
Effectiveness, Tolerability, and Drug Survival of Risankizumab in a Real-World Setting: A Three-Year Retrospective Multicenter Study—IL PSO (ITALIAN LANDSCAPE PSORIASIS)

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  , , ,
, , ,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
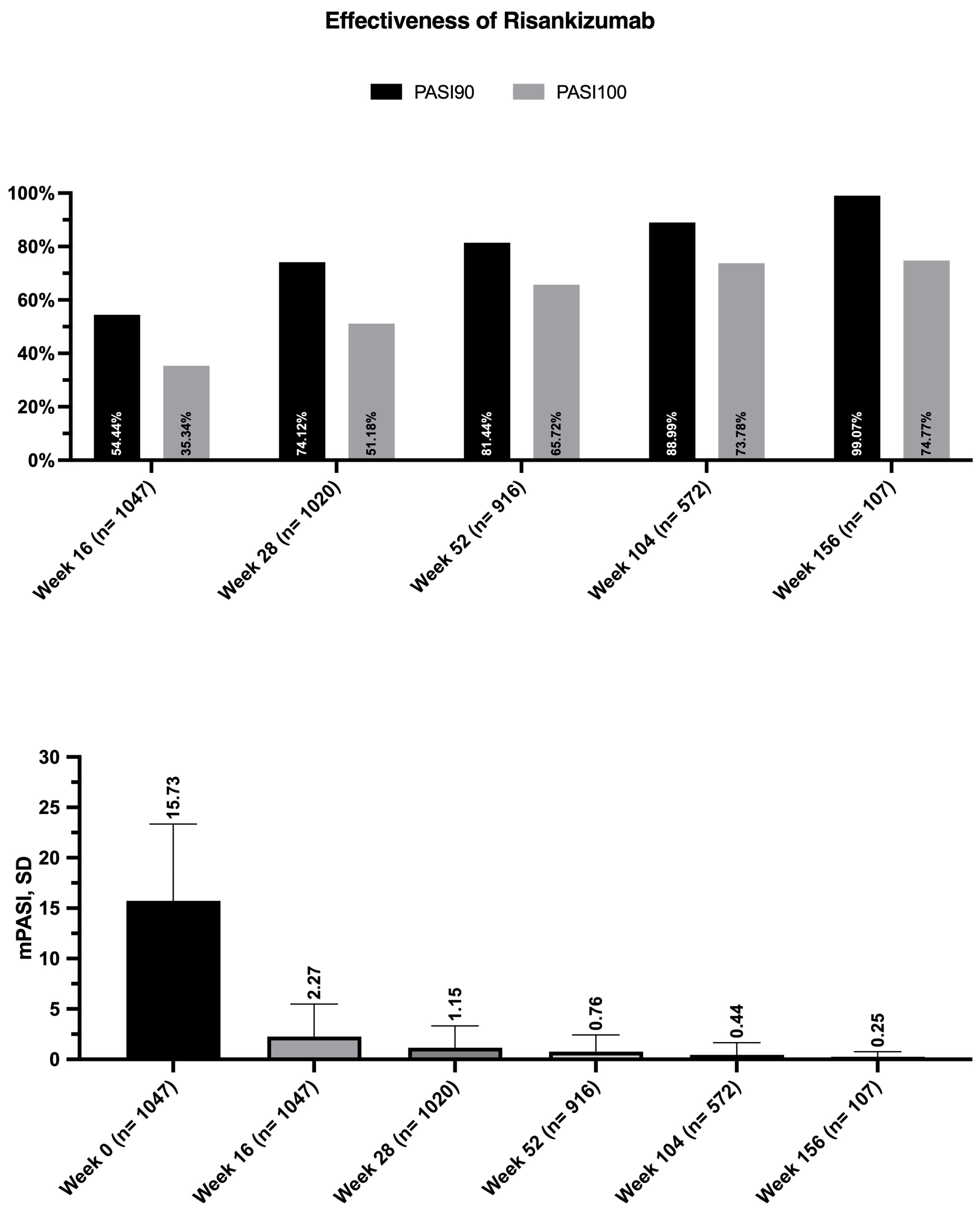
3.2. Risankizumab Effectiveness
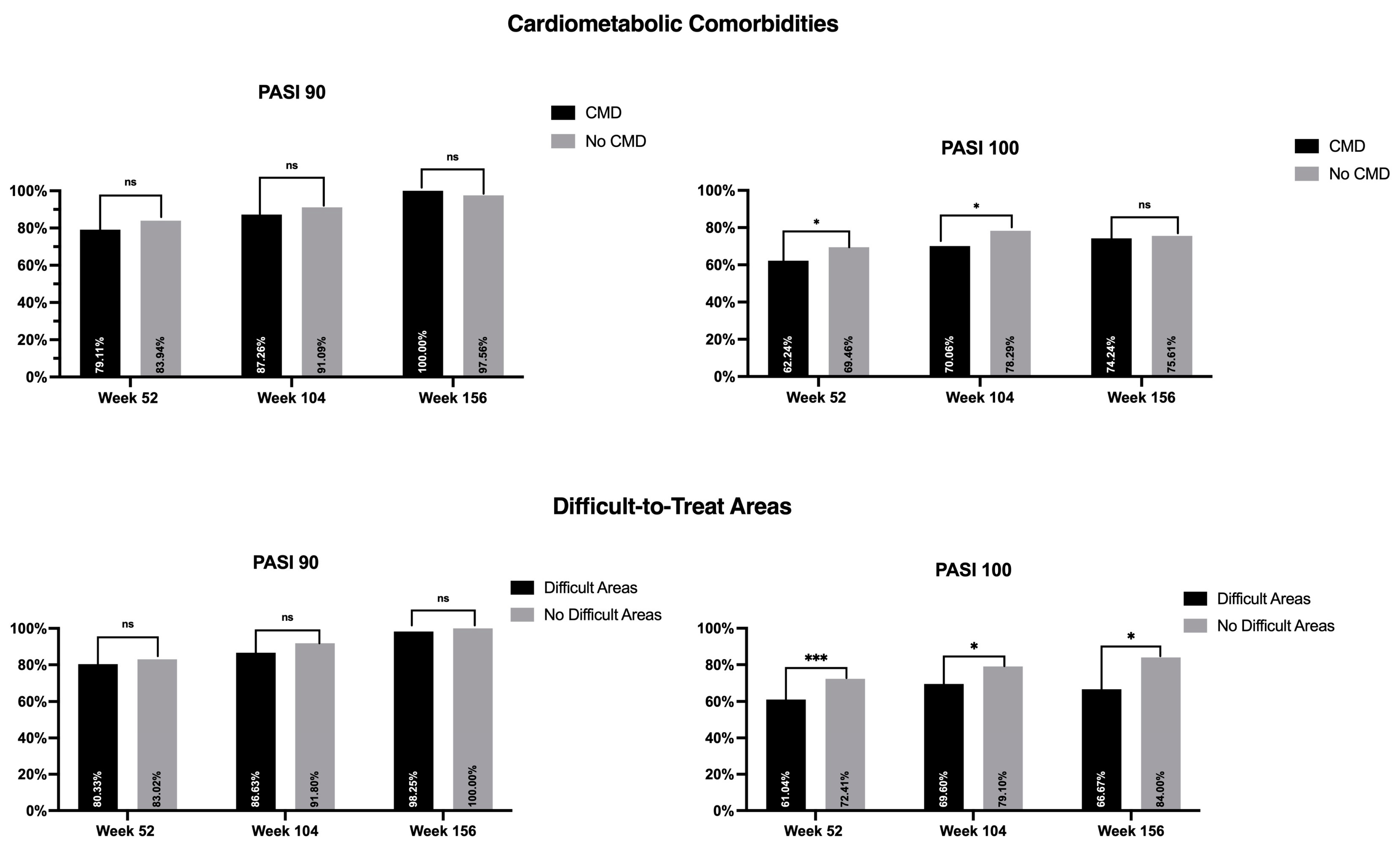
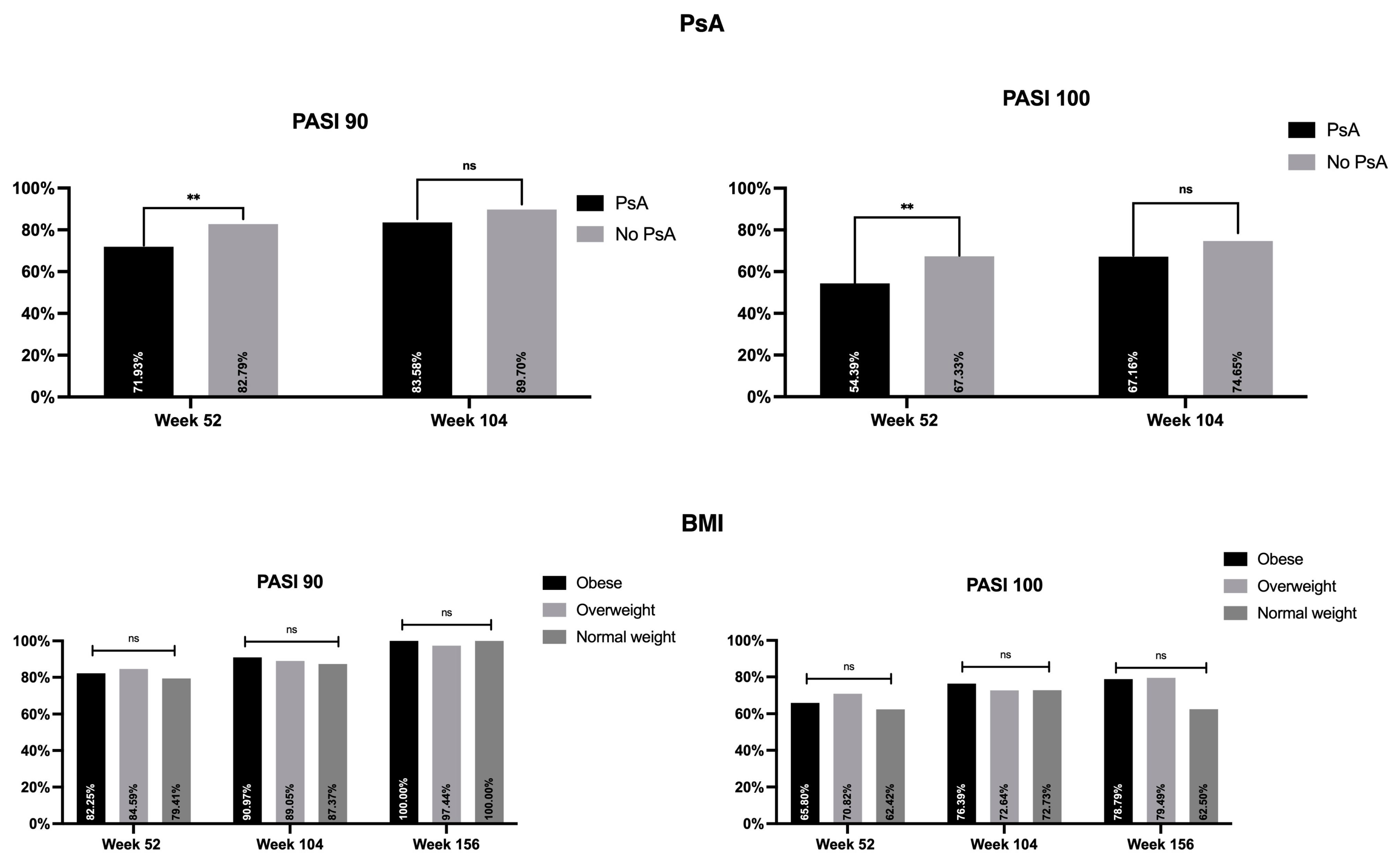
3.3. Effectiveness of Risankizumab in Selected Subpopulations
3.4. Multivariate Logistic Regression
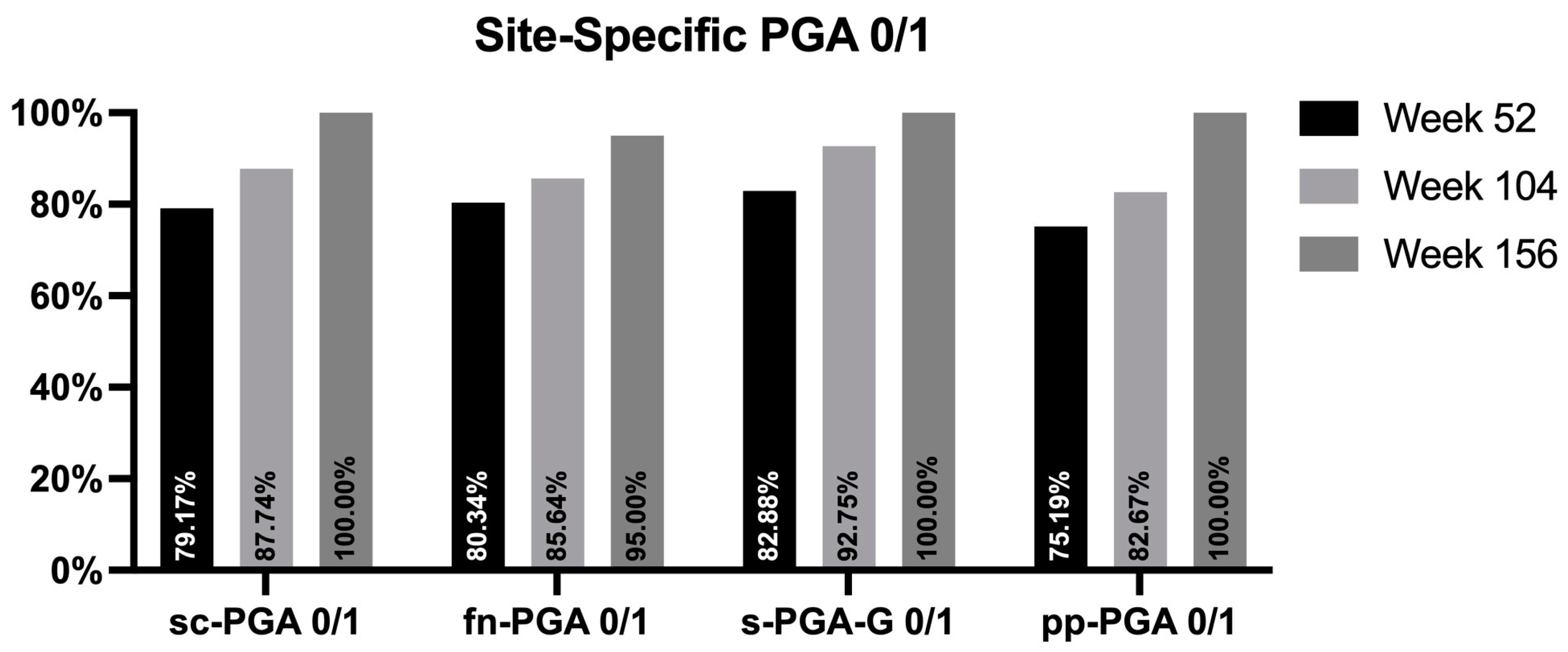
3.5. Long-Term Effectiveness of Risankizumab on Difficult-to-Treat Areas
3.6. Drug Survival
3.7. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armstrong, A.W.; Read, C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Bakshi, H.; Nagpal, M.; Singh, M.; Dhingra, G.A.; Aggarwal, G. Treatment of Psoriasis: A Comprehensive Review of Entire Therapies. Curr. Drug Saf. 2020, 15, 82–104. [Google Scholar] [CrossRef]
