

New Infiltration Technique in the Treatment of the Plantar Fascia Syndrome Based on Platelet-Rich Plasma


Abstract
1. Introduction
2. Materials and Methods
2.1. Type of Study
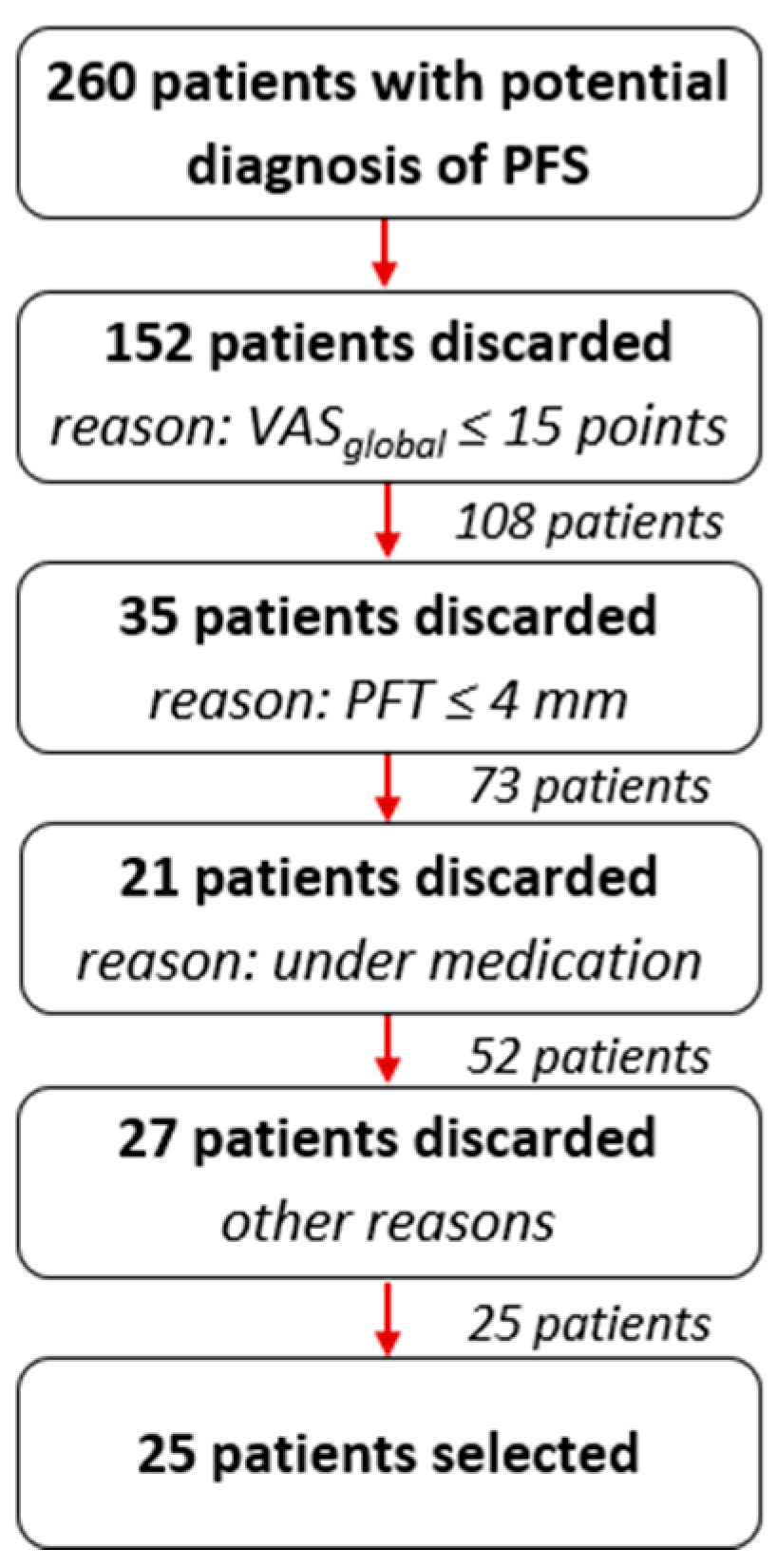
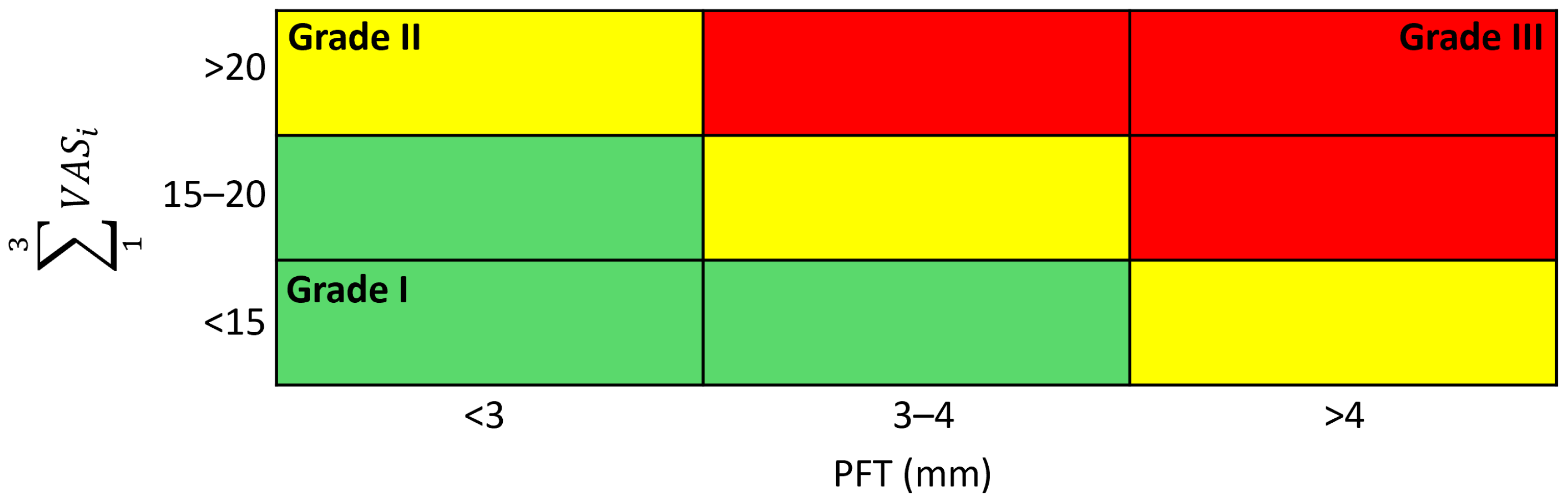
2.2. Plantar Fascia Syndrome: Diagnosis and Classification
2.3. Procedure—Infiltration Technique
2.3.1. Preparation of the Patient
2.3.2. PRP Administration
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Evolution of the Clinical Variables between Consecutive Visits
3.2. Evolution of Clinical Variables in Relation to the Day of Treatment
