

Comparison of the Efficacy of Two Protocol Treatments in Patients with Symptomatic Disc Displacement without Reduction: A Randomized Controlled Trial
 ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
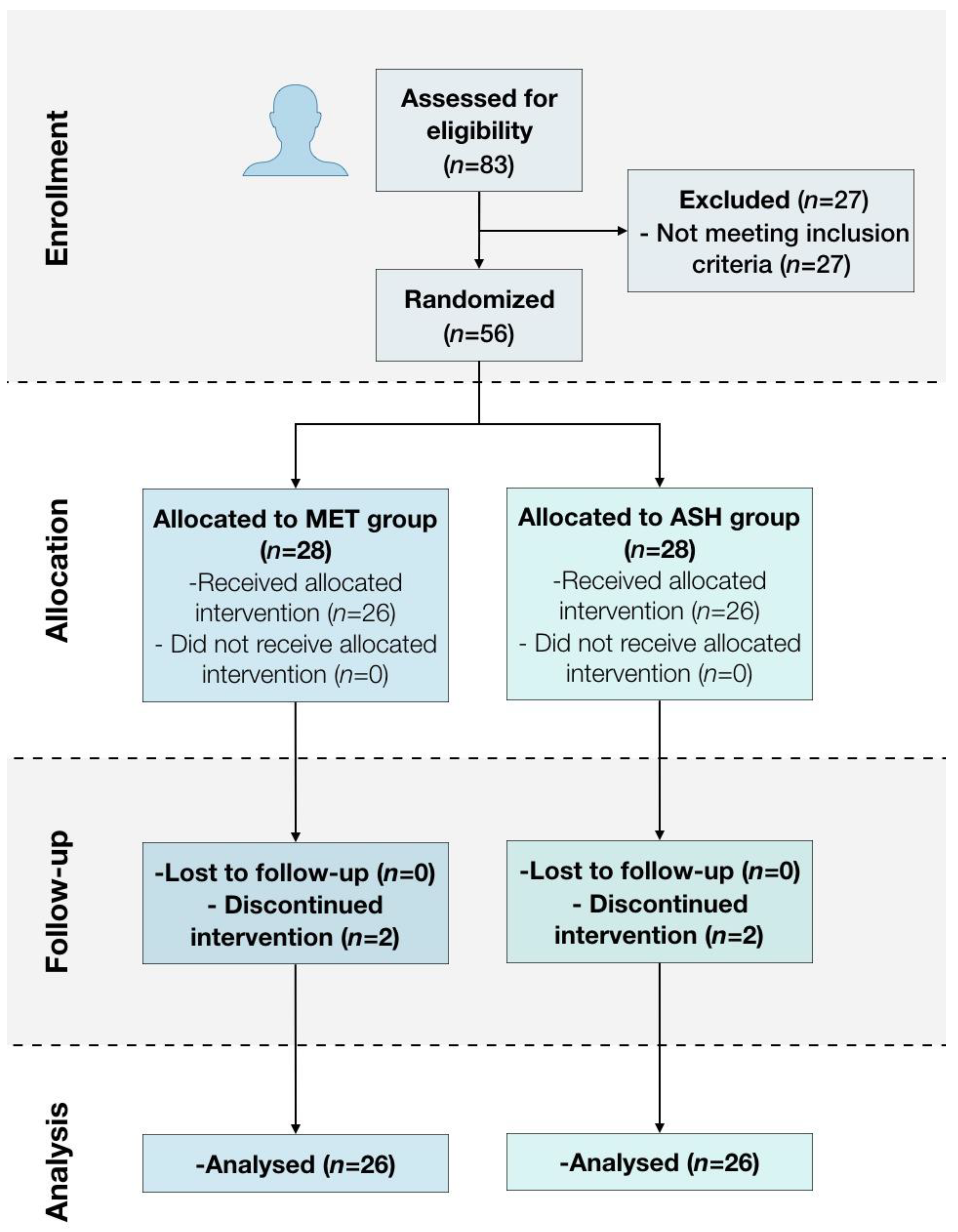
2.1. Participants
2.2. Study Protocol, Randomization, and Blinding
2.3. Interventions
2.3.1. Mandibular Exercise Therapy (MET Group)
2.3.2. Arthrocentesis + Sodium Hyalorante (ASH)
2.4. Outcomes
2.4.1. Pain Intensity (VAS)
2.4.2. Oral Health-Related Quality of Life (OHRQoL)
2.4.3. Mouth Opening (MO)
2.5. Statistical Methods
2.6. Changes to Protocol
3. Results
3.1. Patients’ Characteristics
3.2. Pain Intensity (VAS)
3.3. Oral Health-Related Quality of Life (OHIP-14)
3.4. Mouth Opening (MO)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okeson, J.P. Management of Temporomandibular Disorders and Occlusion, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2012; ISBN 978-0-323-08331-7. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of Temporomandibular Joint Disorders: A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.J.; Lamster, I.B.; Greenspan, J.S.; Pitts, N.B.; Scully, C.; Warnakulasuriya, S. Global Burden of Oral Diseases: Emerging Concepts, Management and Interplay with Systemic Health. Oral Dis. 2016, 22, 609–619. [Google Scholar] [CrossRef]
- Ferrillo, M.; Migliario, M.; Marotta, N.; Fortunato, F.; Bindi, M.; Pezzotti, F.; Ammendolia, A.; Giudice, A.; Foglio Bonda, P.L.; de Sire, A. Temporomandibular Disorders and Neck Pain in Primary Headache Patients: A Retrospective Machine Learning Study. Acta Odontol. Scand. 2023, 81, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Vale Braido, G.V.; do Svensson, P.; dos Santos Proença, J.; Mercante, F.G.; Fernandes, G.; de Godoi Gonçalves, D.A. Are Central Sensitization Symptoms and Psychosocial Alterations Interfering in the Association between Painful TMD, Migraine, and Headache Attributed to TMD? Clin. Oral Investig. 2022, 27, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Talaat, W.M.; Adel, O.I.; Al Bayatti, S. Prevalence of Temporomandibular Disorders Discovered Incidentally during Routine Dental Examination Using the Research Diagnostic Criteria for Temporomandibular Disorders. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Poluha, R.L.; Grossmann, E.; Iwaki, L.C.V.; Uchimura, T.T.; Santana, R.G.; Iwaki Filho, L. Myofascial Trigger Points in Patients with Temporomandibular Joint Disc Displacement with Reduction: A Cross-Sectional Study. J. Appl. Oral Sci. 2018, 26, e20170578. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardini, L.; Winocur, E.; Piccotti, F.; Ahlberg, J.; Lobbezoo, F. Research Diagnostic Criteria for Temporomandibular Disorders: A Systematic Review of Axis I Epidemiologic Findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 453–462. [Google Scholar] [CrossRef]
