
Effects of a Single Session of Systemic Vibratory Therapy on Flexibility, Perception of Exertion and Handgrip Strength in Chronic Obstructive Pulmonary Disease Individuals: A Quasi-Experimental Clinical Trial

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
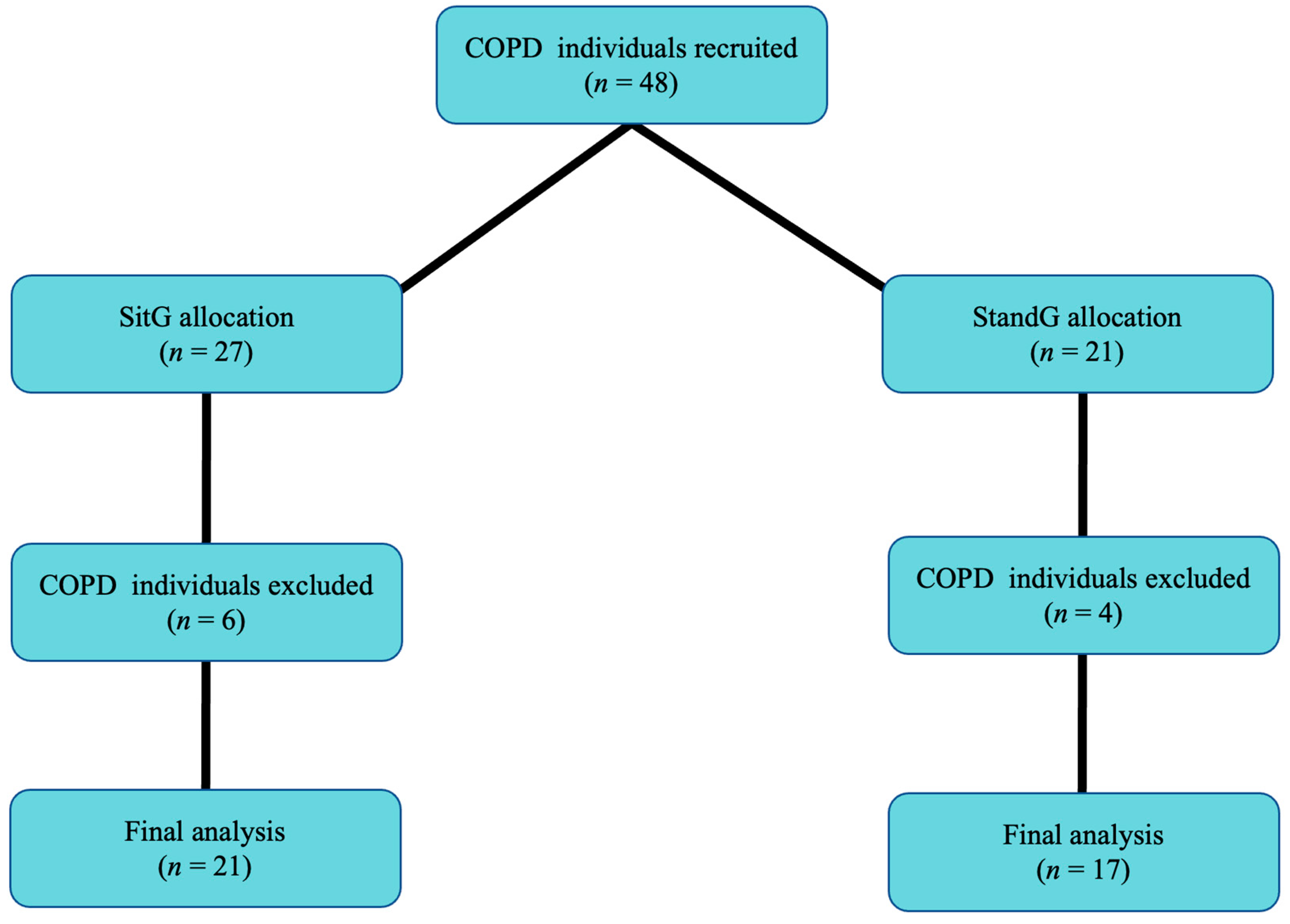
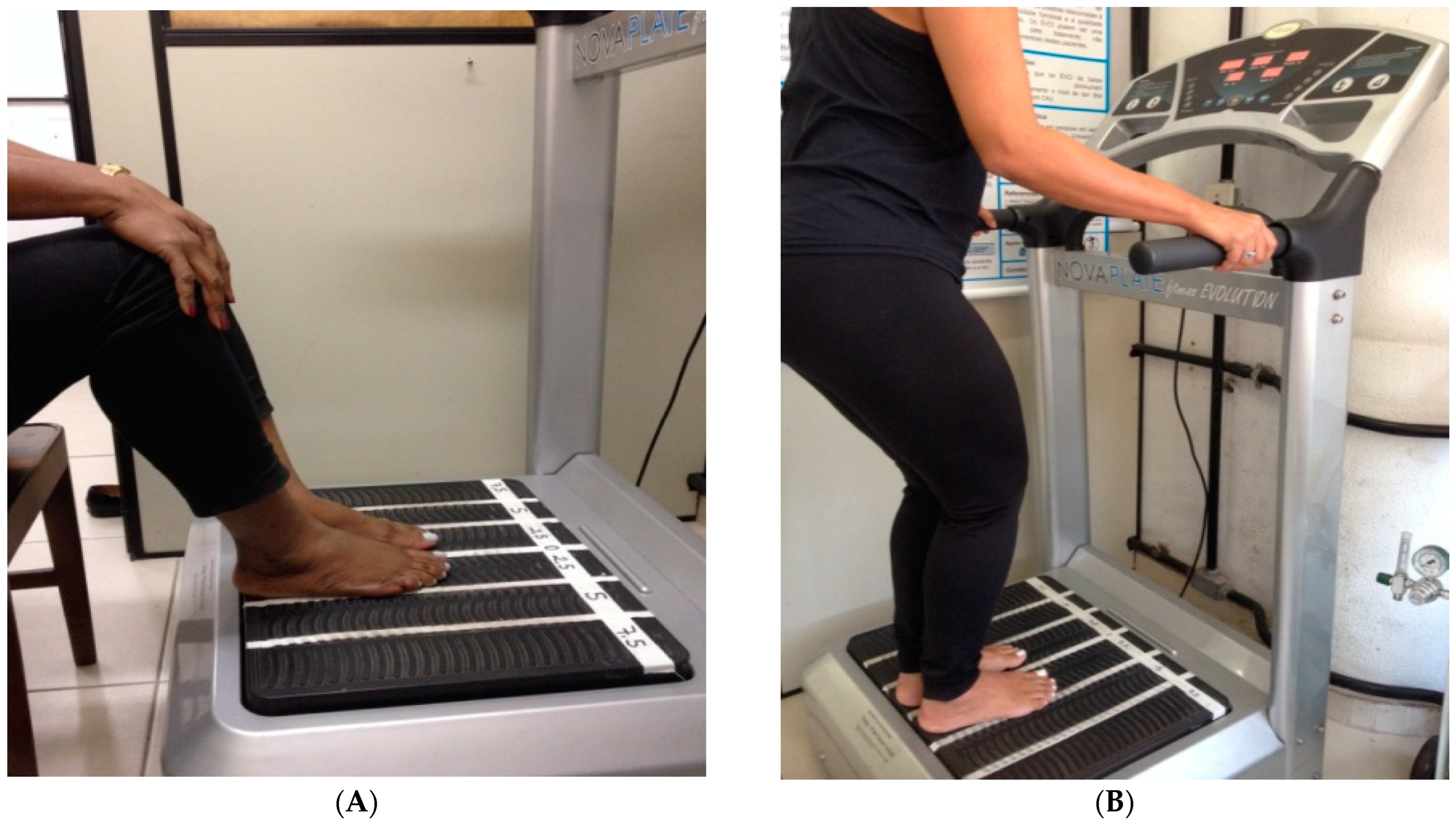
2.1. Study Design
2.2. Participants
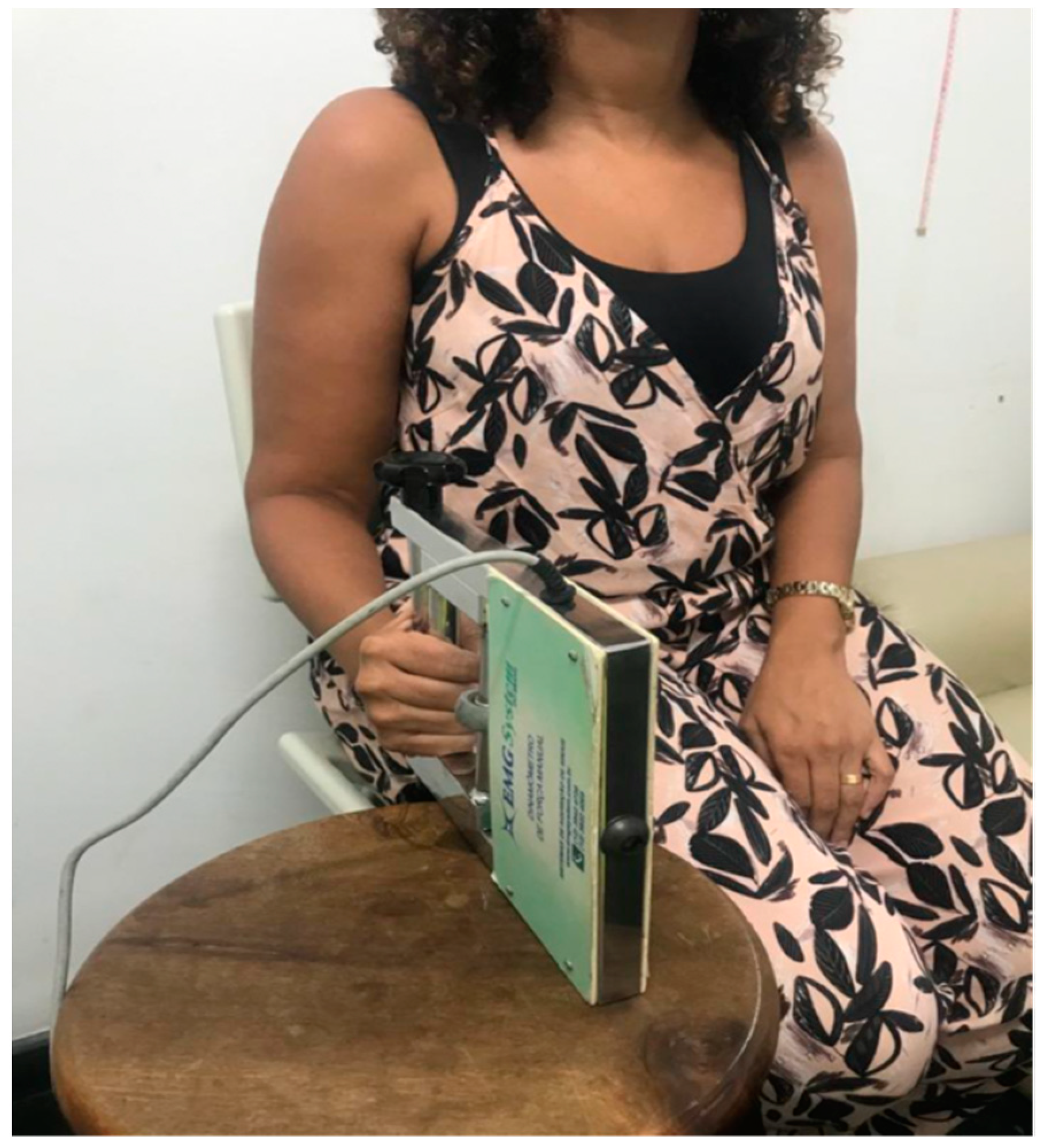
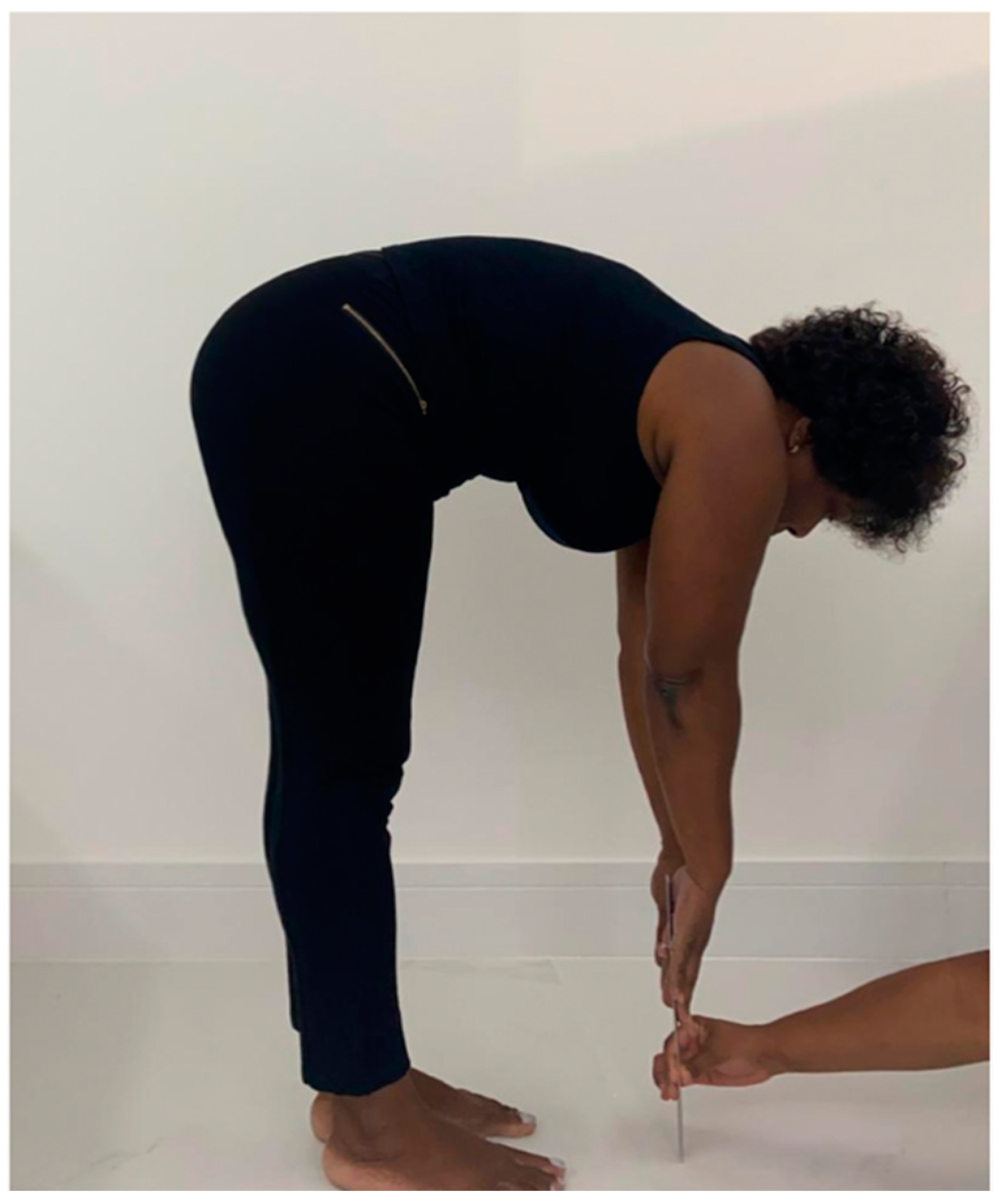
2.3. Study Protocol (Procedures)
2.4. Statistical Analysis
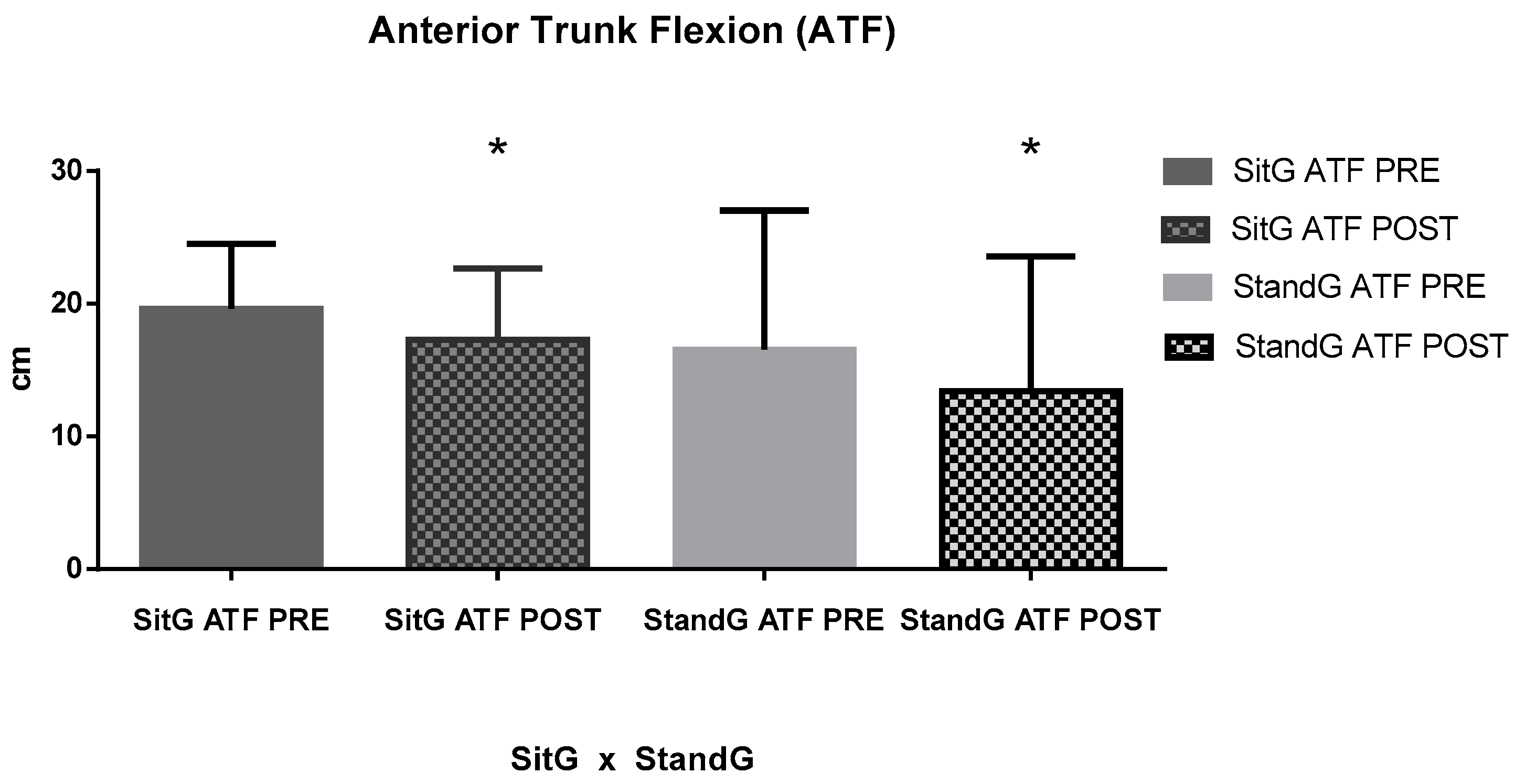
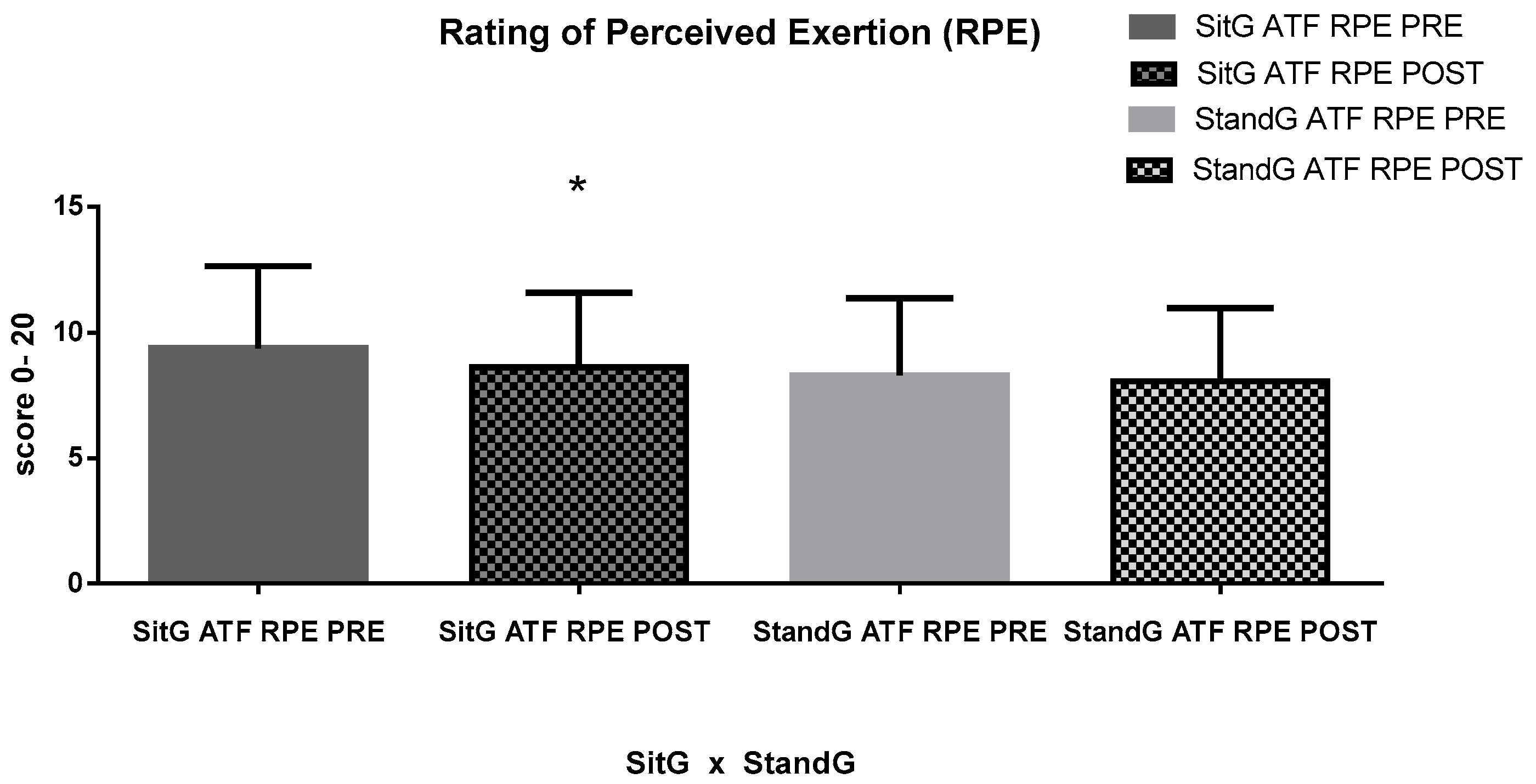
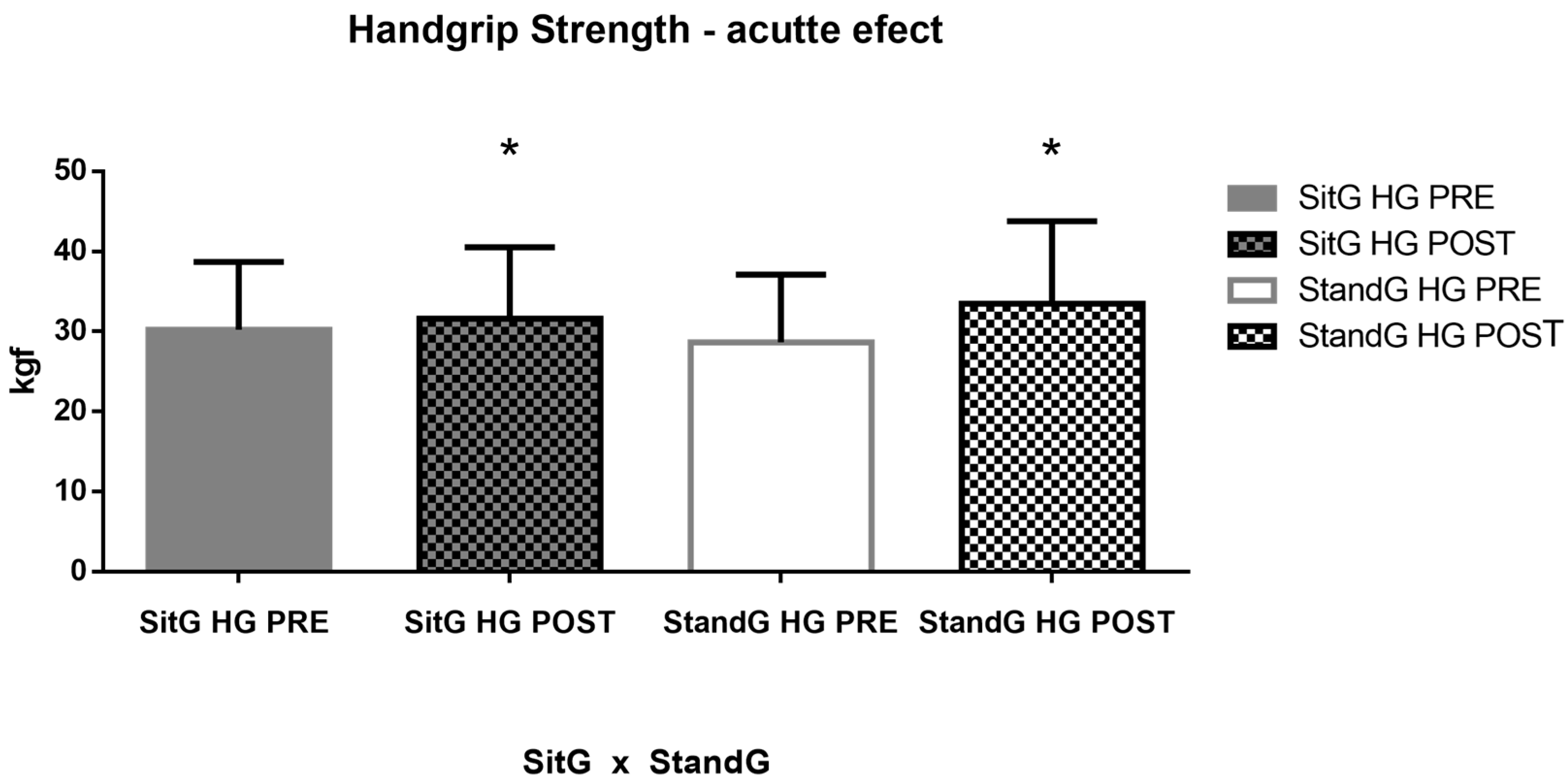
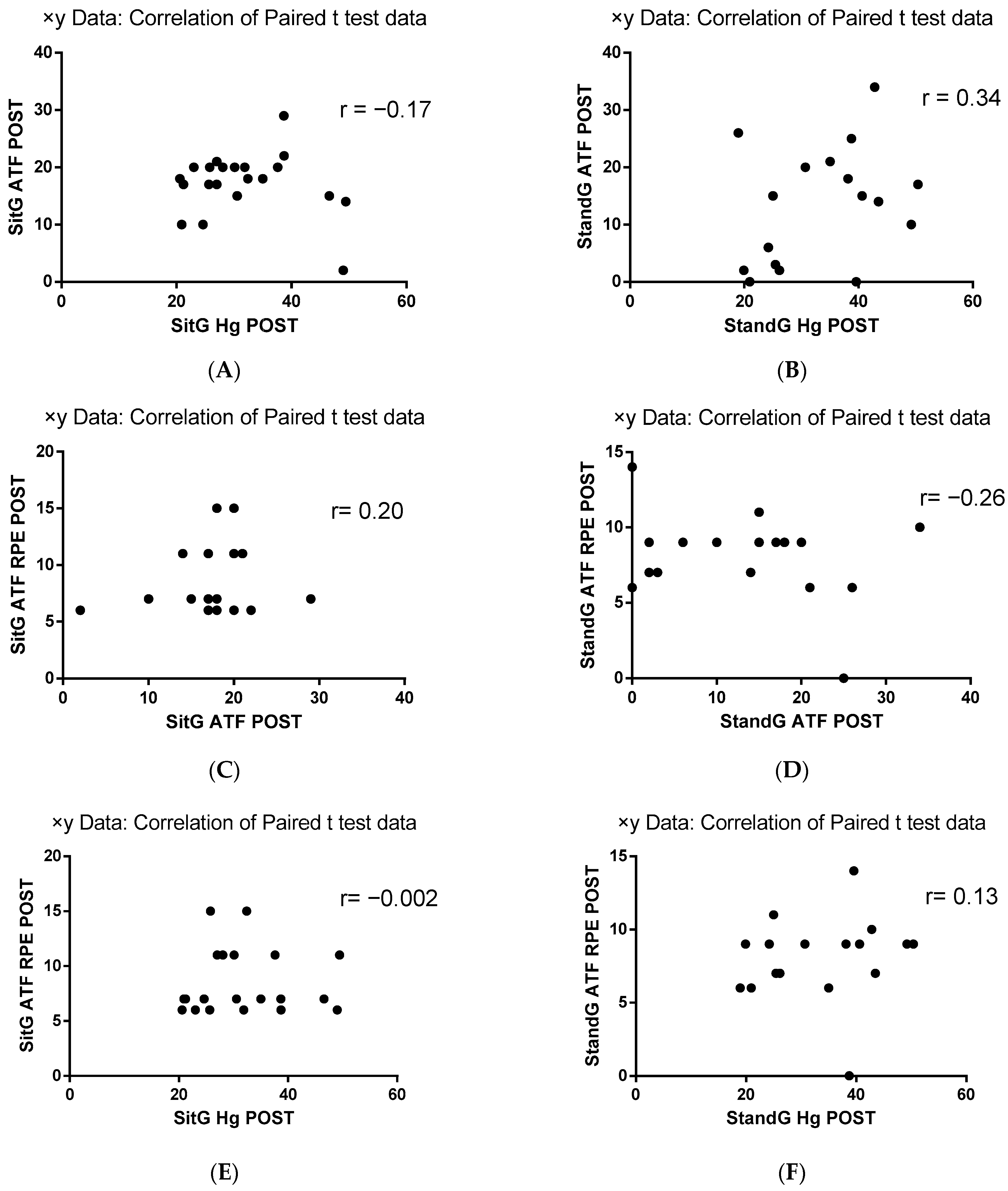
3. Results
Individual Characteristics
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease—Report. Global Initiative for Chronic Obstructive Lung Disease. 2023. Available online: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf (accessed on 6 July 2022).
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 15, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Gea, J.; Pascual, S.; Casadevall, C.; Orozco-Levi, M.; Barreiro, E. Muscle dysfunction in chronic obstructive pulmonary disease: Update on causes and biological findings. J. Thorac. Dis. 2015, 7, E418–E438. [Google Scholar] [CrossRef] [PubMed]
- Rassler, B. Impaired function of upper limb muscles in patients with chronic obstructive pulmonary disease. Indian J. Med. Res. 2013, 138, 443–445. [Google Scholar] [PubMed]
- Barreiro, E.; Jaitovich, A. Muscle atrophy in chronic obstructive pulmonary disease: Molecular basis and potential therapeutic targets. J. Thorac. Dis. 2018, 10 (Suppl. S12), S1415–S1424. [Google Scholar] [CrossRef]
- Ho, G.J.; Liew, S.M.; Ng, C.J.; Hisham Shunmugam, R.; Glasziou, P. Development of a search strategy for an evidence based retrieval service. PLoS ONE 2016, 11, e0167170. [Google Scholar] [CrossRef]
- Maltais, F.; Decramer, M.; Casaburi, R.; Barreiro, E.; Burelle, Y.; Debigaré, R.; Dekhuijzen, P.N.R.; Franssen, F.; Gayan-Ramirez, G.; Gea, J.; et al. An official american thoracic society/european respiratory society statement: Update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2014, 189, 15–62. [Google Scholar] [CrossRef]
