
Impaired Semen Quality in Patients with Chronic Prostatitis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
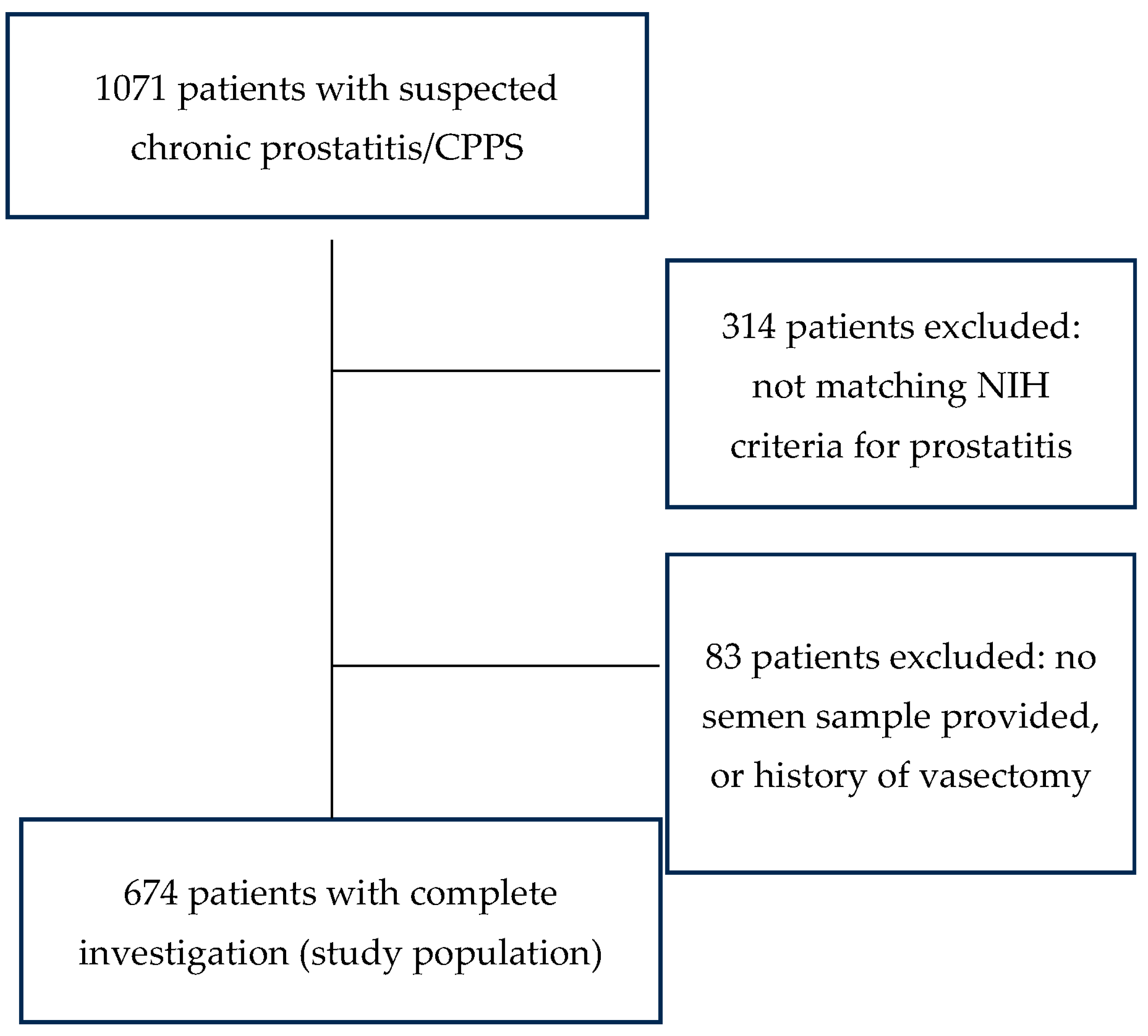
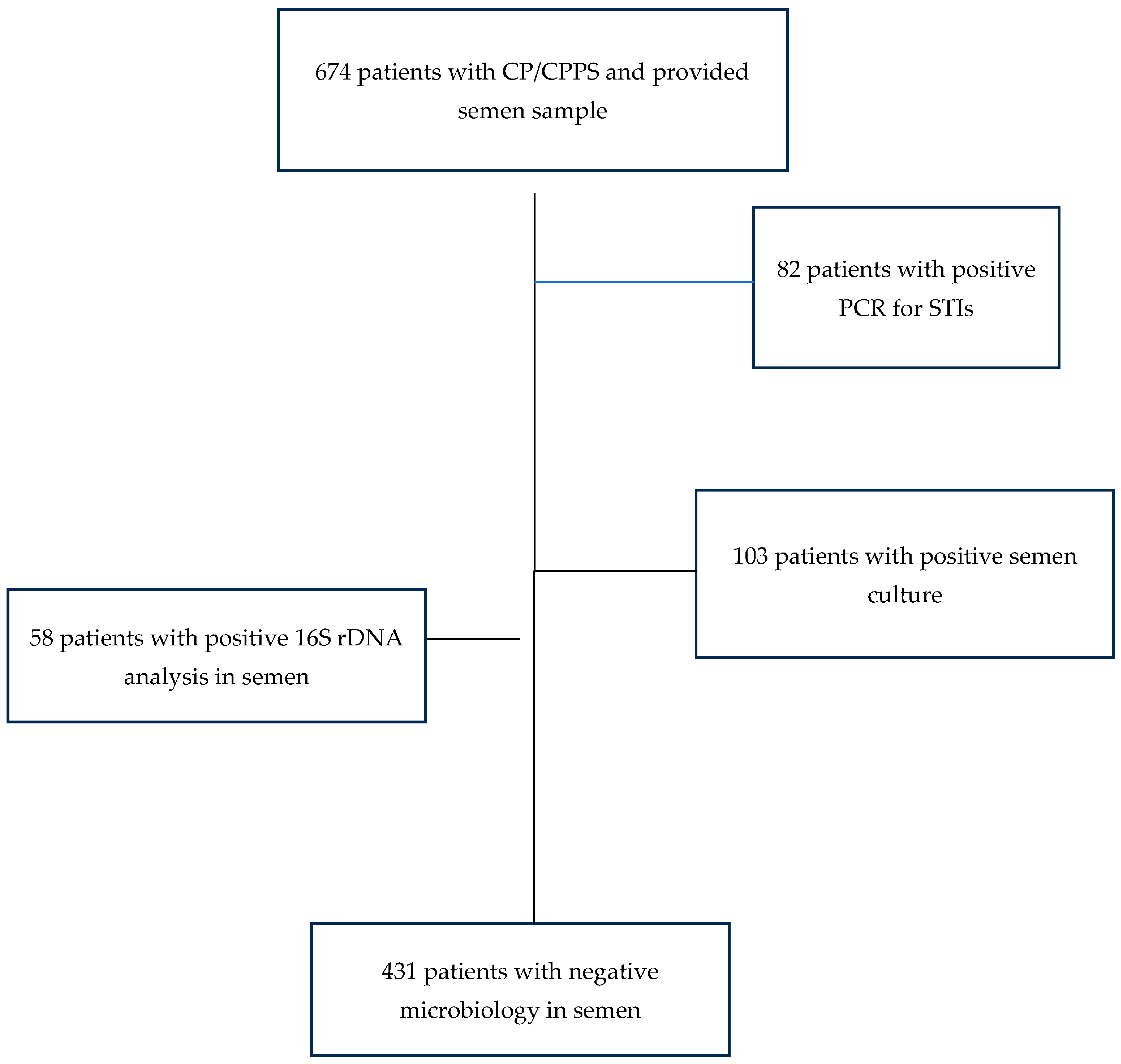
2.1. Study Population
2.2. Clinical Investigations
2.3. Laboratory Methods
2.4. Semen Analysis
2.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Questionnaires
3.3. Andrological Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suskind, A.M.; Berry, S.H.; Ewing, B.A.; Elliott, M.N.; Suttorp, M.J.; Clemens, J.Q. The prevalence and overlap of interstitial cystitis/bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: Results of the RAND Interstitial Cystitis Epidemiology male study. J. Urol. 2013, 189, 141–145. [Google Scholar] [CrossRef]
- Krieger, J.N.; Lee, S.W.; Jeon, J.; Cheah, P.Y.; Liong, M.L.; Riley, D.E. Epidemiology of prostatitis. Int. J. Antimicrob. Agents 2008, 31 (Suppl. S1), S85–S90. [Google Scholar] [CrossRef]
- Sharp, V.J.; Takacs, E.B.; Powell, C.R. Prostatitis: Diagnosis and treatment. Am. Fam. Physician 2010, 82, 397–406. [Google Scholar]
- Nickel, J.C.; Alexander, R.B.; Schaeffer, A.J.; Landis, J.R.; Knauss, J.S.; Propert, K.J.; Chronic Prostatitis Collaborative Research Network Study Group. Leukocytes and bacteria in men with chronic prostatitis/chronic pelvic pain syndrome compared to asymptomatic controls. J. Urol. 2003, 170, 818–822. [Google Scholar] [CrossRef]
- Nickel, J.C.; Ardern, D.; Downey, J. Cytologic evaluation of urine is important in evaluation of chronic prostatitis. Urology 2002, 60, 225–227. [Google Scholar] [CrossRef]
- Rees, J.; Abrahams, M.; Doble, A.; Cooper, A.; Prostatitis Expert Reference Group (PERG). Diagnosis and treatment of chronic bacterial prostatitis and chronic prostatitis/chronic pelvic pain syndrome: A consensus guideline. BJU Int. 2015, 116, 509–525. [Google Scholar] [CrossRef]
- Krieger, J.N.; Nyberg, L.; Nickel, J.C. NIH consensus definition and classification of prostatitis. JAMA 1999, 282, 236–237. [Google Scholar] [CrossRef]
- Nickel, J.C.; Shoskes, D.; Wang, Y.; Alexander, R.B.; Fowler, J.E.; Zeitlin, S.; Chronic Prostatitis Collaborative Research Network Study Group. How does the pre-massage and post-massage 2-glass test compare to the Meares-Stamey 4-glass test in men with chronic prostatitis/chronic pelvic pain syndrome? J. Urol. 2006, 176, 119–124. [Google Scholar] [CrossRef]