- Sbidian, E.; Chaimani, A.; Garcia-Doval, I.; Do, G.; Hua, C.; Mazaud, C.; Droitcourt, C.; Hughes, C.; Ingram, J.R.; Naldi, L.; et al. Systemic pharmacological treatments for chronic plaque psoriasis: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 12, CD011535. [Google Scholar] [CrossRef] [PubMed]
- Dave, R.; Alkeswani, A. An Overview of Biologics for Psoriasis. J. Drugs. Dermatol. 2021, 20, 1246–1247. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Geat, D.; Conti, A.; Dapavo, P.; Piaserico, S.; De Simone, C.; Bianchi, L.; Costanzo, A.; Malagoli, P.; Malara, G.; et al. TNF-α inhibitors biosimilars as first line systemic treatment for moderate-to-severe chronic plaque psoriasis. Expert. Rev. Clin. Immunol. 2020, 16, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Ghoreschi, K.; Balato, A.; Enerbäck, C.; Sabat, R. Therapeutics targeting the IL-23 and IL-17 pathway in psoriasis. Lancet 2021, 397, 754–766. [Google Scholar] [CrossRef]
- Valenti, M.; Narcisi, A.; Pavia, G.; Gargiulo, L.; Costanzo, A. What Can IBD Specialists Learn from IL-23 Trials in Dermatology? J. Crohns Colitis 2022, 16 (Suppl. S2), ii20–ii29. [Google Scholar] [CrossRef]
- Elgaard, C.D.B.; Iversen, L.; Hjuler, K.F. Guselkumab, tildrakizumab, and risankizumab in a real-world setting: Drug survival and effectiveness in the treatment of psoriasis and psoriatic arthritis. J. Dermatol. Treat. 2023, 34, 2133531. [Google Scholar] [CrossRef]
- Gordon, K.B.; Strober, B.; Lebwohl, M.; Augustin, M.; Blauvelt, A.; Poulin, Y.; Papp, A.K.; Sofen, H.; Puig, L.; Foley, P.; et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): Results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet 2018, 392, 650–661. [Google Scholar] [CrossRef]
- Warren, R.B.; Blauvelt, A.; Poulin, Y.; Beeck, S.; Kelly, M.; Wu, T.; Geng, Z.; Paul, C. Efficacy and safety of risankizumab vs. secukinumab in patients with moderate-to-severe plaque psoriasis (IMMerge): Results from a phase III, randomized, open-label, efficacy-assessor-blinded clinical trial. Br. J. Dermatol. 2021, 184, 50–59. [Google Scholar] [CrossRef]