- Rejc, E.; Floreani, M.; Taboga, P.; Botter, A.; Toniolo, L.; Cancellara, L.; Narici, M.; Šimunič, B.; Pišot, R.; Biolo, G.; et al. Loss of maximal explosive power of lower limbs after 2 weeks of disuse and incomplete recovery after retraining in older adults. J. Physiol. 2018, 15, 647–665. [Google Scholar] [CrossRef]
- Janssens, T.; Van de Moortel, Z.; Geidl, W.; Carl, J.; Pfeifer, K.; Lehbert, N.; Wittmann, M.; Schultz, K.; von Leupoldt, A. Impact of disease-specific fears on pulmonary rehabilitation trajectories in patients with COPD. J. Clin. Med. 2019, 8, 1460. [Google Scholar] [CrossRef]
- Adolfo, J.R.; Dhein, W.; Sbruzzi, G. Intensity of physical exercise and its effect on functional capacity in COPD: Systematic review and meta-analysis. J. Bras. Pneumol. 2019, 45, 20180011. [Google Scholar] [CrossRef]
- Abdulai, R.M.; Jensen, T.J.; Patel, N.R.; Polkey, M.I.; Jansson, P.; Celli, B.R.; Rennard, S.I. Deterioration of limb muscle function during acute exacerbation of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2018, 15, 433–449. [Google Scholar] [CrossRef]
- Mccarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2020, 16, CD012626. [Google Scholar] [CrossRef]
- Wouters, E.F.; Posthuma, R.; Koopman, M.; Liu, W.-Y.; Sillen, M.J.; Hajian, B.; Sastry, M.; Spruit, M.A.; Franssen, F.M. An update on pulmonary rehabilitation techniques for patients with chronic obstructive pulmonary disease. Expert Rev. Respir. Med. 2020, 14, 149–161. [Google Scholar] [CrossRef]
- Corhay, J.L.; Nguyen, D.; Van Cauwenberge, H.; Louis, R. Pulmonary rehabilitation and COPD: Providing patients a good environment for optimizing therapy. Int. J. Chron Obstruct. Pulm. Dis. 2014, 9, 27–39. [Google Scholar] [CrossRef]
- Opplert, J.; Babault, N. Acute effects of dynamic stretching on muscle flexibility and performance: An analysis of the current literature. Sports Med. 2018, 48, 299–325. [Google Scholar] [CrossRef]
- Furness, T.; Joseph, C.; Naughton, G.; Welsh, L.; Lorenzen, C. Benefits of whole-body vibration to people with COPD: A community-based efficacy trial. BMC Pulm. Med. 2014, 8, 14–38. [Google Scholar] [CrossRef]
- Gloeckl, R.; Heinzelmann, I.; Baeuerle, S.; Damm, E.; Schwedhelm, A.-L.L.; Diril, M.; Buhrow, D.; Jerrentrup, A.; Kenn, K. Effects of whole body vibration in patients with chronic obstructive pulmonary disease—A randomized controlled trial. Respir. Med. 2012, 1, 75–83. [Google Scholar] [CrossRef]