- Leib, Z.; Bartoov, B.; Eltes, F.; Servadio, C. Reduced semen quality caused by chronic abacterial prostatitis: An enigma or reality? Fertil. Steril. 1994, 61, 1109–1116. [Google Scholar] [CrossRef]
- Solomon, M.; Henkel, R. Semen culture and the assessment of genitourinary tract infections. Indian J. Urol. 2017, 33, 188–193. [Google Scholar]
- Ausmees, K.; Korrovits, P.; Timberg, G.; Punab, M.; Mändar, R. Semen quality and associated reproductive indicators in middle-aged males: The role of non-malignant prostate conditions and genital tract inflammation. World J. Urol. 2013, 31, 1411–1425. [Google Scholar] [CrossRef] [PubMed]
- Motrich, R.D.; Maccioni, M.; Molina, R.; Tissera, A.; Olmedo, J.; Riera, C.M.; Rivero, V.E. Reduced semen quality in chronic prostatitis patients that have cellular autoimmune response to prostate antigens. Hum. Reprod. 2005, 20, 2567–2572. [Google Scholar] [CrossRef] [PubMed]
- Li, J.L. The effect of chronic prostatitis on the semen quality. Med. Inn. China 2009, 6, 48–49. [Google Scholar]
- Wang, Q.; Cui, Y.H.; Zhang, J.P.; Kong, Y.H. Study on effective living spermatic index of semen in chronic bacterial prostatitis patients. J. Jining Med. Coll. 2000, 23, 53. [Google Scholar]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen, 6th ed.; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Pedersen, M.R.; Osther, P.J.S.; Rafaelsen, S.R. Ultrasound Evaluation of Testicular Volume in Patients with Testicular Microlithiasis. Ultrasound Int. Open 2018, 4, E99–E103. [Google Scholar] [CrossRef] [PubMed]
- Lotti, F.; Frizza, F.; Balercia, G.; Barbonetti, A.; Behre, H.M.; Calogero, A.E.; Cremers, J.F.; Francavilla, F.; Isidori, A.M.; Kliesch, S.; et al. The European Academy of Andrology (EAA) ultrasound study on healthy, fertile men: An overview on male genital tract ultrasound reference ranges. Andrology 2022, 10 (Suppl. S2), 118–132. [Google Scholar] [CrossRef] [PubMed]
