

Effect of Resistance Exercise on Body Composition and Functional Capacity in Older Women with Sarcopenic Obesity—A Systematic Review with Narrative Synthesis

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategies
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
3. Results
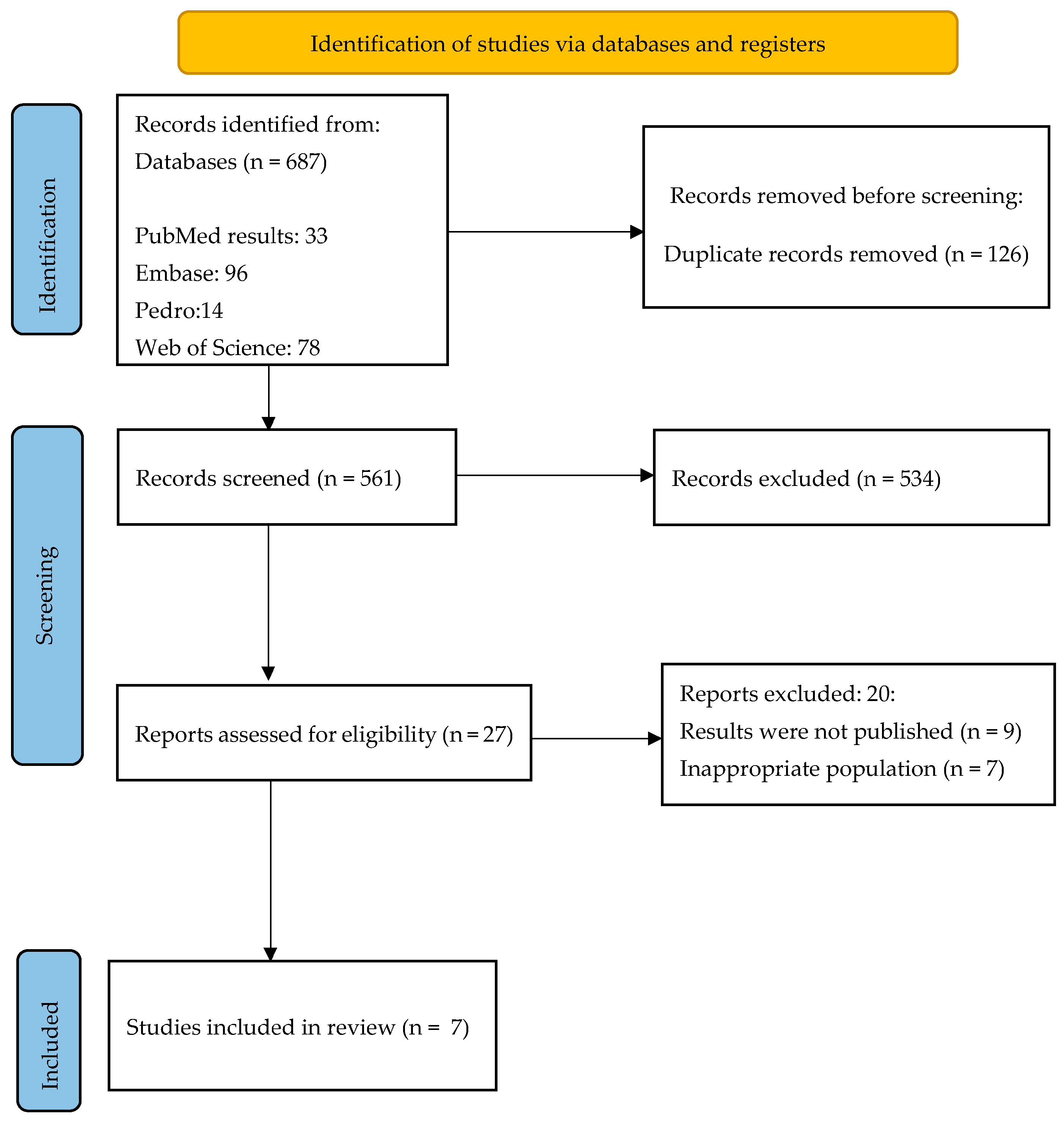
3.1. Study Selection and Characteristics
3.2. Setting and Training Equipment
3.3. Dosage of Exercise Program
3.4. Results According to the Outcomes
3.4.1. Body Composition Measures
3.4.2. Strength
3.4.3. Functional Capacity
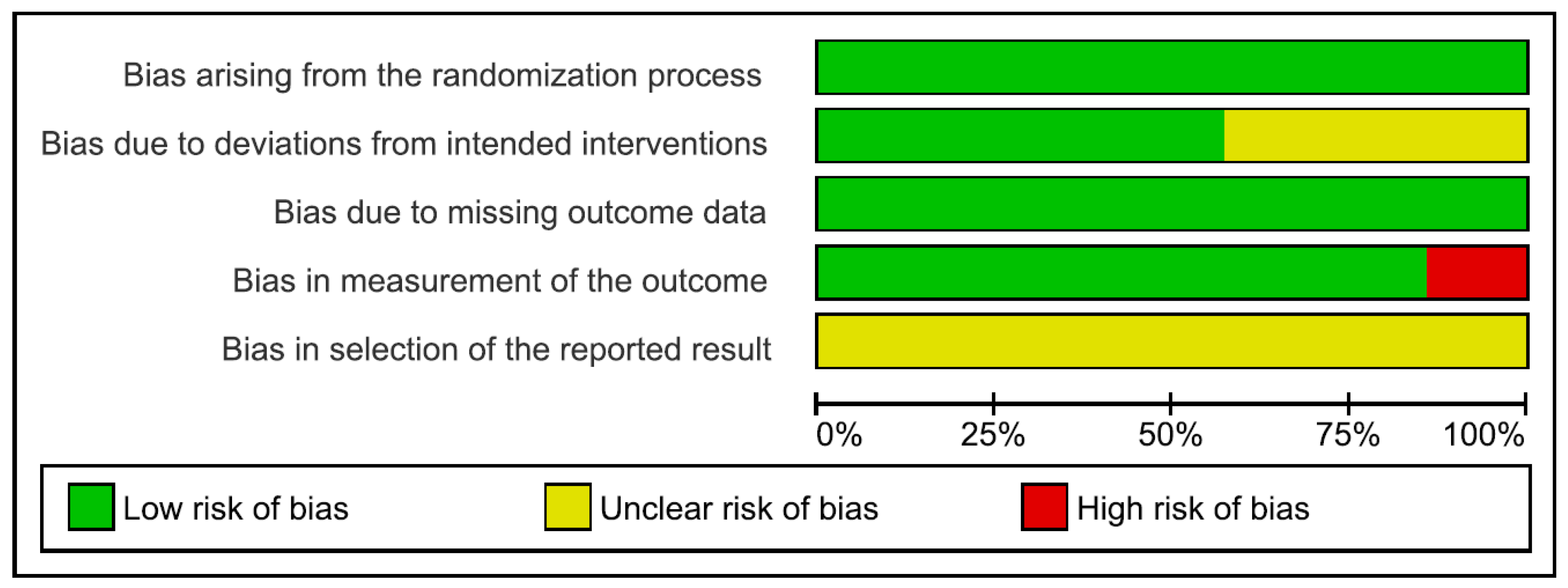
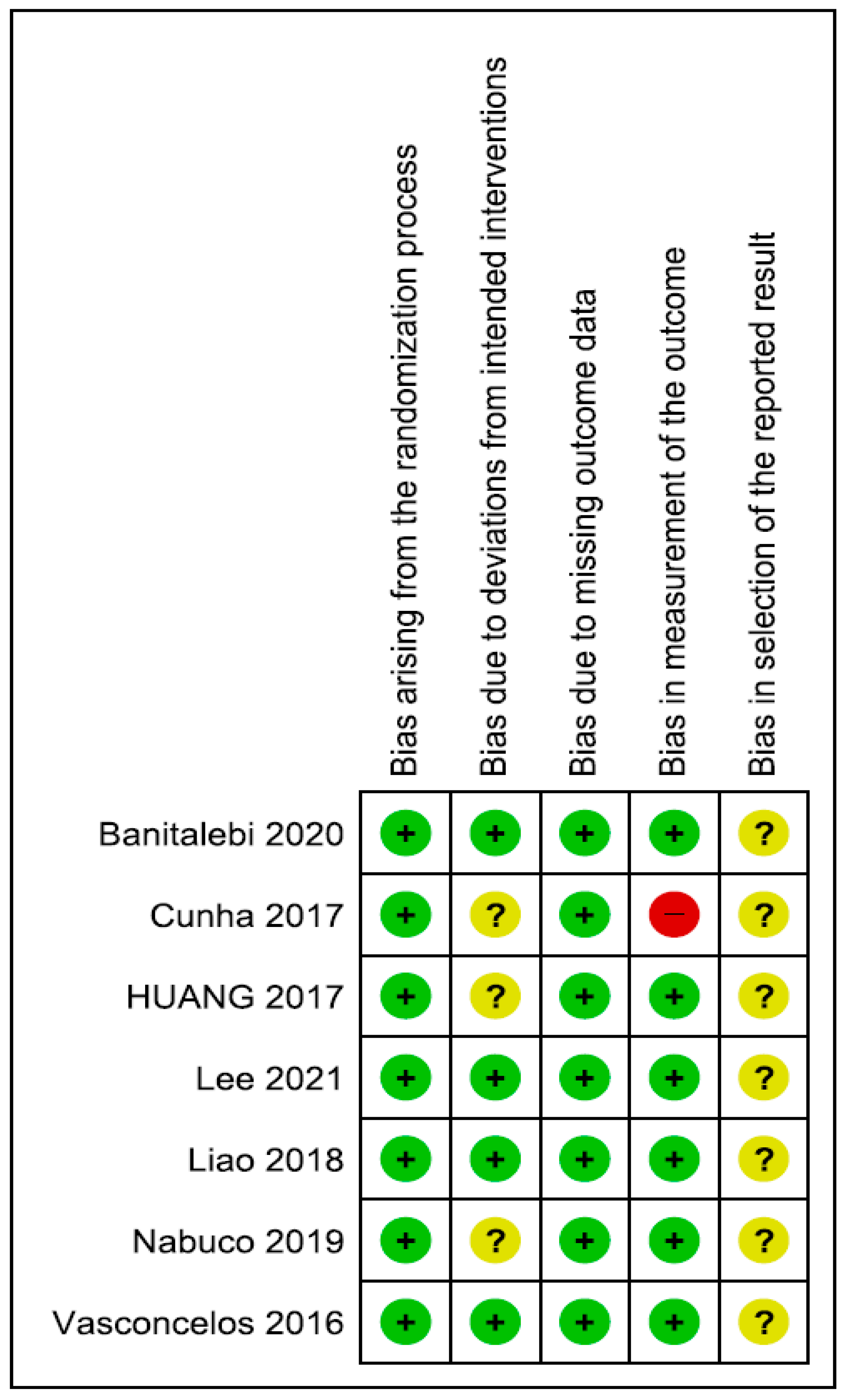
3.5. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 1RM | 1-repetition maximum |
| 10 MW | 10 m walk |
| 30 CST | 30 s chair stand test |
| ALM | Appendicular lean mass |
| AMI | Appendicular lean mass index |
| BF% | Body fat percentage |
| BMI | Body mass index |
| FFR | Functional forward reach |
| GS | Grip strength |
| HC | Hip circumference |
| LMI | Lean muscle mass index |
| LST | Lean soft tissue |
| RCT | Randomised controlled trial |
| RSP | Raising from a sitting position |
| SLS | Single-leg stance |
| SMI | Skeletal muscle mass index |
| SO | Sarcopenic obesity |
| TSM | Total skeletal mass (kg) |
| TUG | Timed up and go |
| WC | Waist circumference |
| WHR | Waist–hip ratio |
Appendix A. Search Strategy
| Database | Search Strategy |
| PubMed |
Population: #1 ((((“Sarcopenia”[Mesh]) OR (“Muscular Atrophy”[Mesh])) OR (“Muscle Weakness”[Mesh])) OR (Sarcopenia[Title/Abstract])) OR (sarcopenic[Title/Abstract]) #2 (((((“Obesity”[Mesh]) OR (“Overweight”[Mesh])) OR (obese[Title/Abstract])) OR (obesity[Title/Abstract])) OR (obestic[Title/Abstract])) OR (overweight[Title/Abstract]) #3 Intervention:((((((((((((((((((((((((((((((((((“Weight Lifting”[Mesh])) OR (“Resistance Training”[Mesh])) OR (Resistance Training[Title/Abstract])) OR (resistance exercise[Title/Abstract])) OR (Training, Resistance[Title/Abstract])) OR (Strength Training[Title/Abstract])) OR (Training, Strength[Title/Abstract])) OR (Weight-Lifting Strengthening Program[Title/Abstract])) OR (Strengthening Program, Weight-Lifting[Title/Abstract])) OR (Strengthening Programs, Weight-Lifting[Title/Abstract])) OR (Weight Lifting Strengthening Program[Title/Abstract])) OR (Weight-Lifting Strengthening Programs[Title/Abstract])) OR (Weight-Lifting Exercise Program[Title/Abstract])) OR (Exercise Program, Weight-Lifting[Title/Abstract])) OR (Exercise Programs, Weight-Lifting[Title/Abstract])) OR (Weight Lifting Exercise Program[Title/Abstract])) OR (Weight-Lifting Exercise Programs[Title/Abstract])) OR (Weight-Bearing Strengthening Program[Title/Abstract])) OR (Strengthening Program, Weight-Bearing[Title/Abstract])) OR (Strengthening Programs, Weight-Bearing[Title/Abstract])) OR (Weight Bearing Strengthening Program[Title/Abstract])) OR (Weight-Bearing Strengthening Programs[Title/Abstract])) OR (Weight-Bearing Exercise Program[Title/Abstract])) OR (Exercise Program, Weight-Bearing[Title/Abstract])) OR (Exercise Programs, Weight-Bearing[Title/Abstract])) OR (Weight Bearing Exercise Program[Title/Abstract])) OR (Weight-Bearing Exercise Programs[Title/Abstract])) OR (Lifting, Weight[Title/Abstract])) OR (Liftings, Weight[Title/Abstract])) OR (Weight Liftings[Title/Abstract])) OR (elastic band[Title/Abstract])) OR (body weight training[Title/Abstract])) OR (strengthening exercise[Title/Abstract])) OR (strength exercise[Title/Abstract]) #4 