- Bernardo-Filho, M.; Taiar, R.; Sañudo, B.; Furness, T. Clinical Approaches of Whole Body Vibration Exercises. Rehabil. Res. Pract. 2018, 21, 9123625. [Google Scholar] [CrossRef]
- Sañudo, B.; Seixas, A.; Gloeckl, R.; Rittweger, J.; Rawer, R.; Taiar, R.; van der Zee, E.A.; van Heuvelen, M.J.; Lacerda, A.C.; Sartorio, A.; et al. Potential application of whole body vibration exercise for improving the clinical conditions of COVID-19 infected individuals: A narrative review from the world association of vibration exercise experts (wavex) panel. Int. J. Environ. Res. Public Health 2020, 17, 3650. [Google Scholar] [CrossRef]
- Sá-Caputo, D.C.; Seixas, A.; Taiar, R.; Bernardo-Filho, M. Vibration therapy for health promotion. In Complementary Therapies; IntechOpen: Rijeka, Croatia, 2022. [Google Scholar] [CrossRef]
- van Heuvelen, M.J.G.; Rittweger, J.; Judex, S.; Sañudo, B.; Seixas, A.; Fuermaier, A.B.M.; Tucha, O.; Nyakas, C.; Marín, P.J.; Taiar, R.; et al. Reporting guidelines for whole-body vibration studies in humans, animals and cell cultures: A consensus statement from an international group of experts. Biology 2021, 10, 965. [Google Scholar] [CrossRef]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef]
- Sá-Caputo, D.C.; Paineiras-Domingos, L.L.; Oliveira, R.; Neves, M.F.T.; Brandão, A.; Marin, P.J.; Sañudo, B.; Furness, T.; Taiar, R.; Bernardo-Filho, M. Acute effects of whole-body vibration on the pain level, flexibility, and cardiovascular responses in individuals with metabolic syndrome. Dose-Response 2018, 16, 1559325818802139. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Marconi, E.; Dionello, C.F.; Morel, D.S.; Sá-Caputo, D.C.; Sousa-Gonçalves, C.R.; Paineiras-Domingos, L.L.; Teixeira-Silva, Y.; Pereira, M.J.S.; Bernardo-Filho, M. Whole body vibration and auriculotherapy improve handgrip strength in individuals with knee osteoarthritis. J. Tradit. Chin. Med. 2019, 39, 707–715. [Google Scholar]
- Paiva, P.C.; Figueiredo, C.A.; Reis-Silva, A.; Francisca-Santos, A.; Paineiras-Domingos, L.L.; Martins-Anjos, E.; Melo-Oliveira, M.E.S.; Moreira-Marconi, E.; Guedes-Aguiar, E.O.; Xavier, V.L.; et al. Acute and cumulative effects with whole-body vibration exercises using 2 biomechanical conditions on the flexibility and rating of perceived exertion in individuals with metabolic syndrome: A randomized clinical trial pilot study. Dose-Response 2019, 17, 1559325819886495. [Google Scholar] [CrossRef] [PubMed]