4. Discussion
5. Conclusions
- One single infiltration with 2 mL of platelet-rich plasma (PRP) in patients diagnosed with the Plantar Fascia Syndrome (PFS) is effective in the treatment of this pathology. Healing times are shortened and the effect is maintained in the long term.
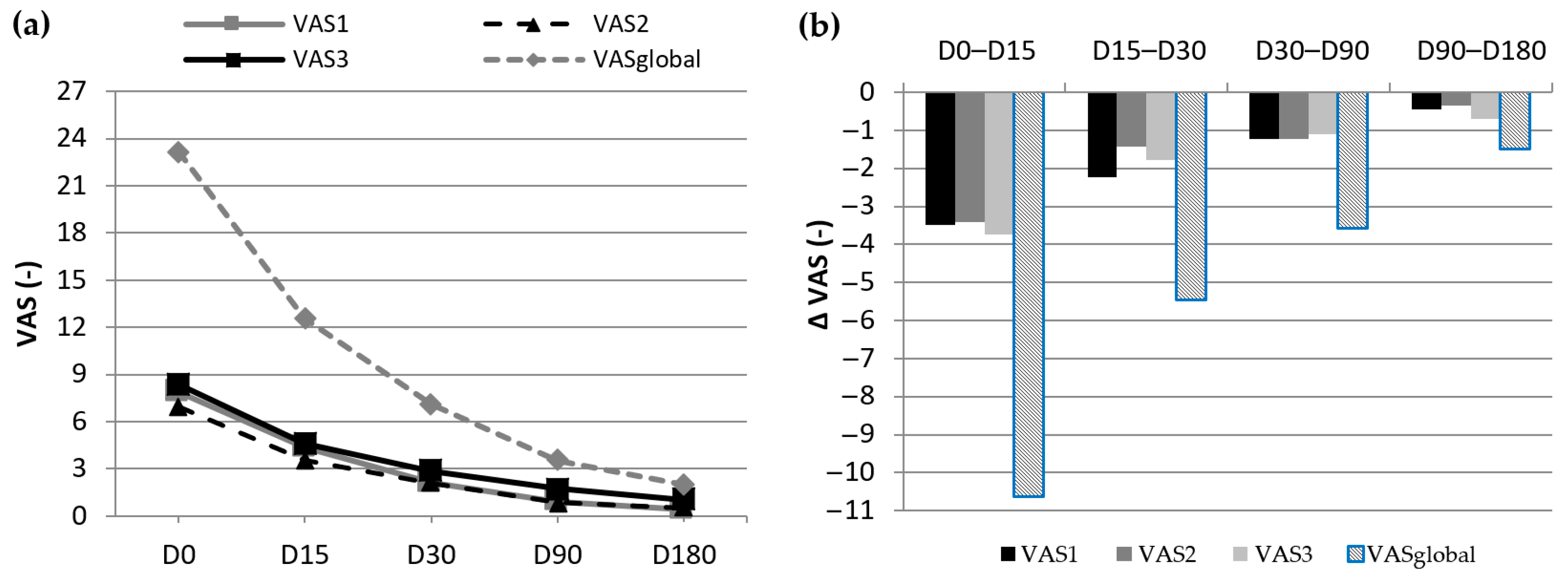
- There is a significant decrease in the pain measured during the 6 month study with the Visual Analogue Scale (first steps in the morning, first steps after a long rest, and sensitivity to touch in the affected area) according to the protocol schedule (Days 15, 30, 90, and 180).