- Domann, E.; Hong, G.; Imirzalioglu, C.; Turschner, S.; Kühle, J.; Watzel, C.; Chakraborty, T. Culture-independent identification of pathogenic bacteria and polymicrobial infections in the genitourinary tract of renal transplant recipients. J. Clin. Microbiol. 2003, 41, 5500–5510. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, M.; Dimitrakov, J.; Diemer, T.; Huwe, P.; Weidner, W. Das Prostatitissyndrom. Ejakulatveränderungen und Auswirkungen auf die Fertilität [Prostatitis syndrome. Changes in the ejaculate and effects on fertility]. Urol. A 2001, 40, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.J.; Lotti, F.; Baldi, E.; Schlatt, S.; Festin, M.P.R.; Björndahl, L.; Toskin, I.; Barratt, C.L.R. Distribution of semen examination results 2020—A follow up of data collated for the WHO semen analysis manual 2010. Andrology 2021, 9, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Tyloch, J.F.; Wieczorek, A.P. The standards of an ultrasound examination of the prostate gland: Part 1. J. Ultrason. 2016, 16, 378–390. [Google Scholar] [CrossRef]
- Pilatz, A.; Discher, T.; Lochnit, G.; Wolf, J.; Schuppe, H.C.; Schüttler, C.G.; Hossain, H.; Weidner, W.; Lohmeyer, J.; Diemer, T. Semen quality in HIV patients under stable antiretroviral therapy is impaired compared to WHO 2010 reference values and on sperm proteome level. AIDS 2014, 28, 875–880. [Google Scholar] [CrossRef]
- Park, H.; Lee, G. Roles of Ureaplasma Species in Idiopathic Chronic Prostatitis: A Case-Control Study. World J. Men’s Health 2019, 37, 355–362. [Google Scholar] [CrossRef]
- Mashaly, M.; Masallat, D.T.; Elkholy, A.A.; Abdel-Hamid, I.A.; Mostafa, T. Seminal Corynebacterium strains in infertile men with and without leucocytospermia. Andrologia 2016, 48, 355–359. [Google Scholar] [CrossRef]
- Vilvanathan, S.; Kandasamy, B.; Jayachandran, A.L.; Sathiyanarayanan, S.; Tanjore Singaravelu, V.; Krishnamurthy, V.; Elangovan, V. Bacteriospermia and its impact on basic semen parameters among infertile men. Interdiscip. Perspect. Infect. Dis. 2016, 2016, 2614692. [Google Scholar] [CrossRef] [PubMed]
- Moretti, E.; Capitani, S.; Figura, N.; Pammolli, A.; Federico, M.G.; Giannerini, V. The presence of bacteria species in semen and sperm quality. J. Assist. Reprod. Genet. 2009, 26, 47–56. [Google Scholar] [CrossRef]
