reference tooth morphology and alignment on model measurement accuracy. Ann. Transl. Med. 2022, 10, 670. [Google Scholar] [CrossRef]
- Dalstra, M.; Melsen, B. From alginate impressions to digital virtual models: Accuracy and reproducibility. J. Orthod. 2009, 36, 36–41. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Intraoral Scan (IOS) | Digitized Plaster Model after Alginate Impression (DPMA) | Digitized Plaster Model after Silicone Impression (DPMS) | Plaster Model (PM) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Mean ± SD | p * | Dahlberg | Mean ± SD | p * | Dahlberg | Mean ± SD | p * | Dahlberg | Mean ± SD | p * | Dahlberg |
| MD 16 | 0.02 ± 0.05 | 0.434 | 0.01 | −0.12 ± 0.19 | 0.251 | 0.04 | −0.03 ± 0.06 | 0.264 | 0.01 | 0.06 ± 0.05 | 0.07 | 0.02 |
| MD 14 | −0.01 ± 0.05 | 0.81 | 0.00 | −0.04 ± 0.07 | 0.27 | 0.01 | 0.00 ± 0.05 | 0.874 | 0.00 | 0.06 ± 0.05 | 0.07 | 0.02 |
| MD 13 | 0.01 ± 0.05 | 0.603 | 0.00 | −0.03 ± 0.06 | 0.276 | 0.01 | −0.04 ± 0.05 | 0.152 | 0.01 | 0.02 ± 0.08 | 0.621 | 0.01 |
| MD 11 | 0.01 ± 0.03 | 0.485 | 0.00 | −0.06 ± 0.01 | <0.001 | 0.02 | −0.03 ± 0.05 | 0.212 | 0.01 | 0.02 ± 0.08 | 0.621 | 0.01 |
| BL16 | −0.05 ± 0.04 | 0.079 | 0.01 | −0.04 ± 0.04 | 0.089 | 0.01 | −0.04 ± 0.03 | 0.072 | 0.01 | −0.02 ± 0.04 | 0.374 | 0.01 |
| BL 14 | −0.03 ± 0.05 | 0.251 | 0.01 | 0.00 ± 0.07 | 0.954 | 0.00 | −0.01 ± 0.06 | 0.835 | 0.00 | −0.02 ± 0.08 | 0.621 | 0.01 |
| BL 13 | −0.03 ± 0.04 | 0.194 | 0.01 | −0.06 ± 0.06 | 0.115 | 0.02 | −0.03 ± 0.04 | 0.164 | 0.01 | −0.04 ± 0.05 | 0.178 | 0.01 |
| BL 11 | −0.05 ± 0.08 | 0.257 | 0.02 | −0.02 ± 0.06 | 0.567 | 0.01 | −0.01 ± 0.03 | 0.363 | 0.00 | 0.00 ± 0.07 | 1 | 0.00 |
| Intraoral Scan (IOS) | Digitized Plaster Model after Alginate Impression (DPMA) | Digitized Plaster Model after Silicone Impression (DPMS) | Plaster Model (PM) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Mean ± SD | p * | Dahlberg | Mean ± SD | p * | Dahlberg | Mean ± SD | p * | Dahlberg | Mean ± SD | p * | Dahlberg |
| MD 16 | 0.21 ± 0.20 | 0.085 | 0.07 | 0.36 ± 0.24 | 0.028 | 0.11 | −0.03 ± 0.09 | 0.517 | 0.01 | 0.02 ± 0.04 | 0.374 | 0.01 |
| MD 14 | 0.31 ± 0.18 | 0.017 | 0.10 | 0.12 ± 0.28 | 0.385 | 0.04 | 0.02 ± 0.08 | 0.655 | 0.01 | 0.00 ± 0.00 | 1 | 0.00 |
| MD 13 | 0.32 ± 0.28 | 0.063 | 0.10 | −0.02 ± 0.22 | 0.879 | 0.01 | −0.02 ± 0.07 | 0.533 | 0.01 | 0.00 ± 0.07 | 1 | 0.00 |