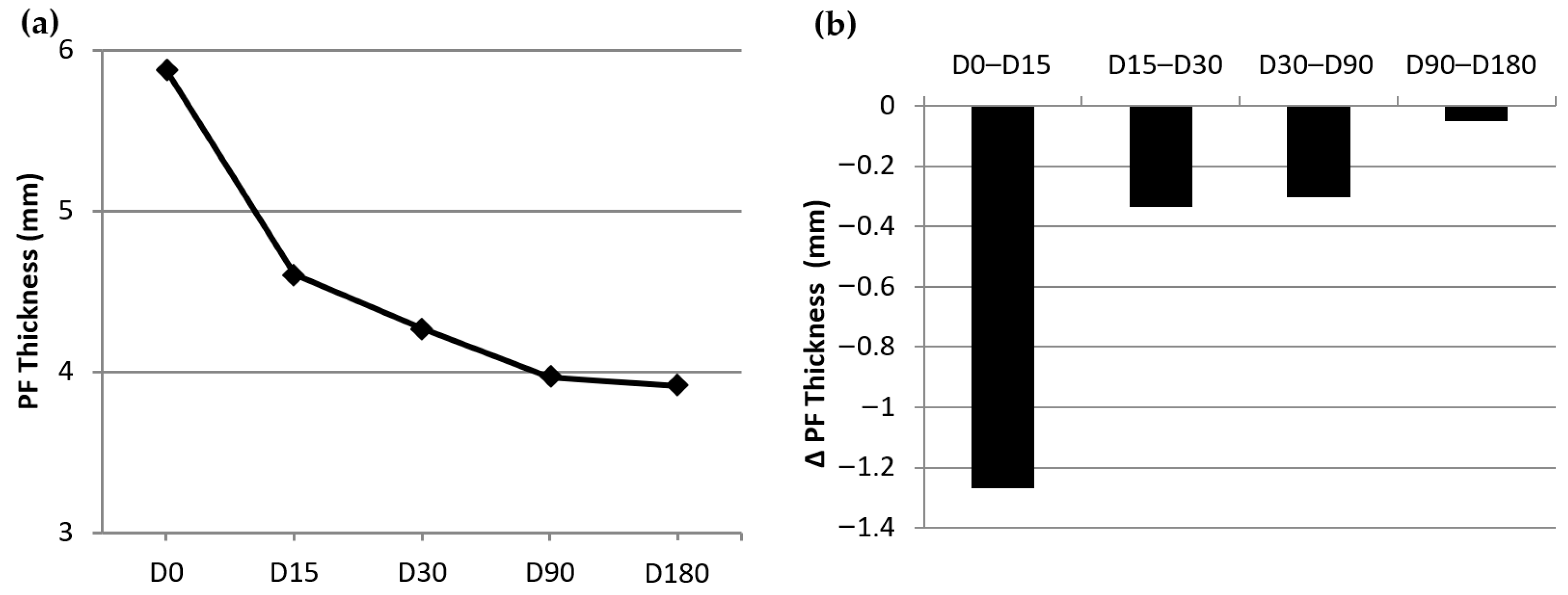
- There is a significant decrease in the plantar fascia thickness (PFT) measured during the 6 months study using ultrasonography according to the protocol schedule.
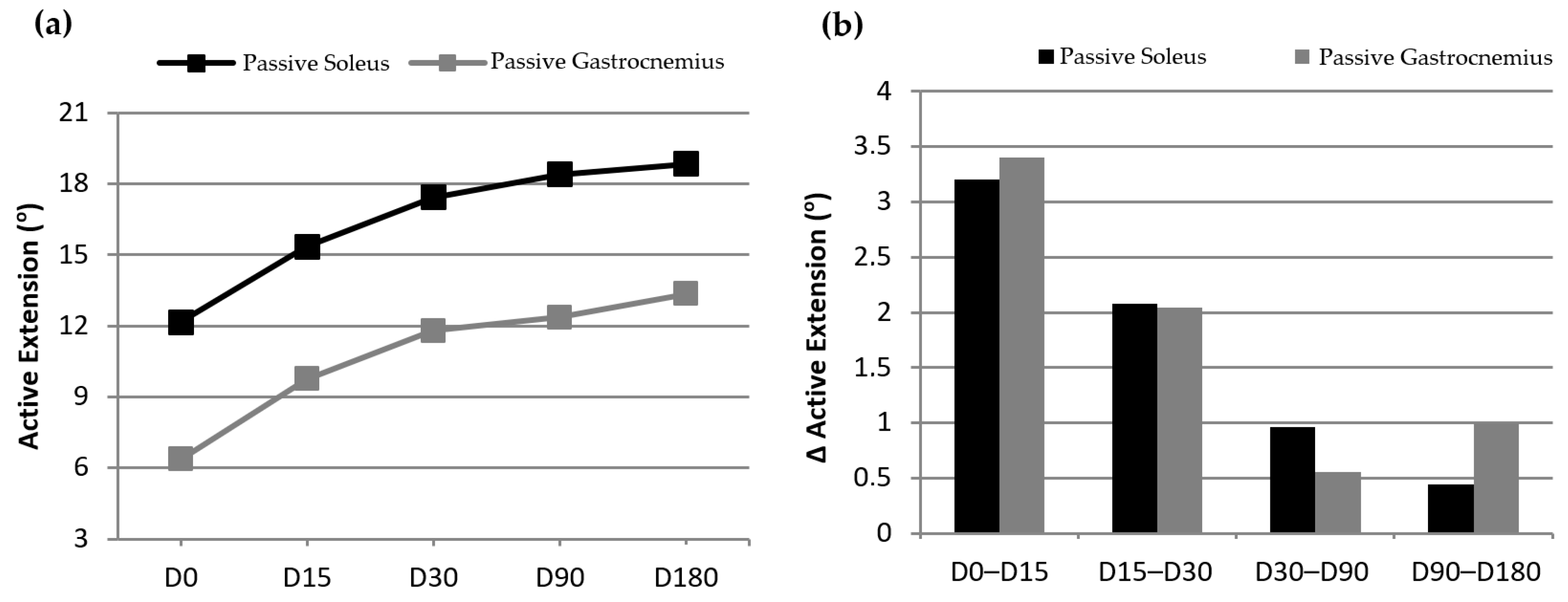
- There is a significant increase in the active extension of the ankle as measured during the 6 month study, both in passive soleus and passive gastrocnemius according to the protocol schedule.