- Poveda-Roda, R.; Bagan, J.V.; Sanchis, J.-M.; Carbonell, E. Temporomandibular Disorders. A Case-Control Study. Med. Oral Patol. Oral Cir. Bucal 2012, 17, e794–e800. [Google Scholar] [CrossRef]
- Katzberg, R.W.; Westesson, P.L.; Tallents, R.H.; Drake, C.M. Anatomic Disorders of the Temporomandibular Joint Disc in Asymptomatic Subjects. J. Oral Maxillofac. Surg. 1996, 54, 147–153; discussion 153–155. [Google Scholar] [CrossRef]
- Wongwatana, S.; Kronman, J.H.; Clark, R.E.; Kabani, S.; Mehta, N. Anatomic Basis for Disk Displacement in Temporomandibular Joint (TMJ) Dysfunction. Am. J. Orthod. Dentofac. Orthop. 1994, 105, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Kavuncu, V.; Sahin, S.; Kamanli, A.; Karan, A.; Aksoy, C. The Role of Systemic Hypermobility and Condylar Hypermobility in Temporomandibular Joint Dysfunction Syndrome. Rheumatol. Int. 2006, 26, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Garcia, R.; Arrington, J.A. The Relationship between Cervical Whiplash and Temporomandibular Joint Injuries: An MRI Study. Cranio 1996, 14, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Pérez del Palomar, A.; Doblaré, M. An Accurate Simulation Model of Anteriorly Displaced TMJ Discs with and without Reduction. Med. Eng. Phys. 2007, 29, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Miernik, M.; Więckiewicz, W. The Basic Conservative Treatment of TMJ Anterior Disc Displacement Without Reduction-Review. Adv. Clin. Exp. Med. 2015, 24, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Naeije, M.; te Veldhuis, A.H.; te Veldhuis, E.C.; Visscher, C.M.; Lobbezoo, F. Disc Displacement within the Human Temporomandibular Joint: A Systematic Review of a ‘Noisy Annoyance’. J. Oral Rehabil. 2013, 40, 139–158. [Google Scholar] [CrossRef]
- Kurita, K.; Westesson, P.L.; Yuasa, H.; Toyama, M.; Machida, J.; Ogi, N. Natural Course of Untreated Symptomatic Temporomandibular Joint Disc Displacement without Reduction. J. Dent. Res. 1998, 77, 361–365. [Google Scholar] [CrossRef]
- Imirzalioglu, P.; Biler, N.; Agildere, A.M. Clinical and Radiological Follow-up Results of Patients with Untreated TMJ Closed Lock. J. Oral Rehabil. 2005, 32, 326–331. [Google Scholar] [CrossRef]
- Dimitroulis, G. The Prevalence of Osteoarthrosis in Cases of Advanced Internal Derangement of the Temporomandibular Joint: A Clinical, Surgical and Histological Study. Int. J. Oral Maxillofac. Surg. 2005, 34, 345–349. [Google Scholar] [CrossRef]
