Influence of Seasonality and Public-Health Interventions on the COVID-19 Pandemic in Northern Europe

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Methodology
2.1. Data
2.2. Statistical Analysis
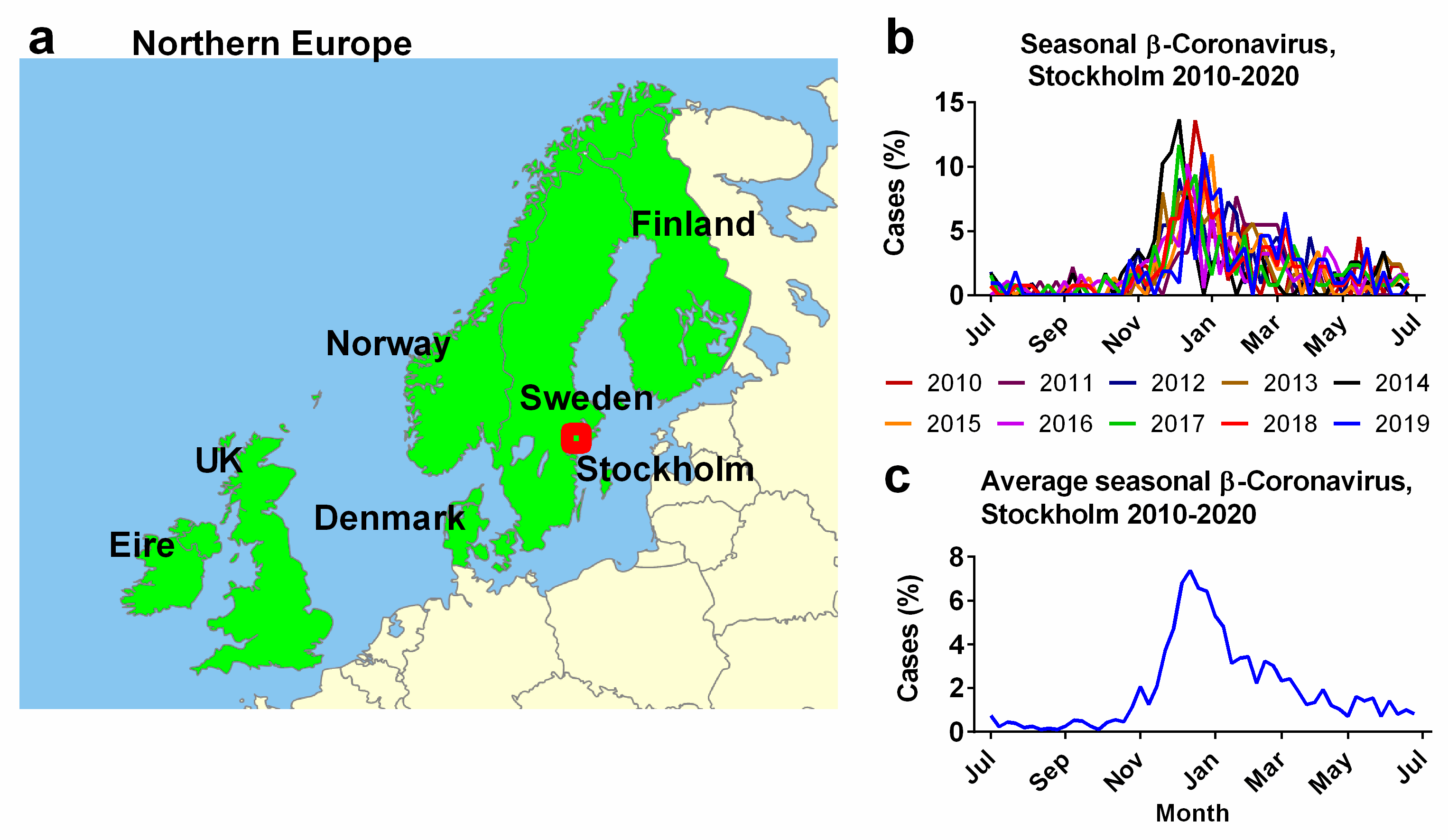
2.3. Study Area
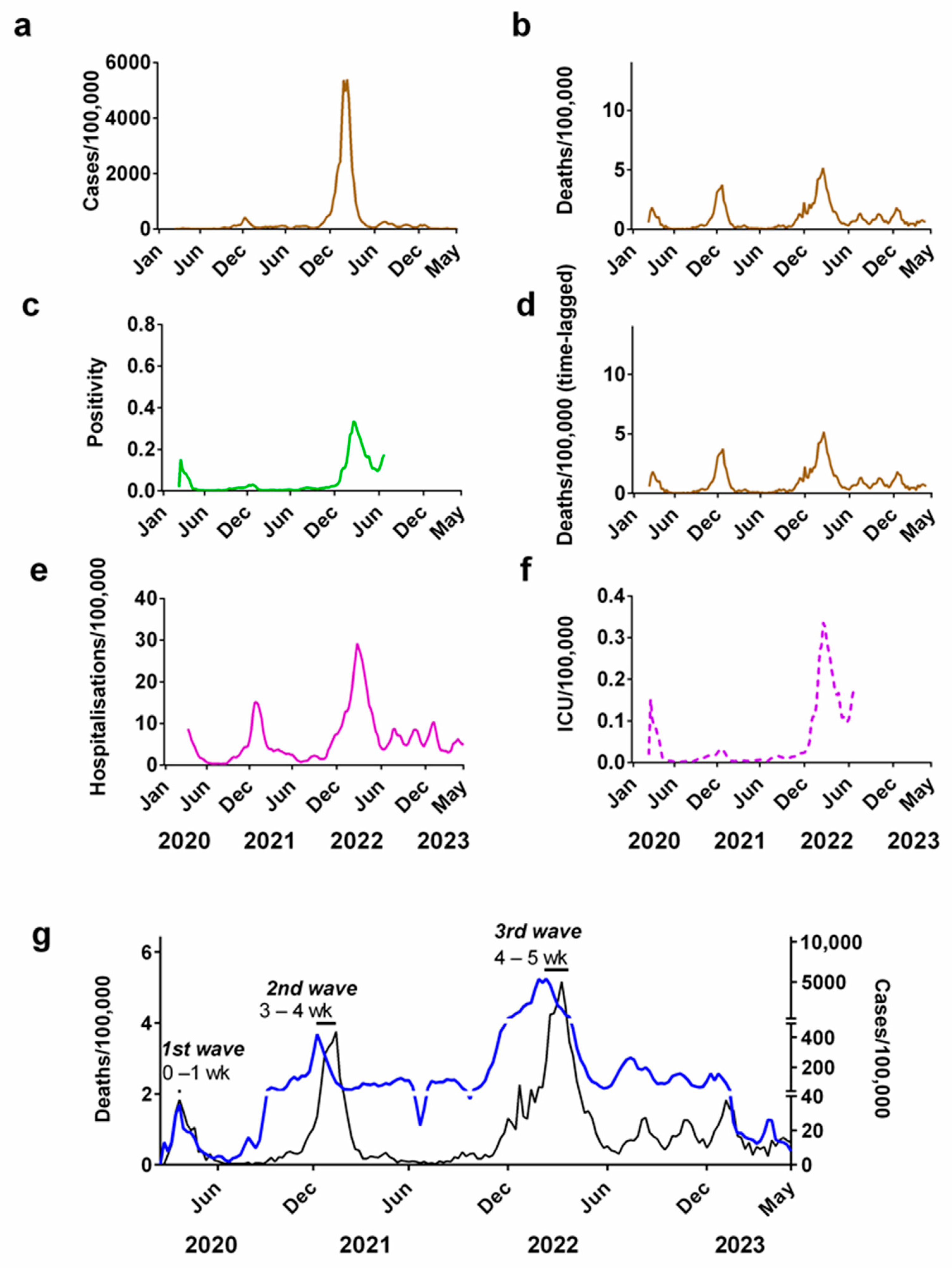
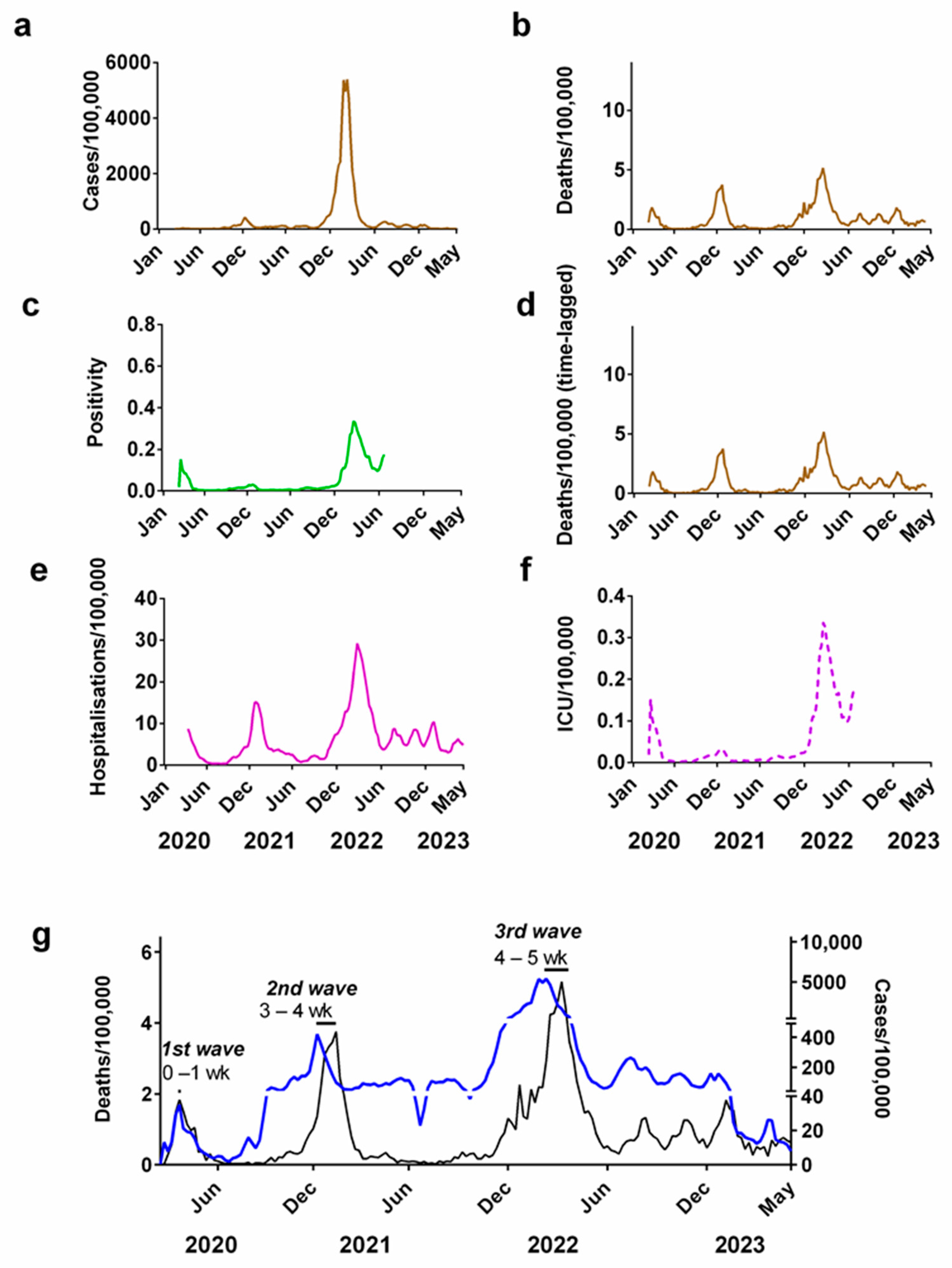
2.4. Describing the Progression of the COVID-19 Pandemic for Each Country
3. Results and Discussion
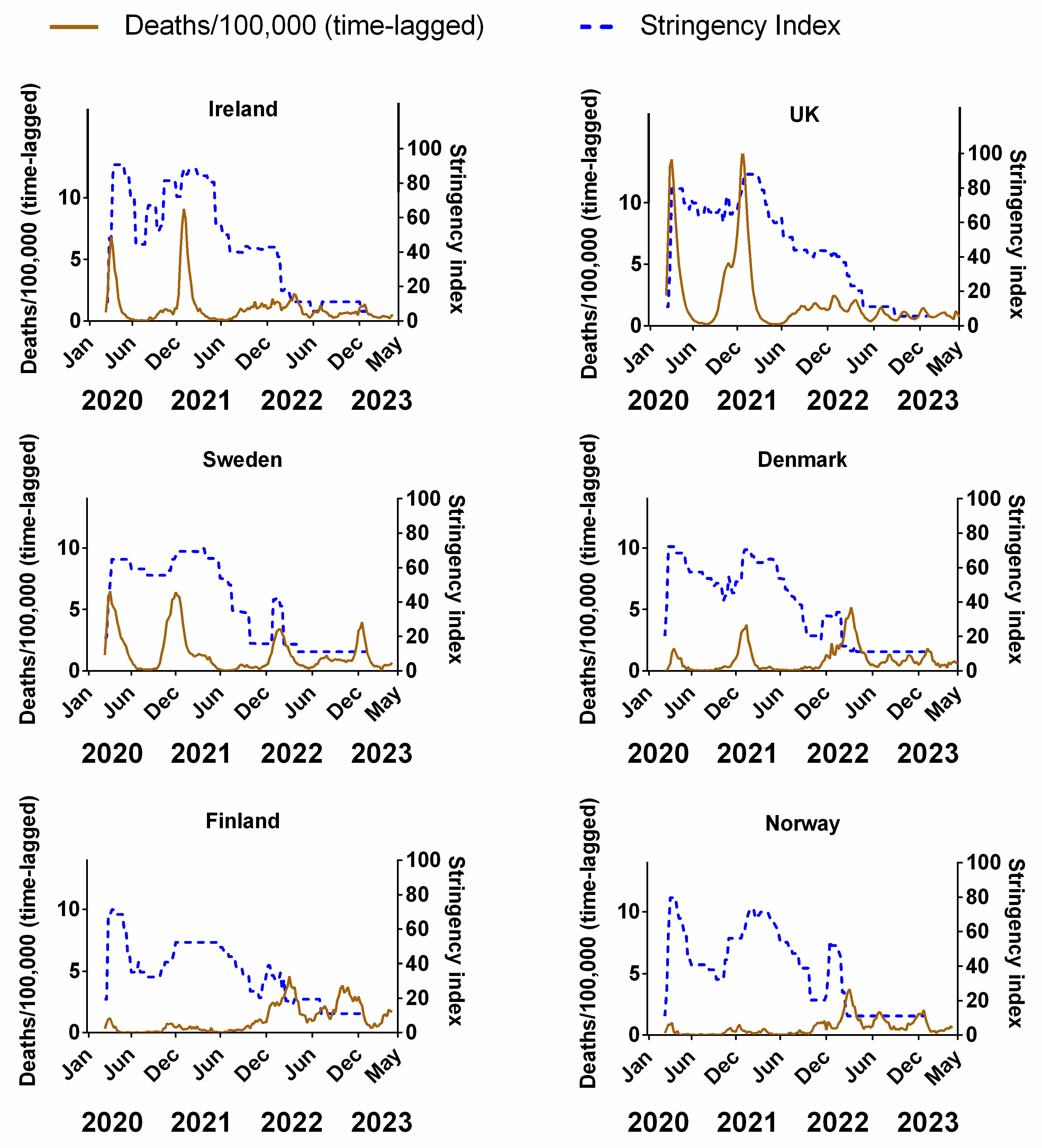
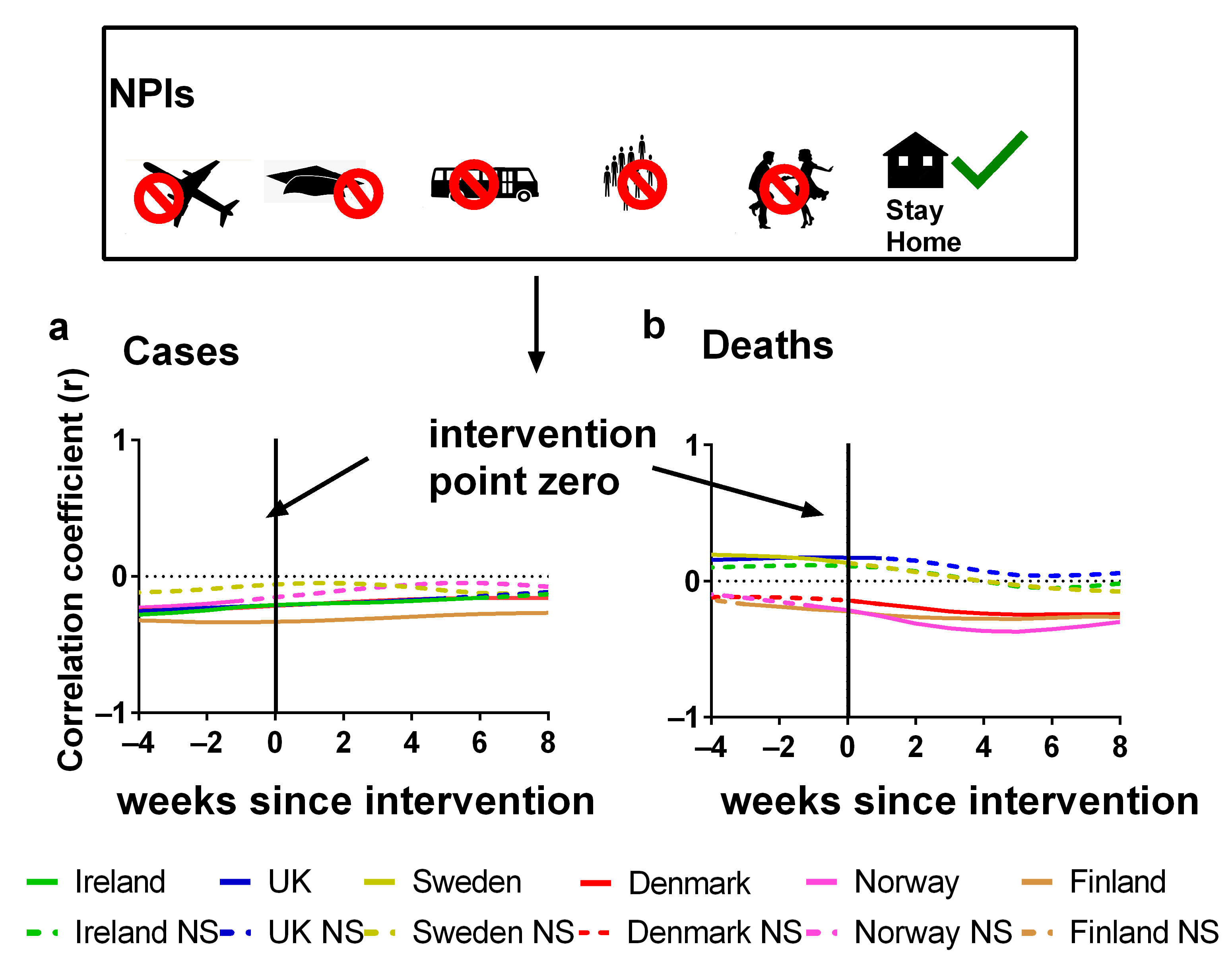
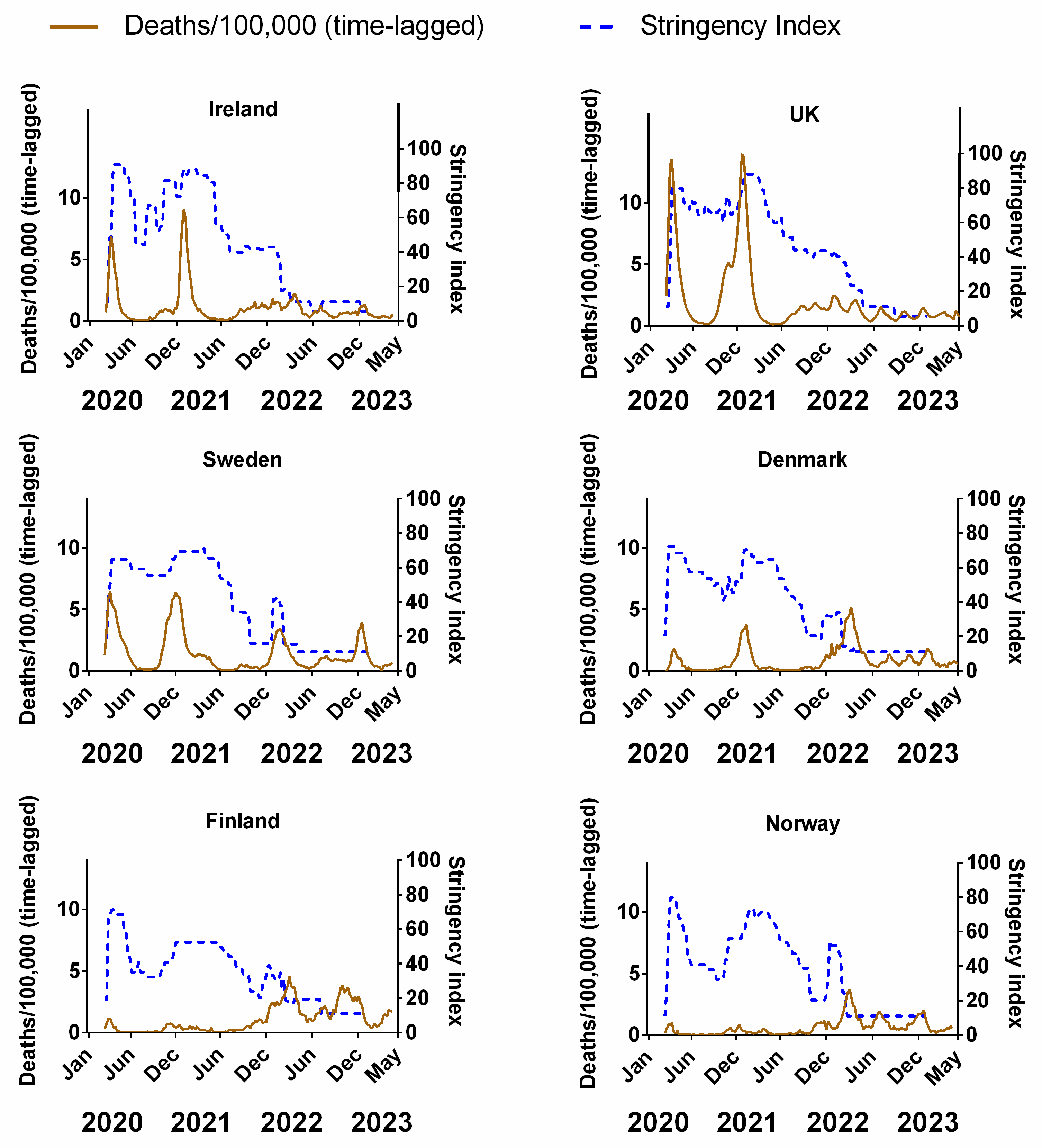
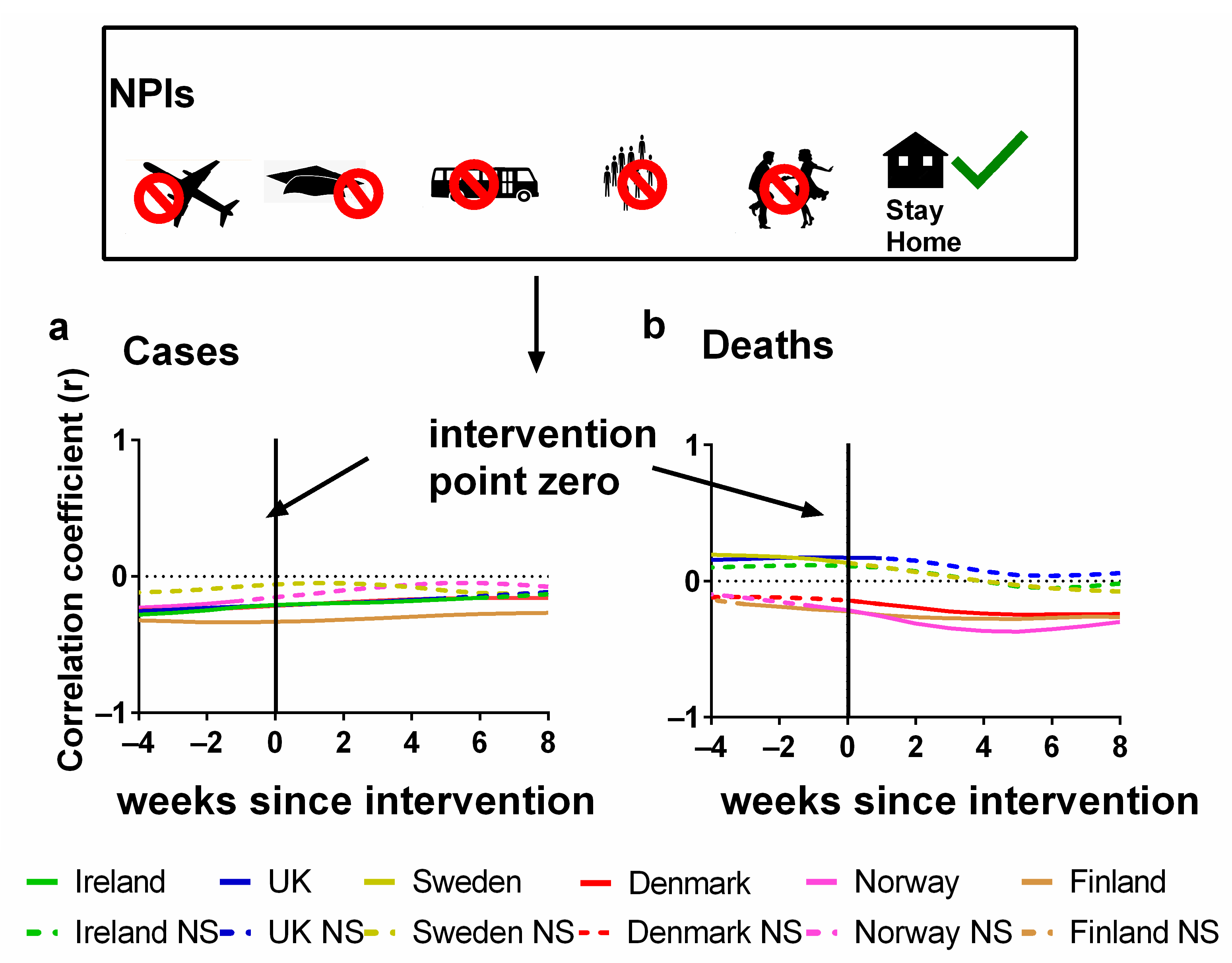
3.1. Influence of Non-Pharmaceutical Interventions on Pandemic Progression in Northern Europe
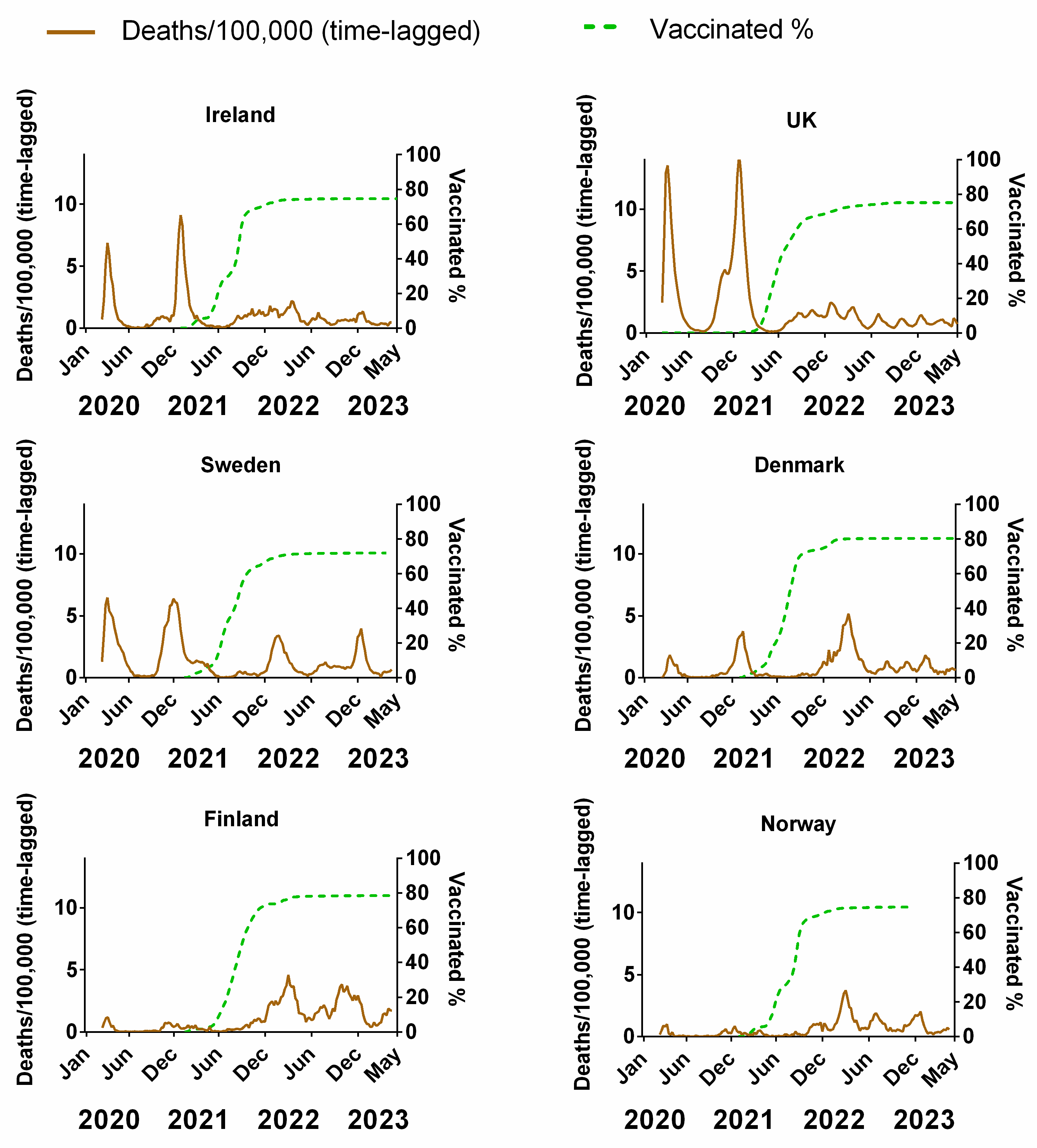
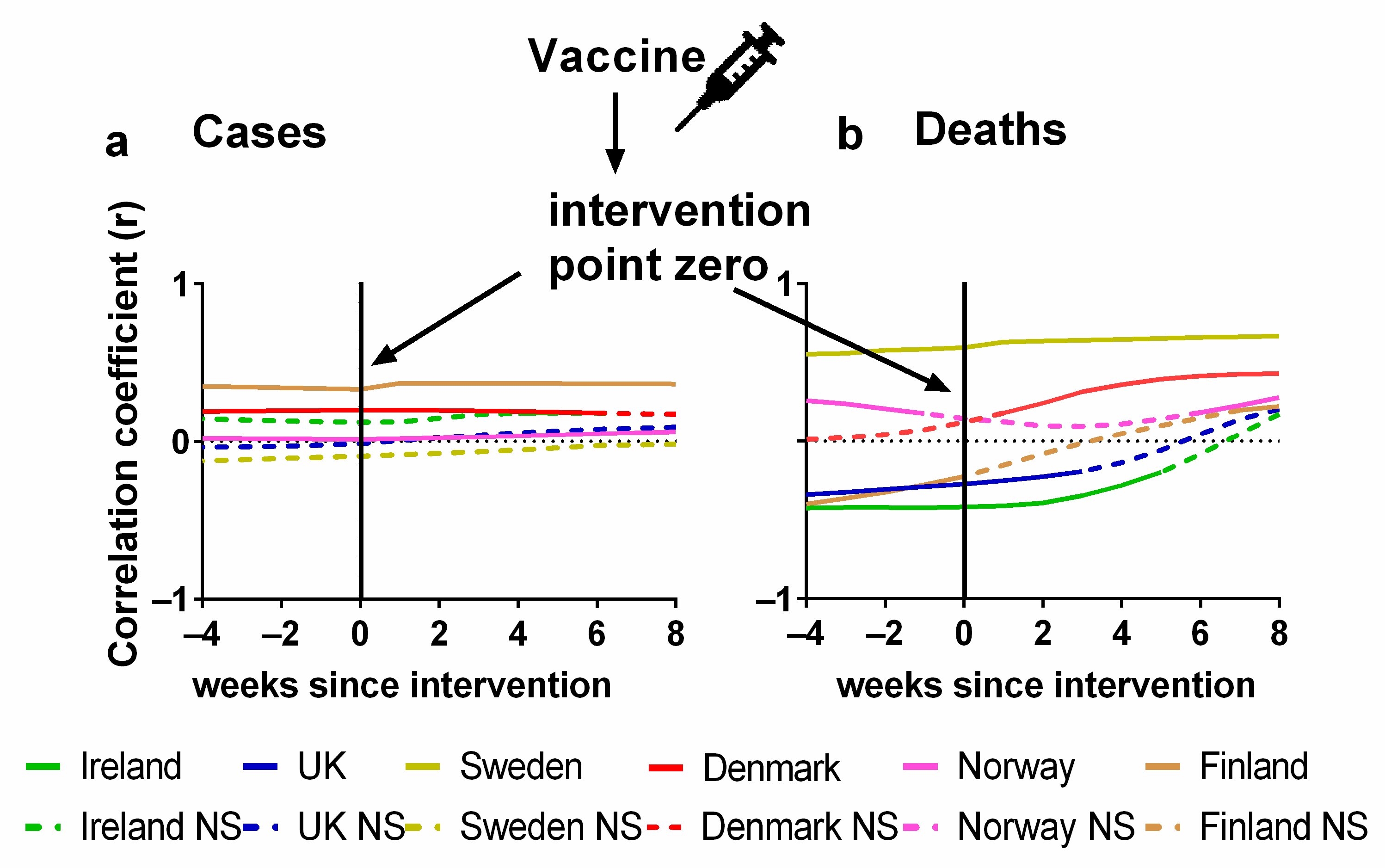
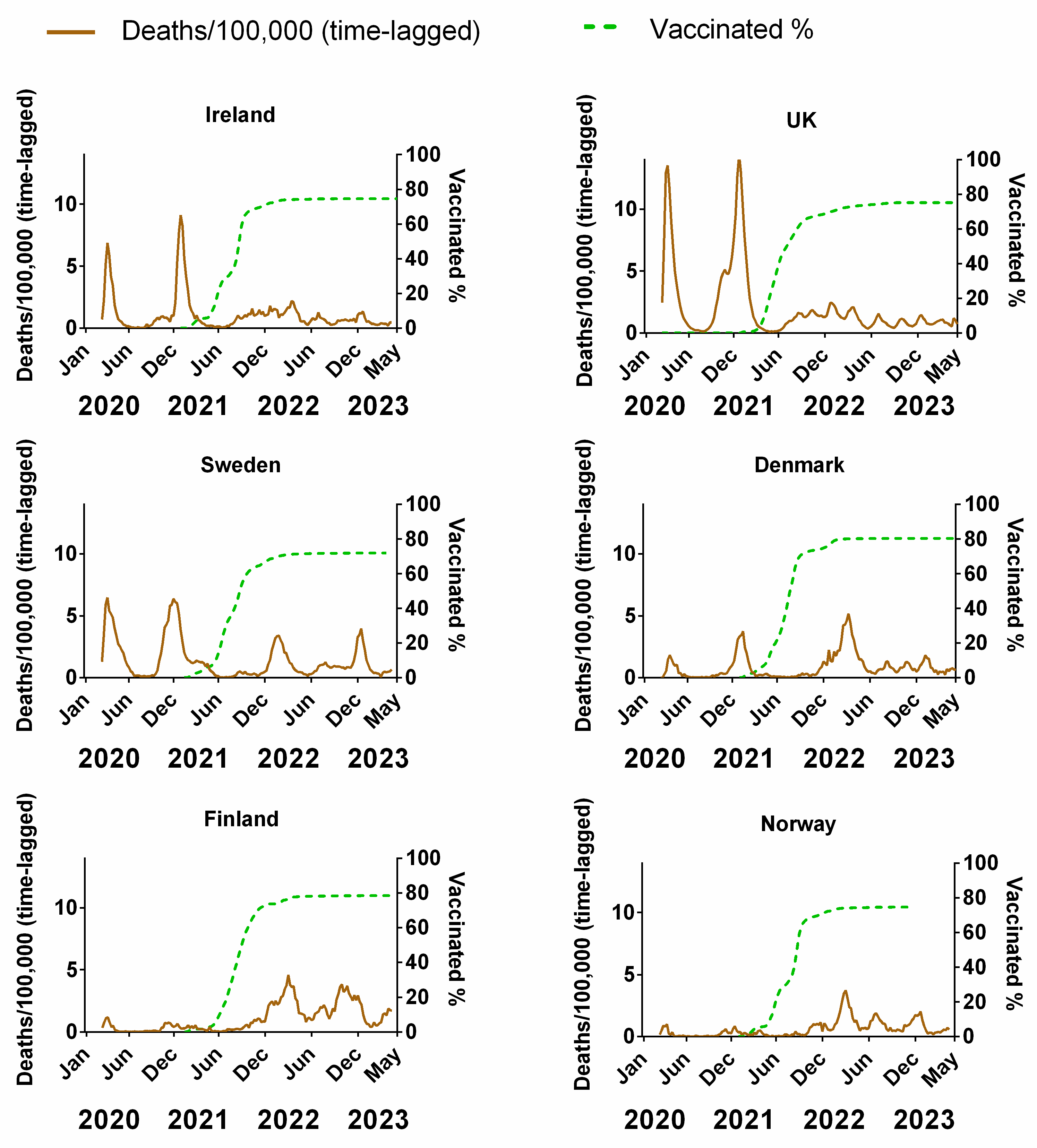
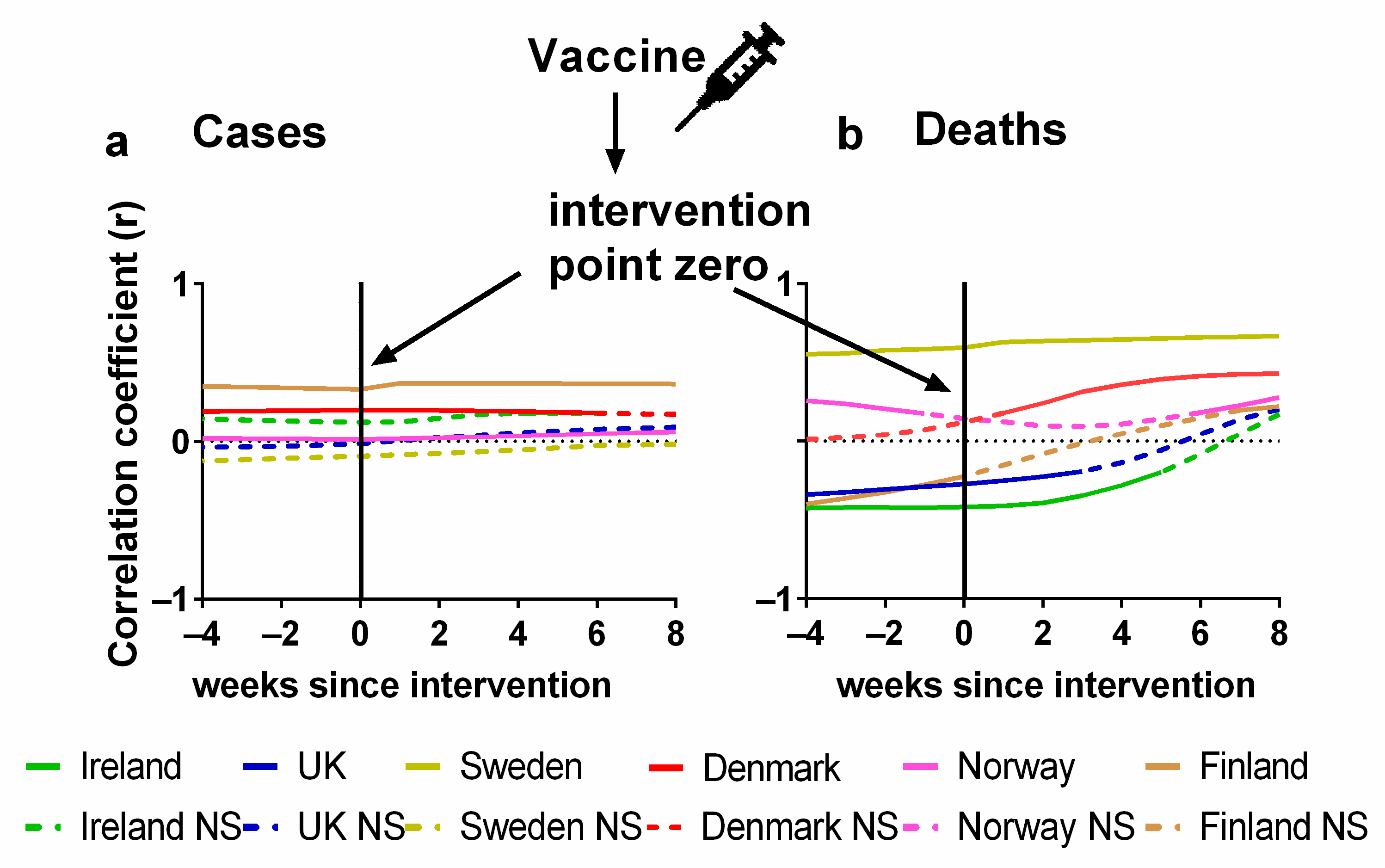