- Karatrantou, K.; Bilios, P.; Bogdanis, G.C.; Ioakimidis, P.; Soulas, E.; Gerodimos, V. Effects of whole-body vibration training frequency on neuromuscular performance: A randomized controlled study. Biol. Sport 2019, 36, 273–282. [Google Scholar] [CrossRef]
- Saldıran, T.Ç.; Atıcı, E.; Rezaei, D.A.; Öztürk, Ö.; Uslu, B.; Özcan, B.A.; Melo-Oliveira, M.E.S.; Lourenço-Revelles, G.M.G.; Moreira-Marconi, E.; Guedes-Aguiar, E.O.; et al. The acute effects of different intensity whole-body vibration exposure on muscle tone and strength of the lower legs, and hamstring flexibility: A pilot study. J. Sport Rehabil. 2021, 30, 235–241. [Google Scholar] [CrossRef]
- Paineiras-Domingos, L.L.; da Cunha Sá-Caputo, D.; Reis, A.S.; Francisca Santos, A.; Sousa-Gonçalves, C.R.; dos Anjos, E.M.; Pereira, M.J.d.S.; Sartorio, A.; Bernardo-Filho, M. Assessment through the short physical performance battery of the functionality in individuals with metabolic syndrome exposed to whole-body vibration exercises. Dose-Response 2018, 1, 16. [Google Scholar] [CrossRef]
- Sá-Caputo, D.C.; Paineiras-Domingos, L.L.; Francisca-Santos, A.; dos Anjos, E.M.; Reis, A.S.; Neves, M.F.T.; Oigman, W.; Oliveira, R.; Brandão, A.; Machado, C.B.; et al. Whole-body vibration improves the functional parameters of individuals with metabolic syndrome: An exploratory study. BMC Endocr. Disord. 2019, 19, 6. [Google Scholar] [CrossRef]
- Lamari, N.; Marino, L.C.; Cordeiro, J.A.; Pellegrini, A.M. Flexibilidade anterior do tronco no adolecente após o pico da velocidade de crescimento em estatura. Acta Ortop. Bras. 2007, 15, 25–29. [Google Scholar] [CrossRef]
- Lee, S.Y. Handgrip strength: An irreplaceable indicator of muscle function. Ann. Rehabil. Med. 2021, 45, 167–169. [Google Scholar] [CrossRef]
- Zhou, J.; Pang, L.; Chen, N.; Wang, Z.; Wang, C.; Hai, Y.; Lyu, M.; Lai, H.; Lin, F. Whole-body vibration training—Better care for COPD patients: A systematic review and meta-analysis. Int. J. Chron. Obstruct. Pulm. Dis. 2018, 10, 3243–3254. [Google Scholar] [CrossRef]
- Lage, V.K.S.; Lacerda, A.C.R.; Neves, C.D.C.; Chaves, M.G.A.; Soares, A.A.; Lima, L.P.; Matos, M.A.; Leite, H.R.; Fernandes, J.S.C.; Oliveira, V.C.; et al. Cardiorespiratory responses in different types of squats and frequencies of whole body vibration in patients with chronic obstructive pulmonary disease. J. Appl. Physiol. 2019, 126, 23–29. [Google Scholar] [CrossRef]