- Al-Baghdadi, M.; Durham, J.; Araujo-Soares, V.; Robalino, S.; Errington, L.; Steele, J. TMJ Disc Displacement without Reduction Management: A Systematic Review. J. Dent. Res. 2014, 93, 37S–51S. [Google Scholar] [CrossRef]
- La Touche, R.; Boo-Mallo, T.; Zarzosa-Rodríguez, J.; Paris-Alemany, A.; Cuenca-Martínez, F.; Suso-Martí, L. Manual Therapy and Exercise in Temporomandibular Joint Disc Displacement without Reduction. A Systematic Review. Cranio 2022, 40, 440–450. [Google Scholar] [CrossRef]
- Moldez, M.; Camones, V.; Ramos, G.; Padilla, M.; Enciso, R. Effectiveness of Intra-Articular Injections of Sodium Hyaluronate or Corticosteroids for Intracapsular Temporomandibular Disorders: A Systematic Review and Meta-Analysis. J. Oral Facial Pain Headache 2018, 32, 53–66. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.I.; Iizuka, T.; Matsuki, M.; Ono, T. Recapturing the Persistent Anteriorly Displaced Disk by Mandibular Manipulation after Pumping and Hydraulic Pressure to the Upper Joint Cavity of the Temporomandibular Joint. Cranio 1987, 5, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Nagori, S.A.; Roy Chowdhury, S.K.; Thukral, H.; Jose, A.; Roychoudhury, A. Single Puncture versus Standard Double Needle Arthrocentesis for the Management of Temporomandibular Joint Disorders: A Systematic Review. J. Oral Rehabil. 2018, 45, 810–818. [Google Scholar] [CrossRef]
- Guarda-Nardini, L.; De Almeida, A.; Manfredini, D. Arthrocentesis of the Temporomandibular Joint: Systematic Review and Clinical Implications of Research Findings. J. Oral Facial Pain Headache 2021, 35, 17–29. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, S.; Fang, F. Arthrocentesis vs Conservative Therapy for the Management of TMJ Disorders: A Systematic Review and Meta-Analysis. J. Stomatol. Oral Maxillofac. Surg. 2023, 124, 101283. [Google Scholar] [CrossRef] [PubMed]
- Guarda-Nardini, L.; Manfredini, D.; Ferronato, G. Arthrocentesis of the Temporomandibular Joint: A Proposal for a Single-Needle Technique. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.; Fonseca, R.; Cunha, T.; Oliveira, P.; Gonçalvez, R.; Grossmann, E.; Almeida-Leite, C.; Januzzi, E. Temporoman-dibular Joint Dysfunction—Sequential Infiltration Protocol of Sodium Hyaluronate at Different Molecular Weights. Ann Med. 2019, 28, 51. [Google Scholar] [CrossRef]
- Ohrbach, R. (Ed.) Diagnostic Criteria for Temporomandibular Disorders: Assessment Instruments. Version 15 May 2016. [Critérios de Diagnóstico para Disfunção Temporomandibular: Portuguese Version Sept2017] Faria C, Coutinho FA, Resende T, Ferreira H, Gonçalves M, Gomes R, Gomes D, Pinto JC, Trans. Available online: www.rdc-tmdinternational.org (accessed on 20 March 2020).