3.2. Influence of Vaccinations on Pandemic Progression in Northern Europe
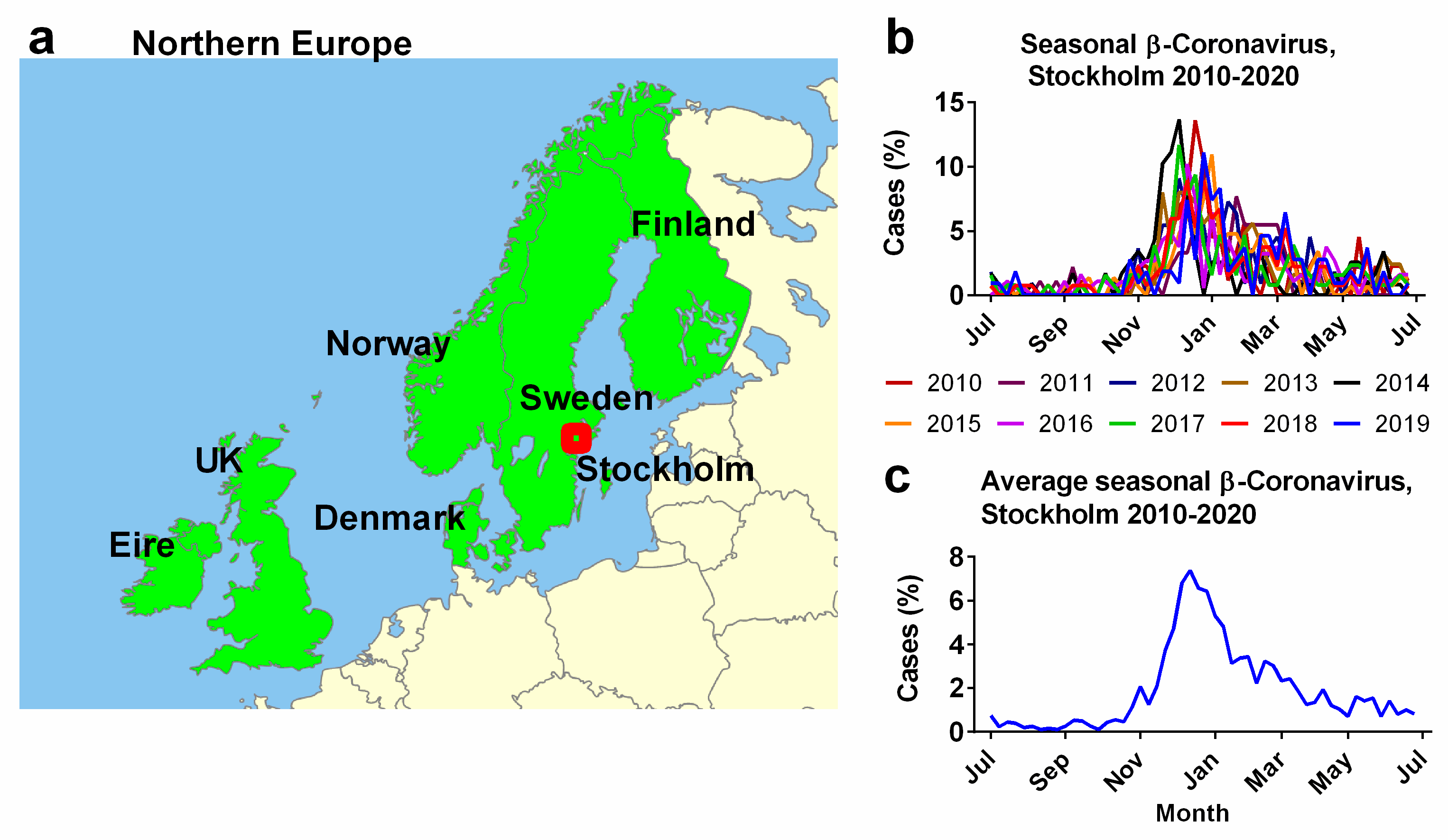
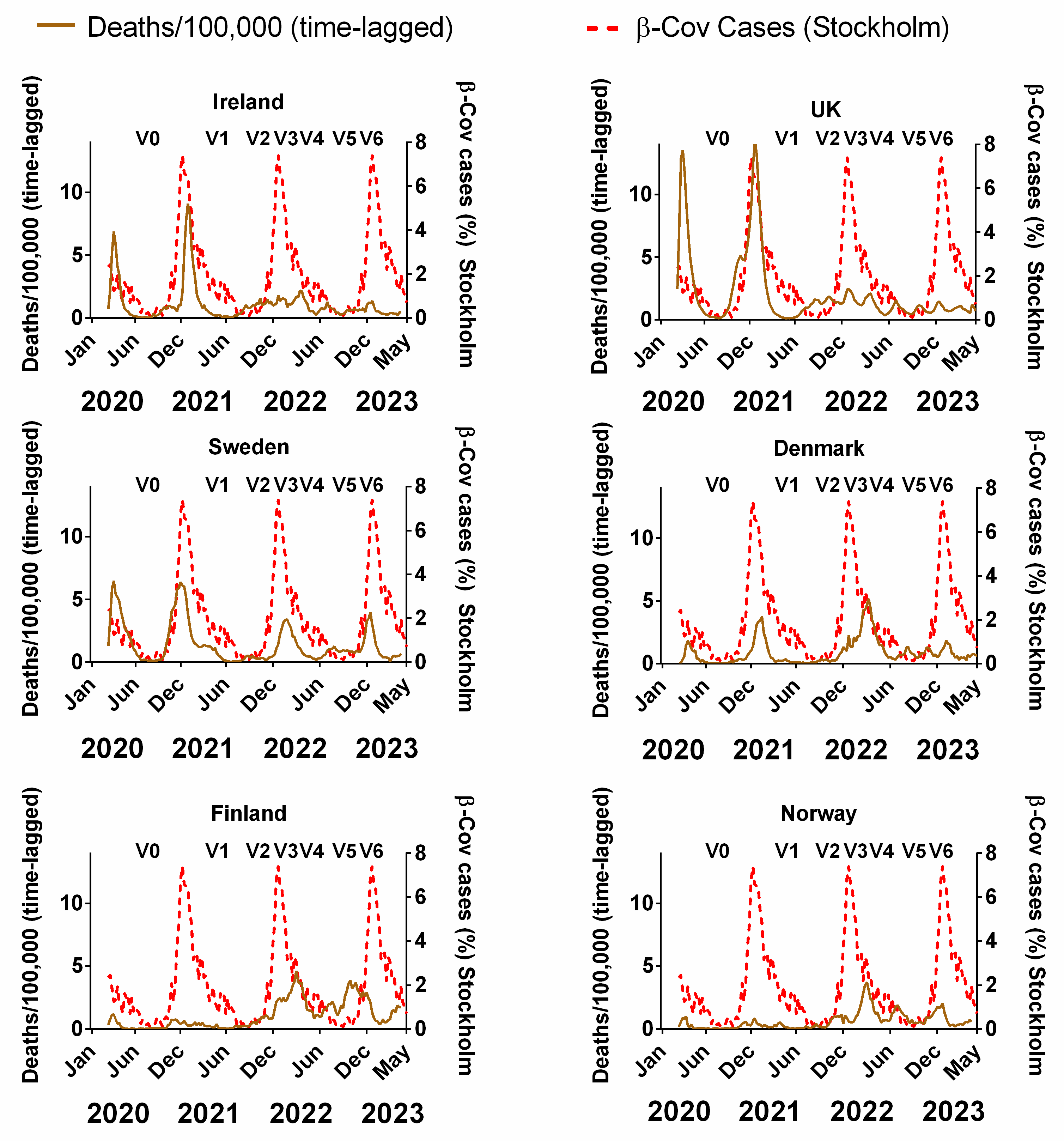
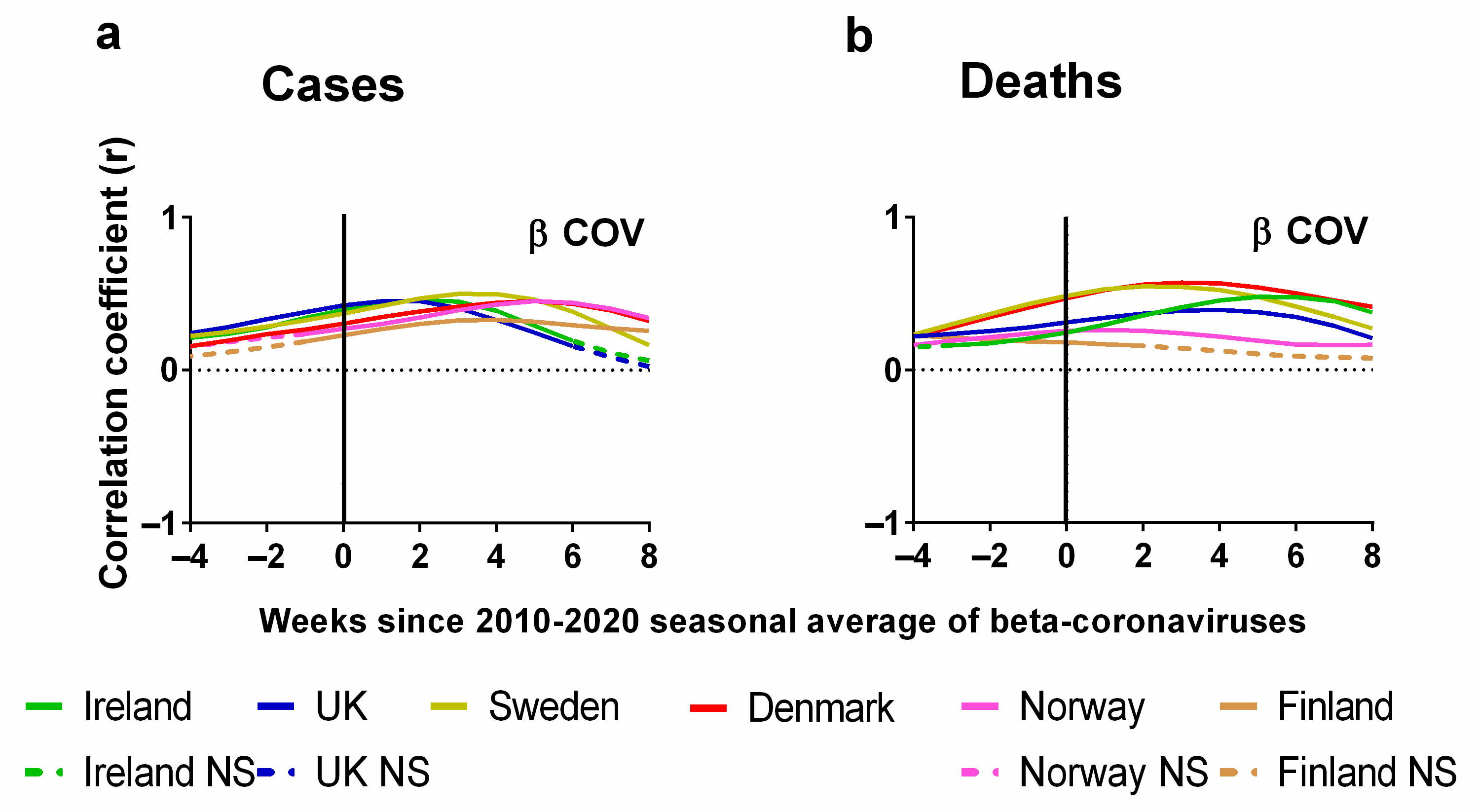
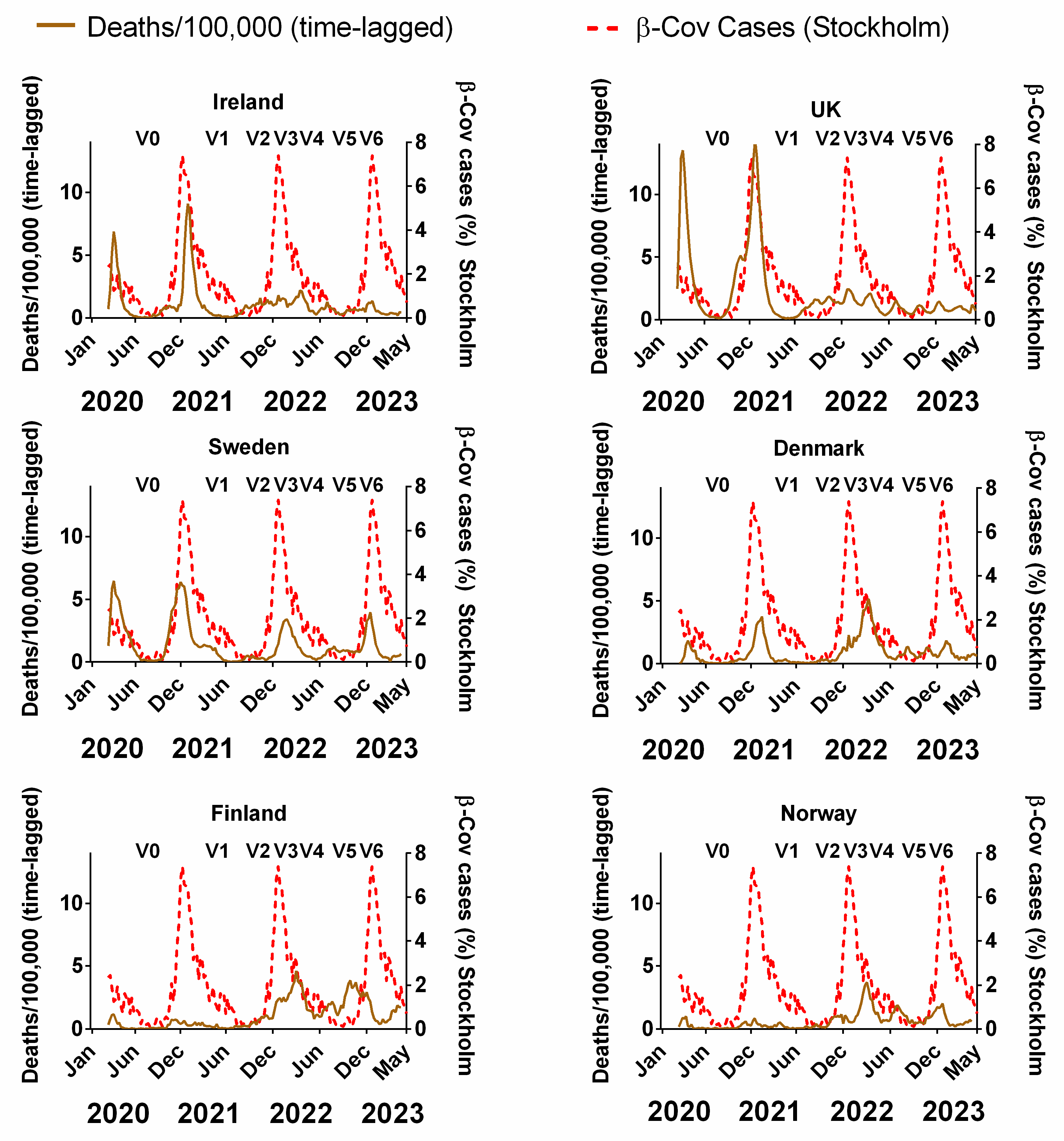
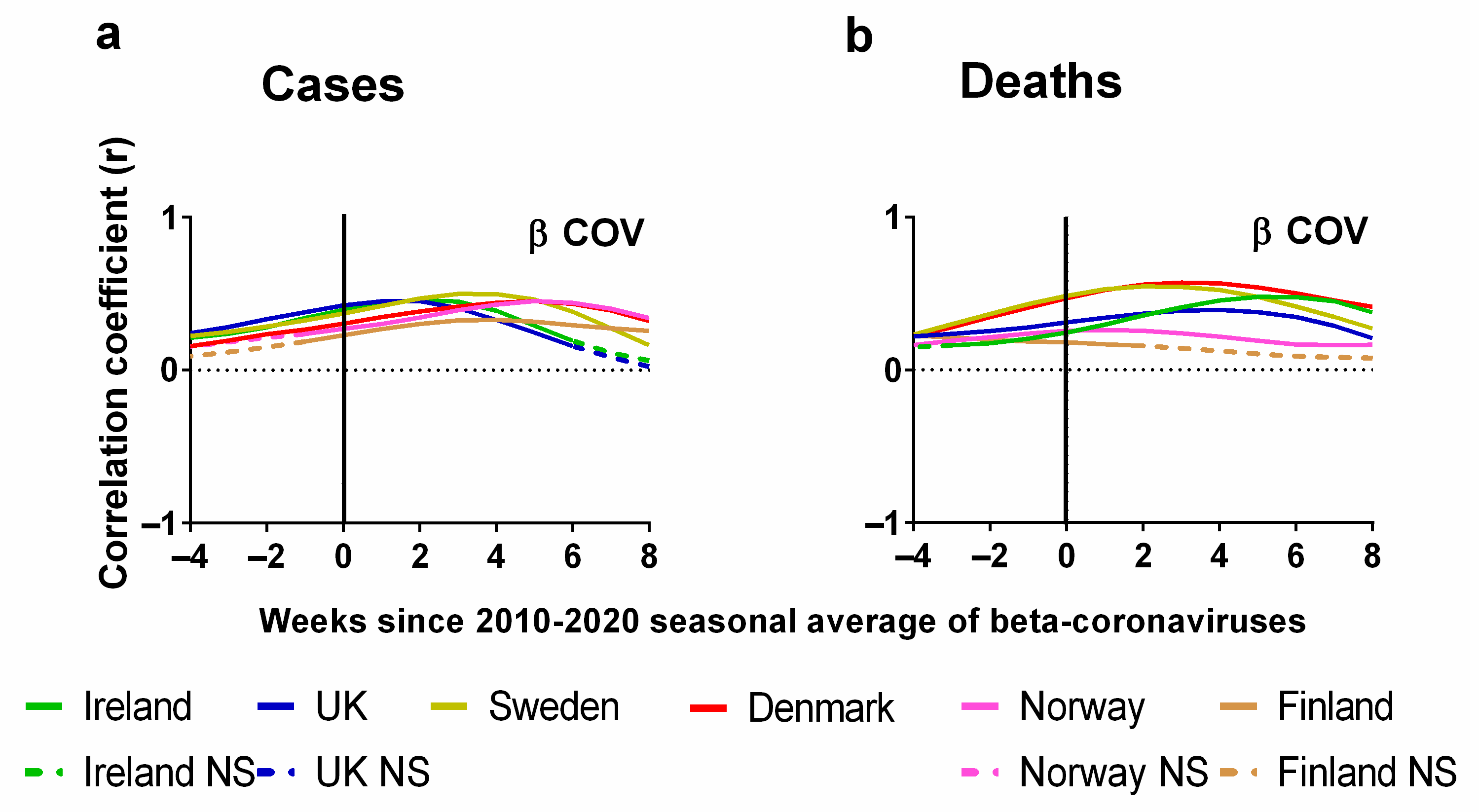
3.3. Influence of Seasonality on Pandemic Progression in Northern Europe
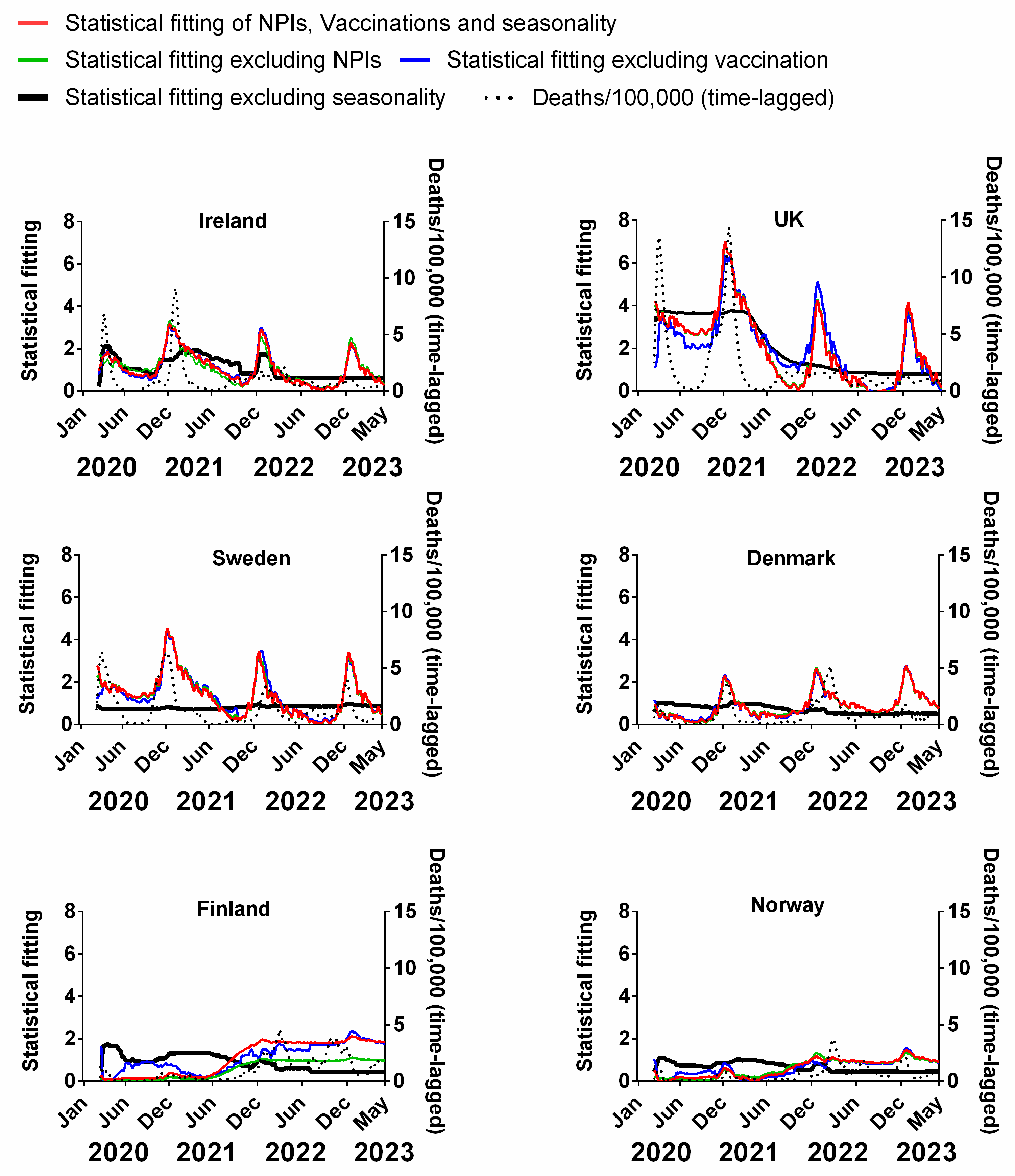
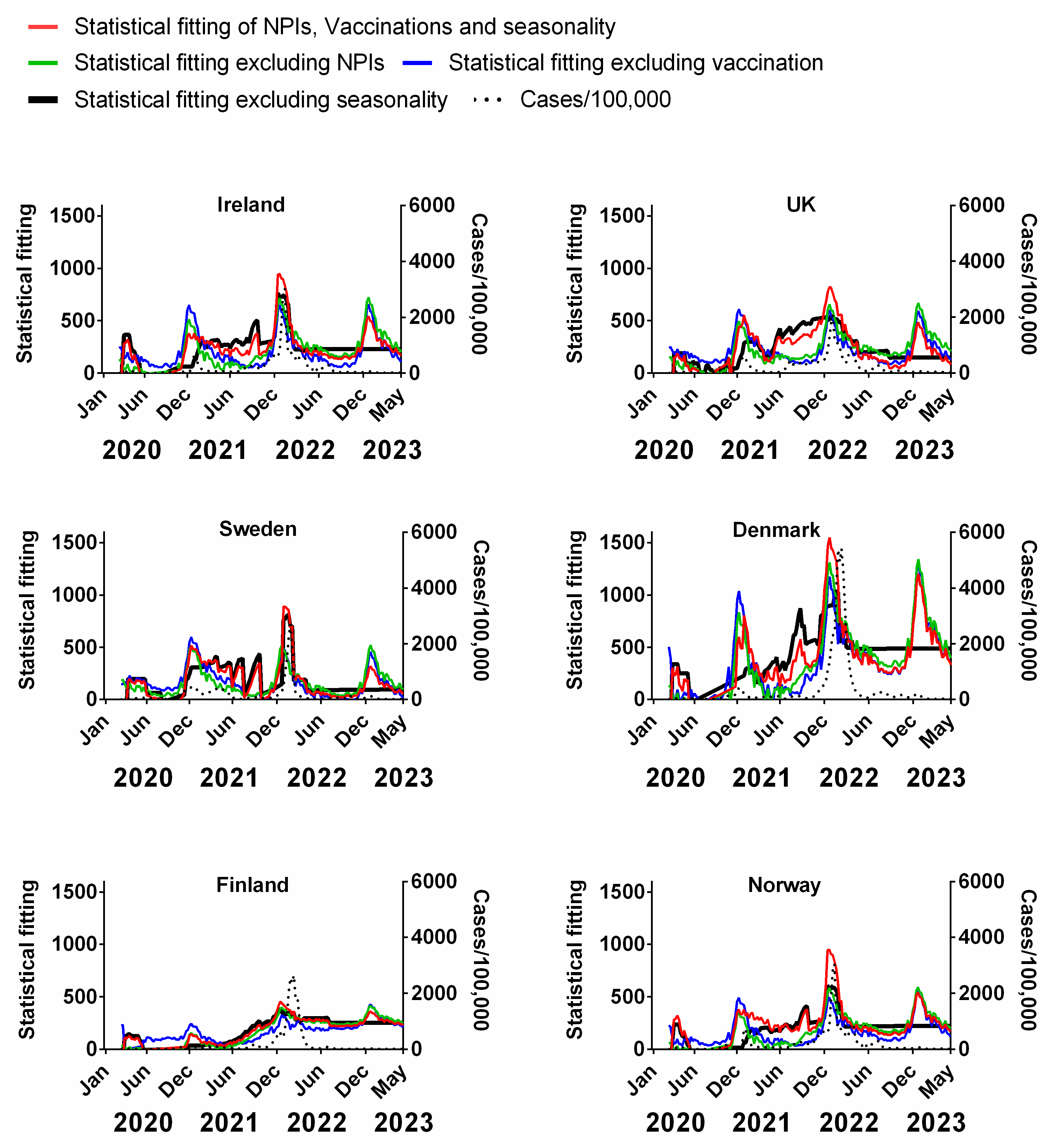
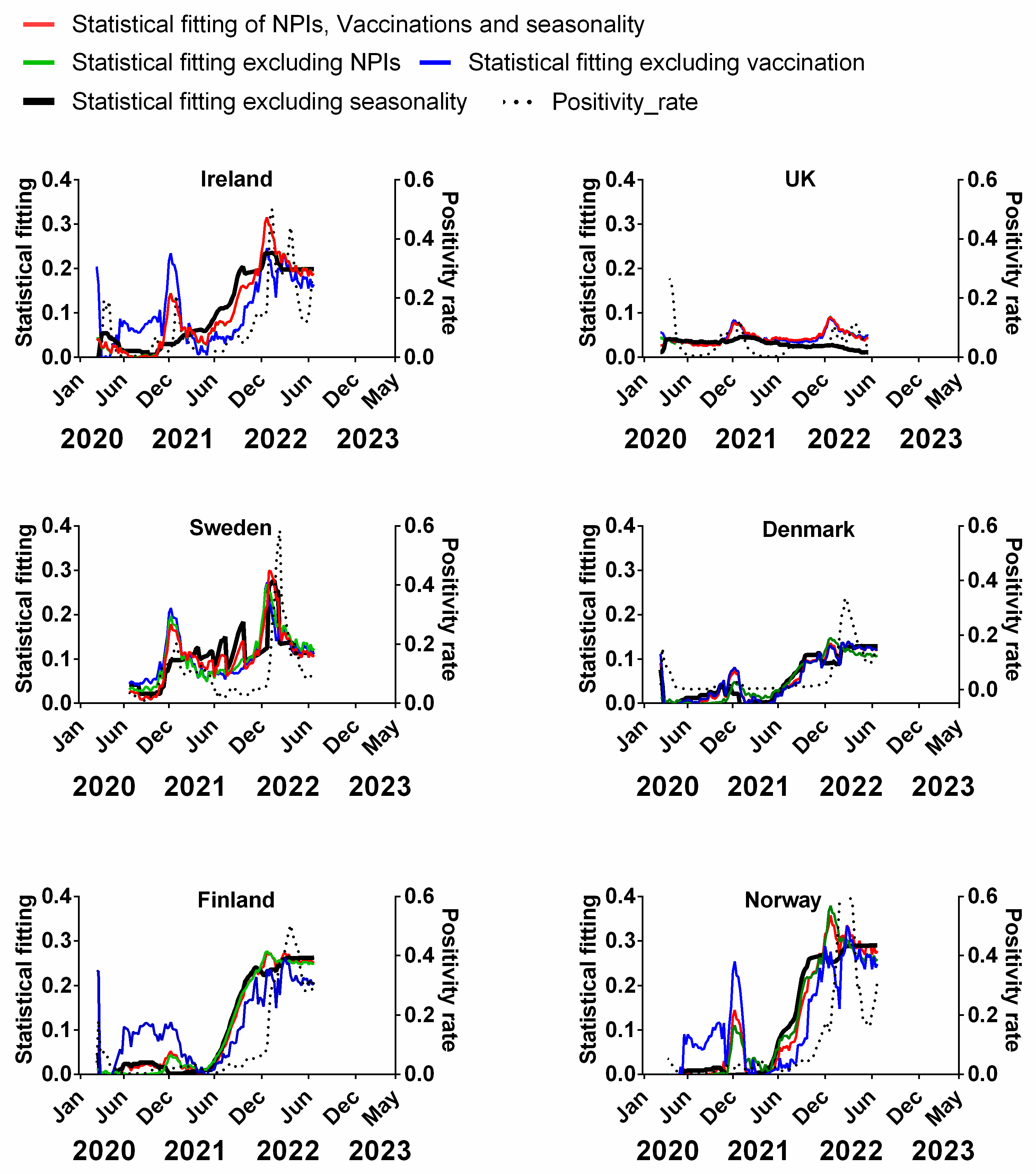
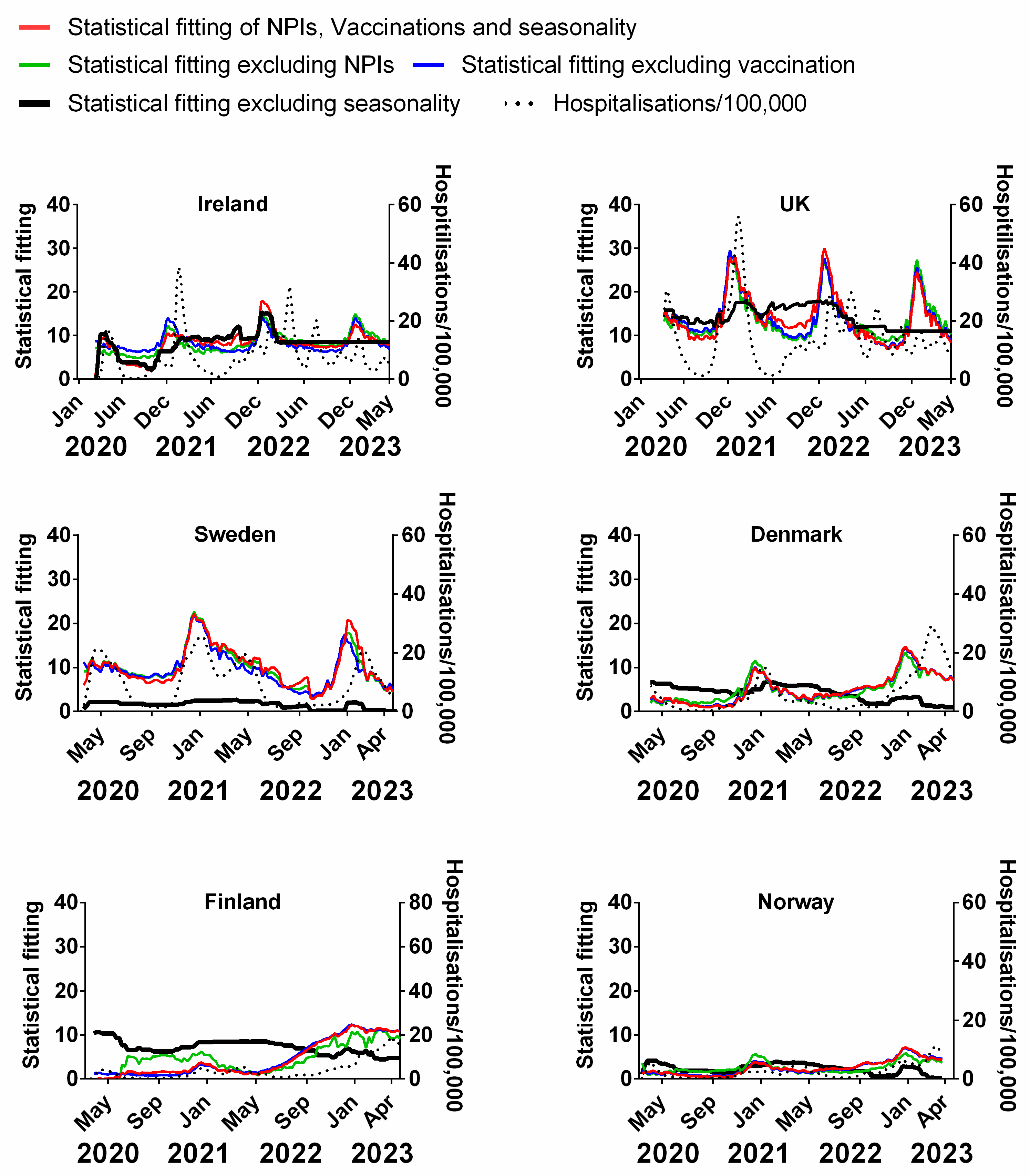
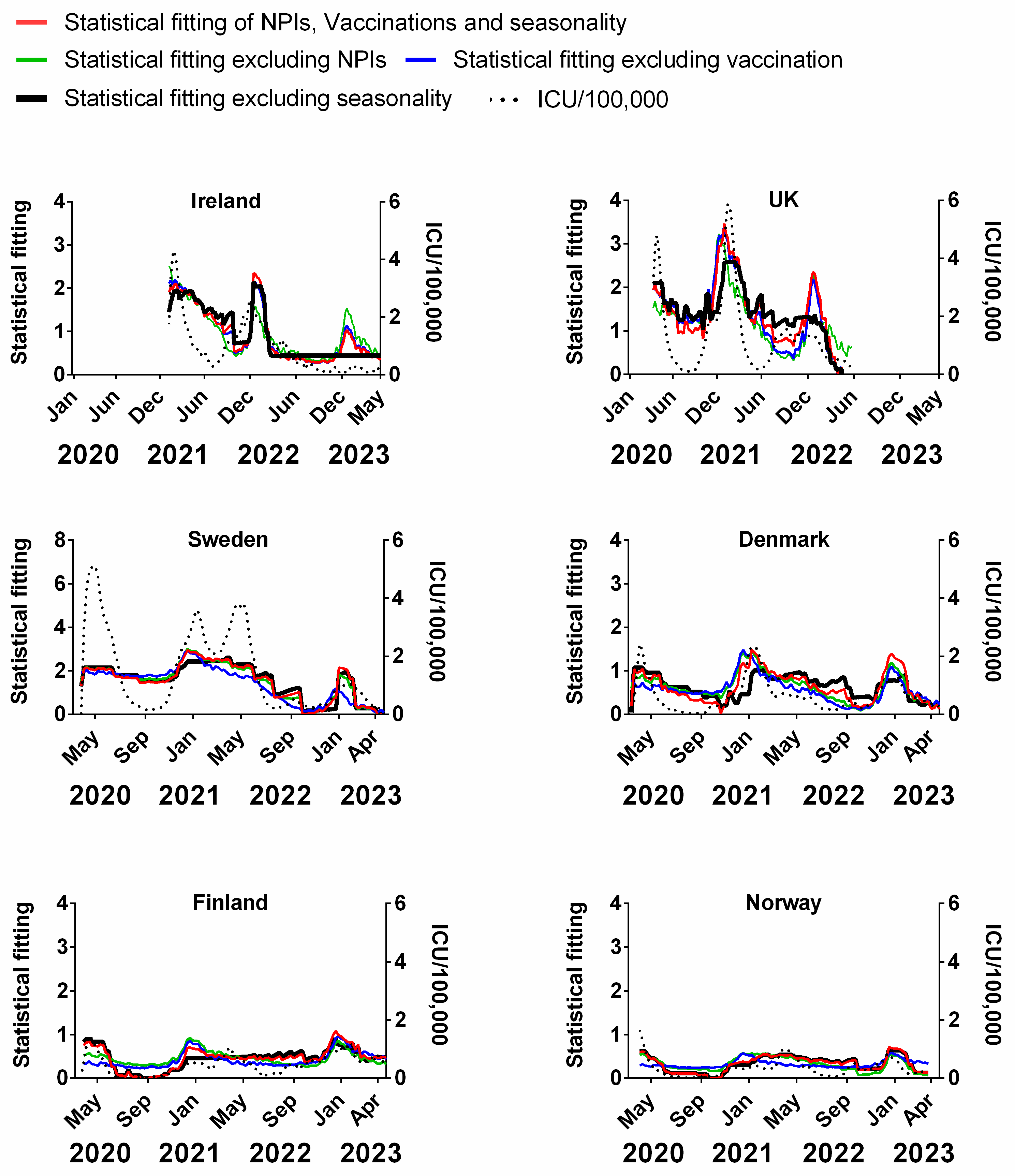
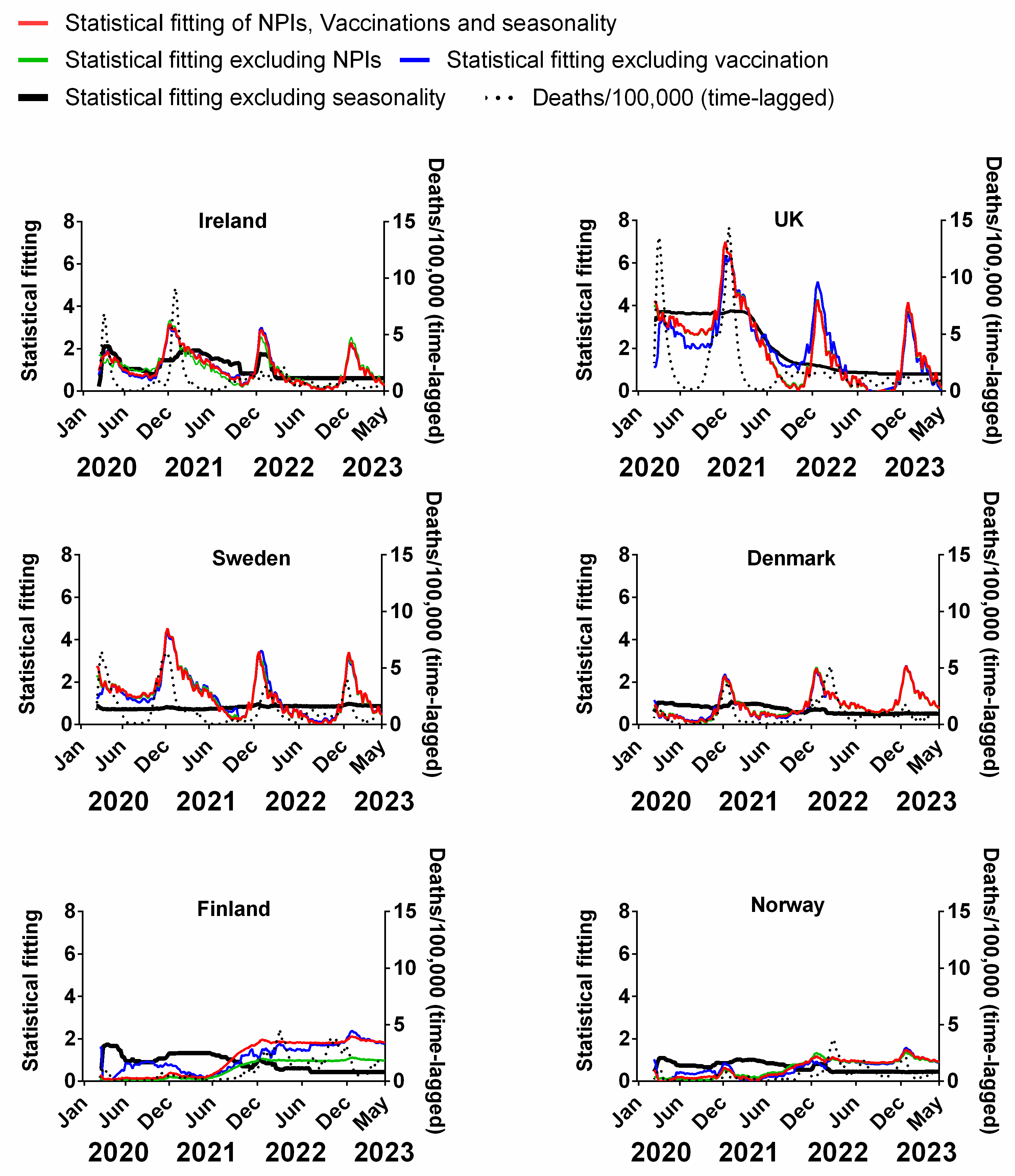
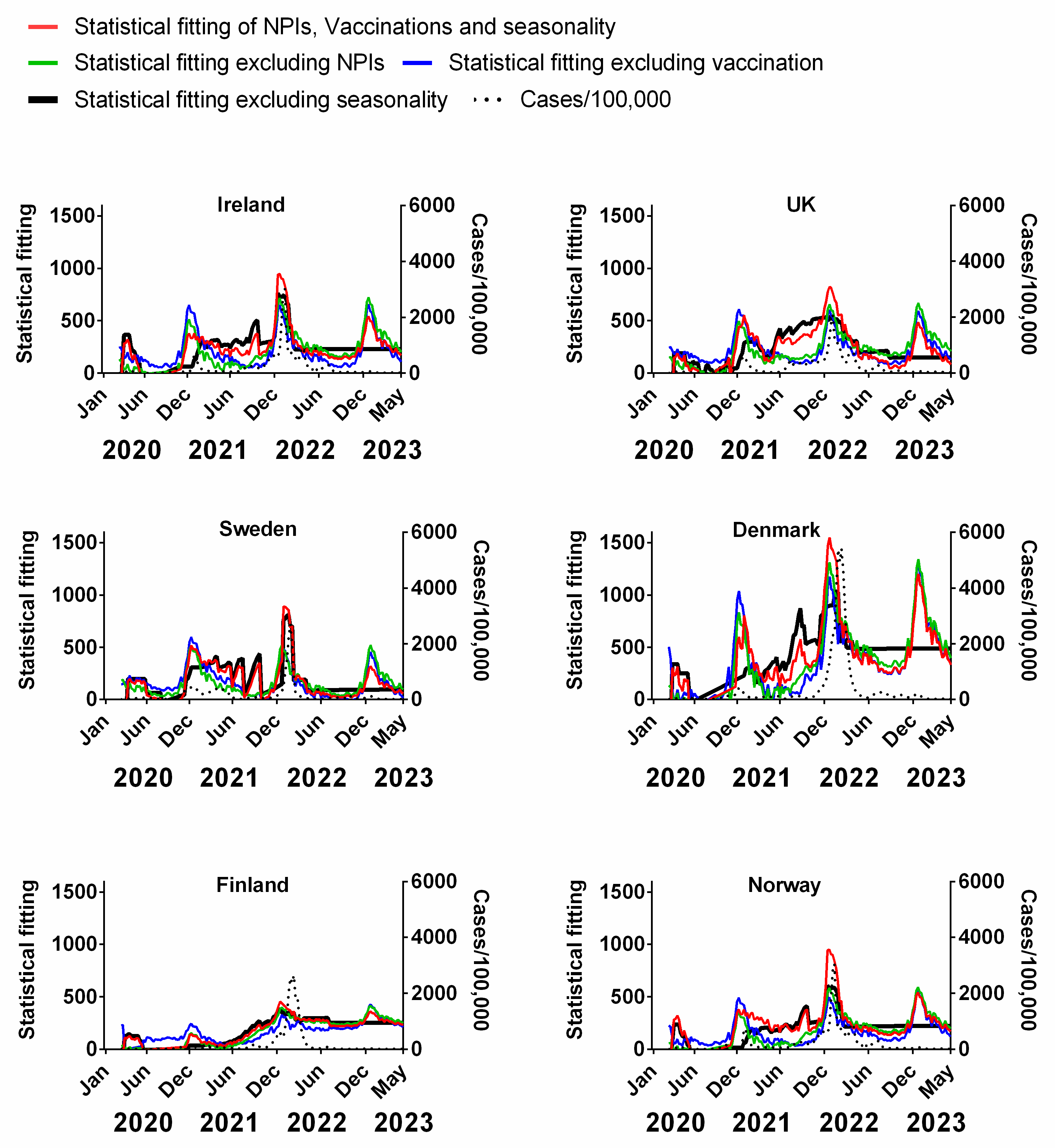
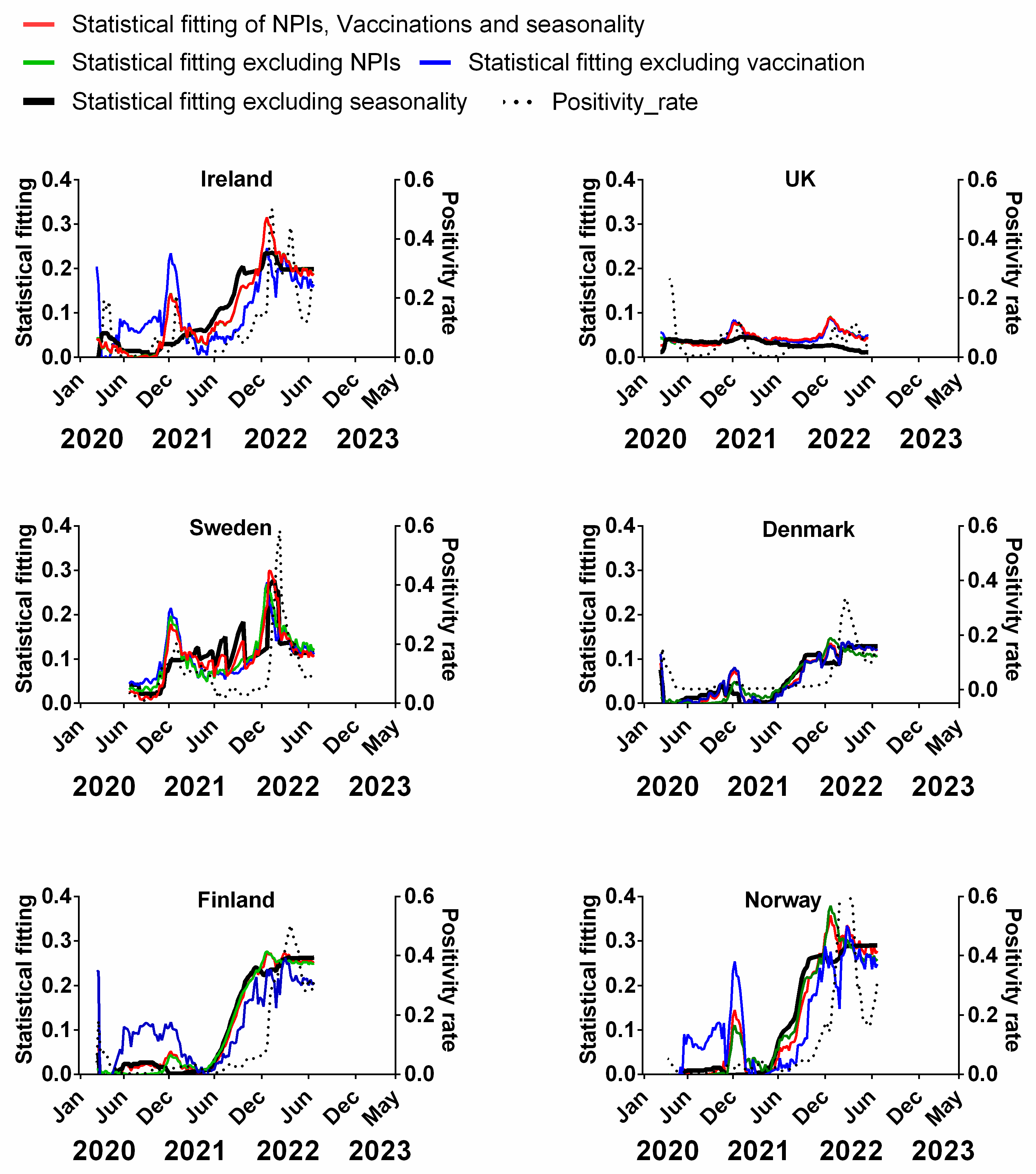
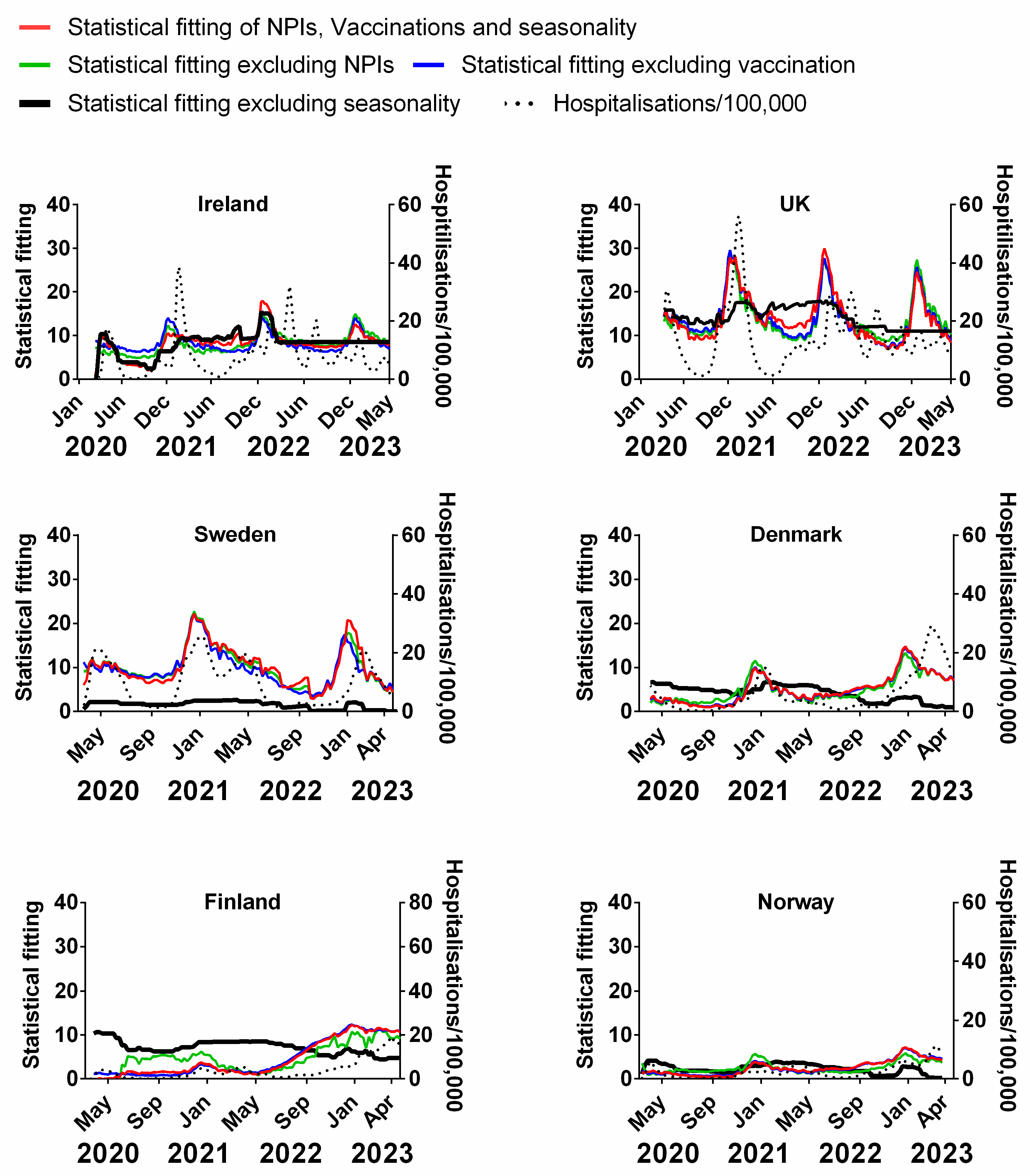
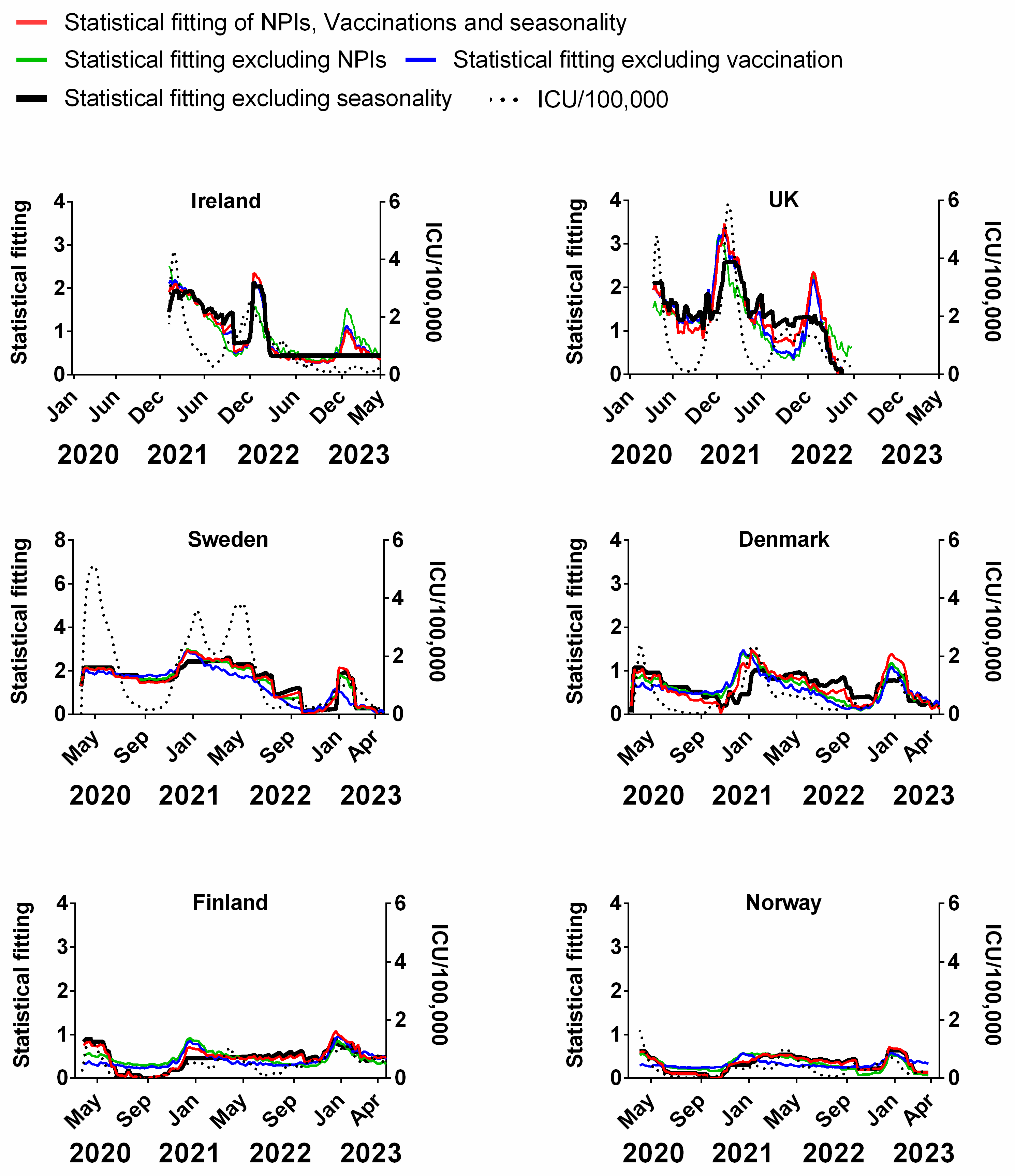
3.4. Influence of Multiple Factors on Pandemic Progression in Northern Europe
4. Study Limitations and Future Research Directions
5. Conclusions and Recommendations