- The improvement in clinical variables was maintained throughout the 6 months of the study.
- After 6 months, there is a clear correlation between plantar fascia thickness decrease and pain decrease.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dunn, J.; Link, C.; Felson, D.; Crincoli, M.G.; Keysor, J.J.; McKinlay, J.B. Prevalence of foot and ankle conditions in a multietnic community sample of older adults. Am. J. Epidemiol. 2004, 159, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Clement, D.B.; Taunton, J.E.; Smart, G.W.; McNicol, K.L. A Survey of Overuse Running Injuries. Physician Sportsmed. 1981, 9, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, R. Clinical Practice, Plantar Fasciitis. N. Engl. J. Med. 2004, 350, 2159–2166. [Google Scholar] [CrossRef] [PubMed]
- Dubin, J. Evidence based treatment for plantar fasciitis. Review of literature. Sports Ther. 2007, 27. Available online: https://dubinchiro.com/plantar.pdf (accessed on 29 November 2023).
- Landorf, K.B.; Menz, H.B. Plantar heel pain and fasciitis. BMJ Clin. Evid. 2008, 2008, 1111. [Google Scholar] [PubMed]
- Wearing, S.C.; E Smeathers, J.; Urry, S.R.; Hennig, E.M.; Hills, A.P. The pathomechanics of plantar fasciitis. Sports Med. 2006, 36, 585–611. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.J.; Lee, K.S.; Miller, A.T.; Wang, S. Platelet-rich plasma for the treatment of chronic plantar fasciopathy in adults: A case series. Foot Ankle Spec. 2014, 7, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Pardo Camps, F. Eficacia de la Infiltración de Plasma Rico en Plaquetas (PRP) en Pacientes Diagnosticados de Síndrome de la Fascia Plantar Desde el Punto de Vista Clínico i Funcional. (Efficacy of Platelet-Rich Plasma (PRP) Infiltrations in Patients Diagnosed with Plantar Fascia Syndrome (PFS) from a Clinical and Functional Perspective). Ph.D. Thesis, Universidad Complutense de Madrid, Madrid, Spain, 2016. [Google Scholar]
- Riddle, D.L.; Schappert, S.M. Volume of ambulatory care visits and patterns of care of patients diagnosed with plantar fasciitis: A national study of medi-cal doctors. Foot Ankle Int. 2004, 25, 303–310. [Google Scholar] [CrossRef]
- Hillmann, G.; Geurtsen, W. Tissue engineering—An exciting future. Clin. Oral. Investig. 2001, 5, 1. [Google Scholar] [CrossRef]
- Tate, K.; Crane, D. Platelet rich plasma graffts in musculoskeletal medicine. J. Prolotherapy 2010, 2, 371–376. [Google Scholar]
- Marx, R.E. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Olea, J.; Olea, N. Plasma enriquecido de plaquetas en regeneración ósea maxilar con implantes óseointegrados y estudio de microscopía óptica y electrónica. electrónica (Enriched platelet plasma in maxillary bone regeneration with osseointegrated implants and study of optical and electronic microscopy). Rev. Española Odontoestomatológica De Implant. 2002, 10, 146–150. [Google Scholar]
- Gehring, S.; Hoerauf, H.; Laqua, H.; Kirchner, H.; Klüter, H. Preparation of autologous platelets for the ophthalmologic treat-ment of macular holes. Transfusion 1999, 39, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Márquez de Aracena del Cid, R.; Montero de Espinosa Escoriaza, I.; Muñoz Saez, M. Tratamiento con concentrado plaquetario plasmático subconjuntival y tópico en el transplante de limbo. (Treatment with subconjunctival and topical plasmatic plate-let concentrate in limbus transplantation). Mapfre Med. 2006, 17, 280–285. [Google Scholar]
- Kjaergard, H.K.; Pedersen, J.H.; Krasnik, M.; Weis-Fogh, U.S.; Fleron, H.; Griffin, H.E. Prevention of air leakage by spraying vivostat fibrin sealant after lung resection in pigs. Chest 2000, 117, 1124–1127. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Whitman, D.H.; Berry, R.L.; Green, D.M. Platelet gel: An autologous alternative to fibrin glue with applications in oral and max-illofacial surgery. J. Oral. Maxillofac. Surg. 1997, 17, 1124–1127. [Google Scholar] [CrossRef]