| MD 11 | 0.02 ± 0.10 | 0.728 | 0.01 | −0.03 ± 0.20 | 0.784 | 0.01 | 0.01 ± 0.07 | 0.773 | 0.00 | −0.12 ± 0.18 | 0.208 | 0.04 |
| BL16 | −0.36 ± 0.20 | 0.017 | 0.11 | −0.12 ± 0.20 | 0.245 | 0.04 | −0.01 ± 0.06 | 0.826 | 0.00 | 0.00 ± 0.00 | 1 | 0.00 |
| BL 14 | −0.06 ± 0.26 | 0.64 | 0.02 | 0.07 ± 0.33 | 0.661 | 0.02 | 0.02 ± 0.05 | 0.394 | 0.01 | 0.00 ± 0.00 | 1 | 0.00 |
| BL 13 | 0.40 ± 0.20 | 0.011 | 0.13 | 0.21 ± 0.13 | 0.022 | 0.07 | 0.01 ± 0.04 | 0.711 | 0.00 | −0.00 ± 0.00 | 1 | 0.00 |
| BL 11 | 0.31 ± 0.14 | 0.008 | 0.10 | 0.44 ± 0.21 | 0.009 | 0.14 | 0.04 ± 0.05 | 0.178 | 0.01 | −0.02 ± 0.04 | 0.374 | 0.01 |
| Parameter | IOS AS * ± SD | DPMA AS * ± SD | DPMS AS * ± SD | PM AS * ± SD | p ** | η2 *** |
|---|---|---|---|---|---|---|
| 16 MD | 10.40 a ± 0.64 | 10.47 ab ± 0.62 | 10.56 b ± 0.70 | 10.24 bc ± 0.67 | 0.001 | 0.214 |
| 16 BL | 6.72 a ± 0.49 | 6.53 a ± 0.49 | 6.61 a ± 0.56 | 7.21 b ± 0.61 | <0.001 | 0.429 |
| 46 MD | 10.89 a ± 0.62 | 10.98 ab ± 0.56 | 11.00 b ± 0.65 | 10.69 c ± 0.72 | <0.001 | 0.320 |
| 46 BL | 5.66 a ± 0.49 | 5.41 b ± 0.50 | 5.52 a ± 0.42 | 6.89 c ± 1.34 | <0.001 | 0.537 |
| 14 MD | 7.22 a ± 0.40 | 7.28 a ± 0.35 | 7.29 a ± 0.41 | 6.79 b ± 0.49 | <0.001 | 0.465 |
| 14 BL | 5.87 a ± 0.40 | 5.75 b ± 0.37 | 5.80 ab ± 0.42 | 6.01 a ± 0.58 | 0.023 | 0.136 |
| 44 MD | 7.01 ± 0.41 | 7.00 ± 0.40 | 7.01 ± 0.42 | 6.93 ± 0.53 | 0.143 | 0.066 |
| 44 BL | 4.67 ± 0.39 | 4.42 ± 0.43 | 4.40 ± 0.40 | 4.69 ± 1.03 | 0.134 | 0.073 |
| 13 MD | 8.11 a ± 0.41 | 8.21 a ± 0.39 | 8.22 a ± 0.38 | 7.89 b ± 0.47 | <0.001 | 0.316 |
| 13 BL | 7.40 a ± 0.41 | 7.62 b ± 0.47 | 7.84 c ± 0.43 | 7.06 a ± 0.70 | <0.001 | 0.446 |
| 43 MD | 6.94 a ± 0.37 | 7.05 a ± 0.33 | 7.07 a ± 0.34 | 6.74 b ± 0.43 | <0.001 | 0.390 |
| 43 BL | 6.71 a ± 0.50 | 6.98 b ± 0.55 | 7.19 c ± 0.49 | 6.68 ab ± 0.86 | <0.001 | 0.310 |
| 11 MD | 8.71 a ± 0.53 | 8.77 a ± 0.51 | 8.74 a ± 0.52 | 8.46 b ± 0.64 | 0.001 | 0.285 |
| 11 BL | 6.61 a ± 0.44 | 6.73 a ± 0.49 | 7.06 b ± 0.45 | 6.25 c ± 0.65 | <0.001 | 0.480 |
| 41 MD | 5.41 a ± 0.28 | 5.51 b ± 0.32 | 5.56 b ± 0.33 | 5.41 ab ± 0.37 | 0.016 | 0.135 |
| 41 BL | 5.51 a ± 0.44 | 5.74 b ± 0.38 | 6.06 c ± 0.35 | 5.46 ab ± 0.91 | <0.001 | 0.338 |
| Parameter | ICC (95% CI) | ME * | Mean Difference (95% CI) | p |
|---|---|---|---|---|
| 16 MD | ||||
| PM-IOS | 0.705 (0.468–0.848) | 0.35 | −0.16 (−0.34–0.03) | 0.087 |
| PM-DPMA | 0.725 (0.439–0.868) | 0.31 | −0.24 (−0.40–(−0.07)) | 0.006 |
| PM-DPMS | 0.674 (0.294–0.850) | 0.35 | −0.33 (−0.51–(−0.15)) | 0.001 |