- Gloeckl, R.; Schneeberger, T.; Leitl, D.; Reinold, T.; Nell, C.; Jarosch, I.; Kenn, K.; Koczulla, A.R. Whole-body vibration training versus conventional balance training in patients with severe COPD—A randomized, controlled trial. Resp. Res. 2021, 4, 138. [Google Scholar] [CrossRef]
- Jeong, M.; Kang, H.K.; Song, P.; Park, H.K.; Jung, H.; Lee, S.-S.; Koo, H.-K. Hand grip strength in patients with chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulm. Dis. 2017, 12, 2385–2390. [Google Scholar] [CrossRef]
- Fonseca, J.; Machado, F.V.C.; Santin, L.C.; Medeiros, L.; Andrello, A.C.; Hernandes, N.A.; Pitta, F. Use of different reference values for handgrip strength in individuals with COPD: Analysis of agreement, discriminative capacity, and main clinical implications. J. Bras. Pneumol. 2022, 48, e20210510. [Google Scholar] [CrossRef]
- Severijns, D.; Lamers, I.; Kerkhofs, L.; Feys, P. Hand grip fatigability in persons with multiple sclerosis according to hand dominance and disease progression. J. Rehabil. Med. 2015, 47, 154–160. [Google Scholar] [CrossRef]
- Sá-Caputo, D.C.; Ronikeili-Costa, P.; Carvalho-Lima, R.P.P.; Bernardo, L.C.C.; Bravo-Monteiro, M.O.O.; Costa, R.; De Moraes-Silva, J.; Paiva, D.N.; Machado, C.B.; Mantilla-Giehl, P.; et al. Whole-body vibration exercises and the improvement of the flexibility in patient with metabolic syndrome. Rehabil. Res. Pract. 2014, 2014, 628518. [Google Scholar] [CrossRef]
- Perret, C.; Poiraudeau, S.; Fermanian, J.; Colau, M.M.; Benhamou, M.A.; Revel, M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch. Phys. Med. Rehabil. 2001, 82, 566–570. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Fess, E.E. A method for checking Jamar dynamometer calibration. J. Hand Ther. 1987, 1, 28–32. [Google Scholar] [CrossRef]
- Coelho-Oliveira, A.C.; Lacerda, A.C.R.; de Souza, A.L.C.; Santos, L.M.M.; Fonseca, S.F.; dos Santos, J.M.; Ribeiro, V.G.C.; Leite, H.R.; Figueiredo, P.H.S.; Fernandes, J.S.C.; et al. Acute whole-body vibration exercise promotes favorable handgrip neuromuscular modifications in rheumatoid arthritis: A cross-over randomized clinical. BioMed Res. Int. 2021, 2, 9774980. [Google Scholar] [CrossRef]