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of Four Pain Intensity Rating Scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- Amaral, J.; Sanches, C.; Marques, D.; Vaz Patto, J.; Barcelos, F.; Mata, A. Validation of Oral Health Impact Profile-14 and Its Association with Hypossialia in a Sjögren Syndrome Portuguese Population. Acta Reumatol. Port. 2018, 43, 137–145. [Google Scholar]
- Ozdamar, S.M.; Alev, B.; Yarat, A. The Impact of Arthrocentesis with and without Hyaluronic Acid Injection in the Prognosis and Synovial Fluid Myeloperoxidase Levels of Patients with Painful Symptomatic Internal Derangement of Temporomandibular Joint: A Randomised Controlled Clinical Trial. J. Oral Rehabil. 2017, 44, 73–80. [Google Scholar] [CrossRef]
- Öhrnell Malekzadeh, B.; Johansson Cahlin, B.; Widmark, G. Conservative Therapy versus Arthrocentesis for the Treatment of Symptomatic Disk Displacement without Reduction: A Prospective Randomized Controlled Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Li, D.T.S.; Wong, N.S.M.; Li, S.K.Y.; McGrath, C.P.; Leung, Y.Y. Timing of Arthrocentesis in the Management of Temporomandibular Disorders: An Integrative Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2021, 50, 1078–1088. [Google Scholar] [CrossRef] [PubMed]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Mechanisms of Action and Efficacy of Hyaluronic Acid, Corticosteroids and Platelet-Rich Plasma in the Treatment of Temporomandibular Joint Osteoarthritis—A Systematic Review. Int. J. Mol. Sci. 2021, 22, 7405. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.L.; Look, J.O.; Hodges, J.S.; Swift, J.Q.; Decker, K.L.; Hathaway, K.M.; Templeton, R.B.; Fricton, J.R. Randomized Effectiveness Study of Four Therapeutic Strategies for TMJ Closed Lock. J. Dent. Res. 2007, 86, 58–63. [Google Scholar] [CrossRef]
- Poluha, R.L.; De la Torre Canales, G.; Bonjardim, L.R.; Conti, P.C.R. Somatosensory and Psychosocial Profile of Patients with Painful Temporomandibular Joint Clicking. J. Oral Rehabil. 2020, 47, 1346–1357. [Google Scholar] [CrossRef]
- Bitiniene, D.; Zamaliauskiene, R.; Kubilius, R.; Leketas, M.; Gailius, T.; Smirnovaite, K. Quality of Life in Patients with Temporomandibular Disorders. A Systematic Review. Stomatologija 2018, 20, 3–9. [Google Scholar]
- Castaño-Joaqui, O.G.; Maza Muela, C.; Casco Zavala, B.; Casares García, G.; Domínguez Gordillo, A.Á. Long Term Oral Health Related Quality of Life after TMJ Arthrocentesis with Hyaluronic Acid. A Retrospective Cohort Study. J. Craniomaxillofac. Surg. 2022, 50, 583–589. [Google Scholar] [CrossRef]


{kind=link}
| MET (n = 26) | ASH (n = 26) | p-Value | |
|---|---|---|---|
| Age, mean (SD) | 48.6 (14.3) | 47.3 (18.3) | 0.964 |
| Sex, n (%) | |||
| Females | 22 (84.6) | 16 (61.5) | 0.118 |
| Males | 4 (15.4) | 10 (38.5) | |
| Education, n (%) | |||
| Elementary | 1 (3.8) | 5 (19.2) | 0.217 |
| Middle | 2 (7.7) | 10 (38.5) | |
| Higher | 2 (7.1) | 7 (25.0) | |
| DDwR, n (%) | |||
| Unilateral plus myalgia | 20 (76.9) | 22 (84.6) | 0.482 |
| Bilateral plus myalgia | 6 (23.1) | 4 (15.4) |
| Periods | MET (n = 26) | ASH (n = 26) | p-Value | |
|---|---|---|---|---|
| Baseline | 6.8 (2.3) | 6.7 (2.2) | 0.648 | |
| VAS (mm) | 1 month | 5.0 (2.4) | 3.3 (1.2) | 0.328 |