| 16 BL | ||||
| PM-IOS | 0.149 (−0.092–0.481) ns | 0.47 | 0.50 (0.24–0.75) | <0.001 |
| PM-DPMA | 0.243 (−0.095–0.554) | 0.42 | 0.68 (0.46–0.91) | <0.001 |
| PM-DPMS | 0.251 (−0.078–0.549) | 0.46 | 0.61 (0.36–0.85) | <0.001 |
| 46 MD | ||||
| PM-IOS | 0.781 (0.591–0.912) | 0.27 | −0.20 (−0.34–(−0.05)) | 0.008 |
| PM-DPMA | 0.797 (0.309–0.925) | 0.23 | −0.29 (−0.41–(−0.17)) | <0.001 |
| PM-DPMS | 0.798 (0.276–0.927) | 0.24 | −0.31 (−0.44–(−0.19)) | <0.001 |
| 46 BL | ||||
| PM-IOS | 0.139 (−0.101–0.412) ns | 0.88 | 1.24 (0.77–1.70) | <0.001 |
| PM-DPMA | 0.106 (−0.096–0.358) ns | 0.89 | 1.48 (1.00–1.95) | <0.001 |
| PM-DPMS | 0.100 (−0.101–0.519) ns | 0.89 | 1.37 (0.90–1.84) | <0.001 |
| Parameter | ICC (95% CI) | ME * | Mean Difference (95% CI) | p |
|---|---|---|---|---|
| 14 MD | ||||
| PM-IOS | 0.337 (0.031–0.639) | 0.39 | −0.43 (−0.61–(−0.26)) | <0.001 |
| PM-DPMA | 0.448 (0.110–0.693) | 0.34 | −0.49 (−0.66–(−0.32)) | <0.001 |
| PM-DPMS | 0.439 (0.115–0.683) | 0.37 | −0.50 (−0.66–(−0.34)) | <0.001 |
| 14 BL | ||||
| PM-IOS | 0.232 (−0.080–0.522) | 0.47 | 0.14 (−0.07–0.34) | 0.186 |
| PM-DPMA | 0.234 (−0.072–0.522) | 0.48 | 0.26 (0.07–0.44) | 0.007 |
| PM-DPMS | 0.190 (−0.098–0.463) | 0.44 | 0.21 (0.02–0.40) | 0.035 |
| 44 MD | ||||
| PM-IOS | 0.680 (0.433–0.833) | 0.27 | −0.08 (−0.22–0.06) | 0.263 |
| PM-DPMA | 0.659 (0.401–0.821 | 0.27 | −0.07 (−0.22–0.07) | 0.309 |
| PM-DPMS | 0.744 (0.515–0.872) | 0.23 | −0.13 (−0.25–(−0.01)) | 0.035 |
| 44 BL | ||||
| PM-IOS | 0.039 (−0.336–0.395) ns | 0.75 | 0.02 (−0.38–0.42) | 0.918 |
| PM-DPMA | 0.032 (−0.313–0.376) ns | 0.77 | 0.27 (−0.13–0.67) | 0.181 |
| PM-DPMS | 0.016 (−0.324–0.361) ns | 0.76 | 0.29 (−0.12–0.69) | 0.156 |
| Parameter | ICC (95% CI) | ME * | Mean Difference (95% CI) | p |
|---|---|---|---|---|
| 13 MD | ||||
| PM-IOS | 0.550 (0.201–0.766) | 0.28 | −0.22 (−0.37–(−0.08)) | 0.004 |
| PM-DPMA | 0.426 (0.017–0.698 | 0.29 | −0.33 (−0.48–(−0.17)) | <0.001 |
| PM-DPMS | 0.42 (0.003–0.698) | 0.29 | −0.34 (−0.49–(−0.18)) | <0.001 |
| 13 BL | ||||
| PM-IOS | 0.324 (0.117–0.547) | 0.38 | −0.34 (−0.61–(−0.07)) | 0.015 |
| PM-DPMA | 0.192 (−0.120–0.491) | 0.51 | −0.57 (0.85–(−0.29)) | <0.001 |
| PM-DPMS | 0.151 (−0.112–0.433) | 0.53 | −0.79 (−1.06-(−0.52)) | <0.001 |
| 43 MD | ||||
| PM-IOS | 0.530 (0.184–0.753) | 0.26 | −0.20 (−0.34–(−0.07)) | 0.004 |
| PM-DPMA | 0.526 (−0.027–0.795) | 0.21 | −0.31 (−0.43–(−0.20)) | <0.001 |