Gender:((((“Female”[Mesh]) OR (“Women”[Mesh])) OR (female[Title/Abstract])) OR (woman[Title/Abstract])) OR (women[Title/Abstract]) #5 Study design: ((((((((((((((((“Single-Blind Method”[Mesh]) OR (“Double-Blind Method”[Mesh])) OR (“Randomized Controlled Trials as Topic”[Mesh])) OR (Randomized Controlled Trial[Publication Type])) OR (“Intention to Treat Analysis”[Mesh])) OR (“Controlled Clinical Trials as Topic”[Mesh])) OR (“Clinical Trials as Topic”[Mesh])) OR (Clinical Trial[Publication Type])) OR (randomized controlled trial[Publication Type])) OR (random*[Title/Abstract])) OR (allocation[Title/Abstract])) OR (random allocation[Title/Abstract])) OR (placebo[Title/Abstract])) OR (single blind[Title/Abstract])) OR (double blind[Title/Abstract])) OR (randomized controlled trial*[Title/Abstract])) OR (RCT[Title/Abstract]) #6 #1 AND #2 AND #3 AND #4 AND #5 |
| Web of Science |
#1 (((TS=(Sarcopenia)) OR TS=(sarcopenic)) OR TS=(Muscular Atrophy)) OR TS=(Muscle Weakness) #2 (((TS=(obese)) OR TS=(obesity)) OR TS=(obestic)) OR TS=(overweight) #3 (((((((((((((TS=(Weight Lifting)) OR TS=(Resistance Training)) OR TS=(resistance exercise)) OR TS=(Strength Training)) OR TS=(Weight-Lifting Strengthening Program)) OR TS=(Weight-Lifting Exercise Program)) OR TS=(Weight-Bearing Strengthening Program)) OR TS=(Weight Bearing Exercise Program)) OR TS=(Liftings, Weight)) OR TS=(Lifting, Weight)) OR TS=(elastic band)) OR TS=(body weight training)) OR TS=(strengthening exercise)) OR TS=(strength exercise) #4 ((TS=(female)) OR TS=(woman)) OR TS=(women) #5 ((((((((TS=(Single-Blind Method)) OR TS=(Double-Blind Method)) OR TS=(Randomized Controlled Trial)) OR TS=(Clinical Trials)) OR TS=(random allocation)) OR TS=(placebo)) OR TS=(single blind)) OR TS=(double blind)) OR TS=(RCT) #6 #1 AND #2 AND #3 AND #4 AND #5 |
| Cochrane |
#1 MeSH descriptor: [Sarcopenia] explode all trees #2 MeSH descriptor: [Muscular Atrophy] explode all trees #3 MeSH descriptor: [Muscle Weakness] explode all trees #4 (Sarcopenia):ti,ab,kw (Word variations have been searched) #5 (sarcopenic):ti,ab,kw (Word variations have been searched) #6 #1 OR #2 OR #3 OR #4 OR #5 #7 MeSH descriptor: [Obesity] explode all trees #8 MeSH descriptor: [Overweight] explode all trees #9 (obese):ti,ab,kw (Word variations have been searched) #10 (obesity):ti,ab,kw (Word variations have been searched) #11 (obestic):ti,ab,kw (Word variations have been searched) #12 (overweight):ti,ab,kw (Word variations have been searched) #13 #7 OR #8 OR #9 OR #10 OR #11 OR 12 #14 MeSH descriptor: [Weight Lifting] explode all trees #15 MeSH descriptor: [Resistance Training] explode all trees #16 (“resistance training”):ti,ab,kw (Word variations have been searched) #17 (resistance exercise):ti,ab,kw (Word variations have been searched) #18 (Training, Resistance):ti,ab,kw (Word variations have been searched) #19 (Strength Training):ti,ab,kw (Word variations have been searched) #20 (Training, Strength):ti,ab,kw (Word variations have been searched) #21 (Weight-Lifting Strengthening Program):ti,ab,kw (Word variations have been searched) #22 (Strengthening Program, Weight-Lifting):ti,ab,kw (Word variations have been searched) #23 (Strengthening Programs, Weight-Lifting):ti,ab,kw (Word variations have been searched) #24 (Weight Lifting Strengthening Program):ti,ab,kw (Word variations have been searched) #25 (Weight-Lifting Strengthening Programs):ti,ab,kw (Word variations have been searched) #26 (Weight-Lifting Exercise Program):ti,ab,kw (Word variations have been searched) #27 (Exercise Program, Weight-Lifting):ti,ab,kw (Word variations have been searched) #28 (Exercise Programs, Weight-Lifting):ti,ab,kw (Word variations have been searched) #29 (Weight Lifting Exercise Program):ti,ab,kw (Word variations have been searched) #30 (Weight-Lifting Exercise Programs):ti,ab,kw (Word variations have been searched) #31 (Weight-Bearing Strengthening Program):ti,ab,kw (Word variations have been searched) #32 (Strengthening Program, Weight-Bearing):ti,ab,kw (Word variations have been searched) #33 (Strengthening Programs, Weight-Bearing):ti,ab,kw (Word variations have been searched) #34 (Weight Bearing Strengthening Program):ti,ab,kw (Word variations have been searched) #35 (Weight-Bearing Strengthening Programs):ti,ab,kw (Word variations have been searched) #36 (Weight-Bearing Exercise Program):ti,ab,kw (Word variations have been searched) #37 (Exercise Program, Weight-Bearing):ti,ab,kw (Word variations have been searched) #38 (Exercise Programs, Weight-Bearing):ti,ab,kw (Word variations have been searched) #39 (Weight Bearing Exercise Program):ti,ab,kw (Word variations have been searched) #40 (Weight Bearing Exercise Programs):ti,ab,kw (Word variations have been searched) #41 (Lifting, Weight):ti,ab,kw (Word variations have been searched) #42 (Liftings, Weight):ti,ab,kw (Word variations have been searched) #43 (Weight Liftings):ti,ab,kw (Word variations have been searched) #44 (elastic band):ti,ab,kw (Word variations have been searched) #45 (body weight training):ti,ab,kw (Word variations have been searched) #46 (strengthening exercise):ti,ab,kw (Word variations have been searched) #47 (strength exercise):ti,ab,kw (Word variations have been searched) #48 #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 OR #47 #49 MeSH descriptor: [Female] explode all trees #50 MeSH descriptor: [Women] explode all trees #51 (female):ti,ab,kw (Word variations have been searched) #52 (Woman):ti,ab,kw (Word variations have been searched) #53 (Women):ti,ab,kw (Word variations have been searched) #54 #49 OR #50 OR #51 OR #52 OR #53 #55 #6 AND #13 AND #48 AND #54 |
| Embase |
#1. ‘sarcopenia’/exp OR ‘sarcopenia #2. ‘muscle atrophy’/exp OR ‘muscle atrophy’ #3. ‘muscle weakness’/exp OR ‘muscle weakness’ #4. sarcopenia:ab,ti #5. sarcopenic:ab,ti #6. #1 OR #2 OR #3 OR #4 OR #5 #7. ‘obesity’/exp OR ‘obesity’ #8. obese:ab,ti #9. obesity:ab,ti #10. obestic:ab,ti #11. #7 OR #8 OR #9 OR #10 #12. ‘weight lifting’/exp OR ‘weight lifting’ #13. ‘resistance training’/exp OR ‘resistance training’ #14. ‘resistance training’:ab,ti #15. ‘weight lifting’:ab,ti #16. ‘resistance exercise’:ab,ti #17. ‘training, resistance’:ab,ti #18. ‘strength training’:ab,ti #19. ‘training, strength’:ab,ti #20. ‘weight-lifting exercise program’:ab,ti #21. ‘weight-bearing strengthening program’:ab,ti #22. ‘exercise programs, weight-bearing’:ab,ti #23. ‘weight bearing exercise program’:ab,ti #24. ‘weight-bearing exercise programs’:ab,ti #25. ‘lifting, weight’:ab,ti #26. ‘weight liftings’:ab,ti #27. ‘elastic band’:ab,ti #28. ‘body weight training’:ab,ti #29. ‘strengthening exercise’:ab,ti #30. ‘strength exercise’:ab,ti #31. #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR#19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 #32. ‘female’/exp OR ‘female’ #33. female:ab,ti #34. woman:ab,ti #35. women:ab,ti #36. #32 OR #33 OR #34 OR #35 #37. ‘single blind procedure’/exp