- Blauvelt, A.; Leonardi, C.L.; Gooderham, M.; Papp, K.A.; Philipp, S.; Wu, J.J.; Igarashi, A.; Flack, M.; Geng, Z.; Wu, T.; et al. Efficacy and safety of continuous risankizumab therapy vs treatment withdrawal in patients with moderate to severe plaque psoriasis: A phase 3 randomized clinical trial. JAMA Dermatol. 2020, 156, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Gooderham, M.; Thaçi, D.; Crowley, J.J.; Ryan, C.; Krueger, J.G.; Tsai, T.-F.; Flack, M.; Gu, Y.; Williams, A.D.; et al. Risankizumab compared with adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): A randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet 2019, 394, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, L.; Ibba, L.; Malagoli, P.; Amoruso, F.; Argenziano, G.; Balato, A.; Bardazzi, F.; Burlando, M.; Carrera, C.G.; Damiani, G.; et al. A risankizumab super responder profile identified by long-term real-life observation-IL PSO (Italian Landscape Psoriasis). J. Eur. Acad. Dermatol. Venereol. 2023; published online ahead of print. [Google Scholar] [CrossRef]
- Gkalpakiotis, S.; Cetkovska, P.; Arenberger, P.; Dolezal, T.; Arenbergerova, M.; Velackova, B.; Fialova, J.; Kojanova, M. Risankizumab for the Treatment of Moderate-to-Severe Psoriasis: Real-Life Multicenter Experience from the Czech Republic. Dermatol. Ther. 2021, 11, 1345–1355. [Google Scholar] [CrossRef]
- Gisondi, P.; Fargnoli, M.C.; Amerio, P.; Argenziano, G.; Bardazzi, F.; Bianchi, L.; Chiricozzi, A.; Conti, A.; Corazza, M.; Costanzo, A.; et al. Italian adaptation of EuroGuiDerm guideline on the systemic treatment of chronic plaque psoriasis. Ital. J. Dermatol. Venerol. 2022, 157 (Suppl. S1), 1–78. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Skyrizi (Risankizumab): Summary of Product Characteristics. 2019. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/skyrizi (accessed on 8 March 2023).