- Farahani, L.; Tharakan, T.; Yap, T.; Ramsay, J.W.; Jayasena, C.N.; Minhas, S. The semen microbiome and its impact on sperm function and male fertility: A systematic review and meta-analysis. Andrology 2021, 9, 115–144. [Google Scholar] [CrossRef] [PubMed]
- Fraczek, M.; Hryhorowicz, M.; Gaczarzewicz, D.; Szumala-Kakol, A.; Kolanowski, T.J.; Beutin, L.; Kurpisz, M. Can apoptosis and necrosis coexist in ejaculated human spermatozoa during in vitro semen bacterial infection? J. Assist. Reprod. Genet. 2015, 32, 771–779. [Google Scholar] [CrossRef]
- Ni, K.; Spiess, A.; Schuppe, H.; Steger, K. The impact of sperm protamine deficiency and sperm DNA damage on human male fertility: A systematic review and meta-analysis. Andrology 2016, 4, 789–799. [Google Scholar] [CrossRef]
- Marconi, M.; Pilatz, A.; Wagenlehner, F.; Diemer, T.; Weidner, W. Impact of infection on the secretory capacity of the male accessory glands. Int. Braz. J. Urol. 2009, 35, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Lotti, F.; Corona, G.; Mondaini, N.; Maseroli, E.; Rossi, M.; Filimberti, E.; Noci, I.; Forti, G.; Maggi, M. Seminal, clinical and colour-Doppler ultrasound correlations of prostatitis-like symptoms in males of infertile couples. Andrology 2014, 2, 30–41. [Google Scholar] [CrossRef]
- Nallella, K.P.; Sharma, R.K.; Aziz, N.; Agarwal, A. Significance of sperm characteristics in the evaluation of male infertility. Fertil. Steril. 2006, 85, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Brito, L.F.C.; Althouse, G.C.; Aurich, C.; Chenoweth, P.J.; Eilts, B.E.; Love, C.C.; Luvoni, G.C.; Mitchell, J.R.; Peter, A.T.; Pugh, D.G.; et al. Andrology laboratory review: Evaluation of sperm concentration. Theriogenology 2016, 85, 1507–1527. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.; Zhou, Z.; Liu, S.; Li, Q.; Yao, J.; Li, W.; Yan, J. The effect of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) on semen parameters in human males: A systematic review and meta-analysis. PLoS ONE 2014, 9, e94991. [Google Scholar] [CrossRef] [PubMed]