OR ‘single blind procedure’ #38. ‘double blind procedure’/exp OR ‘double blind procedure’ #39. ‘randomized controlled trial (topic)’/exp OR ‘randomized controlled trial (topic)’ #40. ‘randomized controlled trial’/exp OR ‘randomized controlled trial’ #41. ‘intention to treat analysis’/exp OR ‘intention to treat analysis’ #42. ‘controlled clinical trial (topic)’/exp OR ‘controlled clinical trial (topic)’ #43. ‘clinical trial (topic)’/exp OR ‘clinical trial (topic)’ #44. ‘clinical study’:ab,ti #45. ‘randomized controlled trial’:ab,ti #46. random*:ab,ti #47. allocation:ab,ti #48. placebo:ab,ti #49. ‘single blind’:ab,ti #50. ‘double blind’:ab,ti #51. ‘randomized controlled trial*’:ab,ti #52. rct:ab,ti #53. #37 OR #38 OR #39 OR #40 OR #41 OR #42 OR #43 OR #44 OR #45 OR #46 OR #47 OR #48 OR #49 OR #50 OR #51 OR #52 #54. #6 AND #11 AND #31 AND #36 AND #53 |
| Pedro |
# Abstract & Title: “Sarcopenic obesity” # Therapy: Strength training # Method: clinical trial # When Searching: Match all search terms (AND) |
References
- Duda, K.; Majerczak, J.; Nieckarz, Z.; Heymsfield, S.B.; Zoladz, J.A. Human Body Composition and Muscle Mass. In Muscle and Exercise Physiology; Elsevier: Amsterdam, The Netherlands, 2019; pp. 3–26. ISBN 978-0-12-814593-7. [Google Scholar]
- United Nations. World Population Ageing; United Nations: New York, NY, USA, 2019; p. 2. [Google Scholar]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European Consensus on Definition and Diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Yuan, D.; Jin, H.; Liu, Q.; Zhang, J.; Ma, B.; Xiao, W.; Li, Y. Publication Trends for Sarcopenia in the World: A 20-Year Bibliometric Analysis. Front. Med. 2022, 9, 802651. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; De Souza, R.J.; Thabane, L.; Raina, P. The Prevalence of Sarcopenia in Community-Dwelling Older Adults, an Exploration of Differences between Studies and within Definitions: A Systematic Review and Meta-Analyses. Age Ageing 2019, 48, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.-C.; Chang, S.-F.; Tsai, H.-C. The Relationship between Sarcopenia and Injury Events: A Systematic Review and Meta-Analysis of 98,754 Older Adults. J. Clin. Med. 2022, 11, 6474. [Google Scholar] [CrossRef] [PubMed]
- Ansaripour, A.; Arjomandi Rad, A.; Koulouroudias, M.; Angouras, D.; Athanasiou, T.; Kourliouros, A. Sarcopenia Adversely Affects Outcomes Following Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 5573. [Google Scholar] [CrossRef]
- Gómez-Martínez, M.; Rodríguez-García, W.; González-Islas, D.; Orea-Tejeda, A.; Keirns-Davis, C.; Salgado-Fernández, F.; Hernández-López, S.; Jiménez-Valentín, A.; Ríos-Pereda, A.V.; Márquez-Cordero, J.C.; et al. Impact of Body Composition and Sarcopenia on Mortality in Chronic Obstructive Pulmonary Disease Patients. J. Clin. Med. 2023, 12, 1321. [Google Scholar] [CrossRef]
- Veronese, N.; Demurtas, J.; Soysal, P.; Smith, L.; Torbahn, G.; Schoene, D.; Schwingshackl, L.; Sieber, C.; Bauer, J.; Cesari, M.; et al. Sarcopenia and Health-Related Outcomes: An Umbrella Review of Observational Studies. Eur. Geriatr. Med. 2019, 10, 853–862. [Google Scholar] [CrossRef]
- Wu, W.-T.; Lee, T.-M.; Han, D.-S.; Chang, K.-V. The Prevalence of Sarcopenia and Its Impact on Clinical Outcomes in Lumbar Degenerative Spine Disease—A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 773. [Google Scholar] [CrossRef]