- Anitua, E.A. Enhancement of Osseointegration by Generating a Dynamic Implant Surface. J. Oral Implant. 2006, 32, 72–76. [Google Scholar] [CrossRef]
- Ballester, J.F.; Álvarez, A.; López, I.; Molinos, J.R.; Arnás, M.; Vera, J.M. Protocolo para la obtención de PDGF a partir de PRF. (Proto-col for obtaining PDGF from PRF). Rev. Esp. Odontoestomatológica De Implant. 2004, 12, 14–29. [Google Scholar]
- Van Der Berg, W.B.; Van Der Kraan, P.M.; Scharsthul, A.; van Beuningen, H.M. Growth factors and cartilage repair. Clin. Ortop. 2001, 391, S244–S250. [Google Scholar] [CrossRef]
- Sánchez, M.; Anitua, E.; Azofra, J.; Andía, I.; Padilla, S.; Mujika, I. Comparison of surgically repaired Achilles tears using platelet-rich fibrin matrices. Am. J. Sports Med. 2007, 35, 245–251. [Google Scholar] [CrossRef]
- Cugat, R.; Wang-Seagusa, A.; Ares, O.; Seijas, R.; Cuscó, X. Infiltration of plasma rich in growth factors for osteoarthritis of the knee shrot-term effects on function and quality of life. Arch. Orthop. Trauma Surg. 2010, 131, 1167–1173. [Google Scholar]
- Rubio-Azpeitia, E.; Bilbao, A.M.; Sánchez, P.; Delgado, D.; Andia, I. The Properties of 3 Different Plasma Formulations and Their Effects on Tendinopathic Cells. Am. J. Sports Med. 2016, 44, 1952–1961. [Google Scholar] [CrossRef] [PubMed]
- Moojem, D.J.; Everts, P.A.; Schure, R.M.; Overdevest, E.P.; van Zundert, A.; Knape, J.T.A.; Castelein, R.M.; Creemers, L.B.; Dhert, W.J.A. Antimicrobial activity of platelet-leukocyte gel against Staphyloccus aureus. J. Orthop. Res. 2008, 26, 404–410. [Google Scholar] [CrossRef]
- Abellanet, I. La Terapia de Lesiones de Tejidos Blandos y Articulaciones con Plasma Rico en Plaquetas en Caballos de Deporte: Evidencia Clínica y Bioquímica que Valida su Utilización. (Therapy of Soft Tissue Injuries and Joints with Platelet-Rich Plasma in Sports Horses: Clinical and Biochemical Evidence Validating Its Use). Ph.D. Thesis, Universidad Autónoma de Barcelona, Barcelona, Spain, 2009. [Google Scholar]
- Gupta, M.; Latkar Ch Patil, S. Efficacy and role of local injection of platelet rich plasma and local corticosteroid injection in the treatment of plantar fasciitis. Indian J. Appl. Res. 2015, 5, 558–561. [Google Scholar]
- Petraglia, F.; Ramazzina, I.; Costantino, C. Plantar fasciitis in athletes: Diagnostic and treatment strategies. A systematic review. Muscle Ligaments Tendons J. 2017, 7, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Vertuccio, A.; Perugia, D.; Lanzetti, R.; Massimiani, A.; Lacopo, A.; Nusca, S.; Baldini, R.; Santoboni, F.; Latini, E.; Vetrano, M.; et al. Demographic and Clinical Factors Predict Focused Shockwave Therapy Results on Patients with Plantar Fasciitis. A Multilevel Analysis. Muscle Ligaments Tendons J. 2021, 11, 376–382. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.; Andia, I.; Zumstein, M.A.; Zhang, C.Q.; Pinto, N.R.; Bielecki, T. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: Cur-rent consensus, clinical implications and perspectives. Muscles Ligaments Tendons J. 2014, 4, 3–9. [Google Scholar] [CrossRef]
- Dyck, D.; Boyajian-O´Neill, L. Plantar Fasciitis. Clin. J. Sport Med. 2004, 14, 305–309. [Google Scholar] [CrossRef]
- Chana, P. Eficacia de los Impulsos Eléctricos de Bajo Voltaje en la Fasciosis Plantar. (Low voltage Electrical Impulses Efficacy in Plantar Fasciosis). Ph.D. Thesis, Universidad Complutense de Madrid, Madrid, Spain, 2013. [Google Scholar]