- The stringency of NPIs, e.g., travel restrictions, “stay-at-home” measures, mask mandates and social distancing;
- The percentage of the population fully vaccinated with COVID-19 vaccines (defined in terms of the original recommended numbers of doses for each vaccine);
- The expected seasonality of human beta-coronaviruses (since SARS-CoV-2 is a human beta-coronavirus)—using as a proxy the decadal average of human beta-coronavirus incidences in Sweden based on Swedish clinical data (2010–2020) recorded before the COVID-19 pandemic began.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Glossary
- Confirmed Case: most Northern European countries (Ireland, Norway, Finland and Sweden) used a positive RT-PCR test as confirmation of a case of COVID-19 regardless of whether symptoms were apparent or not, for most of the pandemic—except for the first few months while testing capacity was still being built up. The UK used a combination of RT-PCR and antigen (lateral flow device) tests to confirm positive cases. According to Our World in Data, the case definition for Denmark remained unclear but was defined by the Danish State Serum Institute (SSI) as a person testing positive for COVID-19 antigen who was registered by the sampling date [89,122]. The reported case figures on a given date do not necessarily show the number of new cases on that day—this is due to delays in reporting, additionally, the actual number of cases is likely to be much higher than the number of confirmed cases—due to limited testing [89].
- Death: the definition of COVID-19 death varied between Northern European countries, e.g., in the UK, deaths were published for people who died up to 28 days after having a positive COVID test or if COVID-19 was recorded on their death certificate [90]. In