- Puig, L. Obesity and psoriasis: Body weight and body mass index influence the response to biological treatment. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.; Langley, R.G.; Zhu, Y.; Zhou, H.; Song, M.; Shen, Y.K.; Lafferty, K.P.; Reich, K. Use of dose-exposure-response relationships in Phase 2 and Phase 3 guselkumab studies to optimize dose selection in psoriasis. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2082–2086. [Google Scholar] [CrossRef]
- Crowley, J.J.; Langley, R.G.; Gordon, K.B.; Pinter, A.; Ferris, L.K.; Rubant, S.; Photowala, H.; Xue, Z.; Wu, T.; Zhan, T.; et al. Efficacy of Risankizumab versus Secukinumab in Patients with Moderate-to-Severe Psoriasis: Subgroup Analysis from the IMMerge Study. Dermatol. Ther. 2022, 12, 561–575. [Google Scholar] [CrossRef]
- Berenguer-Ruiz, S.; Aparicio-Domínguez, M.; Herranz-Pinto, P.; Ruíz-Villaverde, R.; López-Ferrer, A.; Santos-Juanes, J.; Fernández-Freire, L.R.; Hospital-Gil, M.; Arias-Santiago, S.; Carretero-Hernández, G.; et al. Effectiveness and safety of tildrakizumab for the treatment of psoriasis in real-world settings at 24 weeks: A retrospective, observational, multicentre study by the Spanish Psoriasis Group. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 2517–2525. [Google Scholar] [CrossRef]
- Ricceri, F.; Chiricozzi, A.; Peris, K.; Prignano, F. Successful use of anti-IL-23 molecules in overweight-to-obese psoriatic patients: A multicentric retrospective study. Dermatol. Ther. 2022, 35, e15793. [Google Scholar] [CrossRef]
- Adamczyk, M.; Bartosińska, J.; Raczkiewicz, D.; Adamska, K.; Adamski, Z.; Czubek, M.; Kręcisz, B.; Kłujszo, E.; Lesiak, A.; Narbutt, J.; et al. Risankizumab Therapy for Moderate-to-Severe Psoriasis-A Multi-Center, Long-Term, Real-Life Study from Poland. J. Clin. Med. 2023, 12, 1675. [Google Scholar] [CrossRef] [PubMed]
- Orsini, D.; Frascione, P.; Assorgi, C.; Pacifico, A.; Sperduti, I.; Gargiulo, L.; Ibba, L.; Valenti, M.; Costanzo, A.; Narcisi, A. Risankizumab for the treatment of genital psoriasis: A 1-year, real-world experience. J. Eur. Acad. Dermatol. Venereol 2023. published online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Orsini, D.; Gargiulo, L.; Ibba, L.; Ingurgio, R.C.; Valenti, M.; Perugini, C.; Pacifico, A.; Maramao, F.S.; Frascione, P.; Costanzo, A.; et al. Effectiveness of risankizumab in plaque psoriasis with involvement of difficult-to-treat areas: A real-world experience from two referral centers. J. Dermatolog. Treat. 2023, 34, 2220849. [Google Scholar] [CrossRef] [PubMed]
- Yiu, Z.Z.N.; Becher, G.; Kirby, B.; Laws, P.; Reynolds, N.J.; Smith, C.H.; Warren, R.B.; Griffiths, C.E.M.; Browne, F.; Evans, I.; et al. Drug Survival Associated with Effectiveness and Safety of Treatment with Guselkumab, Ixekizumab, Secukinumab, Ustekinumab, and Adalimumab in Patients with Psoriasis. JAMA Dermatol. 2022, 158, 1131–1141, Erratum in JAMA Dermatol. 2022, 158, 1461. [Google Scholar] [CrossRef] [PubMed]
- Yiu, Z.Z.N.; Mason, K.J.; Hampton, P.J.; Reynolds, N.J.; Smith, C.H.; Lunt, M.; Griffiths, C.E.M.; Warren, R.B.; the BADBIR Study Group. Drug survival of adalimumab, ustekinumab and secukinumab in patients with psoriasis: A prospective cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br. J. Dermatol. 2020, 183, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, L.; Pavia, G.; Valenti, M.; de Nalda, A.L.; Perugini, C.; Costanzo, A.; Narcisi, A. Safety of Biologic Therapies in Patients with Moderate-to-Severe Plaque Psoriasis and Concomitant Viral Hepatitis: A Monocentric Retrospective Study. Dermatol. Ther. 2022, 12, 1263–1270. [Google Scholar] [CrossRef]