- Yuan, S.; Larsson, S.C. Epidemiology of Sarcopenia: Prevalence, Risk Factors, and Consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.M.; Wells, J.C.K.; Smith, S.R.; Stephan, B.C.M.; Siervo, M. Sarcopenic Obesity: A Critical Appraisal of the Current Evidence. Clin. Nutr. 2012, 31, 583–601. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.E.; Crimmins, E.M. The Impact of Insulin Resistance and Inflammation on the Association Between Sarcopenic Obesity and Physical Functioning. Obesity 2012, 20, 2101–2106. [Google Scholar] [CrossRef] [PubMed]
- Hirani, V.; Naganathan, V.; Blyth, F.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Longitudinal Associations between Body Composition, Sarcopenic Obesity and Outcomes of Frailty, Disability, Institutionalisation and Mortality in Community-Dwelling Older Men: The Concord Health and Ageing in Men Project. Age Ageing 2017, 46, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Cho, J.J.; Park, Y.S. Relationship between Sarcopenic Obesity and Cardiovascular Disease Risk as Estimated by the Framingham Risk Score. J. Korean Med. Sci. 2015, 30, 264. [Google Scholar] [CrossRef]
- Atkins, J.L.; Whincup, P.H.; Morris, R.W.; Lennon, L.T.; Papacosta, O.; Wannamethee, S.G. Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality: A Population-Based Cohort Study of Older Men. J. Am. Geriatr. Soc. 2014, 62, 253–260. [Google Scholar] [CrossRef]
- Hashemi, R.; Shafiee, G.; Motlagh, A.D.; Pasalar, P.; Esmailzadeh, A.; Siassi, F.; Larijani, B.; Heshmat, R. Sarcopenia and Its Associated Factors in Iranian Older Individuals: Results of SARIR Study. Arch. Gerontol. Geriatr. 2016, 66, 18–22. [Google Scholar] [CrossRef]
- Wu, I.; Lin, C.; Hsiung, C.A.; Wang, C.; Wu, C.; Chan, D.D.; Li, T.; Lin, W.; Huang, K.; Chen, C.; et al. Epidemiology of Sarcopenia among Community-dwelling Older Adults in Taiwan: A Pooled Analysis for a Broader Adoption of Sarcopenia Assessments. Geriatr. Gerontol. Int. 2014, 14, 52–60. [Google Scholar] [CrossRef]
- Bouchard, D.R.; Dionne, I.J.; Brochu, M. Sarcopenic/Obesity and Physical Capacity in Older Men and Women: Data From the Nutrition as a Determinant of Successful Aging (NuAge)—The Quebec Longitudinal Study. Obesity 2009, 17, 2082–2088. [Google Scholar] [CrossRef]
- Tiidus, P.M. Benefits of Estrogen Replacement for Skeletal Muscle Mass and Function in Post-Menopausal Females: Evidence from Human and Animal Studies. Eurasian J. Med. 2011, 43, 109–114. [Google Scholar] [CrossRef]
- Batsis, J.A.; Mackenzie, T.A.; Barre, L.K.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, Sarcopenic Obesity and Mortality in Older Adults: Results from the National Health and Nutrition Examination Survey III. Eur. J. Clin. Nutr. 2014, 68, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Drescher, C.; Konishi, M.; Ebner, N.; Springer, J. Loss of Muscle Mass: Current Developments in Cachexia and Sarcopenia Focused on Biomarkers and Treatment. J. Cachexia Sarcopenia Muscle 2015, 6, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Payette, H.; Roubenoff, R.; Jacques, P.F.; Dinarello, C.A.; Wilson, P.W.F.; Abad, L.W.; Harris, T. Insulin-like Growth Factor-1 and Interleukin 6 Predict Sarcopenia in Very Old Community-Living Men and Women: The Framingham Heart Study. J. Am. Geriatr. Soc. 2003, 51, 1237–1243. [Google Scholar] [CrossRef]