Ireland “COVID-19 deaths include deaths in all possible, probable and confirmed COVID-19 cases (as per the COVID-19 case definition)—unless there is a clear alternative cause of death that cannot be related to COVID-19 infection (e.g., trauma). There should be no period of complete recovery from COVID-19 between the illness and death” [123]. In Denmark, Sweden and Norway, a death with COVID-19 was defined as a death occurring ≤30 days after a positive SARS-CoV-2 test, regardless of reported cause of death [122,124]. Nonetheless, broadly speaking, these definitions refer to “deaths with COVID-19” [89,90]. Establishing what subset of these deaths were “deaths from COVID-19” or even deaths where COVID-19 was a major factor is still a matter of debate [75,91].
- Positivity rate: the proportion of reported RT-PCR tests returning a positive result [89].
- Stringency index: the stringency index is a composite measure of nine metrics: school closures; workplace closures; cancellation of public events; restrictions on public gatherings; closures of public transport; stay-at-home requirements; public information campaigns; restrictions on internal movements; and international travel controls. The index is on a scale from 0 to 100 (100 = strictest). For further details on its construction, see Hale et al., 2021 [4].
- Fully vaccinated individuals: defined as the fraction of population who received all doses prescribed by the initial vaccination protocol. This equates to one dose for the Johnson & Johnson DNA vaccine [8]; two doses for the Oxford/AstraZeneca DNA vaccine [7] and two doses for the Pfizer/BioNTech [5] or Moderna mRNA [6] vaccines. This definition does not consider “boosters”. Typically, people are not considered vaccinated until 14 days after the final dose.