- Huang, Y.W.; Tsai, T.F. A drug safety evaluation of risankizumab for psoriasis. Expert Opin. Drug Saf. 2020, 19, 395–402. [Google Scholar] [CrossRef]
- Ibba, L.; Gargiulo, L.; Vignoli, C.A.; Fiorillo, G.; Valenti, M.; Costanzo, A.; Narcisi, A. Safety of anti-IL-23 drugs in patients with moderate-to-severe plaque psoriasis and previous tuberculosis infection: A monocentric retrospective study. J. Dermatolog. Treat. 2023, 34, 2241585. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Rodriguez-Fernandez-Freire, L.; Pérez-Gil, A.; Font-Ugalde, P.; Galán-Gutiérrez, M. Risankizumab: Efficacy, Safety, and Survival in the Mid-Term (52 Weeks) in Real Clinical Practice in Andalusia, Spain, According to the Therapeutic Goals of the Spanish Psoriatic Guidelines. Life 2022, 12, 1883. [Google Scholar] [CrossRef]
- Woods, R.H. Potential cerebrovascular accident signal for risankizumab: A disproportionality analysis of the FDA Adverse Event Reporting System (FAERS). Br. J. Clin. Pharmacol. 2022, 89, 2386–2395. [Google Scholar] [CrossRef]
- Egeberg, A.; Thyssen, J.P. Increased reporting of cerebrovascular accidents with use of risankizumab observed in the FDA Adverse Events Reporting System (FAERS). Br. J. Dermatol. 2023, 188, ljad039. [Google Scholar] [CrossRef] [PubMed]
- Mattay, S.S.; Zamani, M.; Saturno, D.; Loftus, E.V.; Ciorba, M.A.; Yarur, A.; Singh, S.; Deepak, P. Risk of Major Adverse Cardiovascular Events in Immune-Mediated Inflammatory Disorders on Biologics and Small Molecules: Network Meta-Analysis. Clin. Gastroenterol. Hepatol. 2023. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 1047 |
|---|---|
| N (%) | |
| Male | 705 (67.34%) |
| PsA | 127 (12.13%) |
| At least one difficult-to-treat site * | 623 (59.50%) |
| At least one cardiometabolic comorbidity | 535 (51.10%) |
| Arterial hypertension | 293 (29.98%) |
| Obesity (BMI ≥ 30) | 256 (24.45%) |
| Type II diabetes mellitus | 124 (11.84%) |
| CVD | 56 (5.35%) |
| Hypercholesterolemia | 118 (11.27%) |
| Bio-naïve | 601 (57.40%) |
| Mean ± SD | |
| Age, years | 51.37 ± 14.95 |
| PASI at baseline | 15.73 ± 7.62 |
| BMI | 28.05 ± 5.66 |
| PsA | No PsA | Univariate Analysis | Multivariate Analysis | |
| p-Value | OR [CI 95%]; p-Value | |||
| PASI 90 w52 | 82/114 (71.93%) | 664/802 (82.79%) | 0.005 | 0.54 [0.34–0.84]; 0.006 |
| PASI 100 w52 | 62/114 (54.39%) | 540/802 (67.33%) | 0.006 | 0.61 [0.40–0.92]; 0.019 |
| PASI 90 w104 | 56/67 (83.58%) | 453/505 (89.70%) | 0.13 | 0.61 [0.30-1.25]; 0.18 |
| PASI 100 w104 | 45/67 (67.16%) | 377/505 (74.65%) | 0.19 | 0.73 [0.42-1.27]; 0.27 |
| Difficult Areas | No Difficult Areas | Univariate Analysis | Multivariate Analysis | |
| p-Value | OR [CI 95%]; p-Value | |||
| PASI 90 w52 | 433/539 (80.33%) | 313/377 (83.02%) | 0.30 | NA |
| PASI 100 w52 | 329/539 (61.04%) | 273/377 (72.41%) | <0.001 | 0.56 [0.41–0.76]; <0.001 |
| PASI 90 w104 | 285/328 (86.89%) | 224/244 (91.80%) | 0.063 | 0.58 [0.33–1.02]; 0.06 |
| PASI 100 w104 | 229/328 (69.82%) | 193/244 (79.10%) | 0.013 | 0.59 [0.40–0.88]; 0.009 |
| PASI 90 w156 | 56/57 (98.25%) | 50/50 (100.00%) | 0.35 | NA |
| PASI 100 w156 | 38/57 (66.67%) | 42/50 (84.00%) | 0.039 | 0.38 [0.15–0.97]; 0.043 |