- Crocetto, F.; Risolo, R.; Colapietro, R.; Bellavita, R.; Barone, B.; Ballini, A.; Arrigoni, R.; Francesco Caputo, V.; Luca, G.; Grieco, P.; et al. Heavy Metal Pollution and Male Fertility: An Overview on Adverse Biological Effects and Socio-Economic Implications. Endocr. Metab. Immune Disord. Drug Targets 2023, 23, 129–146. [Google Scholar]
- Ilacqua, A.; Izzo, G.; Emerenziani, G.P.; Baldari, C.; Aversa, A. Lifestyle and fertility: The influence of stress and quality of life on male fertility. Reprod. Biol. Endocrinol. 2018, 16, 115. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameter | Median (IQR) or n (%) | Number of Patients (n) |
|---|---|---|
| Age (years) | 40 (32–49) | 674 |
| Type of prostatitis | 674 | |
| 50 (7.4%) | |
| 624 (92.6%) | ||
| IPSS (points) | 10 (5–16) | 588 |
| IIEF (points) | 25 (15–29) | 423 |
| CPSI-I (points) | 12 (9–14) | 563 |
| CPSI-II (points) | 3 (2–5) | 563 |
| CPSI-III (points) | 9 (7–11) | 563 |
| Total testosterone (ng/dL) | 430 (321–541) | 551 |
| PSA (ng/mL) | 0.71 (0.48–1.12) | 636 |
| Estradiol (pg/mL) | 32 (27–37) | 430 |
| CRP (mg/L) | 0.5 (0.5–1.5) | 641 |
| Median testicular volume (mL) | 15.0 (12–17) | 383 |
| Prostate volume (mL) | 22.0 (17–28) | 442 |
| Parameter | Patients with Chronic Prostatitis/CPPS (n = 674) | WHO 2021 Reference Values 1 | p 1 | Number of Patients | Out of Reference Value (%) |
|---|---|---|---|---|---|
| Volume | 2.3 (1.2–3.5) | 1.4 2 | <0.001 | 674 | 27.5 |
| pH value | 7.6 (7.4–7.9) | ≥7.2 3 | n.a. | 672 | 4.6 |
| Sperm concentration (106/mL) | 44.0 (16.8–102.45) | 16 2 | <0.001 | 673 | 24.4 |
| Total sperm count (106/ejaculate) | 63 (0–205.8) | 39 2 | <0.001 | 664 | 43.4 |
| Progressive motility (%) | 47 (30–55) | 30 2 | <0.001 | 655 | 27.2 |
| Sperm vitality (%) | 60 (44.25–73) | 58 2 | <0.001 | 196 | 44.4 |
| Normal morphology (%) | 8 (4–13) | 4 2 | 0.563 | 619 | 25.4 |
| α-glucosidase (mU/ejaculate) | 28.15 (13.9–55.6) | ≥20/ejaculate 3 | n.a. | 639 | 37.3 |
| Fructose (µmol/ejaculate) | 16.1 (8.2–32.4) | ≥13/ejaculate 3 | n.a. | 647 | 39.7 |
| Zinc (µmol/ejaculate) | 4.9 (2.7–10.6) | ≥2.4/ejaculate 3 | n.a. | 538 | 21.6 |
| Peroxidase-positive leukocytes (106/mL) | 0 (0–3) | <1 3 | n.a. | 450 | 44.4 |
| Elastase (ng/mL) | 37.0 (12.48–109.75) | <250 4 | n.a. | 624 | 11.3 |
| Interleukin-8 (pg/mL) | 3706.5 (2035.25–6860.75) | <10,000 4 | n.a. | 563 | 14.9 |