- Time-lagged death: a time-lagged measurement of death due to COVID-19 (per 100,000 of the population) was used to estimate the probable time period between infection and death. This is an especially useful metric because it is because it is a proxy for a subset of infections. Although there are a wide variety of estimates of the average time from infection to death (in cases that end in death), we chose a period of 3 weeks, which is commonly used in other analyses [2,37,86].
- Hospitalised patients: median number of patients in hospital due to COVID-19 on a given week per 100,000 of the population [89]. In Denmark, hospitalisation with COVID-19 was defined as a patient hospitalised for at least 12 h or any length of time in intensive care during the 14 days following sampling date of a positive SARS-CoV-2 test or as a patient testing positive during hospitalisation [122].
- Intensive care unit (ICU) occupancy: median number of patients in ICU due to COVID-19 in a given week [89].
References
- Lenharo, M. WHO Declares End to COVID-19’s Emergency Phase. Nature 2023. [CrossRef] [PubMed]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the Effects of Non-Pharmaceutical Interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Brauner, J.M.; Mindermann, S.; Sharma, M.; Johnston, D.; Salvatier, J.; Gavenčiak, T.; Stephenson, A.B.; Leech, G.; Altman, G.; Mikulik, V.; et al. Inferring the Effectiveness of Government Interventions against COVID-19. Science 2021, 371, eabd9338. [Google Scholar] [CrossRef] [PubMed]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A Global Panel Database of Pandemic Policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and Efficacy of the ChAdOx1 nCoV-19 Vaccine (AZD1222) against SARS-CoV-2: An Interim Analysis of Four Randomised Controlled Trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1–2a Trial of Ad26.COV2.S Covid-19 Vaccine. N. Engl. J. Med. 2021, 384, 1824–1835. [Google Scholar] [CrossRef]
- Korang, S.K.; von Rohden, E.; Veroniki, A.A.; Ong, G.; Ngalamika, O.; Siddiqui, F.; Juul, S.; Nielsen, E.E.; Feinberg, J.B.; Petersen, J.J.; et al. Vaccines to Prevent COVID-19: A Living Systematic Review with Trial Sequential Analysis and Network Meta-Analysis of Randomized Clinical Trials. PLoS ONE 2022, 17, e0260733. [Google Scholar] [CrossRef]
- Stokel-Walker, C. What Do We Know about COVID Vaccines and Preventing Transmission? BMJ 2022, 376, o298. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global Impact of the First Year of COVID-19 Vaccination: A Mathematical Modelling Study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Alrasheedi, A.A. The Prevalence of COVID-19 in Europe by the End of November 2022: A Cross-Sectional Study. Cureus 2023, 15, e33546. [Google Scholar] [CrossRef] [PubMed]
- Cáceres, C.F. Unresolved COVID Controversies: ‘Normal Science’ and Potential Non-Scientific Influences. Glob. Public Health 2022, 17, 622–640. [Google Scholar] [CrossRef] [PubMed]
- Ashmore, P.; Sherwood, E. An Overview of COVID-19 Global Epidemiology and Discussion of Potential Drivers of Variable Global Pandemic Impacts. J. Antimicrob. Chemother. 2023, 78, ii2–ii11. [Google Scholar] [CrossRef] [PubMed]
- Onyeaka, H.; Anumudu, C.K.; Al-Sharify, Z.T.; Egele-Godswill, E.; Mbaegbu, P. COVID-19 Pandemic: A Review of the Global Lockdown and Its Far-Reaching Effects. Sci. Prog. 2021, 104, 00368504211019854. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, M.Z.; Nasir, N.; Mahmood, S.F.; Khan, S.; Kanji, A.; Nasir, A.; Syed, M.A.; Aamir, U.B.; Hasan, Z. Exploring the Relationship between SARS-CoV-2 Variants, Illness Severity at Presentation, in-Hospital Mortality and COVID-19 Vaccination in a Low Middle-Income Country: A Retrospective Cross-Sectional Study. Health Sci. Rep. 2023, 6, e1703. [Google Scholar] [CrossRef]
- Ferguson, N.; Laydon, D.; Nedjati Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunuba Perez, Z.; Cuomo-Dannenburg, G.; et al. Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand; Imperial College: London, UK, 2020. [Google Scholar]
- Sebastiani, G.; Massa, M.; Riboli, E. COVID-19 Epidemic in Italy: Evolution, Projections and Impact of Government Measures. Eur. J. Epidemiol. 2020, 35, 341–345. [Google Scholar] [CrossRef]
- Valencia, M.; Becerra, J.E.; Reyes, J.C.; Castro, K.G. Assessment of Early Mitigation Measures against COVID-19 in Puerto Rico: March 15-May 15, 2020. PLoS ONE 2020, 15, e0240013. [Google Scholar] [CrossRef]
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Druckenmiller, H.; Huang, L.Y.; Hultgren, A.; Krasovich, E.; et al. The Effect of Large-Scale Anti-Contagion Policies on the COVID-19 Pandemic. Nature 2020, 584, 262–267. [Google Scholar] [CrossRef]
- Banholzer, N.; van Weenen, E.; Lison, A.; Cenedese, A.; Seeliger, A.; Kratzwald, B.; Tschernutter, D.; Salles, J.P.; Bottrighi, P.; Lehtinen, S.; et al. Estimating the Effects of Non-Pharmaceutical Interventions on the Number of New Infections with COVID-19 during the First Epidemic Wave. PLoS ONE 2021, 16, e0252827. [Google Scholar] [CrossRef]
- Banholzer, N.; Lison, A.; Özcelik, D.; Stadler, T.; Feuerriegel, S.; Vach, W. The Methodologies to Assess the Effectiveness of Non-Pharmaceutical Interventions during COVID-19: A Systematic Review. Eur. J. Epidemiol. 2022, 37, 1003–1024. [Google Scholar] [CrossRef] [PubMed]
- Mallapaty, S. Vaccines Are Curbing COVID: Data from Israel Show Drop in Infections. Nature 2021, 590, 197. [Google Scholar] [CrossRef] [PubMed]
- Roghani, A. The Influence of COVID-19 Vaccination on Daily Cases, Hospitalization, and Death Rate in Tennessee, United States: Case Study. JMIRx Med. 2021, 2, e29324. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Rocklöv, J. The Effective Reproductive Number of the Omicron Variant of SARS-CoV-2 Is Several Times Relative to Delta. J. Travel Med. 2022, 29, taac037. [Google Scholar] [CrossRef] [PubMed]
- Sigal, A. Milder Disease with Omicron: Is It the Virus or the Pre-Existing Immunity? Nat. Rev. Immunol. 2022, 22, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G. The Epidemiological Relevance of the COVID-19-Vaccinated Population Is Increasing. Lancet Reg. Health Eur. 2021, 11, 100272. [Google Scholar] [CrossRef] [PubMed]
- Marking, U.; Havervall, S.; Norin, N.G.; Christ, W.; Gordon, M.; Ng, H.; Blom, K.; Phillipson, M.; Mangsbo, S.; Sörensen, A.S.; et al. High Rate of BA.1, BA.1.1 and BA.2 Infection in Triple Vaccinated. medRxiv 2022. [Google Scholar] [CrossRef]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 255–263. [Google Scholar] [CrossRef]
- Herby, J.; Jonung, L.; Hanke, S. A Literature Review and Meta-Analysis of the Effects of Lockdowns on COVID-19 Mortality; Studies in Applied Economics; The Johns Hopkins Institute for Applied Economics, Global Health, and the Study of Business Enterprise: Baltimore, MD, USA, 2022. [Google Scholar]
- Fukumoto, K.; McClean, C.T.; Nakagawa, K. No Causal Effect of School Closures in Japan on the Spread of COVID-19 in Spring 2020. Nat. Med. 2021, 27, 2111–2119. [Google Scholar] [CrossRef]
- Bundgaard, H.; Bundgaard, J.S.; Raaschou-Pedersen, D.E.T.; von Buchwald, C.; Todsen, T.; Norsk, J.B.; Pries-Heje, M.M.; Vissing, C.R.; Nielsen, P.B.; Winsløw, U.C.; et al. Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers. Ann. Intern. Med. 2021, 174, 335–343. [Google Scholar] [CrossRef]
- Mader, S.; Rüttenauer, T. The Effects of Non-Pharmaceutical Interventions on COVID-19 Mortality: A Generalized Synthetic Control Approach Across 169 Countries. Front. Public Health 2022, 10, 820642. [Google Scholar] [CrossRef] [PubMed]
- Meintrup, D.; Nowak-Machen, M.; Borgmann, S. A Comparison of Germany and the United Kingdom Indicates That More SARS-CoV-2 Circulation and Less Restrictions in the Warm Season Might Reduce Overall COVID-19 Burden. Life 2022, 12, 953. [Google Scholar] [CrossRef] [PubMed]
- Vickers, D.M.; Baral, S.; Mishra, S.; Kwong, J.C.; Sundaram, M.; Katz, A.; Calzavara, A.; Maheu-Giroux, M.; Buckeridge, D.L.; Williamson, T. Stringency of Containment and Closures on the Growth of SARS-CoV-2 in Canada Prior to Accelerated Vaccine Roll-Out. Int. J. Infect. Dis. 2022, 118, 73–82. [Google Scholar] [CrossRef]
- Kuhbandner, C.; Homburg, S. Commentary: Estimating the Effects of Non-Pharmaceutical Interventions on COVID-19 in Europe. Front. Med. 2020, 7, 580361. [Google Scholar] [CrossRef]
- Wood, S.N. Inferring UK COVID-19 Fatal Infection Trajectories from Daily Mortality Data: Were Infections Already in Decline before the UK Lockdowns? Biometrics 2022, 78, 1127–1140. [Google Scholar] [CrossRef] [PubMed]
- Bjørnskov, C. Did Lockdown Work? An Economist’s Cross-Country Comparison; Social Science Research Network: Rochester, NY, USA, 2020. [Google Scholar]
- Boudou, M.; ÓhAiseadha, C.; Garvey, P.; O’Dwyer, J.; Hynds, P. Breakpoint Modelling of Temporal Associations between Non-Pharmaceutical Interventions and Symptomatic COVID-19 Incidence in the Republic of Ireland. PLoS ONE 2021, 16, e0255254. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Mindermann, S.; Rogers-Smith, C.; Leech, G.; Snodin, B.; Ahuja, J.; Sandbrink, J.B.; Monrad, J.T.; Altman, G.; Dhaliwal, G.; et al. Understanding the Effectiveness of Government Interventions against the Resurgence of COVID-19 in Europe. Nat. Commun. 2021, 12, 5820. [Google Scholar] [CrossRef]
- Marabotti, C. Efficacy and Effectiveness of Covid-19 Vaccine—Absolute vs. Relative Risk Reduction. Expert Rev. Vaccines 2022, 21, 873–875. [Google Scholar] [CrossRef]
- Brown, R.B. Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials. Medicina 2021, 57, 199. [Google Scholar] [CrossRef]
- Olliaro, P.; Torreele, E.; Vaillant, M. COVID-19 Vaccine Efficacy and Effectiveness—The Elephant (Not) in the Room. Lancet Microbe 2021, 2, e279–e280. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Kumar, A. Increases in COVID-19 Are Unrelated to Levels of Vaccination across 68 Countries and 2947 Counties in the United States. Eur. J. Epidemiol. 2021, 36, 1237–1240. [Google Scholar] [CrossRef] [PubMed]
- Neher, R.A.; Dyrdak, R.; Druelle, V.; Hodcroft, E.B.; Albert, J. Potential Impact of Seasonal Forcing on a SARS-CoV-2 Pandemic. Swiss Med. Wkly. 2020, 150, w20224. [Google Scholar] [CrossRef] [PubMed]
- Kissler, S.M.; Tedijanto, C.; Goldstein, E.; Grad, Y.H.; Lipsitch, M. Projecting the Transmission Dynamics of SARS-CoV-2 through the Postpandemic Period. Science 2020, 368, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, M.; Hugentobler, W.J.; Iwasaki, A. Seasonality of Respiratory Viral Infections. Annu. Rev. Virol. 2020, 7, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Dyrdak, R.; Hodcroft, E.B.; Wahlund, M.; Neher, R.A.; Albert, J. Interactions between Seasonal Human Coronaviruses and Implications for the SARS-CoV-2 Pandemic: A Retrospective Study in Stockholm, Sweden, 2009–2020. J. Clin. Virol. 2021, 136, 104754. [Google Scholar] [CrossRef] [PubMed]
- Nichols, G.L.; Gillingham, E.L.; Macintyre, H.L.; Vardoulakis, S.; Hajat, S.; Sarran, C.E.; Amankwaah, D.; Phalkey, R. Coronavirus Seasonality, Respiratory Infections and Weather. BMC Infect. Dis. 2021, 21, 1101. [Google Scholar] [CrossRef]
- Coccia, M. COVID-19 Pandemic over 2020 (with Lockdowns) and 2021 (with Vaccinations): Similar Effects for Seasonality and Environmental Factors. Environ. Res. 2022, 208, 112711. [Google Scholar] [CrossRef]
- Stewart, P.D.S.; Bach, J.L. Temperature Dependent Viral Tropism: Understanding Viral Seasonality and Pathogenicity as Applied to the Avoidance and Treatment of Endemic Viral Respiratory Illnesses. Rev. Med. Virol. 2022, 32, e2241. [Google Scholar] [CrossRef]
- Fontal, A.; Bouma, M.J.; San-José, A.; López, L.; Pascual, M.; Rodó, X. Climatic Signatures in the Different COVID-19 Pandemic Waves across Both Hemispheres. Nat. Comput. Sci. 2021, 1, 655–665. [Google Scholar] [CrossRef]
- Rucinski, S.L.; Binnicker, M.J.; Thomas, A.S.; Patel, R. Seasonality of Coronavirus 229E, HKU1, NL63, and OC43 From 2014 to 2020. Mayo Clin. Proc. 2020, 95, 1701–1703. [Google Scholar] [CrossRef]
- Jüni, P.; Rothenbühler, M.; Bobos, P.; Thorpe, K.E.; da Costa, B.R.; Fisman, D.N.; Slutsky, A.S.; Gesink, D. Impact of Climate and Public Health Interventions on the COVID-19 Pandemic: A Prospective Cohort Study. Can. Med. Assoc. J. 2020, 192, E566–E573. [Google Scholar] [CrossRef] [PubMed]
- Kanzawa, M.; Spindler, H.; Anglemyer, A.; Rutherford, G.W. Will Coronavirus Disease 2019 Become Seasonal? J. Infect. Dis. 2020, 222, 719–721. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Majumder, M.S.; Liu, D.; Poirier, C.; Mandl, K.D.; Lipsitch, M.; Santillana, M. The Role of Absolute Humidity on Transmission Rates of the COVID-19 Outbreak. medRxiv 2020. [Google Scholar] [CrossRef]
- Engelbrecht, F.A.; Scholes, R.J. Test for COVID-19 Seasonality and the Risk of Second Waves. One Health 2021, 12, 100202. [Google Scholar] [CrossRef] [PubMed]
- Smit, A.J.; Fitchett, J.M.; Engelbrecht, F.A.; Scholes, R.J.; Dzhivhuho, G.; Sweijd, N.A. Winter Is Coming: A Southern Hemisphere Perspective of the Environmental Drivers of SARS-CoV-2 and the Potential Seasonality of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5634. [Google Scholar] [CrossRef] [PubMed]
- Kifer, D.; Bugada, D.; Villar-Garcia, J.; Gudelj, I.; Menni, C.; Sudre, C.; Vučković, F.; Ugrina, I.; Lorini, L.F.; Posso, M.; et al. Effects of Environmental Factors on Severity and Mortality of COVID-19. Front. Med. 2021, 7, 607786. [Google Scholar] [CrossRef]
- Hoogeveen, M.J.; Hoogeveen, E.K. Comparable Seasonal Pattern for COVID-19 and Flu-like Illnesses. One Health 2021, 13, 100277. [Google Scholar] [CrossRef]
- Wiemken, T.L.; Khan, F.; Puzniak, L.; Yang, W.; Simmering, J.; Polgreen, P.; Nguyen, J.L.; Jodar, L.; McLaughlin, J.M. Seasonal Trends in COVID-19 Cases, Hospitalizations, and Mortality in the United States and Europe. Sci. Rep. 2023, 13, 3886. [Google Scholar] [CrossRef]
- Shamsa, E.H.; Shamsa, A.; Zhang, K. Seasonality of COVID-19 Incidence in the United States. Front. Public Health 2023, 11, 1298593. [Google Scholar] [CrossRef]
- Quinn, G.A.; Connolly, R.; ÓhAiseadha, C.; Hynds, P. A Tale of Two Scientific Paradigms: Conflicting Scientific Opinions on What “Following the Science” Means for SARS-CoV-2 and the COVID-19 Pandemic. OSF Prepr. 2021. Available online: https://osf.io/s9z2p/ (accessed on 20 October 2023).