- Chen, H.-T.; Chung, Y.-C.; Chen, Y.-J.; Ho, S.-Y.; Wu, H.-J. Effects of Different Types of Exercise on Body Composition, Muscle Strength, and IGF-1 in the Elderly with Sarcopenic Obesity. J. Am. Geriatr. Soc. 2017, 65, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, H.; Loenneke, J.P.; Thiebaud, R.S.; Stager, J.M.; Abe, T. Possibility of Leg Muscle Hypertrophy by Ambulation in Older Adults: A Brief Review. Clin. Interv. Aging 2013, 8, 369–375. [Google Scholar] [CrossRef]
- Taaffe, D.R. Sarcopenia--Exercise as a Treatment Strategy. Aust. Fam. Physician 2006, 35, 130–134. [Google Scholar]
- Ormsbee, M.J.; Prado, C.M.; Ilich, J.Z.; Purcell, S.; Siervo, M.; Folsom, A.; Panton, L. Osteosarcopenic Obesity: The Role of Bone, Muscle, and Fat on Health. J. Cachexia Sarcopenia Muscle 2014, 5, 183–192. [Google Scholar] [CrossRef]
- Trouwborst, I.; Verreijen, A.; Memelink, R.; Massanet, P.; Boirie, Y.; Weijs, P.; Tieland, M. Exercise and Nutrition Strategies to Counteract Sarcopenic Obesity. Nutrients 2018, 10, 605. [Google Scholar] [CrossRef]
- Sadaqa, M.; Németh, Z.; Makai, A.; Prémusz, V.; Hock, M. Effectiveness of Exercise Interventions on Fall Prevention in Ambulatory Community-Dwelling Older Adults: A Systematic Review with Narrative Synthesis. Front. Public Health 2023, 11, 1209319. [Google Scholar] [CrossRef]
- Toigo, M.; Boutellier, U. New Fundamental Resistance Exercise Determinants of Molecular and Cellular Muscle Adaptations. Eur. J. Appl. Physiol. 2006, 97, 643–663. [Google Scholar] [CrossRef]
- Ormsbee, M.J.; Thyfault, J.P.; Johnson, E.A.; Kraus, R.M.; Choi, M.D.; Hickner, R.C. Fat Metabolism and Acute Resistance Exercise in Trained Men. J. Appl. Physiol. 2007, 102, 1767–1772. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, A.; Krawczyk, S.N.; Potiaumpai, M.; Signorile, J.F. High-Speed Circuit Training vs Hypertrophy Training to Improve Physical Function in Sarcopenic Obese Adults: A Randomized Controlled Trial. Exp. Gerontol. 2014, 60, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Talar, K.; Hernández-Belmonte, A.; Vetrovsky, T.; Steffl, M.; Kałamacka, E.; Courel-Ibáñez, J. Benefits of Resistance Training in Early and Late Stages of Frailty and Sarcopenia: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. J. Clin. Med. 2021, 10, 1630. [Google Scholar] [CrossRef] [PubMed]
- Ghiotto, L.; Muollo, V.; Tatangelo, T.; Schena, F.; Rossi, A.P. Exercise and Physical Performance in Older Adults with Sarcopenic Obesity: A Systematic Review. Front. Endocrinol. 2022, 13, 913953. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.-W.; Jung, S.-W.; Kim, S.-W.; Lee, J.-M.; Jung, H.C.; Song, J.-K. Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial. Int. J. Environ. Res. Public. Health 2021, 18, 6762. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Kohl, M.; Fröhlich, M.; Jakob, F.; Engelke, K.; von Stengel, S.; Schoene, D. Effects of High-Intensity Resistance Training on Osteopenia and Sarcopenia Parameters in Older Men with Osteosarcopenia-One-Year Results of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2020, 35, 1634–1644. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater Reliability: The Kappa Statistic. Biochem. Medica 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Hartmann, K.E.; Matchar, D.B.; Chang, S.M. Chapter 6: Assessing Applicability of Medical Test Studies in Systematic Reviews. In Methods Guide for Medical Test Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2012. [Google Scholar]
- Julian, P.T.H.; Jelena, S.; Matthew, J.P.; Roy, G.E.; Jonathan, A.C.S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook/current/chapter-08 (accessed on 2 November 2023).