| Parameter | Patients with Chronic Prostatitis Type IIIA (n = 50) | Patients with Chronic Prostatitis Type IIIB (n = 624) | p 1 |
|---|---|---|---|
| Age (years) | 44 (31–53) | 40 (32–48) | 0.286 |
| IPSS (points) | 11 (6–16) | 10 (5–16) | 0.619 |
| IIEF (points) | 23 (12–30) | 25 (15–29) | 0.486 |
| CPSI-I (points) | 11 (7–14) | 12 (9–15) | 0.146 |
| CPSI-II (points) | 3 (1–6) | 3 (2–5) | 0.828 |
| CPSI-III (points) | 9 (7–10) | 9 (7–11) | 0.535 |
| Total testosterone (ng/dL) | 441 (345–519) | 430 (319–543) | 0.653 |
| PSA (ng/mL) | 1.13 (0.83–2.16) | 0.69 (0.47–1.08) | 0.478 |
| Estradiol (pg/mL) | 33 (29–41) | 32 (26–379 | 0.069 |
| CRP (mg/L) | 0.7 (0.5–2.05) | 0.5 (0.5–1.40) | 0.261 |
| Median testicular volume (mL) | 15 (13–20) | 15 (12–17) | 0.259 |
| Prostate volume (mL) | 20.2 (18–30) | 22 (17.45–28.18) | 0.652 |
| Correlation Coefficient r | p (Univariate) | Correlation Coefficient ß | p (Multivariate) | |
|---|---|---|---|---|
| Age (years) | 0.023 | 0.556 | 0.061 | 0.409 |
| IPSS total score | 0.039 | 0.342 | −0.175 | 0.163 |
| IIEF total score | −0.034 | 0.147 | −0.058 | 0.435 |
| CPSI total score | 0.053 | 0.213 | 0.309 | 0.015 |
| Testicular volume (mL) | 0.063 | 0.212 | 0.236 | 0.814 |
| Prostate volume (mL) | 0.107 | 0.023 | 0.038 | 0.587 |
| CRP (mg/L) | −0.016 | 0.692 | −0.018 | 0.709 |
| PSA (ng/mL) | 0.022 | 0.579 | −0.062 | 0.206 |
| Estradiol (pg/mL) | −0.044 | 0.367 | −0.058 | 0.271 |
| Total testosterone (ng/dL) | 0.009 | 0.831 | 0.038 | 0.472 |
| Parameter | Patients with Negative Microbiology in Semen (n = 431) | Patients with Positive Microbiology in Semen (n = 103) | Patients with Positive PCR for STI (n = 82) | Patients with Positive 16S rDNA (n = 58) | WHO 2021 Reference Values | p 1 |
|---|---|---|---|---|---|---|
| Volume | 2.5 (1.5–3.7) | 1.7 (0.8–2.9) | 2.5 (1.8–3.4) | 2.3 (1.5–3.8) | 1.4 2 | <0.001 |
| pH value | 7.6 (7.4–7.9) | 7.6 (7.4–8.0) | 7.6 (7.5–7.9) | 7.7 (7.4–8.1) | ≥7.2 2 | 0.997 |
| Sperm concentration (106/mL) | 48.6 (19.6–112.5) | 37 (12.6–93.9) | 33.6 (10.8–84.2) | 43.5 (16.9–68.8) | 16 2 | 0.416 |
| Total sperm count (106/ejaculate) | 77 (5.4–230.5) | 14.1 (0.1–103.4) | 70.6 (7.7–343) | 70.4 (10.7–147.4) | 39 2 | <0.001 |