- Moroh, J.E.; Innocent, D.C.; Chukwuocha, U.M.; Vasavada, A.; Kumar, R.; Siddiq, M.A.; Rais, M.A.; Rabaan, A.A.; Alshehri, W.M.; Alharbi, A.M.; et al. Seasonal Variation and Geographical Distribution of COVID-19 across Nigeria (March 2020–July 2021). Vaccines 2023, 11, 298. [Google Scholar] [CrossRef] [PubMed]
- Adebowale, A.S.; Afolabi, R.F.; Bello, S.; Salawu, M.M.; Bamgboye, E.A.; Adeoye, I.; Dairo, M.D.; Kivumbi, B.; Wanyana, I.; Seck, I.; et al. Spread and Seasonality of COVID-19 Pandemic Confirmed Cases in Sub-Saharan Africa: Experience from Democratic Republic of Congo, Nigeria, Senegal, and Uganda. BMC Infect. Dis. 2023, 23, 187. [Google Scholar] [CrossRef] [PubMed]
- ÓhAiseadha, C.; Quinn, G.A.; Connolly, R.; Wilson, A.; Connolly, M.; Soon, W.; Hynds, P. Unintended Consequences of COVID-19 Non-Pharmaceutical Interventions (NPIs) for Population Health and Health Inequalities. Int. J. Environ. Res. Public Health 2023, 20, 5223. [Google Scholar] [CrossRef] [PubMed]
- UK Health Security Agency. Effectiveness of Non-Pharmaceutical Interventions to Reduce Transmission of COVID-19 in the UK A Rapid Mapping Review 2023; UK Health Security Agency: London, UK, 2023. [Google Scholar]
- Townsend, J.P.; Hassler, H.B.; Lamb, A.D.; Sah, P.; Nishio, A.A.; Nguyen, C.; Tew, A.D.; Galvani, A.P.; Dornburg, A. Seasonality of Endemic COVID-19. mBio 2023, 14, e01426-23. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M. Our World in Data: Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 8 October 2021).
- Brummitt, R.K. World Geographical Scheme for Recording Plant Distributions, 2nd ed.; Biodiversity Information Standards (TDWG): Sofia, Bulgaria, 2001. [Google Scholar]
- Burgess, S.; Ponsford, M.J.; Gill, D. Are We Underestimating Seroprevalence of SARS-CoV-2? BMJ 2020, 370, m3364. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. The End of the COVID-19 Pandemic. Eur. J. Clin. Investig. 2022, 52, e13782. [Google Scholar] [CrossRef]
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.K.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.L.; Ferris, M.; et al. Screening of Healthcare Workers for SARS-CoV-2 Highlights the Role of Asymptomatic Carriage in COVID-19 Transmission. eLife 2020, 9, e58728. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. Reconciling Estimates of Global Spread and Infection Fatality Rates of COVID-19: An Overview of Systematic Evaluations. Eur. J. Clin. Investig. 2021, 51, e13554. [Google Scholar] [CrossRef]
- Tsang, T.K.; Wu, P.; Lin, Y.; Lau, E.H.Y.; Leung, G.M.; Cowling, B.J. Effect of Changing Case Definitions for COVID-19 on the Epidemic Curve and Transmission Parameters in Mainland China: A Modelling Study. Lancet Public Health 2020, 5, e289–e296. [Google Scholar] [CrossRef]
- Silverman, J.D.; Hupert, N.; Washburne, A.D. Using Influenza Surveillance Networks to Estimate State-Specific Prevalence of SARS-CoV-2 in the United States. Sci. Transl. Med. 2020, 12, eabc1126. [Google Scholar] [CrossRef] [PubMed]
- Reese, H.; Iuliano, A.D.; Patel, N.N.; Garg, S.; Kim, L.; Silk, B.J.; Hall, A.J.; Fry, A.; Reed, C. Estimated Incidence of Coronavirus Disease 2019 (COVID-19) Illness and Hospitalization-United States, February-September 2020. Clin. Infect. Dis. 2021, 72, e1010–e1017. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal Dynamics in Viral Shedding and Transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed]
- Mandavilli, A. Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be. The New York Times, 29 August 2020. [Google Scholar]
- Jaafar, R.; Aherfi, S.; Wurtz, N.; Grimaldier, C.; Van Hoang, T.; Colson, P.; Raoult, D.; La Scola, B. Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates. Clin. Infect. Dis. 2020, 72, e921. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, T.; Spencer, E.A.; Brassey, J.; Heneghan, C. Viral Cultures for COVID-19 Infectious Potential Assessment—A Systematic Review. Clin. Infect. Dis. 2020, 73, e3884–e3899. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, J.B. Perspective | No, More Testing Doesn’t Explain the Rise of COVID-19 Cases in the U.S. Washington Post, 22 June 2020. [Google Scholar]
- Begley, S. Trump Said More COVID-19 Testing “creates More Cases.” We Did the Math. STAT, 20 July 2020. [Google Scholar]
- Feuer, W. Trump Blames Rise in Coronavirus Cases on Increased Testing, despite Evidence of More Spread. Available online: https://www.cnbc.com/2020/06/23/trump-blames-rise-in-coronavirus-cases-on-testing-despite-signs-of-spread.html (accessed on 4 June 2022).
- Ward, T.; Johnsen, A. Understanding an Evolving Pandemic: An Analysis of the Clinical Time Delay Distributions of COVID-19 in the United Kingdom. PLoS ONE 2021, 16, e0257978. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A.; Axfors, C.; Contopoulos-Ioannidis, D.G. Second versus First Wave of COVID-19 Deaths: Shifts in Age Distribution and in Nursing Home Fatalities. Environ. Res. 2021, 195, 110856. [Google Scholar] [CrossRef]
- Polechová, J.; Johnson, K.D.; Payne, P.; Crozier, A.; Beiglböck, M.; Plevka, P.; Schernhammer, E. SARS-CoV-2 Rapid Antigen Tests Provide Benefits for Epidemic Control—Observations from Austrian Schools. J. Clin. Epidemiol. 2022, 145, 14–19. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). Our World in Data. 2020. Available online: https://ourworldindata.org/coronavirus#citation (accessed on 30 November 2023).
- Department of Health and Social Care. New UK-Wide Methodology Agreed to Record COVID-19 Deaths; Department of Health and Social Care: London, UK, 2020. [Google Scholar]
- Baral, S.; Chandler, R.; Prieto, R.G.; Gupta, S.; Mishra, S.; Kulldorff, M. Leveraging Epidemiological Principles to Evaluate Sweden’s COVID-19 Response. Ann. Epidemiol. 2021, 54, 21–26. [Google Scholar] [CrossRef]
- Vu, C.; Kawaguchi, E.S.; Torres, C.H.; Lee, A.H.; Wald-Dickler, N.; Holtom, P.D.; Stafylis, C.; Klausner, J.D.; Khan, S. A More Accurate Measurement of the Burden of Coronavirus Disease 2019 Hospitalizations. Open Forum Infect. Dis. 2022, 9, ofac332. [Google Scholar] [CrossRef]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.A. Coronavirus Disease 2019: The Harms of Exaggerated Information and Non-Evidence-Based Measures. Eur. J. Clin. Investig. 2020, 50, e13222. [Google Scholar] [CrossRef] [PubMed]
- Banholzer, N.; Feuerriegel, S.; Vach, W. Estimating and Explaining Cross-Country Variation in the Effectiveness of Non-Pharmaceutical Interventions during COVID-19. Sci. Rep. 2022, 12, 7526. [Google Scholar] [CrossRef] [PubMed]
- Bendavid, E.; Oh, C.; Bhattacharya, J.; Ioannidis, J.P.A. Assessing Mandatory Stay-at-Home and Business Closure Effects on the Spread of COVID-19. Eur. J. Clin. Investig. 2021, 51, e13484. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.-Y.; Blakemore, C. The Impact of Multiple Non-Pharmaceutical Interventions on Controlling COVID-19 Outbreak without Lockdown in Hong Kong: A Modelling Study. Lancet Reg. Health West Pac. 2022, 20, 100343. [Google Scholar] [CrossRef] [PubMed]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; et al. Effectiveness of Public Health Measures in Reducing the Incidence of COVID-19, SARS-CoV-2 Transmission, and COVID-19 Mortality: Systematic Review and Meta-Analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; van der Westhuizen, H.-M.; von Delft, A.; Price, A.; Fridman, L.; Tang, L.-H.; et al. An Evidence Review of Face Masks against COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2014564118. [Google Scholar] [CrossRef] [PubMed]
- Lupu, D.; Tiganasu, R. The Implications of Globalization on COVID-19 Vaccination in Europe. Sci. Rep. 2022, 12, 17474. [Google Scholar] [CrossRef]
- Suárez-Álvarez, A.; López-Menéndez, A.J. Is COVID-19 Vaccine Inequality Undermining the Recovery from the COVID-19 Pandemic? J. Glob. Health 2022, 12, 05020. [Google Scholar] [CrossRef]
- Nyachoti, D.O.; Fwelo, P.; Springer, A.E.; Kelder, S.H. Association between Gross National Income per Capita and COVID-19 Vaccination Coverage: A Global Ecological Study. BMC Public Health 2023, 23, 2415. [Google Scholar] [CrossRef]
- Acharya, C.B.; Schrom, J.; Mitchell, A.M.; Coil, D.A.; Marquez, C.; Rojas, S.; Wang, C.Y.; Liu, J.; Pilarowski, G.; Solis, L.; et al. Viral Load Among Vaccinated and Unvaccinated, Asymptomatic and Symptomatic Persons Infected With the SARS-CoV-2 Delta Variant. Open Forum Infect. Dis. 2022, 9, ofac135. [Google Scholar] [CrossRef] [PubMed]
- UK Health Security Agency. COVID-19 Vaccine Surveillance Report. Week 9; UK Health Security Agency: London, UK, 2022. [Google Scholar]
- Mulot, M.; Segalas, C.; Leyrat, C.; Besançon, L. Re: Subramanian and Kumar. Vaccination Rates and COVID-19 Cases. Eur. J. Epidemiol. 2021, 36, 1243–1244. [Google Scholar] [CrossRef] [PubMed]
- Björk, J.; Modig, K.; Kahn, F.; Ahlbom, A. Revival of Ecological Studies during the COVID-19 Pandemic. Eur. J. Epidemiol. 2021, 36, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Ballin, M.; Nordström, A. Risk of Infection, Hospitalisation, and Death up to 9 Months after a Second Dose of COVID-19 Vaccine: A Retrospective, Total Population Cohort Study in Sweden. Lancet 2022, 399, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Dolgin, E. COVID Vaccine Immunity Is Waning—How Much Does That Matter? Nature 2021, 597, 606–607. [Google Scholar] [CrossRef] [PubMed]
- Price, R.H.M.; Graham, C.; Ramalingam, S. Association between Viral Seasonality and Meteorological Factors. Sci. Rep. 2019, 9, 929. [Google Scholar] [CrossRef]
- Martinez, M.E. The Calendar of Epidemics: Seasonal Cycles of Infectious Diseases. PLoS Pathog. 2018, 14, e1007327. [Google Scholar] [CrossRef]
- Raiteux, J.; Eschlimann, M.; Marangon, A.; Rogée, S.; Dadvisard, M.; Taysse, L.; Larigauderie, G. Inactivation of SARS-CoV-2 by Simulated Sunlight on Contaminated Surfaces. Microbiol. Spectr. 2021, 9, e0033321. [Google Scholar] [CrossRef]
- Dabisch, P.; Schuit, M.; Herzog, A.; Beck, K.; Wood, S.; Krause, M.; Miller, D.; Weaver, W.; Freeburger, D.; Hooper, I.; et al. The Influence of Temperature, Humidity, and Simulated Sunlight on the Infectivity of SARS-CoV-2 in Aerosols. Aerosol Sci. Technol. 2021, 55, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Colston, J.M.; Hinson, P.; Nguyen, N.-L.H.; Chen, Y.T.; Badr, H.S.; Kerr, G.H.; Gardner, L.M.; Martin, D.N.; Quispe, A.M.; Schiaffino, F.; et al. Effects of Hydrometeorological and Other Factors on SARS-CoV-2 Reproduction Number in Three Contiguous Countries of Tropical Andean South America: A Spatiotemporally Disaggregated Time Series Analysis. IJID Reg. 2023, 6, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Gilaberte, J.B.; Martín-Iranzo, N.; Aguilera, J.; Almenara-Blasco, M.; de Gálvez, M.V.; Gilaberte, Y. Correlation between UV Index, Temperature and Humidity with Respect to Incidence and Severity of COVID 19 in Spain. Int. J. Environ. Res. Public Health 2023, 20, 1973. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, M.G.; Christiansen, L.E.; Græsbøll, K. Seasonal Variation in the Transmission Rate of COVID-19 in a Temperate Climate Can Be Implemented in Epidemic Population Models by Using Daily Average Temperature as a Proxy for Seasonal Changes in Transmission Rate. Microb. Risk Anal. 2022, 22, 100235. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Huang, J.; Li, C.; Zhao, Y.; Wang, D.; Huang, Z.; Yang, K. The Role of Seasonality in the Spread of COVID-19 Pandemic. Environ. Res. 2021, 195, 110874. [Google Scholar] [CrossRef] [PubMed]
- Bloom-Feshbach, K.; Alonso, W.J.; Charu, V.; Tamerius, J.; Simonsen, L.; Miller, M.A.; Viboud, C. Latitudinal Variations in Seasonal Activity of Influenza and Respiratory Syncytial Virus (RSV): A Global Comparative Review. PLoS ONE 2013, 8, e54445. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Morgenstern, C.; Kelly, J.; Lowe, R.; Munday, J.; Villabona-Arenas, C.J.; Gibbs, H.; Pearson, C.A.B.; Prem, K.; Leclerc, Q.J.; et al. The Impact of Non-Pharmaceutical Interventions on SARS-CoV-2 Transmission across 130 Countries and Territories. BMC Med. 2021, 19, 40. [Google Scholar] [CrossRef]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The Unintended Consequences of COVID-19 Vaccine Policy: Why Mandates, Passports and Restrictions May Cause More Harm than Good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef]
- Holmager, T.L.; Lynge, E.; Kann, C.E.; St-Martin, G. Geography of COVID-19 in Denmark. Scand. J. Public Health 2021, 49, 88–95. [Google Scholar] [CrossRef]
- White, P.; Crowe, C.; Bowe, A.; Brennan, A.; Bruton, O.; O’Sullivan, M.B.; O’Mahony, M.T.; Sheahan, A.; Barrett, P. An Audit of COVID-19 Death Reporting in Counties Cork and Kerry, Ireland, Winter 2021–2022. Ir. J. Med. Sci. 2023, 192, 1589–1594. [Google Scholar] [CrossRef]
- Juul, F.E.; Jodal, H.C.; Barua, I.; Refsum, E.; Olsvik, Ø.; Helsingen, L.M.; Løberg, M.; Bretthauer, M.; Kalager, M.; Emilsson, L. Mortality in Norway and Sweden during the COVID-19 Pandemic. Scand. J. Public Health 2022, 50, 38–45. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Northern European Countries | NPIs | Vaccination | Seasonality |
|---|---|---|---|
| Ireland | x | x | ✓ |
| UK | x | x | ✓ |
| Sweden | x | x | ✓ |
| Denmark | x | x | ✓ |
| Finland | x | x | ✓ |
| Norway | x | x | ✓ |
| Northern European Countries | NPIs | Vaccination | Seasonality |
|---|---|---|---|
| Ireland | x | x | ✓ |
| UK | x | x | ✓ |
| Sweden | x | x | ✓ |
| Denmark | x | x | ✓ |
| Finland | x | x | ✓ |
| Norway | x | x | ✓ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinn, G.A.; Connolly, M.; Fenton, N.E.; Hatfill, S.J.; Hynds, P.; ÓhAiseadha, C.; Sikora, K.; Soon, W.; Connolly, R. Influence of Seasonality and Public-Health Interventions on the COVID-19 Pandemic in Northern Europe. J. Clin. Med. 2024, 13, 334. https://doi.org/10.3390/jcm13020334
Quinn GA, Connolly M, Fenton NE, Hatfill SJ, Hynds P, ÓhAiseadha C, Sikora K, Soon W, Connolly R. Influence of Seasonality and Public-Health Interventions on the COVID-19 Pandemic in Northern Europe. Journal of Clinical Medicine. 2024; 13(2):334. https://doi.org/10.3390/jcm13020334
Chicago/Turabian StyleQuinn, Gerry A., Michael Connolly, Norman E. Fenton, Steven J. Hatfill, Paul Hynds, Coilín ÓhAiseadha, Karol Sikora, Willie Soon, and Ronan Connolly. 2024. "Influence of Seasonality and Public-Health Interventions on the COVID-19 Pandemic in Northern Europe" Journal of Clinical Medicine 13, no. 2: 334. https://doi.org/10.3390/jcm13020334
APA StyleQuinn, G. A., Connolly, M., Fenton, N. E., Hatfill, S. J., Hynds, P., ÓhAiseadha, C., Sikora, K., Soon, W., & Connolly, R. (2024). Influence of Seasonality and Public-Health Interventions on the COVID-19 Pandemic in Northern Europe. Journal of Clinical Medicine, 13(2), 334. https://doi.org/10.3390/jcm13020334