- Sousa-Gonçalves, C.R.; Tringali, G.; Tamini, S.; De Micheli, R.; Soranna, D.; Taiar, R.; Sá-Caputo, D.; Moreira-Marconi, E.; Paineiras-Domingos, L.; Bernardo-Filho, M.; et al. Acute effects of whole-body vibration alone or in combination with maximal voluntary contractions on cardiorespiratory, musculoskeletal, and neuromotor fitness in obese male adolescents. Dose-Response 2019, 17, 1559325819890492. [Google Scholar] [CrossRef]
- Ahmadi, A.; Eftekhari, M.H.; Mazloom, Z.; Masoompour, M.; Fararooei, M.; Eskandari, M.H.; Mehrabi, S.; Bedeltavana, A.; Famouri, M.; Zare, M.; et al. Fortified whey beverage for improving muscle mass in chronic obstructive pulmonary disease: A single-blind, randomized clinical trial. Resp. Res. 2020, 21, 216. [Google Scholar] [CrossRef]
- Strandkvist, V.; Andersson, M.; Backman, H.; Larsson, A.; Stridsman, C.; Lindberg, A. Hand grip strength is associated with fatigue among men with COPD: Epidemiological data from northern Sweden. Physiother. Theory Pract. 2020, 36, 408–416. [Google Scholar] [CrossRef]
- Cheung, C.-L.; Nguyen, U.-S.D.T.; Au, E.; Tan, K.C.B.; Kung, A.W.C. Association of handgrip strength with chronic diseases and multimorbidity. Age 2013, 35, 929–941. [Google Scholar] [CrossRef]
- Tsuburai, T.; Komase, Y.; Tsuruoka, H.; Oyama, B.; Muraoka, H.; Hida, N.; Kobayashi, T.; Matsushima, S. The relationship between peak inspiratory flow and hand grip strength measurement in men with mild chronic obstructive pulmonary disease. BMC Pulm. Med. 2022, 22, 65. [Google Scholar] [CrossRef]
- Turan, Z.; Özyemişçi Taşkıran, Ö.; Erden, Z.; Köktürk, N.; Kaymak Karataş, G. Does hand grip strength decrease in chronic obstructive pulmonary disease exacerbation? A cross-sectional study. Turk. J. Med. Sci. 2019, 49, 802–808. [Google Scholar] [CrossRef]
- Pfeifer, C.E.; Ross, L.M.; Weber, S.R.; Sui, X.; Blair, S.N. Are flexibility and muscle-strengthening activities associated with functional limitation? Sports Med. Health Sci. 2022, 4, 95–100. [Google Scholar] [CrossRef]
- Cardinale, M.; Bosco, C. The use of vibration as an exercise session. Exerc. Sport Sci. Rev. 2003, 31, 3–7. [Google Scholar] [CrossRef]
- Di Giminiani, R.; Manno, R.; Scrimaglio, R.; Sementilli, G.; Tihanyi, J. Effects of individualized whole-body vibration on muscle flexibility and mechanical power. J. Sports Med. Phys. Fit. 2010, 50, 139–151. [Google Scholar]