| PM-DPMS | 0.544 (−0.059–0.816) | 0.20 | −0.33 (−0.44–(−0.23)) | <0.001 |
| 43 BL | ||||
| PM-IOS | 0.542 (0.227–0.753) | 0.48 | −0.03 (−0.29–0.22) | 0.786 |
| PM-DPMA | 0.528 (0.211–0.744) | 0.47 | −0.30 (0.55–0.05) | 0.019 |
| PM-DPMS | 0.405 (0.021–0.677) | 0.49 | −0.51 (−0.77–0.25) | <0.001 |
| Parameter | ICC (95% CI) | ME * | Mean Difference (95% CI) | p |
|---|---|---|---|---|
| 11 MD | ||||
| PM-IOS | 0.647 (0.327–0.824) | 0.32 | −0.25 (−0.42–(−0.08)) | 0.006 |
| PM-DPMA | 0.661 (0.214–0.851) | 0.29 | −0.31 (−0.46–(−0.16)) | <0.001 |
| PM-DPMS | 0.647 (0.271–0.833) | 0.31 | −0.28 (−0.45–(−0.12)) | 0.001 |
| 11 BL | ||||
| PM-IOS | 0.232 (−0.080–0.522) | 0.47 | −0.35 (−0.60–(−0.10)) | 0.007 |
| PM-DPMA | 0.234 (−0.072–0.522) | 0.48 | −0.48 (−0.73–(−0.22)) | 0.001 |
| PM-DPMS | 0.190 (−0.098–0.463) | 0.44 | −0.80 (−1.03–(−0.57)) | <0.001 |
| 41 MD | ||||
| PM-IOS | 0.625 (0.342–0.803) | 0.21 | 0.00 (−0.11–0.11) | 0.985 |
| PM-DPMA | 0.640 (0.370–0.810) | 0.20 | −0.10 (−0.21–0.01) | 0.067 |
| PM-DPMS | 0.353 (0.023–0.622) | 0.28 | −0.15 (−0.30–(−0.01)) | 0.041 |
| 41 BL | ||||
| PM-IOS | 0.493 (0.162–0.723) | 0.48 | −0.05 (−0.32–0.23) | 0.726 |
| PM-DPMA | 0.438 (0.114–0.682) | 0.51 | −0.28 (−0.55–(−0.01)) | 0.043 |
| PM-DPMS | 0.342 (−0.037–0.632) | 0.51 | −0.60 (−0.87–(−0.33)) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrović, V.; Šlaj, M.; Buljan, M.; Čivljak, T.; Zulijani, A.; Perić, B. Comparison of Tooth Size Measurements in Orthodontics Using Conventional and 3D Digital Study Models. J. Clin. Med. 2024, 13, 730. https://doi.org/10.3390/jcm13030730
Petrović V, Šlaj M, Buljan M, Čivljak T, Zulijani A, Perić B. Comparison of Tooth Size Measurements in Orthodontics Using Conventional and 3D Digital Study Models. Journal of Clinical Medicine. 2024; 13(3):730. https://doi.org/10.3390/jcm13030730
Chicago/Turabian StylePetrović, Valentina, Martina Šlaj, Mia Buljan, Tadej Čivljak, Ana Zulijani, and Berislav Perić. 2024. "Comparison of Tooth Size Measurements in Orthodontics Using Conventional and 3D Digital Study Models" Journal of Clinical Medicine 13, no. 3: 730. https://doi.org/10.3390/jcm13030730
APA StylePetrović, V., Šlaj, M., Buljan, M., Čivljak, T., Zulijani, A., & Perić, B. (2024). Comparison of Tooth Size Measurements in Orthodontics Using Conventional and 3D Digital Study Models. Journal of Clinical Medicine, 13(3), 730. https://doi.org/10.3390/jcm13030730