- Lee, Y.-H.; Lee, P.-H.; Lin, L.-F.; Liao, C.-D.; Liou, T.-H.; Huang, S.-W. Effects of Progressive Elastic Band Resistance Exercise for Aged Osteosarcopenic Adiposity Women. Exp. Gerontol. 2021, 147, 111272. [Google Scholar] [CrossRef]
- Banitalebi, E.; Faramarzi, M.; Ghahfarokhi, M.M.; SavariNikoo, F.; Soltani, N.; Bahramzadeh, A. Osteosarcopenic Obesity Markers Following Elastic Band Resistance Training: A Randomized Controlled Trial. Exp. Gerontol. 2020, 135, 110884. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, K.S.S.; Dias, J.M.D.; Araújo, M.C.; Pinheiro, A.C.; Moreira, B.S.; Dias, R.C. Effects of a Progressive Resistance Exercise Program with High-Speed Component on the Physical Function of Older Women with Sarcopenic Obesity: A Randomized Controlled Trial. Braz. J. Phys. Ther. 2016, 20, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Nabuco, H.C.G.; Tomeleri, C.M.; Fernandes, R.R.; Sugihara Junior, P.; Cavalcante, E.F.; Cunha, P.M.; Antunes, M.; Nunes, J.P.; Venturini, D.; Barbosa, D.S.; et al. Effect of Whey Protein Supplementation Combined with Resistance Training on Body Composition, Muscular Strength, Functional Capacity, and Plasma-Metabolism Biomarkers in Older Women with Sarcopenic Obesity: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Nutr. ESPEN 2019, 32, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-W.; Ku, J.-W.; Lin, L.-F.; Liao, C.-D.; Chou, L.-C.; Liou, T.-H. Body Composition Influenced by Progressive Elastic Band Resistance Exercise of Sarcopenic Obesity Elderly Women: A Pilot Randomized Controlled Trial. Eur. J. Phys. Rehabil. Med. 2017, 53, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.M.; Ribeiro, A.S.; Tomeleri, C.M.; Schoenfeld, B.J.; Silva, A.M.; Souza, M.F.; Nascimento, M.A.; Sardinha, L.B.; Cyrino, E.S. The Effects of Resistance Training Volume on Osteosarcopenic Obesity in Older Women. J. Sports Sci. 2018, 36, 1564–1571. [Google Scholar] [CrossRef]
- Liao, C.-D.; Tsauo, J.-Y.; Huang, S.-W.; Ku, J.-W.; Hsiao, D.-J.; Liou, T.-H. Effects of Elastic Band Exercise on Lean Mass and Physical Capacity in Older Women with Sarcopenic Obesity: A Randomized Controlled Trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Weineck, M.; Kohl, M.; von Stengel, S.; Giessing, J.; Fröhlich, M.; Schoene, D. High Intensity Resistance Exercise Training to Improve Body Composition and Strength in Older Men With Osteosarcopenia. Results of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). Front. Sports Act. Living 2020, 2, 4. [Google Scholar] [CrossRef]
- Frimel, T.N.; Sinacore, D.R.; Villareal, D.T. Exercise Attenuates the Weight-Loss-Induced Reduction in Muscle Mass in Frail Obese Older Adults. Med. Sci. Sports Exerc. 2008, 40, 1213. [Google Scholar] [CrossRef]
- Chen, N.; He, X.; Feng, Y.; Ainsworth, B.E.; Liu, Y. Effects of Resistance Training in Healthy Older People with Sarcopenia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Rev. Aging Phys. Act. 2021, 18, 23. [Google Scholar] [CrossRef]
- Vlietstra, L.; Hendrickx, W.; Waters, D.L. Exercise Interventions in Healthy Older Adults with Sarcopenia: A Systematic Review and Meta-Analysis. Australas. J. Ageing 2018, 37, 169–183. [Google Scholar] [CrossRef]
- Santos, L.; Ribeiro, A.S.; Schoenfeld, B.J.; Nascimento, M.A.; Tomeleri, C.M.; Souza, M.F.; Pina, F.L.C.; Cyrino, E.S. The Improvement in Walking Speed Induced by Resistance Training Is Associated with Increased Muscular Strength but Not Skeletal Muscle Mass in Older Women. Eur. J. Sport Sci. 2017, 17, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Borde, R.; Hortobágyi, T.; Granacher, U. Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis. Sports Med. Auckl. NZ 2015, 45, 1693–1720. [Google Scholar] [CrossRef]
- Steib, S.; Schoene, D.; Pfeifer, K. Dose-Response Relationship of Resistance Training in Older Adults: A Meta-Analysis. Med. Sci. Sports Exerc. 2010, 42, 902. [Google Scholar] [CrossRef]
- Zachary, Y.; Kerr, M.A.; Christy, L.; Collins, M.A.; Dawn Comstock, R. Epidemiology of Weight Training-Related Injuries Presenting to United States Emergency Departments, 1990 to 2007. Available online: https://journals.sagepub.com/doi/10.1177/0363546509351560 (accessed on 5 January 2024).
- Liao, C.-D.; Tsauo, J.-Y.; Wu, Y.-T.; Cheng, C.-P.; Chen, H.-C.; Huang, Y.-C.; Chen, H.-C.; Liou, T.-H. Effects of Protein Supplementation Combined with Resistance Exercise on Body Composition and Physical Function in Older Adults: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef] [PubMed]
- Bergia, R.E.; Hudson, J.L.; Campbell, W.W. Effect of Whey Protein Supplementation on Body Composition Changes in Women: A Systematic Review and Meta-Analysis. Nutr. Rev. 2018, 76, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.-J.; Liao, C.-D.; Tsai, M.-W.; Chen, C.-N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef]
- Yin, Y.-H.; Liu, J.Y.W.; Välimäki, M. Dietary Behaviour Change Intervention for Managing Sarcopenic Obesity among Community-Dwelling Older People: A Pilot Randomised Controlled Trial. BMC Geriatr. 2023, 23, 597. [Google Scholar] [CrossRef]
- Espinoza, S.E.; Lee, J.L.; Wang, C.-P.; Ganapathy, V.; MacCarthy, D.; Pascucci, C.; Musi, N.; Volpi, E. Intranasal Oxytocin Improves Lean Muscle Mass and Lowers LDL Cholesterol in Older Adults with Sarcopenic Obesity: A Pilot Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2021, 22, 1877–1882.e2. [Google Scholar] [CrossRef]
- Jabbour, J.; Rahme, M.; Mahfoud, Z.R.; El-Hajj Fuleihan, G. Effect of High Dose Vitamin D Supplementation on Indices of Sarcopenia and Obesity Assessed by DXA among Older Adults: A Randomized Controlled Trial. Endocrine 2022, 76, 162–171. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Rothstein Criticisms of Meta-Analysis. In Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 377–387. ISBN 978-0-470-74338-6. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Reference | Participants | Duration | Intervention | Outcomes | Summary of Results |
|---|---|---|---|---|---|