- Fowler, B.D.; Palombo, K.T.M.; Feland, J.B.; Blotter, J.D. Effects of whole-body vibration on flexibility and stiffness: A literature review. Int. J. Exerc. Sci. 2019, 12, 735–747. [Google Scholar]
- Kerti, M.; Balogh, Z.; Kelemen, K.; Varga, J.T. The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD. Int. J. Chron. Obstruct. Pulm. Dis. 2018, 13, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Ritzmann, R.; Kramer, A.; Gruber, M.; Gollhofer, A.; Taube, W. EMG activity during whole body vibration: Motion artifacts or stretch reflexes? Eur. J. Appl. Physiol. 2010, 110, 143–151. [Google Scholar] [CrossRef]
- Cochrane, D.J.; Stannard, S.R.; Firth, E.C.; Rittweger, J. Acute whole-body vibration elicits post-activation potentiation. Eur. J. Appl. Physiol. 2010, 108, 311–319. [Google Scholar] [CrossRef]
- Cardim, A.B.; Marinho, P.E.; Nascimento, J.F.; Fuzari, H.K.; Dornelas de Andrade, A. Does whole-body vibration improve the functional exercise capacity of subjects with COPD? A meta-analysis. Respir. Care 2016, 61, 1552–1559. [Google Scholar] [CrossRef]
- Torres-Nunes, L.; da Costa-Borges, P.P.; Paineiras-Domingos, L.L.; Bachur, J.A.; Coelho-Oliveira, A.C.; da Cunha de Sá-Caputo, D.; Bernardo-Filho, M. Effects of the whole-body vibration exercise on sleep disorders, body temperature, body composition, tone, and clinical parameters in a child with down syndrome who underwent total atrioventricular septal defect surgery: A case-report. Children 2023, 10, 213. [Google Scholar] [CrossRef]
- Lage, V.K.S.; Lacerda, A.C.R.; Neves, C.D.C.; Chaves, M.G.A.; Soares, A.A.; Lima, L.P.; Martins, J.B.; Matos, M.A.; Vieira, L.M.; Teixeira, A.L.; et al. Acute effects of whole-body vibration on inflammatory markers in people with chronic obstructive pulmonary disease: A pilot study. Rehabil. Res. Pract. 2018, 2, 5480214. [Google Scholar] [CrossRef]
- Rhee, S.Y.; Song, J.K.; Hong, S.C.; Choi, J.W.; Jeon, H.J.; Shin, D.H.; Ji, E.H.; Choi, E.-H.; Lee, J.; Kim, A.; et al. Intradialytic exercise improves physical function and reduces intradialytic hypotension and depression in hemodialysis patients. Korean J. Intern. Med. 2019, 34, 588–598. [Google Scholar] [CrossRef]
- Puhan, M.A.; Gimeno-Santos, E.; Cates, C.J.; Troosters, T. Pulmonary rehabilsitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2009, 21, CD005305. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | SitG (n = 21) | StandG (n = 17) | p Value |