| CMD | No CMD | Univariate Analysis | Multivariate Analysis | |
| p-Value | OR [CI 95%]; p-Value | |||
| PASI 90 w52 | 375/474 (79.11%) | 371/442 (83.94%) | 0.061 | 0.73 [0.52-1.02]; 0.07 |
| PASI 100 w52 | 295/474 (62.24%) | 307/442 (69.46%) | 0.021 | 0.54 [0.38–0.77]; 0.001 |
| PASI 90 w104 | 274/314 (87.26%) | 235/258 (91.09%) | 0.15 | 0.63 [0.36-1.09]; 0.1 |
| PASI 100 w104 | 220/314 (70.06%) | 202/258 (78.29%) | 0.026 | 0.61 [0.42–0.90]; 0.013 |
| PASI 90 w156 | 66/66 (100.00%) | 40/41 (97.56%) | 0.20 | NA |
| PASI 100 w156 | 49/66 (74.24%) | 31/41 (75.61%) | 0.87 | NA |
| BMI ≥ 30 | 25 ≤ BMI < 30 | BMI < 25 | Univariate Analysis | Multivariate Analysis | |
|---|---|---|---|---|---|
| p-Value | OR [CI 95%]; p-Value | ||||
| PASI 90 w52 | 190/231 (82.25%) | 258/305 (84.59%) | 243/306 (79.41%) | 0.25 | NA |
| PASI 100 w52 | 152/231 (65.80%) | 216/305 (70.82%) | 191/306 (62.42%) | 0.087 | 1.57 [0.98–2.24]; 0.061 |
| PASI 90 w104 | 131/144 (90.97%) | 179/201 (89.05%) | 173/198 (87.37%) | 0.58 | NA |
| PASI 100 w104 | 110/144 (76.39%) | 146/201 (72.64%) | 144/198 (72.73%) | 0.69 | NA |
| PASI 90 w156 | 33/33 (100.00%) | 38/39 (97.44%) | 32/32 (100.00%) | 0.43 | NA |
| PASI 100 w156 | 26/33 (78.79%) | 31/39 (79.49%) | 20/32 (62.50%) | 0.20 | NA |
| Adverse Events | Patients, N (%) |
|---|---|
| Rhinopharyngitis | 21 (2.01) |
| Headache | 15 (1.05) |
| Upper respiratory tract infections | 13 (1.24) |
| Diarrhea | 6 (0.57) |
| Neoplasm diagnosis | 3 (0.29) |
| Flare of atopic eczema | 3 (0.29) |
| Injection-site reaction | 2 (0.19) |
| AEs leading to discontinuation | 7 (0.67) |
| Total | 70 (6.69) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gargiulo, L.; Ibba, L.; Malagoli, P.; Amoruso, F.; Argenziano, G.; Balato, A.; Bardazzi, F.; Burlando, M.; Carrera, C.G.; Damiani, G.; et al. Effectiveness, Tolerability, and Drug Survival of Risankizumab in a Real-World Setting: A Three-Year Retrospective Multicenter Study—IL PSO (ITALIAN LANDSCAPE PSORIASIS). J. Clin. Med. 2024, 13, 495. https://doi.org/10.3390/jcm13020495
Gargiulo L, Ibba L, Malagoli P, Amoruso F, Argenziano G, Balato A, Bardazzi F, Burlando M, Carrera CG, Damiani G, et al. Effectiveness, Tolerability, and Drug Survival of Risankizumab in a Real-World Setting: A Three-Year Retrospective Multicenter Study—IL PSO (ITALIAN LANDSCAPE PSORIASIS). Journal of Clinical Medicine. 2024; 13(2):495. https://doi.org/10.3390/jcm13020495
Chicago/Turabian StyleGargiulo, Luigi, Luciano Ibba, Piergiorgio Malagoli, Fabrizio Amoruso, Giuseppe Argenziano, Anna Balato, Federico Bardazzi, Martina Burlando, Carlo Giovanni Carrera, Giovanni Damiani, and et al. 2024. "Effectiveness, Tolerability, and Drug Survival of Risankizumab in a Real-World Setting: A Three-Year Retrospective Multicenter Study—IL PSO (ITALIAN LANDSCAPE PSORIASIS)" Journal of Clinical Medicine 13, no. 2: 495. https://doi.org/10.3390/jcm13020495
APA StyleGargiulo, L., Ibba, L., Malagoli, P., Amoruso, F., Argenziano, G., Balato, A., Bardazzi, F., Burlando, M., Carrera, C. G., Damiani, G., Dapavo, P., Dini, V., Franchi, C., Gaiani, F. M., Girolomoni, G., Guarneri, C., Lasagni, C., Loconsole, F., Marzano, A. V., ... Narcisi, A. (2024). Effectiveness, Tolerability, and Drug Survival of Risankizumab in a Real-World Setting: A Three-Year Retrospective Multicenter Study—IL PSO (ITALIAN LANDSCAPE PSORIASIS). Journal of Clinical Medicine, 13(2), 495. https://doi.org/10.3390/jcm13020495