| Paolo M. Cunha [49] | 68 Age (≥60 years) | 12 weeks | -Chest press -Horizontal leg press -Seated row -Knee extension -Preacher curl (free weights) -Leg curl -Triceps pushdown -Seated calf raise -Participants of the 1 set per exercise group performed 1 set of 10–15 repetitions maximum for each exercise -Participants of 3 sets per exercise group performed 3 sets of 10–15 repetitions maximum for each exercise | -Body composition was assessed by dual X-ray absorptiometry -Strength was evaluated by 1 repetition maximum testing | -Both training groups increased their scores from pre- to post-training for skeletal muscle mass and total strength. The control group decreased its score for strength. -Only three set groups showed a reduction in relative body fat after the intervention period. |
| Yu-Hao Lee [44] | 27 Age (60–90 years) | 12 weeks | Resistance band exercise targeted: shoulders, arms, lower limbs, chest, and abdomen, with 1–2 exercises included for each muscle group | -Body composition was assessed by data obtained from the dual X-ray absorptiometry Functional capacity was assessed by: -FFR -SLS -10 MW -TUG -30 CST Strength was assessed by grip strength | -The exercise group showed improvement for 10 MW, TUG, and 30 CST. -No significant improvement in FFR, SLS, and grip strength was observed. -No significant differences were observed between the study and control groups in terms of changes to body composition. |
| Karina S. S. Vasconcelos [46] | 31 Age (65–80 years) | 10 weeks |
-Closed and open chain exercise in each leg for posterior, anterior, lateral, and medial muscles of hips and knees -In the first 4 weeks, the resistance exercise program emphasised muscle strengthening and endurance, with concentric and eccentric movements performed at a low speed -From the fifth week, the high-speed “as fast as possible” component was added to the program for concentric movements of exercises -From the seventh to tenth week, concentric and eccentric movements were performed at high speeds -The exercise was only for the legs and hips | -Muscle strength of the lower limbs was measured as the knee extensor strength in joules (J), power in watts (w), and fatigue in percentage (%) using an isokinetic dynamometer -Functional capacity was measured by a 10 MW test | -There were no significant between-group differences for any of the outcomes regarding knee extensors (strength, power, and fatigue). -There was only a significant within-group difference for knee extensor power. -No significant difference regarding the 10 MW test. |
| Shih-Wei HUANG [48] | 35 Age (>60 years) | 12 weeks | -Resistance band exercise -One or two types of exercises for training each muscle group, namely the shoulders, arms, lower limbs, chest, and abdomen | Body composition was assessed by data obtained from the dual X-ray absorptiometry | -BF% and total fat mass in the training group showed significant improvement compared to the control group. -No significant difference was found regarding SMI, BMI, trunk fat, trunk muscle mass, and TSM compared to the control group. |
| Ebrahim Banitalebi [45] | 63 Age (65–80 years) | 12 weeks | -Resistance band exercise -Exercise included major muscle groups (legs, back, abdomen, chest, shoulder, and arms) | Body composition was assessed by data obtained from the dual X-ray absorptiometry Functional capacities were assessed by: -10 MW -30 CST -TUG Strength was assessed by a grip strength test | -30 CST and grip strength showed significant improvement compared to the control group. -No significant improvement was noticed for 10 MW, TUG, BMI, and BF%. |
| Liao et al. [50] | 56 Age (60–80 years) | 12 weeks | -Resistance band exercise -Seated chest press -Seated row -Seated shoulder press -Knee extension -Knee flexion -Hip flexion -Hip extension | Body composition was assessed by data obtained from the dual X-ray absorptiometry. Strength was assessed by: -grip strength Functional capacity was assessed by: -FFR -SLS -10 MW -TUG -30 CST | BF%, TSM, ALM, LMI, AMI, SMI (%), FFR, SLS, 10 MW, TUG, and 30 CST have all shown significant improvement among the experimental group compared to the control group. |
| Nabuco et al. [47] | 26 Age (>60 years) | 12 weeks | -Chest press -Horizontal leg press -Seated row -Knee extension -Preacher curl (free weights) -Leg curl -Triceps pushdown -Seated calf raise | Body composition was assessed by data obtained from the dual X-ray absorptiometry Functional capacity assessed by: -10 MW -RSP Muscle strength was assessed by 1 repetition maximum testing | -Total LST, lower LST, ALST, total fat mass, and BF% have all shown more improvement in the whey + exercise group than the placebo + exercise group. -No significant difference between the two groups was found for trunk fat mass, WC, HC, WHR, 10 MW, RSP, knee extension, chest press, preacher curl, and total strength. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Debes, W.A.; Sadaqa, M.; Németh, Z.; Aldardour, A.; Prémusz, V.; Hock, M. Effect of Resistance Exercise on Body Composition and Functional Capacity in Older Women with Sarcopenic Obesity—A Systematic Review with Narrative Synthesis. J. Clin. Med. 2024, 13, 441. https://doi.org/10.3390/jcm13020441
Debes WA, Sadaqa M, Németh Z, Aldardour A, Prémusz V, Hock M. Effect of Resistance Exercise on Body Composition and Functional Capacity in Older Women with Sarcopenic Obesity—A Systematic Review with Narrative Synthesis. Journal of Clinical Medicine. 2024; 13(2):441. https://doi.org/10.3390/jcm13020441
Chicago/Turabian StyleDebes, Wesam A., Munseef Sadaqa, Zsanett Németh, Ahmad Aldardour, Viktória Prémusz, and Márta Hock. 2024. "Effect of Resistance Exercise on Body Composition and Functional Capacity in Older Women with Sarcopenic Obesity—A Systematic Review with Narrative Synthesis" Journal of Clinical Medicine 13, no. 2: 441. https://doi.org/10.3390/jcm13020441
APA StyleDebes, W. A., Sadaqa, M., Németh, Z., Aldardour, A., Prémusz, V., & Hock, M. (2024). Effect of Resistance Exercise on Body Composition and Functional Capacity in Older Women with Sarcopenic Obesity—A Systematic Review with Narrative Synthesis. Journal of Clinical Medicine, 13(2), 441. https://doi.org/10.3390/jcm13020441