- Vohra, P.K.; Kincaid, B.R.; Japour, C.J.; Sobel, E. Ultrasonographic evaluation of plantar fascia bands. A retrospective study of 211 symptomatic feet. J. Am. Podiatr. Med. Assoc. 2002, 92, 444–449. [Google Scholar] [CrossRef]
- Wearing, S.; Smeathers, J.; Sullivan, P.; Yates, B.; Urry, S.R.; Dubois, P. Plantar Fasciitis: Are pain and fascial thickness associated with arch shape and loading? Phys. Ter. 2007, 87, 1002–1008. [Google Scholar] [CrossRef]
- Mc Millan, A.M.; Landorf, K.; Barret, J.T.; Menz, H.; Bird, A. Diagnostic imaging for chronic plantar heel pain: A systematic review and meta-analysis. J. Foot Ankle Res. 2009, 2, 32. [Google Scholar] [CrossRef] [PubMed]
- Cozen, L. Ortopedia práctica (Practical orthopedics). Elicien. Barc. 1977, 3, 55–62. [Google Scholar]
- Hamilton, W.G. Surgical Anatomy of the Foot and Ankle (Clinical Symposia). Clin. Symp. 1985, 37, 2–32. [Google Scholar]
- Peerbooms, J.C.; Sluimer j Bruijn, D.J.; Gosens, T. Positive effect of an autologous platelet concentrate in lateral epicondylitis in double-blind randomized controlled trial: Platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. Am. J. Sports Med. 2010, 38, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, N.; Marinozzi, A.; Carni, S.; Trovato, U.; Bianchi, A.; Denaro, V. Platelet-rich plasma injections for chronic plantar fasciitis. Int. Orthop. 2012, 19, S1432–S5195. [Google Scholar] [CrossRef] [PubMed]
- Uğurlar, M.; Sönmez, M.M.; Uğurlar, Y.; Adıyeke, L.; Yıldırım, H.; Eren, O.T. Effectiveness of four different treatment modalities in the treatment of chronic plantar fasciitis during a 36-Month Follow-Up Period: A randomized controlled trial. J. Foot Ankle Surg. 2018, 57, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Goel, N.; Talwar, J.; Agarwal, S.; Krishna, L.G.; Rustagi, A. A comparative study between intralesional platelet rich plasma injection and extracorporeal shockwave therapy for the treatment of plantar fasciitis. J. Arthrosc. Jt. Surg. 2021, 8, 246–252. [Google Scholar] [CrossRef]
- Alessio-Mazzola, M.; Stambazzi, C.; Ursino, C.; Tagliafico, A.; Trentini, R.; Formica, M. Ultrasound-Guided autologous Platelet-Rich plasma injections versus Focal Ultrasound-Guided extracorporeal shockwave therapy for plantar fasciitis in Athletes and nonathletes: A Retrospective Comparative Study with minimum 2-Year Follow-Up. J. Foot Ankle Surg. 2023, 62, 417–421. [Google Scholar] [CrossRef]
- Eunkuk, K.; Lee, J.H. Autologous platelet-rich plasma versus dextrose prolotherapy for the treatment of chronic recalcitrant plantar faciitis. PM&R 2014, 6, 152–158. [Google Scholar]
- Baz, A.A.; Gad, A.M.; Waly, M.R. Ultrasound guided injection of platelet rich plasma in cases of chronic plantar fasciitis. Egypt. J. Radiol. Nucl. Med. 2017, 48, 125–132. [Google Scholar] [CrossRef]
- Gonnade, N.; Bajpayee, A.; Elhence, A.; Lokhande, V.; Mehta, N.; Mishra, M.; Kaur, A. Regenerative efficacy of therapeutic quality platelet-rich plasma injections versus phonophoresis with kinesiotaping for the treatment of chronic plantar fasciitis: A prospective randomized pilot study. Asian J. Transfus. Sci. 2018, 12, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Scioli, M. Platelet-rich plasma injection for proximal plantar fasciitis. Tech. Foot Ankle 2011, 10, 7–10. [Google Scholar] [CrossRef]
- Barrett, S.L.; Erredge, S.E. Growth factors for chronic plantar fasciitis. Podiatry Today 2004, 99, 108–113. [Google Scholar]
- Aksahin, E.; Dogruyol, D.; Yüksel, H.Y.; Hapa, O.; Dogan, O.; Celebi, L.; Biçimoglu, A. The comparison of the effect of corticoster-oids and platelet-rich plasma (PRP) for the treatment of plantar fasciitis. Arch. Orthop. Trauma Surg. 2012, 132, 781–785. [Google Scholar] [CrossRef]