| 12 months | 3.0 (2.5) | 2.4 (2.1) | 0.355 |
| OHIP-14, Mean (SD) | MET (n = 26) | ASH (n = 26) | p-Value |
|---|---|---|---|
| Functional Limitation | |||
| Baseline | 2.6 (1.8) | 2.4 (2.0) | 0.597 |
| 1 month | 1.4 (1.4) | 1.1 (1.1) | 0.600 |
| 12 months | 1.5 (1.1) | 0.7 (0.7) | 0.008 * |
| Physical Pain | |||
| Baseline | 6.4 (1.3) | 5.8 (1.4) | 0.116 |
| 1 month | 4.9 (2.0) | 3.3 (1.2) | 0.001 * |
| 12 months | 4.5 (2.0) | 3.6 (1.4) | 0.120 |
| Psychological Discomfort | |||
| Baseline | 5.3 (1.7) | 4.6 (2.0) | 0.246 |
| 1 month | 2.9 (2.2) | 2.2 (1.6) | 0.253 |
| 12 months | 3.7 (2.1) | 1.7 (1.4) | <0.001 * |
| Physical Disability | |||
| Baseline | 4.9 (1.8) | 5.4 (1.6) | 0.270 |
| 1 month | 4.0 (2,1) | 2.3 (1.6) | 0.002 * |
| 12 months | 3.6 (2.4) | 2.5 (1.7) | 0.101 |
| Psychological Disability | |||
| Baseline | 4.2 (1.8) | 3.2 (1.8) | 0.024 |
| 1 month | 2.9 (1.8) | 1.8 (1.5) | 0.029 |
| 12 months | 3.2 (1.9) | 1.5 (1.0) | <0.001 * |
| Social | |||
| Baseline | 3.9 (2.0) | 3.3 (2.1) | 0.460 |
| 1 month | 2.3 (1.9) | 1.2 (1.4) | 0.253 |
| 12 months | 2.7 (1.9) | 1.4 (2.1) | <0.001 * |
| Handicap | |||
| Baseline | 3.0 (1.9) | 2.2 (1.4) | 0.131 |
| 1 month | 1.9 (1.5) | 1.0 (0.8) | 0.033 |
| 12 months | 2.3 (1.6) | 1.1 (1.0) | 0.005 * |
| DC/TMD—Axis I | MET (n = 26) | ASH (n = 26) | p-Value |
|---|---|---|---|
| Pain-free opening | |||
| Baseline | 33.6 (6.2) | 32.6 (5.9) | 0.378 |
| 1 month | 37.2 (5.9) | 38.8 (4.5) | 0.254 |
| 12 months | 37.5 (5.0) | 39.5 (4.7) | 0.125 |
| Difference from baseline | |||
| At 1 month | 3.7 (3.1) | 6.2 (4.4) | 0.007 * |
| At 12 months | 3.9 (3.4) | 6.9 (4.5) | 0.016 * |
| Maximum unassisted opening | |||
| Baseline | 37.1 (5.5) | 36.0 (4.9) | 0.239 |
| 1 month | 39.5 (5.1) | 41.4 (4.0) | 0.142 |
| 12 months | 39.8 (4.6) | 41.7 (4.2) | 0.101 |
| Difference from baseline | |||
| At 1 month | 2.4 (2.5) | 5.4 (3.2) | 0.003 * |
| At 12 months | 2.4 (2.5) | 5.6 (3.7) | 0.008 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Almeida, A.M.; Botelho, J.; Machado, V.; Mendes, J.J.; Manso, C.; González-López, S. Comparison of the Efficacy of Two Protocol Treatments in Patients with Symptomatic Disc Displacement without Reduction: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 3228. https://doi.org/10.3390/jcm12093228
de Almeida AM, Botelho J, Machado V, Mendes JJ, Manso C, González-López S. Comparison of the Efficacy of Two Protocol Treatments in Patients with Symptomatic Disc Displacement without Reduction: A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(9):3228. https://doi.org/10.3390/jcm12093228
Chicago/Turabian Stylede Almeida, André Mariz, João Botelho, Vanessa Machado, José João Mendes, Cristina Manso, and Santiago González-López. 2023. "Comparison of the Efficacy of Two Protocol Treatments in Patients with Symptomatic Disc Displacement without Reduction: A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 9: 3228. https://doi.org/10.3390/jcm12093228
APA Stylede Almeida, A. M., Botelho, J., Machado, V., Mendes, J. J., Manso, C., & González-López, S. (2023). Comparison of the Efficacy of Two Protocol Treatments in Patients with Symptomatic Disc Displacement without Reduction: A Randomized Controlled Trial. Journal of Clinical Medicine, 12(9), 3228. https://doi.org/10.3390/jcm12093228