|---|---|---|---|
| Age (years) | 67.62 ± 6.65 | 67.82 ± 2.65 | p ˃ 0.05 |
| Gender (F/M) | 9/12 | 10/7 | ----- |
| Height (cm) | 160 ± 10.35 | 150.5 ± 29.56 | p ˃ 0.05 |
| Body mass (kg) | 67.33 ± 17.36 | 69.38 ± 18.03 | p ˃ 0.05 |
| BMI (kg/m2) | 25.81 ± 5.54 | 26.02 ± 4.93 | p ˃ 0.05 |
| DMT2 | 5% | 5% | ------ |
| SAH | 10% | 9% | ------ |
| Tabagism | 60% | 70% | ------ |
| pSO2 (%) | 95.95 ± 5.39 | 98.29 ± 0.58 | p ˃ 0.05 |
| RR (rpm) | 20.11 ± 3.32 | 19.50 ± 1.77 | p ˃ 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guedes-Aguiar, E.d.O.; Taiar, R.; Paineiras-Domingos, L.L.; Monteiro-Oliveira, B.B.; da Cunha de Sá-Caputo, D.; Bernardo-Filho, M. Effects of a Single Session of Systemic Vibratory Therapy on Flexibility, Perception of Exertion and Handgrip Strength in Chronic Obstructive Pulmonary Disease Individuals: A Quasi-Experimental Clinical Trial. J. Clin. Med. 2023, 12, 3241. https://doi.org/10.3390/jcm12093241
Guedes-Aguiar EdO, Taiar R, Paineiras-Domingos LL, Monteiro-Oliveira BB, da Cunha de Sá-Caputo D, Bernardo-Filho M. Effects of a Single Session of Systemic Vibratory Therapy on Flexibility, Perception of Exertion and Handgrip Strength in Chronic Obstructive Pulmonary Disease Individuals: A Quasi-Experimental Clinical Trial. Journal of Clinical Medicine. 2023; 12(9):3241. https://doi.org/10.3390/jcm12093241
Chicago/Turabian StyleGuedes-Aguiar, Eliane de Oliveira, Redha Taiar, Laisa Liane Paineiras-Domingos, Bruno Bessa Monteiro-Oliveira, Danúbia da Cunha de Sá-Caputo, and Mario Bernardo-Filho. 2023. "Effects of a Single Session of Systemic Vibratory Therapy on Flexibility, Perception of Exertion and Handgrip Strength in Chronic Obstructive Pulmonary Disease Individuals: A Quasi-Experimental Clinical Trial" Journal of Clinical Medicine 12, no. 9: 3241. https://doi.org/10.3390/jcm12093241
APA StyleGuedes-Aguiar, E. d. O., Taiar, R., Paineiras-Domingos, L. L., Monteiro-Oliveira, B. B., da Cunha de Sá-Caputo, D., & Bernardo-Filho, M. (2023). Effects of a Single Session of Systemic Vibratory Therapy on Flexibility, Perception of Exertion and Handgrip Strength in Chronic Obstructive Pulmonary Disease Individuals: A Quasi-Experimental Clinical Trial. Journal of Clinical Medicine, 12(9), 3241. https://doi.org/10.3390/jcm12093241