- Kalia, R.B.; Singh, V.; Chowdhury, N.; Jain, A.; Singh, S.K.; Das, L. Role of platelet rich plasma in chronic plantar fasciitis: A prospective study. Indian J. Orthop. 2020, 55, 142–148. [Google Scholar] [CrossRef]
- Sathyendra, K.; Solankey, R.D.; Singh, M.; Kumar, S.V.; Singh, G.; Gupta, M.M. Comparative study of local injections of autologous platelet rich plasma versus corticosteroid in management of chronic plantar fasciitis. J. Clin. Orthop. Trauma 2023, 43, 102225. [Google Scholar] [CrossRef]
- Vellingiri, K.; Nagakumar, J.S.; Manohar, V.P.; Lourdu, J.P.; Suryanarayana, M.S.A. A prospective study comparing the efficacy of local injection of Platelet-Rich plasma (PRP) vs. methylprednisolone in plantar fasciitis. Cureus 2022, 14, e25523. [Google Scholar] [CrossRef]
- Pandey, S.; Kumar, N.; Kumar, A.; Biswas, A.; Sinha, U.; Pandey, J.; Ghosh, S.; Das, S.; A Johnson, R.; Kumar, R.; et al. Extracorporeal shockwave therapy versus platelet rich plasma injection in patients of chronic plantar fasciitis: A randomized controlled trial from a tertiary center of eastern India. Cureus 2023, 15, e34430. [Google Scholar] [CrossRef]
- Soraganvi, P.; Nagakiran, K.V.; Raghavendra-Raju, R.P.; Anilkumar, D.; Wooly, S.; Basti, B.D.; Janakiraman, P. Is platelet-rich plasma injection more effective than steroid injection in the treatment of chronic plantar fasciitis in achieving long-term relief? Malays. Orthop. J. 2019, 13, 8–14. [Google Scholar] [CrossRef]
- Ruiz-Hernández, I.M.; Gascó-Adrien, J.; Buen-Ruiz, C.; Perelló-Moreno, L.; Tornero-Prieto, C.; Barrantes-Delgado, G.; García-Gutiérrez, M.; Rapariz-González, J.; Tejada-Gavela, S. Botulinum toxin A versus platelet rich plasma ultrasound-guided injection in the treatment of plantar fasciitis: A randomised controlled trial. Foot Ankle Surg. 2023. [Google Scholar] [CrossRef]
- Hafez, A.; Ismail, F.; Abdelhakeem, M.; Ragaee, S.; Soliman, S. Musculoskeletal ultrasound changes in chronic plantar fascia after treatment with platelet rich plasma compared to steroid. Muscle Ligaments Tendons J. 2023, 13, 126–134. [Google Scholar] [CrossRef]
- Jiménez-Pérez, A.E.; Gonzalez-Arabio, D.; Diaz, A.S.; Maderuelo, J.A.; Ramos-Pascua, L.R. Clinical and imaging effects of corticosteroids and platelet-rich plasma for the treatment of chronic plantar fasciitis: A comparative non randomized prospective study. Foot Ankle Surg. 2018, 25, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, A.; Banerjee, R.; Ghosh, S. Use of Platelet-Rich Plasma Injection for the Treatent of Chronic Plantar Fasciitis. J. Evid. Based Med. Healthc. 2014, 1, 1489–1493. [Google Scholar] [CrossRef]
- Shetty, S.H.; Dhond, A.; Arora, M.; Deore, S. Platelet-Rich plasma has Better Long-Term results than corticosteroids or placebo for chronic plantar fasciitis: Randomized Control trial. J. Foot Ankle Surg. 2019, 58, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Khurana, A.; Dhankhar, V.; Goel, N.; Gupta, R.; Goyal, A. Comparison of midterm results of Platelet Rich Plasma (PRP) versus Steroid for plantar fasciitis: A randomized control trial of 118 patients. J. Clin. Orthop. Trauma 2020, 13, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Prakash, Y.R.; Dhanda, A.; Yallapur, K.L.; Inamdar, S.S.; Darshan, G.T.; Ramakrishna, M. Peppering versus Single Injection Technique in Tennis Elbow—A Prospective Comparative Study. Malays. Orthop. J. 2022, 16, 91–96. [Google Scholar] [CrossRef]
- Ragab, E.; Othman, A. Platelet rich plasma for treatment of chronic plantar fasciitis. Arch. Orthop. Trauma Surg. 2012, 132, 1065–1070. [Google Scholar] [CrossRef]