| Progressive motility (%) | 48 (32–56) | 45 (24–55) | 52 (21–59) | 43 (29–58) | 30 2 | 0.903 |
| Sperm vitality (%) | 61 (45–74) | 60 (39–73) | 68 (30–80) | 67 (54–73) | 58 2 | 0.659 |
| Normal forms (%) | 9 (4–13) | 6 (3–11) | 10 (5–16) | 7 (4–9) | 4 2 | 0.128 |
| α-glucosidase (mU/ejaculate) | 33.1 (16–63.4) | 17.9 (11.4–31.03) | 26.7 (15.2–72.8) | 18 (9.9–27) | ≥20/ejaculate 3 | <0.001 |
| Fructose (µmol/ejaculate) | 17.5 (8.3–35.4) | 13.4 (7.1–23.8) | 24.6 (12.5–44-5) | 9.9 (6.7–16.7) | ≥13/ejaculate 3 | 0.005 |
| Zinc (µmol/ejaculate) | 5.4 (3–11.6) | 4.0 (2.4–7.3) | 7.6 (4.7–17.7) | 4.1 (2.8–5.5) | ≥2.4/ejaculate 3 | 0.015 |
| Peroxidase-positive leukocytes (106/mL) | 0 (0–2) | 1 (0–3) | 0 (0–2) | 2 (1–7) | <1 3 | 0.010 |
| Elastase (ng/mL) | 37 (12–117) | 50 (14.0–211.5) | 27 (10–108) | 43 (15–193) | <250 4 | 0.810 |
| Interleukin-8 (pg/mL) | 3537 (2016–6408) | 4211 (2141.5–8438.5) | 3081 (1720–5361) | 3820 (2205–8266) | <10,000 4 | 0.694 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosellen, J.; Dittmar, F.; Hauptmann, A.; Diemer, T.; Schuppe, H.-C.; Schagdarsurengin, U.; Fritzenwanker, M.; Wagenlehner, F.; Pilatz, A. Impaired Semen Quality in Patients with Chronic Prostatitis. J. Clin. Med. 2024, 13, 2884. https://doi.org/10.3390/jcm13102884
Rosellen J, Dittmar F, Hauptmann A, Diemer T, Schuppe H-C, Schagdarsurengin U, Fritzenwanker M, Wagenlehner F, Pilatz A. Impaired Semen Quality in Patients with Chronic Prostatitis. Journal of Clinical Medicine. 2024; 13(10):2884. https://doi.org/10.3390/jcm13102884
Chicago/Turabian StyleRosellen, Jens, Florian Dittmar, Arne Hauptmann, Thorsten Diemer, Hans-Christian Schuppe, Undraga Schagdarsurengin, Moritz Fritzenwanker, Florian Wagenlehner, and Adrian Pilatz. 2024. "Impaired Semen Quality in Patients with Chronic Prostatitis" Journal of Clinical Medicine 13, no. 10: 2884. https://doi.org/10.3390/jcm13102884
APA StyleRosellen, J., Dittmar, F., Hauptmann, A., Diemer, T., Schuppe, H.-C., Schagdarsurengin, U., Fritzenwanker, M., Wagenlehner, F., & Pilatz, A. (2024). Impaired Semen Quality in Patients with Chronic Prostatitis. Journal of Clinical Medicine, 13(10), 2884. https://doi.org/10.3390/jcm13102884