- Paulus, J.K.; Dahabreh, I.J.; Balk, E.M.; Avendano, E.E.; Lau, J.; Ip, S. Opportunities and challenges in using studies without a control group in comparative effectiveness reviews. Res. Synth. Methods 2013, 5, 152–161. [Google Scholar] [CrossRef]
- Aggarwal, R.; Ranganathan, P. Study designs: Part 4—Interventional studies. Perspect. Clin. Res. 2019, 10, 137–139. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Weight (kg) | Height (m) | BMI (kg/m2) | Symp. Dura. (Months) | |
|---|---|---|---|---|---|
| Mean ± σ | 48.9 ± 9.74 | 76.44 ± 15.10 | 1.64 ± 0.09 | 28.24 ± 4.65 | 15.76 ± 11.91 |
| D0 | D15 | D30 | D90 | D180 | |
|---|---|---|---|---|---|
| VAS1 | 7.86 ± 1.59 | 4.38 ± 2.08 | 2.14 ± 2.10 | 0.9 ± 1.44 | 0.44 ± 0.82 |
| VAS2 | 6.98 ± 1.49 | 3.54 ± 2.37 | 2.1 ± 2.08 | 0.86 ± 1.32 | 0.52 ± 0.82 |
| VAS3 | 8.36 ± 1.38 | 4.62 ± 2.59 | 2.84 ± 2.09 | 1.74 ± 1.76 | 1.04 ± 1.39 |
| VASglobal | 23.18 ± 3.58 | 12.54 ± 6.33 | 7.08 ± 5.71 | 3.5 ± 3.52 | 2 ± 2.58 |
| PFT | 5.87 ± 1.04 | 4.60 ± 1.47 | 4.27 ± 1.42 | 3.96 ± 1.30 | 3.91 ± 1.24 |
| AES | 12.16 ± 4.97 | 15.36 ± 4.5 | 17.44 ± 4.23 | 18.4 ± 4.25 | 18.84 ± 3.99 |
| AEG | 6.36 ± 5.84 | 9.76 ± 4.98 | 11.8 ± 3.98 | 12.36 ± 3.91 | 13.36 ± 3.55 |
| D0–D15 | p-Value | D15–D30 | p-Value | D30–D90 | p-Value | D90–D180 | p-Value | |
|---|---|---|---|---|---|---|---|---|
| VAS1 | −5.72 ± 2.24 | 0.000 | −2.24 ± 1.73 | 0.000 | −1.24 ± 1.76 | 0.003 | −0.46 ± 1.49 | 0.138 * |
| VAS2 | −4.86 ± 1.74 | 0.000 | −1.44 ± 1.85 | 0.000 | −1.24 ± 2.34 | 0.017 | −0.34 ± 1.04 | 0.117 * |
| VAS3 | −5.52 ± 2.31 | 0.000 | −1.78 ± 2.58 | 0.008 | −1.10 ± 2.25 | 0.030 | −0.7 ± 1.19 | 0.007 |
| VASglobal | −16.10 ± 5.42 | 0.000 | −5.46 ± 4.89 | 0.000 | −3.58 ± 5.47 | 0.007 | −1.5 ± 2.90 | 0.016 |
| PFT | −1.60 ± 1.13 | 0.000 | −0.33 ± 0.61 | 0.000 | −0.30 ± 0.41 | 0.002 | −0.05 ± 0.320 | 0.424 * |
| AES | 5.28 ± 3.51 | 0.000 | 2.08 ± 3.93 | 0.017 | 0.96 ± 4.39 | 0.245 * | 0.44 ± 4.33 | 0.530 * |
| AEG | 5.44 ± 4.95 | 0.000 | 2.04 ± 3.67 | 0.019 | 0.56 ± 4.16 | 0.384 * | 1.56 ± 3.41 | 0.034 |
| D0–D15 | p-Value | D0–D30 | p-Value | D0–D90 | p-Value | D0–D180 | p-Value | |
|---|---|---|---|---|---|---|---|---|
| VAS1 | −3.48 ± 1.94 | 0.000 | −5.72 ± 2.24 | 0.000 | −6.96 ± 1.91 | 0.000 | −7.42 ± 1.93 | 0.000 |
| VAS2 | −3.42 ± 2.20 | 0.000 | −4.86 ± 1.74 | 0.000 | −6.10 ± 2.06 | 0.000 | −6.44 ± 1.68 | 0.000 |
| VAS3 | −3.74 ± 2.70 | 0.000 | −5.52 ± 2.31 | 0.000 | −6.62 ± 2.22 | 0.000 | −7.32 ± 1.82 | 0.000 |
| VASglobal | −10.64 ± 6.35 | 0.000 | −16.10 ± 5.42 | 0.000 | −19.68 ± 5.18 | 0.000 | −21.18 ± 4.65 | 0.000 |
| PFT | −1.27 ± 1.01 | 0.000 | −1.60 ± 1.13 | 0.000 | −1.91 ± 1.07 | 0.000 | −1.96 ± 1.09 | 0.000 |
| AES | 3.20 ± 4.42 | 0.000 | 5.28 ± 3.51 | 0.000 | 4.97 ± 4.25 | 0.000 | 6.68 ± 5.28 | 0.000 |
| AEG | 3.40 ± 4.95 | 0.000 | 5.44 ± 4.95 | 0.000 | 5.85 ± 3.91 | 0.000 | 7.00 ± 5.22 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardo-Camps, F.; Pardo-Bosch, F. New Infiltration Technique in the Treatment of the Plantar Fascia Syndrome Based on Platelet-Rich Plasma. J. Clin. Med. 2024, 13, 170. https://doi.org/10.3390/jcm13010170
Pardo-Camps F, Pardo-Bosch F. New Infiltration Technique in the Treatment of the Plantar Fascia Syndrome Based on Platelet-Rich Plasma. Journal of Clinical Medicine. 2024; 13(1):170. https://doi.org/10.3390/jcm13010170
Chicago/Turabian StylePardo-Camps, Francesc, and Francesc Pardo-Bosch. 2024. "New Infiltration Technique in the Treatment of the Plantar Fascia Syndrome Based on Platelet-Rich Plasma" Journal of Clinical Medicine 13, no. 1: 170. https://doi.org/10.3390/jcm13010170
APA StylePardo-Camps, F., & Pardo-Bosch, F. (2024). New Infiltration Technique in the Treatment of the Plantar Fascia Syndrome Based on Platelet-Rich Plasma. Journal of Clinical Medicine, 13(1), 170. https://doi.org/10.3390/jcm13010170